The novel second-generation triterpenoid SCY-247 maintains in vitro and in vivo activity against resistant Candida glabrata
Nathan P. Wiederhold, Laura K. Najvar, Rosie Jaramillo, Marcos Olivo, Hoja P. Patterson, Thomas F. Patterson

TL;DR
SCY-247 is a new antifungal drug that works against drug-resistant Candida glabrata both in lab tests and in mice.
Contribution
SCY-247 shows in vitro and in vivo efficacy against echinocandin-resistant Candida glabrata strains.
Findings
SCY-247 maintained in vitro activity against 24 of 29 echinocandin-resistant C. glabrata strains.
SCY-247 reduced fungal burden in mouse kidneys and lungs in a dose-dependent manner.
Fluconazole and caspofungin failed to reduce fungal burden in mice with resistant C. glabrata infections.
Abstract
Candida glabrata is a major cause of invasive candidiasis and is considered a high-priority fungal pathogen by the World Health Organization. SCY-247 is a second-generation IV/oral triterpenoid antifungal that targets the fungal cell wall by inhibiting glucan synthase. We evaluated the in vitro activity and in vivo efficacy of SCY-247 against echinocandin-resistant C. glabrata. Susceptibility testing was performed against 34 C. glabrata clinical strains, including 29 echinocandin non-susceptible or resistant strains, by the CLSI broth microdilution method. Neutropenic mice were infected intravenously with either an echinocandin-susceptible or resistant strain. Treatment with vehicle control, SCY-247 (16, 32, and 48 mg/kg PO BID), fluconazole (20 mg/kg PO QD), or caspofungin (5 mg/kg IP QD) was initiated 24 hours post-inoculation. Treatment continued for 7 days, and kidney and lung…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
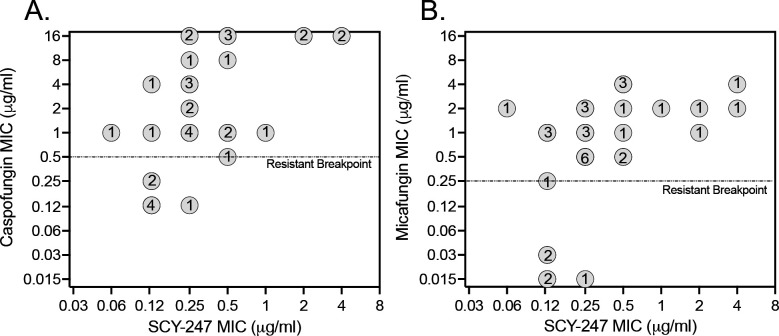 Fig 1
Fig 1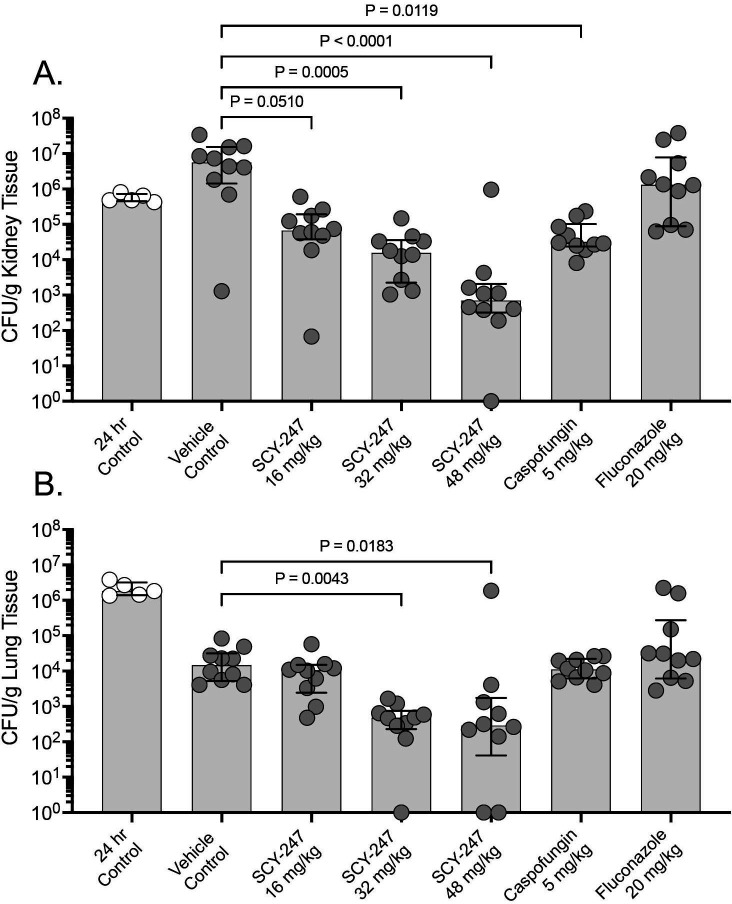 Fig 2
Fig 2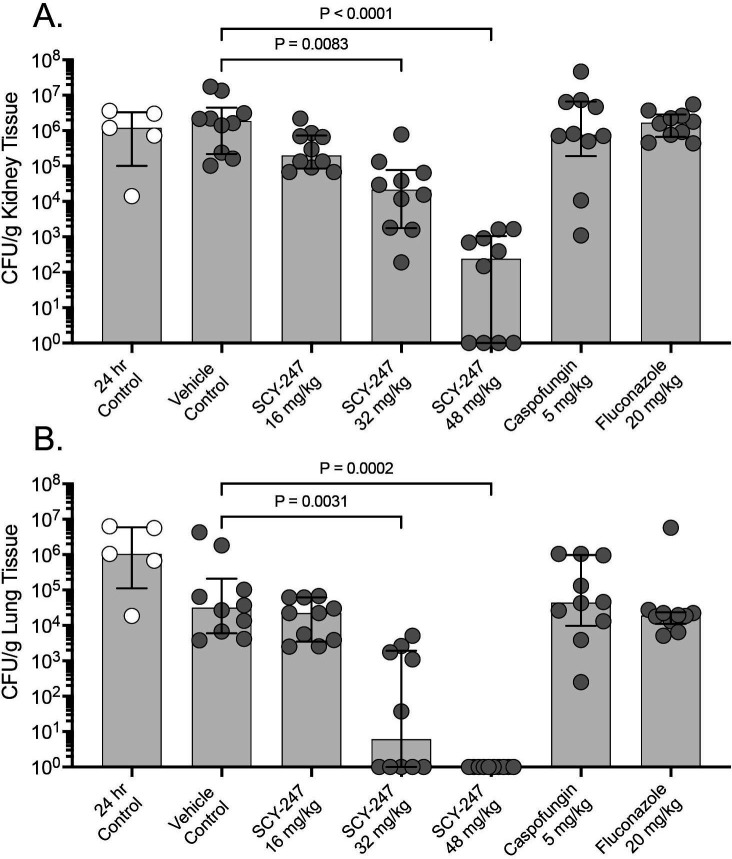 Fig 3
Fig 3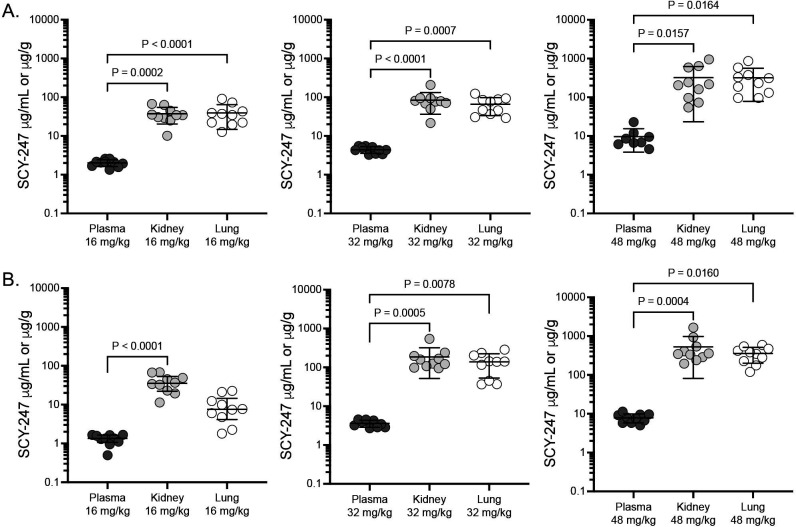 Fig 4
Fig 4| Parameter | SCY-247 | Caspofungin | Micafungin | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All strains | |||||||||||||
| Range | 0.06–4 | 0.125–>8 | ≤0.015–4 | ||||||||||
| MIC50 | 0.25 | 2 | 1 | ||||||||||
| MIC90 | 2 | >8 | 4 | ||||||||||
| GM | 0.325 | 1.920 | 0.635 | ||||||||||
| Modal MIC | 0.25 | 1 | 0.5 | ||||||||||
| Echinocandin non-susceptible or resistant strains | |||||||||||||
| Range | 0.06–4 | 0.25–>8 | 0.25–4 | ||||||||||
| MIC50 | 0.25 | 4 | 1 | ||||||||||
| MIC90 | 2 | >8 | 4 | ||||||||||
| GM MIC | 0.375 | 3.075 | 1.154 | ||||||||||
| Modal MIC | 0.25 | 1 | 0.5 | ||||||||||
| MIC distributions | |||||||||||||
| MIC value | 0.015 | 0.03 | 0.06 | 0.12 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | ≥16 | ||
| SCY-247 | 1 | 8 | 13 | 7 | 1 | 2 | 2 | ||||||
| Caspofungin | 5 | 2 | 1 | 9 | 2 | 4 | 2 | 9 | |||||
| Micafungin | 3 | 2 | 1 | 8 | 8 | 8 | 4 | ||||||
| Treatment group | Echinocandin-susceptible strain | Echinocandin-resistant strain | ||
|---|---|---|---|---|
| Kidney | Lungs | Kidney | Lungs | |
| Vehicle control | 1.07 | −2.10 | 0.19 | −1.52 |
| SCY-247 16 mg/kg | −0.86 | −2.24 | −0.78 | −1.67 |
| SCY-247 32 mg/kg | −1.49 | −3.58 | −1.75 | −5.24 |
| SCY-247 48 mg/kg | −2.83 | −3.80 | −3.70 | −6.02 |
| Caspofungin 5 mg/kg | −1.21 | −2.22 | −0.20 | −1.38 |
| Fluconazole 20 mg/kg | 0.44 | −1.85 | 0.15 | −1.74 |
- —National Institutes of Healthhttp://dx.doi.org/10.13039/100000002
- —National Institutes of Healthhttp://dx.doi.org/10.13039/100000002
- —Scynexis
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Microbial Natural Products and Biosynthesis
INTRODUCTION
Of the invasive mycoses, invasive candidiasis is often the most prevalent, as Candida species are common causes of hospital-acquired pathogens and nosocomial bloodstream infections (1–3). These invasive infections are associated with significant morbidity and mortality (1, 4, 5). In the United States, the second most prevalent species associated with invasive infection is Candida glabrata (now known as Nakaseomyces glabratus) (3, 4). In 2022, this species was designated as a high-priority fungal pathogen by the World Health Organization (6). Current treatment strategies for invasive infections caused by this pathogen include the use of the azoles (e.g., fluconazole, isavuconazole, voriconazole, and posaconazole), a lipid formulation of amphotericin B (polyene), or the echinocandins (anidulafungin, caspofungin, micafungin, and rezafungin) (7). Although effective, each of these classes has drawbacks that may limit clinical responses. For example, amphotericin B formulations are associated with significant nephrotoxicity and are only available intravenously. The echinocandins, although clinically safer than the polyenes, are also only available for intravenous administration, which may limit their use in outpatients. Fluconazole has been a safe and effective treatment option over many years for patients with invasive candidiasis, and this antifungal is available in both oral and intravenous formulations. However, C. glabrata demonstrates reduced susceptibility to fluconazole, and invasive disease caused by fluconazole- and/or echinocandin-resistant C. glabrata strains has been documented at many centers in the United States and other parts of the world (8, 9). Thus, the development of new therapeutic strategies for invasive candidiasis, including those infections caused by resistant C. glabrata, is of paramount importance.
SCY-247 is a second-generation member of the triterpenoid class of antifungals and has potent in vitro activity against Candida species, including C. auris, other yeasts, and several filamentous fungi (10, 11). This in vitro activity has also translated into in vivo efficacy in a murine model of invasive candidiasis caused by C. albicans (12). The objective of this study was to evaluate the in vitro and in vivo activity of SCY-247 against C. glabrata, including echinocandin-resistant strains.
RESULTS
In vitro susceptibility
SCY-247 MICs ranged from 0.06 to 4 μg/mL against all strains (n = 34) included in this study (Table 1). SCY-247, caspofungin, and micafungin MICs ranged from 0.125 to 0.25 μg/mL, 0.125 μg/mL, and ≤0.015–0.03 μg/mL, respectively, against the 5 echinocandin-susceptible strains. Against the 29 strains classified as echinocandin non-susceptible or resistant strains per the CLSI breakpoints (13), SCY-247 MICs ranged from 0.06 to 4 μg/mL, with MIC_90_ and modal MIC values of 2 μg/mL and 0.25 μg/mL, respectively, and the in vitro activity was maintained against 24 of the 29 strains (MIC ≤0.5 µg/mL; Table 1 and Fig. 1). In contrast, against these non-susceptible or resistant strains, caspofungin and micafungin MICs ranged from 0.25 to >8 µg/mL and 0.25 to 4 μg/mL, respectively, with both having higher MIC_90_ values (>8 µg/mL and 4 μg/mL, respectively) and modal MICs (1 μg/mL and 0.5 μg/mL, respectively) than that of SCY-247. SCY-247, fluconazole, and caspofungin MICs were 0.125 μg/mL, 4 μg/mL, and 0.125 μg/mL, respectively, against the echinocandin-susceptible strain used in the in vivo model. Against the echinocandin-resistant strain used to establish invasive disease, the MICs were 0.25 μg/mL, 64 μg/mL, and >8 µg/mL, respectively.
SCY-247 versus caspofungin MICs (A) and SCY-247 versus micafungin MICs (B) against 29 echinocandin non-susceptible or resistant strains of Candida glabrata and 5 echinocandin-susceptible strains. All values are reported in μg/mL. Dotted horizontal lines represent CLSI resistant breakpoints for caspofungin (0.5 μg/mL) and micafungin (0.25 μg/mL) against Candida glabrata. Circled numbers represent the number of strains at SCY-247/caspofungin and SCY-247/micafungin MIC combinations. Two strains had caspofungin MIC values that were classified as intermediate (0.25 μg/mL) for this echinocandin.
Fungal burden versus echinocandin-susceptible strain
SCY-247 was effective in reducing fungal burden, as measured by CFU counts, in both the kidneys and lungs of mice infected with the echinocandin-susceptible C. glabrata strain. A dose-dependent reduction in kidney fungal burden was observed with SCY-247, and CFU counts were significantly lower in mice administered SCY-247 at both the 32 mg/kg and 48 mg/kg dose levels (median values of 4.20 and 2.85 log_10_ CFU/g, respectively) compared to the vehicle control group (6.75 log_10_ CFU/g; P ≤ 0.0005 for both comparisons; Fig. 2A). Fungal burden was also numerically lower in mice administered SCY-247 at 16 mg/kg (4.83 log_10_ CFU/g), although this difference did not reach significance compared to the vehicle control group (P = 0.0510). Treatment with SCY-247 at doses of 32 mg/kg and 48 mg/kg resulted in reductions in fungal burden of >1 log_10_ CFU/g compared to that measured at 24 hours post-inoculation, just prior to the initiation of treatment, indicating fungicidal activity (Table 2). Fungal burden was also significantly lower in mice that received caspofungin (4.47 log_10_ CFU/g; P = 0.0119), with reductions of >1 log_10_ CFU/g compared to that prior to the start of therapy. No reductions in fungal burden were observed with fluconazole (6.12 log_10_ CFU/g). Similar results were also observed in the lungs, where fungal burden was significantly lower in mice that received SCY-247 at 32 mg/kg and 48 mg/kg (median values 2.68 and 2.46 log_10_ CFU/g, respectively) versus vehicle control (4.16 log_10_ CFU/g; P ≤ 0.0183 for both comparisons; Fig. 2B). In contrast, no significant reductions in lung fungal burden were observed in mice treated with SCY-247 at 16 mg/kg, caspofungin, or fluconazole compared to the vehicle control group. Marked reductions in lung fungal burden compared to that measured just prior to the start of therapy (24 hours post-inoculation) were observed in all groups, including the vehicle control, consistent with clearance of Candida from the lungs.
Kidney (A) and lung (B) fungal burden in mice infected with the echinocandin-susceptible Candida glabrata strain at 24 hours post-inoculation, just prior to the start of therapy, and at day 8 in mice treated with vehicle control, SCY-247, caspofungin, or fluconazole by oral gavage for 7 days.
Fungal burden versus echinocandin-resistant strain
SCY-247 was also effective at reducing fungal burden in mice infected with the echinocandin-resistant strain of C. glabrata, which harbored the Fks1p S629P mutation, as dose-dependent reductions in CFU counts were observed in mice infected with this strain. Both the 32 mg/kg and 48 mg/kg doses of SCY-247 resulted in significant reductions in kidney fungal burden (4.33 and 2.38 log_10_ CFU/g, respectively) compared to the vehicle control group (6.27 log_10_ CFU/g; P ≤ 0.0083 for both comparisons; Fig. 3A). Reductions of greater than 1 log_10_ CFU/g were also observed with these two SCY-247 doses compared to that measured prior to the start of therapy, indicating fungicidal activity against the resistant strain (Table 2). No reductions in kidney fungal burden were observed in the SCY-247 16 mg/kg, caspofungin, or fluconazole groups. Similar results were also observed in the lungs of mice infected with the resistant strain, as both the SCY-247 32 mg/kg and 48 mg/kg dose groups had significantly lower CFU counts (0.78 and 0.00 log_10_ CFU/g, respectively) than the vehicle control (4.50 log_10_ CFU/g; P ≤ 0.0031 for each comparison; Fig. 3B). As observed in the kidneys, no reductions in fungal burden were observed in mice treated with a lower dose of SCY-247, caspofungin, or fluconazole. Similar to the echinocandin-susceptible isolate, marked reductions in lung fungal burden compared to that measured just prior to the start of therapy (24 hours post-inoculation) were observed in all groups infected with the echinocandin-resistant strain.
Kidney (A) and lung (B) fungal burden in mice infected with the echinocandin-resistant Candida glabrata strain at 24 hours post-inoculation, just prior to the start of therapy, and on day 8 in mice treated with vehicle control, SCY-247, caspofungin, or fluconazole by oral gavage for 7 days.
SCY-247 plasma and tissue concentrations
SCY-247 trough concentrations were measured in the plasma, kidneys, and lungs of infected mice ~12 hours following the last dose administered on day 7 post-inoculation. SCY-247 concentrations increased in each of these in a dose-dependent fashion (Fig. 4). No differences in achieved concentrations at each dose level were observed between mice infected with the echinocandin-susceptible or echinocandin-resistant strains, although SCY-247 levels were numerically lower in the lungs of mice infected with the resistant strain versus the susceptible strain. The lowest concentrations were observed within the plasma (range of mean plasma concentrations 1.31 to 2.02 μg/mL in the 16 mg/kg group up to 7.62 to 9.63 μg/mL in the 48 mg/kg group). Similar SCY-247 concentrations were observed within the kidneys and lungs at each dose level (range of mean kidney concentrations 38.57 to 530.1 μg/mL; range of mean lung concentrations 9.59 to 355.8 μg/mL), and these were significantly higher than those observed within the plasma (with the exception of the lung concentrations achieved in the 16 mg/kg group in mice infected with the echinocandin-resistant strain). The concentrations achieved within the kidneys and lungs were markedly higher than the SCY-247 MIC against both the susceptible and resistant strains used to establish infection and the MIC_90_ value calculated against all strains tested (MIC_90_, 2 μg/mL).
SCY-247 plasma, kidney, and lung concentrations in mice infected with the echinocandin-susceptible strain (A) or the echinocandin-resistant strain (B) of Candida glabrata. Mice were dosed with SCY-247 orally twice daily for 7 days, and plasma, kidneys, and lungs were collected on day 8, 12 hours after the last dose.
DISCUSSION
SCY-247 is an investigational agent that inhibits glucan synthase, leading to a decrease in (1, 3)-β-d-glucan polymers and a weakening of the fungal cell wall (10, 12, 14). Although its mechanism of action is similar to that of the echinocandins, like ibrexafungerp (formerly SCY-078), SCY-247 is structurally different and thus a member of a separate and relatively new class of antifungals, the triterpenoids. In addition, unlike the echinocandins, SCY-247 is absorbed from the gastrointestinal tract following oral administration. In the current study, SCY-247 demonstrated in vitro activity against C. glabrata isolates that was maintained against the majority of isolates (25 of 29) that were phenotypically resistant or non-susceptible to the echinocandins micafungin and caspofungin. This in vitro activity translated into in vivo efficacy in a neutropenic murine model of disseminated candidiasis against infections caused by both echinocandin-susceptible and echinocandin-resistant strains in which fungicidal activity was observed with the higher doses of SCY-247 that were used. SCY-247 plasma, kidney, and lung tissue concentrations remained elevated, above the MIC values against both isolates tested, approximately 12 hours after the last doses were administered. Within the kidneys and lungs, the SCY-247 concentrations were also above the MIC_90_ value determined against all strains tested.
The results of the current study are consistent with what others have reported for SCY-247. Previous studies have also demonstrated potent in vitro activity for SCY-247 against different Candida species, including C. albicans, C. glabrata, and C. auris, with MIC values similar to those observed for ibrexafungerp (10, 11). Against 65 C. auris strains that included members of clades I through V, SCY-247 demonstrated robust activity, with an MIC_50_ of 0.125 μg/mL for isolates that were FKS wild-type and 1 μg/mL for those harboring FKS1 mutants, for which the MICs for anidulafungin and micafungin were markedly elevated (11). In vitro activity was also observed against the dimorphic fungi Coccidioides immitis and Histoplasma capsulatum, as well as Aspergillus species (10). In vitro activity was also reported against other molds, including Fusarium and Scedosporium species, but similar to that of ibrexafungerp, the potency of SCY-247 was reduced against these fungi compared to that observed for Candida species.
The in vitro activity of SCY-247 against C. albicans also translated into in vivo efficacy in a murine model of disseminated candidiasis. In non-neutropenic mice, treatment with SCY-247 resulted in significant reductions in kidney fungal burden in groups administered doses of 10 mg/kg and 40 mg/kg orally twice daily compared to untreated controls (12). Improvements in survival were also observed, although differences with the untreated control group did not reach statistical significance. Elevated SCY-247 plasma concentrations were also reported after 7 days of therapy. The plasma levels achieved were dose-dependent, and measurable concentrations were noted 36 hours after the last administered dose. The results of this study are consistent with ours in that SCY-247 demonstrated in vivo efficacy against invasive candidiasis, with both reductions in fungal burden and achievable concentrations of this investigational agent being dose-dependent.
Overall, the results of our study demonstrate the potential for SCY-247 in the treatment of invasive C. glabrata infections, including those caused by echinocandin-resistant strains. However, only one echinocandin-resistant strain was used to establish invasive infection. Thus, additional studies may be needed to confirm our findings, including those in which strains with different FKS mutations and higher SCY-247 MICs are used to establish infection. Additional studies are also needed to understand how different FKS mutations, including those not in traditional hotspot regions, may influence SCY-247 activity and whether some cause cross-resistance with ibrexafungerp or the different echinocandins. Finally, while we did measure SCY-247 concentrations at multiple dose levels in different tissues and plasma, we did not include enough dosage groups to conduct a formal pharmacokinetic/pharmacodynamic analysis or demonstrate a clear concentration-response relationship. However, our findings, as well as those reported by others, demonstrate the potential utility of SCY-247 for the treatment of invasive candidiasis.
MATERIALS AND METHODS
Antifungals
For in vitro susceptibility testing, stock solutions of SCY-247 (Scynexis Inc., Jersey City, NJ, USA), fluconazole, caspofungin, and micafungin (Sigma-Aldrich, St. Louis, MO, USA) were prepared in DMSO. Further dilutions were made in DMSO and then in RPMI (0.165 M MOPS, pH 7.0 without bicarbonate). For the in vivo candidiasis model, the acetate salt of SCY-247 (88.7% active moiety SCY-247) was prepared in 0.5% wt/vol methylcellulose in sterile water for injection. Following stirring for 30 minutes, the pH was adjusted to 6.5 using 1 N HCl or 1 N KOH. The preparation was stored protected from light at 2 to 8°C and used within 24 hours of preparation. The clinical intravenous formulations of fluconazole and caspofungin were used for dosing in the in vivo model, and the vehicle control was 0.5% methylcellulose.
Candida glabrata isolates
For in vitro susceptibility testing, C. glabrata clinical strains received by the Fungus Testing Laboratory, UT Health San Antonio, for clinical diagnostic testing were used. Prior to in vitro testing, all strains were subcultured twice on Sabouraud dextrose agar (SDA) for 24 hours at 30°C. For the in vivo model, echinocandin-susceptible (05-761) and resistant strains (DI24-268) were used. The echinocandin-resistant strain harbored a S629P amino acid substitution in hotspot 1 of Fks1p. These strains were subcultured three times on SDA for 48 hours at 37°C. Cells were collected from the third subculture by scraping the surface of the agar plates. The cells were washed three times in sterile saline with 0.1% Tween 20. After the final wash, an aliquot of cells was collected by centrifugation and resuspended in sterile saline, and a hemocytometer was used to adjust the number of cells to the desired starting inoculum. Viability was confirmed by serial dilution of aliquots onto SDA and counting the number of colonies following inoculation at 37°C.
In vitro susceptibility
In vitro susceptibility testing was performed by broth microdilution according to the methods described in the CLSI M27 document (15). The concentration ranges tested were 0.015 to 8 μg/mL for SCY-247, caspofungin, and micafungin, and 0.125 to 64 μg/mL for fluconazole. MICs were read visually after 24 hours of incubation at 35°C as the lowest concentration that resulted in 50% growth inhibition compared to the drug-free control.
Infection model
We utilized our established murine model of C. glabrata invasive candidiasis (16). Briefly, outbred male ICR mice (Envigo, Indianapolis, IN) were housed five per cage and had access to food and water ad libitum. Mice were rendered neutropenic with a single dose of 5-fluorouracil (5 mg/mouse) administered intravenously one day prior to infection. On the day of infection (day 0), mice were infected intravenously with 0.2 mL of C. glabrata with the target number of Candida cells at 1.0 × 10^8^ cells per mouse. Mice were monitored at least twice daily throughout the study to minimize unnecessary pain or distress. One day after inoculation, treatment with vehicle control (methylcellulose by oral gavage twice daily), SCY-247 (16, 32, or 48 mg/kg by oral gavage twice daily), caspofungin (5 mg/kg by intraperitoneal injection once daily), or fluconazole (20 mg/kg by oral gavage once daily) was continued for 7 days. On day 8 post-inoculation, mice were humanely euthanized, and the kidneys and lungs were aseptically removed, weighed, and homogenized. Serial dilutions of the homogenates were plated onto SDA, and after 24 hours of incubation, the number of CFUs per gram of tissue was calculated.
Measurement of SCY-247 plasma and tissue concentration
SCY-247 plasma, kidney, and lung concentrations were measured in neutropenic, infected mice on day 8, approximately 12 hours following the last administered dose on day 7. Tissue and plasma samples were assayed by LC-MS/MS. All methods met a priori method performance acceptance criteria for specificity and inter- and intra-assay performance of <15% coefficient of variation and <±15% accuracy for calibration standards and quality control samples. The calibration range was 5 to 5,000 ng/mL (eight calibration levels). Samples with concentrations beyond this range were diluted. The determination of SCY-247 concentrations in tissues was performed using aliquots of the homogenates prepared for assessment of fungal burden. Mouse plasma (50 µL) or tissue homogenates for standards, quality control, or study samples (50 µL) were treated with 50 µL of internal standard solution (250 ng/mL of SCY-247-d6 in 10:90 dimethyl sulfoxide:acetonitrile) and vortex-mixed for approximately 20 seconds. Sample proteins were precipitated with 1,000 µL of acetonitrile and vortex-mixed for approximately 1 minute. All samples were centrifuged at approximately 14,000 rpm for approximately 5 minutes, whereupon 20 µL were transferred to autosampler vials containing 200 µL of 0.1% (vol/vol) formic acid in 50:50 acetonitrile/water. Analysis was performed employing a Shimadzu (Columbia, MD, USA) HPLC system comprising a SIL-30AC autosampler and an LC-20AD pump and an Applied Biosystems (Foster City, CA, USA) API-5500 QTRAP mass spectrometer operated as a triple quadrupole instrument with a turbo-ion electrospray source in positive ionization mode.
Data analysis
Descriptive statistics were used for the in vitro susceptibility results, including MIC ranges, concentrations that inhibited 50% and 90% of the isolates tested (MIC_50_ and MIC_90_, respectively), geometric mean (GM) MICs, and modal MICs. Differences in SCY-247 plasma and tissue concentrations were assessed for significance by ANOVA with Dunnett’s post-test for multiple comparisons. Differences in fungal burden (CFU/g) were assessed for significance by the Kruskal-Wallis test with Dunn’s test for multiple comparisons. A P-value of <0.05 was considered statistically significant for all comparisons.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. 2004. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 39:309–317. doi:10.1086/42194615306996 · doi ↗ · pubmed ↗
- 2Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A, Kallen A, Limbago B, Fridkin S, National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. 2013. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National healthcare safety network at the centers for disease control and prevention, 2009-2010. Infect Control Hosp Epidemiol 34:1–14. doi:10.1086/66877023221186 · doi ↗ · pubmed ↗
- 3Yapar N. 2014. Epidemiology and risk factors for invasive candidiasis. Ther Clin Risk Manag 10:95–105. doi:10.2147/TCRM.S 4016024611015 PMC 3928396 · doi ↗ · pubmed ↗
- 4Pappas PG, Rex JH, Lee J, Hamill RJ, Larsen RA, Powderly W, Kauffman CA, Hyslop N, Mangino JE, Chapman S, Horowitz HW, Edwards JE, Dismukes WE, NIAID Mycoses Study Group. 2003. A prospective observational study of candidemia: epidemiology, therapy, and influences on mortality in hospitalized adult and pediatric patients. Clin Infect Dis 37:634–643. doi:10.1086/37690612942393 · doi ↗ · pubmed ↗
- 5Denning DW. 2024. Global incidence and mortality of severe fungal disease. Lancet Infect Dis 24:e 428–e 438. doi:10.1016/S 1473-3099(23)00692-838224705 · doi ↗ · pubmed ↗
- 6WHO. 2022. WHO fungal priority pathogens list to guide research, development and public health action. World Health Organization. Available from: https://www.who.int/publications/i/item/9789240060241
- 7Cornely OA, Sprute R, Bassetti M, Chen SC-A, Groll AH, Kurzai O, Lass-Flörl C, Ostrosky-Zeichner L, Rautemaa-Richardson R, Revathi G, et al.. 2025. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis 25:e 280–e 293. doi:10.1016/S 1473-3099(24)00749-739956121 · doi ↗ · pubmed ↗
- 8Pham CD, Iqbal N, Bolden CB, Kuykendall RJ, Harrison LH, Farley MM, Schaffner W, Beldavs ZG, Chiller TM, Park BJ, Cleveland AA, Lockhart SR. 2014. Role of FKS mutations in Candida glabrata: MIC values, echinocandin resistance, and multidrug resistance. Antimicrob Agents Chemother 58:4690–4696. doi:10.1128/AAC.03255-1424890592 PMC 4136002 · doi ↗ · pubmed ↗