Association between dietary zinc intake and herpes simplex virus seropositivity in U.S. adults: a cross-sectional study
Chunhua Liu, Yingguo Liu, Jingjing Liu, Zhaoyong Lv, Yanan Qin, Mengpeng Li

TL;DR
This study found that moderate dietary zinc intake is linked to lower chances of having herpes simplex virus in U.S. adults.
Contribution
The study reveals a U-shaped relationship between dietary zinc intake and herpes simplex virus seropositivity, suggesting moderate zinc intake is protective.
Findings
Higher dietary zinc intake was associated with reduced odds of HSV-1 and HSV-2 seropositivity compared to the lowest intake group.
A U-shaped relationship was observed, indicating that moderate zinc intake is most protective against herpes simplex virus.
Statistical methods confirmed the protective effect of moderate zinc intake after adjusting for covariates.
Abstract
Although recent research has demonstrated an association between serum zinc deficiency and susceptibility to various viral infections, the relationship between dietary zinc intake and herpes simplex virus (HSV) seropositivity remains unclear. The National Health and Nutrition Examination Survey (NHANES) (2007–2016) provides data on HSV-1 and HSV-2 status and dietary zinc intake. The associations between dietary zinc and HSV-1 and HSV-2 were evaluated via various statistical methods, including multivariate logistic regression, restricted cubic spline analysis, and subgroup analysis. In total, 6,483 individuals were enrolled, with 58.9% (3,817/6,483) testing positive for HSV-1 and 19.3% (1,253/6,483) testing positive for HSV-2. After adjusting for all covariates in the multivariate logistic regression, compared with the lowest zinc intake group (Q1: <7.51 mg/day), the adjusted odds…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
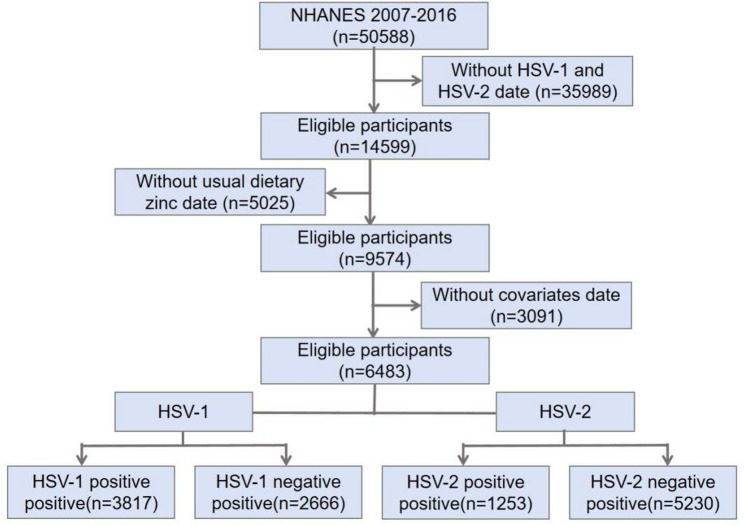 Figure 1
Figure 1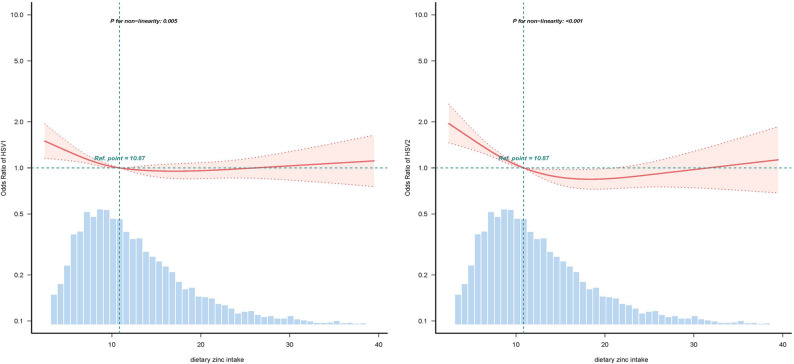 Figure 2
Figure 2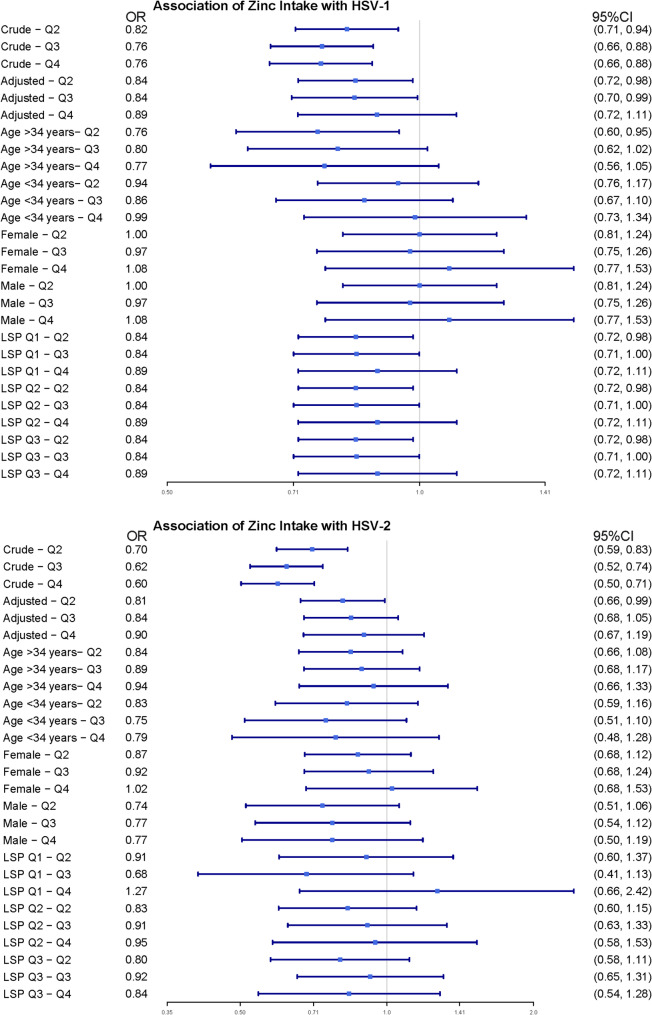 Figure 3
Figure 3- —https://doi.org/10.13039/501100007129Natural Science Foundation of Shandong Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrace Elements in Health · Herpesvirus Infections and Treatments · Viral Infections and Immunology Research
Introduction
Herpes simplex virus (HSV), a double-stranded DNA pathogen with a global prevalence, manifests as two primary serotypes: HSV-1 and HSV-2. HSV-1 spreads predominantly through oral‒to‒oral contact, infecting more than 67% of individuals under 50 years of age, whereas HSV-2 is transmitted primarily via sexual routes, affecting approximately 17% of the 15–49 age cohort [1]. Following initial mucosal invasion, the virus establishes lifelong latency in the sensory ganglia, characterized by periodic reactivation [2]. Although most outbreaks involve self-limiting mucocutaneous lesions, severe complications may arise, including viral encephalitis, herpetic keratitis (a leading cause of infectious blindness), and increased susceptibility to human immunodeficiency virus (HIV) infection [3–5]. The absence of curative vaccines or virucidal agents combined with asymptomatic viral shedding that facilitates transmission underscores the urgent need to investigate modifiable risk factors, such as dietary patterns, in HSV pathogenesis and epidemiology [6].
Zinc is a crucial trace element for human growth, development, and maintenance of immune function [7]. Its immunomodulatory properties extend to both innate and adaptive immunity, wherein it participates in lymphocyte differentiation, cytokine production, and phagocytic activity [8–10]. Zinc status serves as a critical determinant of antiviral immunity, with zinc-deficient populations demonstrating heightened susceptibility to viral infections, including HIV and hepatitis C virus [11, 12]. Moreover, emerging evidence has revealed the direct inhibitory effects of zinc on HSV replication through mechanisms involving viral DNA polymerase interference and capsid destabilization [13–15]. Although the interplay between serum zinc status and viral pathogenesis has been extensively investigated, the specific relationship between dietary zinc intake and HSV seropositivity remains unexplored.
Therefore, further research is necessary to understand the association between dietary zinc consumption and HSV seropositivity. Data from the National Health and Nutrition Examination Survey (NHANES) were drawn upon in the present study.
Materials and methods
Study population
The NHANES, organized by the United States Centers for Disease Control and Prevention (CDC), serves as a critical surveillance system monitoring population health indicators among noninstitutionalized U.S. residents. In accordance with the approval of the National Center for Health Statistics Research Ethics Committee, the protocol mandates documented consent from all participants prior to enrollment. For our study that analyzed existing deidentified records, no supplementary ethical clearance or informed consent was necessary according to federal regulations. Publicly accessible datasets spanning 2007–2016 (5 biennial cycles) were retrieved from the official NHANES repository (https://www.cdc.gov/nchs/nhanes). We utilized data from this five cycles because they represent the most recent consecutive cycles (relative to the present) that contain concurrent laboratory data for both HSV-1/HSV-2 and zinc intake data. Our analytical cohort excluded individuals whose nutritional zinc records were incomplete, whose serological data for herpes simplex virus were unavailable, or whose covariate information was missing. The final sample included complete case data from eligible participants across the designated survey periods.
Dietary zinc intake
Participants in the NHANES dietary survey reported their food and beverage consumption over a 24-hour period, with data collected between 2006 and 2016 via the automated multiple pass method (AMPM) to ensure precise nutrient calculations on the basis of reported intake. The detailed methodologies are described in the NHANES Dietary Interviewer Procedure Manual. Dietary zinc intake was calculated from the first 24-h recall only (DR1TZINC). Zinc intake was analyzed as a continuous variable and categorized into quartiles (Q1–Q4). To validate these results, individuals whose reported 24-hour dietary intake aligned with their habitual consumption patterns were prioritized. Specifically, participants were screened via the variable DR1_300, which corresponds to the following question: “Was the amount of food that {you/NAME} ate yesterday much more than usual, usual, or much less than usual?” Only those who responded “usual” were included. Additionally, the zinc intake categories for Q1 were as follows: <7.51 mg/day, Q2: 7.51–10.87 mg/day, Q3: 10.87–15.63 mg/day, and Q4: >15.63 mg/day.
HSV antibody measurement
To identify HSV-1 and HSV-2 infections, blood samples obtained through venipentesis were analyzed via a solid-phase enzyme immunopoint assay. The publicly released NHANES data file includes HSV-1 data for the 14–49 age group and HSV-2 data for the 18–49 age group. In our study, these two variables were considered independent factors; that is, HSV-1 and HSV-2 infections were defined as positive for their respective viral antibodies, and negative infections were defined as negative for their respective viral antibodies. Records classified as “inconclusive” were excluded from our analysis.
Covariates
We evaluated several potential covariates on the basis of previous literature [16–18], including age; sex; race and ethnicity; body mass index (BMI); marital status; smoking status; excessive alcohol consumption; number of lifetime sexual partners; acquisition time; and caloric, protein, carbohydrate, sugar, fiber, and fat intake. The categories for race and ethnicity included Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, and other races. Marital status was categorized as living alone or being married/living with a partner. BMI was calculated via a standardized approach considering both weight and height. Smoking was defined as having smoked at least 100 cigarettes. Excessive alcohol consumption was defined as periods of drinking 4 or more drinks per day for women and 5 or more for men. Sexual partners were defined as the total number of same-sex or opposite-sex partners with whom any sexual activity occurred. A dietary recall interview was conducted prior to the Mobile Examination Center (MEC) interview to collect participants’ nutritional data over a 24-hour period, including the consumption of calories, protein, carbohydrates, sugar, fiber, and fat.
Statistical analysis
This was a secondary analysis based on publicly available NHANES datasets. Given the complex, multistage probability sampling design of NHANES, all analyses incorporated sampling weights, strata, and primary sampling units (PSUs) to produce nationally representative estimates and valid standard errors, following the analytical guidelines provided by the National Center for Health Statistics (NCHS). Data from five NHANES cycles (2007–2016) were pooled following the NCHS analytic guidelines [19, 20]. Sample weight (WTDRD1), Strata (SDMVSTRA) and PSU (SDMVPSU) were included in every SURVEY procedure (svyset in R) to obtain design-consistent point estimates and Taylor-linearization standard errors.
For continuous variables with a normal distribution, we reported the mean and standard deviation (SD). For nonnormally distributed variables, we used medians and interquartile ranges (IQRs). Categorical variables are presented as percentages. To compare differences between groups, we used one-way analysis of variance (ANOVA) for normally distributed data, the Mann-Whitney test for nonnormally distributed data, and the chi‒square test for categorical data. Logistic regression analysis was used to explore the association between dietary zinc intake and HSV seropositivity. Initially, we used univariate logistic regression to identify factors associated with HSV-1 and HSV-2 seropositivity. After controlling for potential confounding factors, we used a multivariate logistic regression model to clarify the relationships between dietary zinc intake and HSV-1 and HSV-2 seropositivity. Model I was adjusted for age, sex, and race. In Model II, we further adjusted for variables such as marital status, smoking status, excessive alcohol consumption, number of lifetime sexual partners, and acquisition time. In Model III, we included all the covariates.
Furthermore, restricted cubic spline (RCS) regression analysis was used to assess whether there was a nonlinear relationship between dietary zinc intake and HSV-1 and HSV-2 seropositivity. RCS models were fitted with the survey-weighted logistic procedure (survey::svyglm in R) using the 10-year weights described above. Four knots were placed at the 5th, 35th, 65th and 95th weighted percentiles of zinc intake. Finally, a subgroup analysis was conducted to compare the interaction between dietary zinc intake and HSV-1 and HSV-2 seropositivity across different subgroups was used to evaluate the robustness of the study results.
All statistical analyses accounted for the NHANES complex survey design and were conducted using R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
Results
Study population
A total of 50,588 participants were included in the NHANES conducted between 2007 and 2016. After individuals with missing HSV-1 and HSV-2 data were excluded, 14,599 individuals were included in the study. After selecting those for whom data regarding dietary zinc were available, 9,574 people remained. After further screening for individuals who could recollect the food they consumed the previous day and excluding individuals with missing covariates, 6,483 people remained. The final population included 2,666 HSV-1-negative and 3,817 HSV-1-positive individuals. For HSV-2, there were 5,230 HSV-2-negative individuals and 1,253 HSV-2-positive individuals. The mean age was 34.52 ± 8.64 years, and 61.4% were male. The mean daily zinc consumption amount was 12.57 ± 8.23 mg (10.12 ± 5.42 mg for women and 14.87 ± 9.64 mg for men) (Fig. 1).
Fig. 1. The study’s flow diagram. HSV, herpes simplex virus; NHANES, National Health and Nutrition Examination Survey
Baseline characteristics
Table 1 summarizes the baseline demographic characteristics stratified by herpes simplex virus (HSV) infection status. Seropositivity for HSV (types 1 and 2) was associated with advanced age, elevated BMI, lower caloric intake, diminished protein and fat consumption, higher binge drinking frequency, increased lifetime sexual partners, female predominance, increased smoking prevalence, reduced zinc intake, and the highest disease incidence during the 2007–2008 survey cycle. Notably, HSV-1 seropositivity was linked to higher cohabitation rates, with the highest seroprevalence observed in Mexican American individuals. In contrast, HSV-2 seropositivity was correlated with a lower prevalence of cohabitation, the highest incidence among non-Hispanic Black populations, reduced carbohydrate and sugar intake, and an elevated frequency of sexual partners annually.
Table 1. Baseline characteristics and demographic characteristics of the participantsVariablesHSV-1 +(n = 3817)HSV-1 -(n = 2666) P HSV-2 +(n = 1253)HSV-2 -(n = 5230) p Age37.0 (29.0, 43.0)31.0 (25.0, 39.0)< 0.00139.0 (32.0, 45.0)33.0 (26.0, 41.0)< 0.001Gender< 0.001< 0.001Male1874 (49.1%)1461 (54.8%)457 (36.5%)2878 (55.0%)Femlale1943 (50.9%)1205 (45.2%)796 (63.5%)2352 (45.0%)Race and ethnicity< 0.001< 0.001Mexican American791 (20.7%)214 (8.0%)140 (11.2%)865 (16.5%)Other Hispanic436 (11.4%)157 (5.9%)136 (10.9%)457 (8.7%)Non-Hispanic White1528 (40.0%)1561 (58.6%)438 (35.0%)2651 (50.7%)Non-Hispanic Black659 (17.3%)414 (15.5%)464 (37.0%)609 (11.6%)Other/Multi-Racial403 (10.6%)320 (12.0%)75 (6.0%)648 (12.4%)Marital status< 0.001< 0.001Married or living with a partner2432 (63.7%)1521 (57.1%)685 (54.7%)3268 (62.5%)Living alone1385 (36.3%)1145 (42.9%)568 (45.3%)1962 (37.5%)BMI< 0.001< 0.001Low(<18.5)2669 (69.9%)1659 (62.2%)940 (75.0%)3388 (64.8%)Median(18.5–25)57 (1.5%)44 (1.7%)17 (1.4%)84 (1.6%)High(> 25)1091 (28.6%)963 (36.1%)296 (23.6%)1758 (33.6%)Smoking status< 0.001< 0.001Yes1727 (45.2%)1022 (38.3%)651 (52.0%)2098 (40.1%)No2090 (54.8%)1644 (61.7%)602 (48.0%)3132 (59.9%)Number of lifetime sexual partners< 0.001< 0.0010–41305 (34.2%)1045 (39.2%)233 (18.6%)2117 (40.5%)4–101272 (33.3%)815 (30.6%)467 (37.3%)1620 (31.0%)>101240 (32.5%)806 (30.2%)553 (44.1%)1493 (28.5%)Excessive alcohol consumption< 0.001< 0.001Yes633 (16.6%)333 (12.5%)231 (18.4%)735 (14.1%)No3184 (83.4%)2333 (87.5%)1022 (81.6%)4495 (85.9%)Carbohydrate consumption(gm/day)255.8 (188.2, 344.4)266.2 (197.7, 358.9)< 0.001252.7 (180.5, 351.0)262.1 (194.9, 350.4)0.016Fiber consumption(gm/day)14.9 (9.6, 22.2)15.3 (10.4, 22.4)0.00913.2 (8.7, 19.9)15.5 (10.2, 22.9)< 0.001Calorie consumption(kcal/day)2122.0 (1600.0, 2849.0)2268.5 (1699.0, 2955.8)< 0.0012094.0 (1527.0, 2808.0)2200.5 (1673.0, 2915.8)< 0.001Protein consumption(gm/day)80.9 (58.4, 111.7)84.9 (62.5, 113.9)< 0.00176.3 (55.0, 104.9)84.9 (61.4, 114.5)< 0.001Sugar consumption(gm/day)109.3 (67.6, 162.0)109.1 (69.8, 163.6)0.409112.1 (70.0, 172.5)108.3 (68.4, 159.6)0.027Fat consumption(gm/day)77.4 (53.0, 109.5)83.6 (58.6, 115.9)< 0.00178.0 (52.3, 110.3)80.4 (56.6, 112.2)0.008Zinc intake (mg/day)10.6 (7.2, 15.4)11.2 (7.8, 16.0)< 0.0019.7 (6.7, 14.6)11.1 (7.7, 15.9)< 0.001Zinc intake category< 0.001< 0.001Q^a^1(≤ 7.505)1026 (26.9%)595 (22.3%)403 (32.2%)1218 (23.3%)Q^a^2(7.505–10.87)953 (25.0%)675 (25.3%)307 (24.5%)1321 (25.3%)Q^a^3(10.87–15.63)919 (24.1%)697 (26.1%)276 (22.0%)1340 (25.6%)Q^a^4(≥15.63)919 (24.1%)699 (26.2%)267 (21.3%)1351 (25.8%)Source= 0.003< 0.0012007–2008775 (20.3%)450 (16.9%)275 (21.9%)950 (18.2%)2009–2010908 (23.8%)607 (22.8%)315 (25.1%)1200 (22.9%)2011–2012717 (18.8%)525 (19.7%)251 (20.0%)991 (18.9%)2013–2014709 (18.6%)545 (20.4%)216 (17.2%)1038 (19.8%)2015–2016708 (18.5%)539 (20.2%)196 (15.6%)1051 (20.1%)Baseline characteristics categorized by dietary zinc intake. ^a^Quartiles based on dietary zinc consumption
Relationship between dietary zinc intake and HSV infection
Univariate analysis revealed that both HSV-1 and HSV-2 were associated with age; sex; race; marital status; smoking status; excessive alcohol consumption; lifetime number of sexual partners; year of data collection; and calorie intake, protein intake, dietary fiber intake, zinc intake, and zinc intake quartile groups. Additionally, HSV-1 was specifically associated with carbohydrate intake, whereas HSV-2 was associated with sugar intake (Table 2).
Table 2. Associations between covariates and asthma riskVariableHSV-1-OR^a^(95%CI^b^)p ValueHSV-2-OR^a^(95%CI^b^)p ValueZinc intake categoryQ1(≤ 7.505)ReferenceReferenceQ2(7.505–10.87)0.82 (0.71–0.94)0.0050.70 (0.60–0.83)< 0.001Q3(10.87–15.63)0.76 (0.66–0.88)< 0.0010.62 (0.53–0.74)< 0.001Q4(≥15.63)0.76 (0.66–0.88)< 0.0010.60 (0.50–0.71)< 0.001Age1.05 (1.05–1.05)< 0.0011.06 (1.05–1.08)< 0.001GenderMaleReferenceReferenceFemlale1.25 (1.14–1.39)< 0.0012.13 (1.89–2.44)< 0.001Race and ethnicityMexican AmericanReferenceReferenceOther Hispanic0.75 (0.60–0.95)0.0181.85 (1.41–2.38)< 0.001Non-Hispanic White0.26 (0.22–0.31)< 0.0011.02 (0.83–1.25)0.844Non-Hispanic Black0.43 (0.35–0.52)< 0.0014.76 (3.85–5.90)< 0.001Other/Multi-Racial0.34 (0.27–0.42)< 0.0010.71 (0.53–0.96)0.028Marital statusMarried or living with a partnerReferenceReferenceLiving alone0.76 (0.68–0.84)< 0.0010.72 (0.64–0.82)< 0.001BMILow(<18.5)ReferenceReferenceMedian(18.5–25)0.88 (0.58–1.30)0.5140.83 (0.50–1.47)0.501High(> 25)1.24 (0.83–1.86)0.2861.37 (0.83–2.26)0.24Excessive alcohol consumption, nYesReferenceReferenceNo0.72 (0.62–0.83)< 0.0010.72 (0.61–0.85)< 0.001Smoking statusNoReferenceReferenceYes0.75 (0.68–0.83)< 0.0010.62 (0.55–0.70)< 0.001Source2007–2008ReferenceReference2009–20100.87 (0.74–1.01)0.0750.91 (0.76–1.09)0.2942011–20120.79 (0.69–0.93)0.0050.88 (0.72–1.06)0.1752013–20140.76 (0.64–0.89)< 0.0010.72 (0.59–0.88)0.0012015–20160.76 (0.65–0.89)0.0010.65 (0.53–0.79)< 0.001Number of lifetime sexual partners0–4ReferenceReference4–101.25 (1.11–1.41)< 0.0012.63 (2.22–3.12)< 0.001>101.23 (1.09–1.39)< 0.0013.33 (2.86–3.92)< 0.001Calorie consumption(kcal/day)1.00 (1.00–1.00)< 0.0011.00 (1.00–1.00)0.019Protein consumption(gm/day)1.00 (1.00–1.00)0.0091.00 (1.00-1.01)< 0.001Carbohydrate consumption(gm/day)1.00 (1.00–1.00)0.0071.00 (1.00–1.00)0.184Sugar consumption(gm/day)1.00 (1.00–1.00)0.1951.00 (1.00–1.00)0.003Fiber consumption(gm/day)0.99 (0.99–0.99)0.0180.98 (0.97–0.98)< 0.001Fat consumption(gm/day)1.00 (1.00–1.00)< 0.0011.00 (1.00–1.00)0.109Zinc intake (mg/day)0.99 (0.99–0.99)0.0230.98 (0.97–0.99)< 0.001^a^Odds ratio. ^b^Confidence interval
In the multivariable-adjusted model evaluating the associations between zinc intake quartiles (low, low-moderate, moderate-high, and high intake) and HSV-1/HSV-2 infections, the following results were observed. Compared with the low-zinc intake group, the low-moderate intake group presented a reduced risk of HSV-1 infection, with an adjusted odds ratio (OR) of 0.84 (95% confidence interval [CI]: 0.70–0.99, p = 0.028), and a statistically significant reduction in HSV-2 infection risk (OR = 0.81, 95% CI: 0.66–0.99, p = 0.039). Moderate–high zinc intake was associated with a decreased risk of HSV-1 infection (OR = 0.84, 95% CI: 0.70–0.99, p = 0.042), but no statistically significant reduction in HSV-2 infection risk was observed (OR = 0.84, 95% CI: 0.68–1.05, p = 0.136). High zinc intake did not significantly reduce the risk of HSV-1 or HSV-2 infection (p > 0.05) (Table 3).
Table 3. Associations between dietary zinc intake and HSVQuartileHSV-1 OR^a^(95%CI^b^)No.n(%)Crudep ValueModel 1p ValueModel 2p ValueModel 3p ValueZincintake(mg/day)Q^c^1(≤ 7.505)16211026(63.3%)1(Ref)1(Ref)1(Ref)1(Ref)Q^c^2(7.505–10.87)1628953(58.5%)0.82(0.71–0.94)0.0050.8(0.69–0.93)0.0030.81(0.69–0.94)0.0060.84(0.72–0.98)0.028Q^c^3(10.87–15.63)1616919(56.9%)0.76(0.66–0.88)<0.0010.78(0.67–0.91)0.0020.79(0.67–0.92)0.0020.84(0.70–0.99)0.042Q^c^4(≥15.63)1618919(56.8%)0.76(0.66–0.88)<0.0010.83(0.71–0.97)0.0180.81(0.69–0.95)0.0090.89(0.72–1.11)0.292HSV-2 OR^a^(95%CI^b^)Zincintake(mg/day)Q^c^1(≤ 7.14)1621403(24.9%)1(Ref)1(Ref)1(Ref)1(Ref)Q^c^2(7.14–10.53)1628307(18.9%)0.70(0.59–0.83)<0.0010.83(0.69–0.99)0.040.80(0.66–0.97)0.0210.81(0.66–0.99)0.039Q^c^3(10.53–15.23)1616276(17.1%)0.62(0.51–0.74)<0.0010.86(0.71–1.04)0.130.84(0.69–1.02)0.0770.84(0.68–1.05)0.136Q^c^4(≥15.23)1618267(16.5%)0.60(0.50–0.71)<0.0010.96(0.79–1.71)0.690.88(0.72–1.08)0.2370.90(0.67–1.19)0.454Model 1 was adjusted for age, sex, race and ethnicity; Model 2 was adjusted for Model 1 + smoking status, excessive alcohol consumption, sex partner, BMI, marital status, and source; Model 3 was adjusted for Model 2 + caloric consumption, protein consumption, carbohydrate consumption, sugar consumption, fiber consumption, and fat consumption. ^a^Odds ratio. ^b^Confidence interval. ^c^Quartiles based on dietary zinc consumption
These results suggest that low-to-moderate zinc intake may confer a protective effect against both HSV-1 and HSV-2 infections; however, this effect diminishes or becomes insignificant at higher intake levels. Furthermore, restricted cubic spline (RCS) analysis indicated consistent U-shaped trends in the relationships between zinc intake and HSV-1 (p for nonlinearity = 0.005) and HSV-2 (p for nonlinearity < 0.01), supporting a nonlinear dose‒response pattern (Fig. 2).
Fig. 2. Association between dietary zinc intake and the dietary zinc intake odds ratio (HSV-1 on the left; HSV‐2 on the right). The solid and dashed lines represent the predicted values and 95% confidence intervals, respectively. They were adjusted for age, sex, race and ethnicity, smoking status, excessive alcohol consumption, sex partner, BMI, marital status, source, calorie consumption, protein consumption, carbohydrate consumption, sugar consumption, fiber consumption, and fat consumption. Only 99% of the data are shown
Stratified analyses based on additional variables and sensitivity analysis
We performed stratified analyses across multiple subgroups to assess potential variations in the association between dietary zinc intake and HSV-1/HSV-2 seropositivity. Stratification according to sex, age and the number of sexual partners revealed no additional interactions (Fig. 3). We tested the sensitivity of the model using multiple imputation, and the results showed that both HSV-1 and HSV-2 were consistent with the trends in the original model. The results are shown in Table 4.
Fig. 3. Forest plot of multivariable logistics analysis between dietary zinc intake and HSV-1 or HSV-2. Except for the stratification component itself, each stratification factor was adjusted for age, sex, race and ethnicity, smoking status, excessive alcohol consumption, sex partner, BMI, marital status, source, calorie consumption, protein consumption, carbohydrate consumption, sugar consumption, fiber consumption, fat consumption
Table 4. Estimated results after multiple imputationZincintake(mg/day)HSV-1HSV-2estimate p estimate p Q^a^1(≤ 7.14)referenceQ^a^2(7.14–10.53)-0.1760.028-0.2080.039Q^a^3(10.53–15.23)-0.1790.042-0.1690.136Q^a^4(≥15.23)-0.1170.292-0.1080.454^a^Quartiles based on dietary zinc consumption
Discussion
In this cross-sectional analysis, dietary zinc intake exhibited a U-shaped statistical relationship with HSV-1/HSV-2 seroprevalence: participants in the lowest and highest intake quintiles had higher weighted seroprevalence than those in the middle quintiles. Stratified and sensitivity analyses yielded a similar pattern.
As an essential trace element in humans, zinc plays a critical role in immune regulation. Its association with HSV infection has been demonstrated in multiple studies [21–23]. In vitro experiments showed that zinc lactate inactivates more than 97% of HSV-1/2 clinical isolates and disrupts viral replication by inhibiting viral protein synthesis and potentially interfering with DNA replication [24]. Clinical trials have reported that systemic zinc supplementation (e.g., 22.5–50 mg zinc sulfate daily) significantly reduces the severity and recurrence of herpes labialis and genital herpes [25, 26].Conversely, zinc deficiency has been associated with prolonged lesion duration and impaired antiviral responses [27]. Topical zinc formulations (e.g., zinc oxide/glycine cream or 4% zinc sulfate solution) also have potential for shortening lesion duration, reducing recurrence rates (≤ 6% vs. 80% in controls), and alleviating symptoms, with no significant side effects [28, 29]. Zinc oxide nanoparticles were found to directly antagonize HSV-1 infection by suppressing viral genomic replication [30].Collectively, these findings confirm zinc’s capacity to modulate antiviral defense mechanisms against HSV.
Interestingly, the non-linear pattern observed in our study may reflect zinc’s dual immunomodulatory nature. Zinc deficiency impairs the function of innate and adaptive immune cells, such as macrophages, neutrophils, and T lymphocytes, increasing susceptibility to viral infections. However, excessive zinc intake can lead to immune dysregulation, partly through inducing copper deficiency, oxidative stress, and altered cytokine signaling [31, 32]. Similar U-shaped relationships have been proposed for other viral infections, where both zinc deficiency and excess compromise immune balance and antiviral defense [33]. However, direct evidence across different viral infections remains limited, warranting further investigation.
From a public health perspective, our results underscore the importance of balanced micronutrient intake rather than indiscriminate supplementation. Given the widespread use of zinc supplements, understanding the threshold beyond which zinc loses its protective effect is critical for refining dietary guidelines and preventing potential adverse outcomes. Future mechanistic studies should explore how zinc homeostasis interacts with specific immune pathways involved in HSV latency and reactivation.
These findings collectively confirm that zinc can directly inhibit the replication of HSV. However, excessive zinc intake also poses risks. Long-term high-dose zinc intake may lead to copper deficiency-related symptoms, including impaired immune function, reduced high-density lipoprotein levels, and elevated low-density lipoprotein levels, and neurological symptoms [34, 35]. Consequently, the protective effects of zinc against HSV require further large-scale experimental validation to establish optimal intake thresholds.
Strengths and limitations
Our study has several strengths. First, we utilized data from multiple NHANES cycles, which substantially increased the sample size and enhanced the statistical power and generalizability of our findings. Another notable advantage lies in our focus on the continuity of dietary intake. By comparing foods consumed on a daily basis with usual intake patterns, we ensured consistency in assessing zinc consumption, making the results more reflective of real-world scenarios. In addition, we applied rigorous statistical approaches, including multivariate logistic regression, stratified analysis, and nonlinear modeling, to comprehensively explore the relationship between dietary zinc intake and HSV infection. The use of survey weights and consideration of NHANES’complex sampling design further strengthened the representativeness of our results at the population level.
However, several limitations should be acknowledged. First, this study was based on a cross-sectional design, which precludes causal inference. The observed association may also reflect reverse causation, where preexisting HSV infection could influence dietary behaviors or zinc metabolism. Second, although survey weights were applied to account for the complex NHANES design, this approach may reduce statistical precision, particularly in nonlinear spline modeling. Small sample sizes at extreme zinc intake levels may also lead to instability of the curve estimates. Third, despite extensive covariate adjustment, residual confounding cannot be entirely excluded. Furthermore, the reliance on self-reported 24-hour dietary recall data is subject to recall bias and day-to-day variability, which may affect the accuracy of zinc intake assessment. Lastly, the timing of initial HSV infection could not be determined, which may introduce temporal bias.
Future research should prioritize large-scale prospective cohort studies and multicenter randomized controlled trials to establish causal relationships and define optimal zinc intake thresholds for viral infection prevention.
Conclusion
Our analysis revealed a U-shaped association between zinc intake and HSV-1/HSV-2 seropositivity. Although the dual antiviral and immunomodulatory properties of zinc are mechanistically plausible, causality requires confirmation in longitudinal cohorts and randomized controlled trials. If validated, zinc supplementation may emerge as a cost-effective adjunct strategy for HSV prevention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sanna A, Firinu D, Zavattari P, Valera P. Zinc status and autoimmunity: a systematic review and meta-analysis. Nutrients. 2018;10(1).10.3390/nu 10010068 PMC 579329629324654 · doi ↗ · pubmed ↗
- 2Chang JY, Balch C, Puccio J, Oh HS. A narrative review of alternative symptomatic treatments for herpes simplex virus. Viruses. 2023;15(6).10.3390/v 15061314 PMC 1030128437376614 · doi ↗ · pubmed ↗
- 3Abou Aitah K, Allayh AK, Wojnarowicz J, Shaker YM, Swiderska-Sroda A, Lojkowski W. Nanoformulation composed of ellagic acid and functionalized zinc oxide nanoparticles inactivates DNA and RNA viruses. Pharmaceutics. 2021;13(12).10.3390/pharmaceutics 13122174 PMC 870654734959455 · doi ↗ · pubmed ↗
- 4Curtin LR, Mohadjer LK, Dohrmann SM, Kruszon-Moran D, Mirel LB, Carroll MD, Hirsch R, Burt VL, Johnson CL. National Health and Nutrition Examination Survey: sample design, 2007–2010. Vital Health Stat 2. 2013;2(160):1–23.25090039 · pubmed ↗
- 5Schoofs H, Schmit J, Rink L. Zinc toxicity: understanding the limits. Molecules. 2024;29(13).10.3390/molecules 29133130 PMC 1124327938999082 · doi ↗ · pubmed ↗