Ultrasound-Guided Superficial Temporal Artery Cannulation for Proximal Arterial Pressure Monitoring During Coarctation Repair With an Aberrant Right Subclavian Artery in a Low-Birth-Weight Neonate
Masahiro Wakimoto, Motoi Kumagai, Kenji Suzuki

TL;DR
A low-birth-weight neonate with complex heart defects had successful cerebral perfusion monitoring via ultrasound-guided superficial temporal artery cannulation during surgery.
Contribution
Demonstrates a novel use of ultrasound-guided superficial temporal artery cannulation for cerebral perfusion monitoring in a complex neonatal cardiac surgery.
Findings
Ultrasound-guided cannulation of the superficial temporal artery was successfully used for real-time cerebral perfusion monitoring.
The technique provided stable arterial waveforms during aortic cross-clamping in a low-birth-weight neonate.
This approach proved effective when conventional arterial monitoring sites were unreliable due to complex anatomy.
Abstract
Coarctation of the aorta (CoA) complex with an aberrant right subclavian artery (ARSA) poses a significant challenge for intraoperative cerebral perfusion assessment because arterial pressure from both the upper and lower extremities becomes unreliable during aortic arch reconstruction. We report a 14-day-old male neonate weighing 1.819 kg with CoA complex, including patent ductus arteriosus (PDA), right-ventricle-type single ventricle, double-outlet right ventricle, single atrium, total anomalous pulmonary venous return (type IIa), mitral atresia, and ARSA, who underwent left subclavian artery flap aortoplasty, PDA clipping, and pulmonary artery banding. Because both subclavian and descending aortic circulations were expected to be unreliable during aortic cross-clamping, the superficial temporal artery (STA) was selected as the only feasible site for real-time cerebral perfusion…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1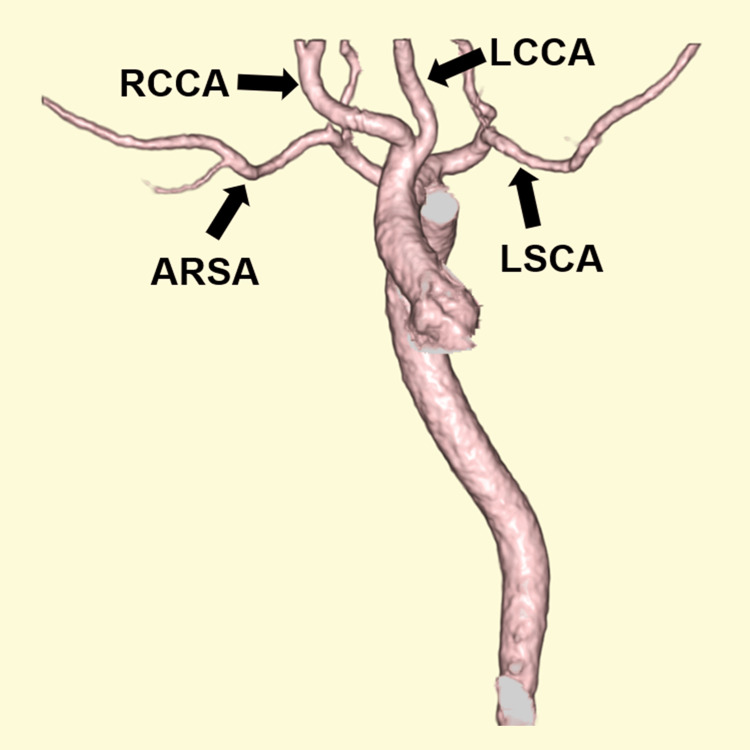 Figure 2
Figure 2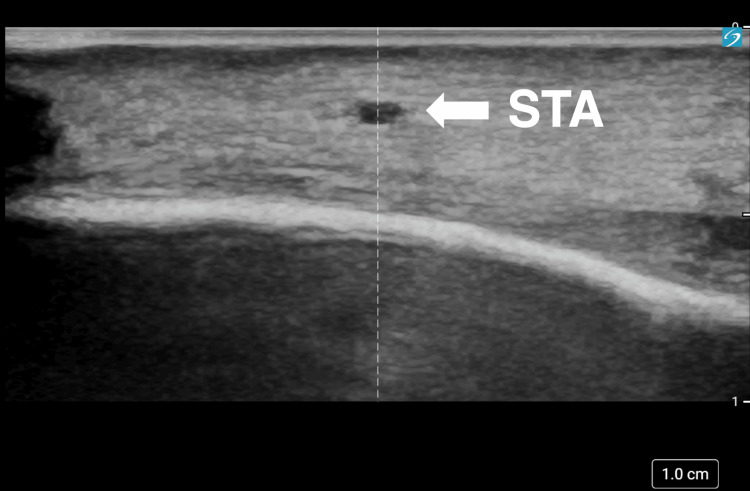 Figure 3
Figure 3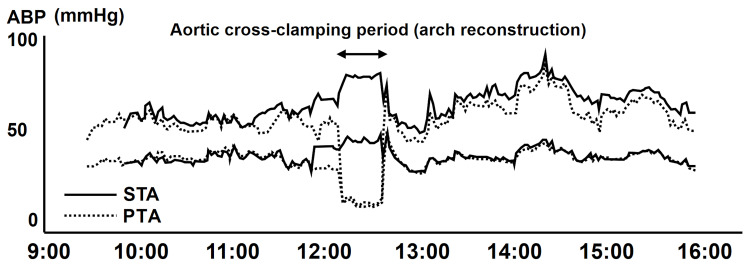 Figure 4
Figure 4| Time point | STA BP (mmHg), SBP/DBP (MAP) | PTA BP (mmHg), SBP/DBP (MAP) | HR (beats/min) |
| Start of surgery | 59/39 (48) | 58/40 (48) | 156 |
| Pre-clamp | 72/42 (51) | 50/31 (38) | 146 |
| During cross-clamp | 80/46 (56) | 13/12 (13) | 150 |
| Post-clamp | 61/43 (50) | 60/46 (51) | 158 |
| End of surgery | 73/40 (50) | 67/40 (48) | 149 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Tracheal and airway disorders · Neonatal and fetal brain pathology
Introduction
Coarctation of the aorta (CoA) is a congenital narrowing of the aortic isthmus, typically located distal to the left subclavian artery and adjacent to the ductal insertion [1]. CoA frequently occurs as part of a broader spectrum of left-sided obstructive lesions rather than as an isolated anomaly and may coexist with additional congenital cardiac malformations.
Aberrant right subclavian artery (ARSA) is an anatomic variation in which the right subclavian artery arises as the fourth branch of the aortic arch from the proximal descending aorta rather than from the brachiocephalic trunk [2].
The combination of CoA and ARSA creates unique hemodynamic challenges, particularly during aortic arch repair, because arterial pressure obtained from either upper or lower extremities may not accurately reflect true cerebral perfusion. In simple terms, during aortic cross-clamping, the blood pressure measured in the arm or leg may not reflect the pressure supplying the brain; therefore, monitoring a proximal arterial pressure waveform helps clinicians assess whether cerebral perfusion is likely being maintained.
In such circumstances, arterial access through the superficial temporal artery (STA) has been reported as a feasible site for continuous arterial pressure monitoring and as a surrogate for cerebral perfusion, particularly in neonates and infants undergoing complex cardiac surgery [3]. However, despite its potential value, STA cannulation remains uncommon in clinical practice, largely due to technical difficulty, small vessel caliber, and limited published experience, especially in low-birth-weight infants and complex congenital heart disease.
Here, we report a neonatal case of CoA complex with ARSA in which STA cannulation was successfully performed to obtain reliable intraoperative cerebral arterial pressure monitoring. This case highlights the clinical relevance of STA access as an alternative monitoring strategy when conventional arterial sites are unreliable or unavailable.
Case presentation
A 14-day-old male neonate was referred for the surgical correction of complex congenital heart disease. At birth, his length was 45.2 cm, and his weight was 1.819 kg. He had been followed prenatally for suspected complex cardiac malformation, lateral ventricular enlargement, cleft lip and palate, and intrauterine growth restriction. He was delivered via elective cesarean section at 40 weeks and four days of gestation.
Postnatal echocardiography confirmed the coarctation complex, including patent ductus arteriosus (PDA), single right ventricle, double-outlet right ventricle, single atrium, total anomalous pulmonary venous return (type IIa), and mitral atresia (Figure 1).
Transthoracic echocardiography demonstrating aortic isthmus narrowing consistent with coarctationSuprasternal notch long-axis view demonstrating discrete narrowing at the aortic isthmus (arrow), consistent with CoA.CoA: coarctation of the aorta
Computed tomography angiography further delineated the aortic arch anatomy, including the aberrant right subclavian artery (Figure 2).
Three-dimensional computed tomography angiography demonstrating aortic arch branching anomaly3D volume-rendered computed tomography angiography demonstrating the aortic arch branching anomaly with an ARSA. Arrows indicate ARSA, LCCA, LSCA, and RCCA.ARSA: aberrant right subclavian artery; LCCA: left common carotid artery; LSCA: left subclavian artery; RCCA: right common carotid artery
Progressive heart failure prompted surgical intervention consisting of left subclavian artery flap aortoplasty for coarctation repair, ductal clipping, and pulmonary artery banding. Given the planned aortic arch cross-clamping in the setting of ARSA, arterial pressure monitoring from the upper or lower extremities was expected to be unreliable as a surrogate for proximal (cerebral) arterial pressure during key phases of the repair. Therefore, STA cannulation was planned for continuous proximal arterial pressure monitoring.
General anesthesia was induced rapidly with midazolam, fentanyl, and rocuronium, followed by endotracheal intubation. A posterior tibial arterial line, peripheral venous access, urinary catheter, STA line, and central venous catheter via the left internal jugular vein were subsequently secured. Because the patient was positioned in the right lateral decubitus position, the left STA was selected for cannulation. A high-resolution ultrasound system (Sonosite PX, Fujifilm, Tokyo, Japan) with a high-frequency linear probe (L19-5) was used to evaluate the STA. The STA measured 0.47×0.35 mm at a depth of approximately 2 mm from the skin surface on preoperative ultrasound (Figure 3).
Preoperative ultrasound image of the left STAShort-axis high-frequency ultrasound image of the left STA at a depth of approximately 2 mm from the skin surface. The inner lumen measured 0.47×0.35 mm on preoperative assessment.STA: superficial temporal artery
Despite the anticipated technical difficulty, a 24-gauge catheter (outer diameter 0.7 mm) designed for peripheral arterial access was successfully inserted under ultrasound guidance, and a stable arterial waveform was obtained.
Surgery was performed through a right lateral thoracotomy at the third intercostal space. The aortic arch and left subclavian artery origin were clamped, and the left subclavian artery was divided to create a flap. The aberrant right subclavian artery, ductus arteriosus, and descending aorta were subsequently cross-clamped. The narrowed aortic segment was incised and repaired using the subclavian flap technique. Pulmonary artery banding was performed using a polytetrafluoroethylene strip.
General anesthesia was maintained with midazolam, fentanyl, and rocuronium. The aortic arch cross-clamp time was 45 minutes, during which continuous cerebral perfusion was successfully monitored using the STA pressure waveform. Following coarctation repair, no significant pressure gradient was observed between the upper and lower extremities (Figure 4, Table 1).
ABP trends during aortic cross-clampingDuring aortic cross-clamping, the PTA pressure waveform became markedly attenuated, whereas the STA pressure waveform remained continuously available for proximal arterial pressure monitoring. Upper and lower traces represent systolic and diastolic pressures.ABP: arterial blood pressure; PTA: posterior tibial artery; STA: superficial temporal artery
Postoperatively, the patient required diaphragmatic plication for phrenic nerve paralysis but otherwise recovered without major complications. He remains under follow-up and is awaiting bidirectional Glenn surgery with Damus-Kaye-Stansel anastomosis, relief of pulmonary venous obstruction, and pulmonary artery reconstruction. Genetic testing revealed partial trisomy of chromosome 12 and partial monosomy of chromosome 17.
Discussion
CoA occurs in approximately 0.04% of live births and accounts for 6-8% of congenital heart disease, whereas an ARSA, the most common aortic arch branching anomaly, has an estimated prevalence of around 1% in the general population and approximately 3% among patients with congenital heart disease [1,2,4]. In standard CoA repair without anomalous vascular branching, arterial pressure monitoring from the right upper extremity generally reflects cerebral perfusion during aortic cross-clamping. However, when ARSA is present, blood flow to the right upper limb may also be interrupted during surgical repair, rendering both upper- and lower-extremity arterial pressure measurements unreliable. In such cases, direct invasive arterial pressure monitoring via the STA may provide a practical option for approximating proximal (cerebral) arterial pressure and assessing cerebral perfusion [3]. Although STA cannulation has been described as a viable monitoring strategy, it is not without risk. Potential complications include thrombosis, local infection, positive blood cultures, local scarring, and cerebral embolization [3]. Careful patient selection and early removal planning are essential to minimize catheter-related morbidity, especially in neonatal and low-birth-weight populations where vessel fragility is pronounced [5].
In the present case, STA cannulation was anticipated to be technically challenging because the patient was a low-birth-weight neonate (1.819 kg) and the STA lumen measured only 0.47×0.35 mm on preoperative ultrasound imaging. However, recent advances in high-resolution ultrasound technology and increased clinician proficiency in ultrasound-guided arterial access have improved procedural feasibility and safety [6-8]. Ultrasound allowed the precise visualization of the artery, needle trajectory, and catheter placement, contributing to the successful establishment of a stable arterial waveform throughout the procedure. Interestingly, the inner luminal dimensions of the STA (0.47×0.35 mm) appeared smaller than the outer diameter of the 24-gauge catheter (0.7 mm), which, at first glance, suggests an unfavorable catheter-to-artery size relationship. It should be emphasized that ultrasound measurements represent the internal lumen in a single two-dimensional plane and may underestimate the functional vessel caliber, particularly when the artery is partially collapsed or transiently vasoconstricted or the luminal border is difficult to delineate (e.g., due to probe pressure or suboptimal imaging plane). In addition, small muscular arteries in neonates are highly compliant and can accommodate temporary deformation and stretching of the vascular wall during needle entry and catheter placement.
Pediatric data indicate that 24-gauge catheters are commonly used for arterial cannulation in very small arteries, with a high technical success rate when ultrasound guidance is employed, albeit at the cost of a relatively high catheter-to-artery diameter ratio and a theoretical increased risk of occlusion [6-8]. In our case, continuous STA waveforms were maintained without clinical evidence of scalp ischemia. The catheter was removed early postoperatively as a precaution to minimize the risk of catheter-related vascular compromise.
A systematic review and meta-analysis found that ultrasound-guided arterial cannulation improves first-attempt success rates and reduces the number of attempts and complications compared with traditional landmark techniques in children [6]. Similarly, randomized and observational studies in infants have demonstrated higher success rates for ultrasound-guided radial arterial cannulation than for palpation-based techniques [7]. In addition, a recent neonatal case series, including very-low-birth-weight infants, reported high success rates for ultrasound-guided peripheral arterial cannulation without major complications [8].
During aortic cross-clamping, the left posterior tibial arterial pressure waveform became markedly attenuated, whereas the STA waveform remained continuously measurable. Although most prior studies have focused on radial or posterior tibial arteries, our case illustrates that these advantages of high-resolution ultrasound can be extended to extremely small-caliber STA access in low-birth-weight neonates. Bhaskar et al. previously described infants with complex aortic arch pathology and aberrant subclavian anatomy in whom STA cannulation provided reliable proximal arterial pressure monitoring when limb pressures were unreliable during aortic arch reconstruction [3]. Our case adds to this limited body of evidence by demonstrating that STA cannulation can be successfully achieved even in a very small neonate with a body weight of 1.819 kg and an STA diameter of only 0.47×0.35 mm. To our knowledge, reports of STA cannulation in such small-caliber vessels in the context of CoA with ARSA are scarce, and our experience underscores the potential role of STA monitoring in carefully selected high-risk neonatal cardiac cases.
A limitation of this report is the absence of multimodal cerebral monitoring beyond STA pressure. Previous reports suggest that multimodal cerebral monitoring modalities such as near-infrared spectroscopy or transcranial Doppler may enhance the reliability of cerebral perfusion assessment when used in combination with STA pressure monitoring [3,9-10]. In this case, regional cerebral oximetry (O3™ Regional Oximetry, Masimo, Irvine, California, United States) could not be utilized due to limited forehead space. When feasible, such adjunct monitoring may provide additional safety margins in similar high-risk neonatal cardiac surgeries.
Conclusions
STA cannulation may serve as a valuable and practical arterial monitoring option in neonates with complex congenital heart disease, particularly when anatomical variations, such as an aberrant right subclavian artery, render conventional monitoring sites unreliable. In this case, the use of high-resolution ultrasound enabled successful cannulation despite the extremely small vessel caliber and contributed to safe intraoperative management. This experience suggests that modern ultrasound-guided vascular access techniques may expand the feasibility of STA monitoring in select high-risk neonatal cardiac surgical populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coarctation of the aorta: from fetal life to adulthood Cardiol J Kenny D Hijazi ZM 487495182011 https://pubmed.ncbi.nlm.nih.gov/21947983/2194798310.5603/cj.2011.0003 · doi ↗ · pubmed ↗
- 2Aberrant right subclavian artery with left aortic arch: associated cardiac anomalies Pediatr Cardiol Zapata H Edwards JE Titus JL 159161141993841521810.1007/BF 00795645 · doi ↗ · pubmed ↗
- 3Selective use of superficial temporal artery cannulation in infants undergoing cardiac surgery Ann Card Anaesth Bhaskar P John J Lone RA Sallehuddin A 6066081820152644025610.4103/0971-9784.166486 PMC 4881661 · doi ↗ · pubmed ↗
- 4Prevalence of the aberrant right subclavian artery reported in a published systematic review of cadaveric studies: the impact of an outlier Clin Anat Polednak AP 102410283020172851451210.1002/ca.22905 · doi ↗ · pubmed ↗
- 5Cannulation of the temporal artery in neonates and infants Paediatr Anaesth Nobuo J Tsunehiko S 7047051720071756465810.1111/j.1460-9592.2006.02188.x · doi ↗ · pubmed ↗
- 6Ultrasound-guided arterial cannulation in the paediatric population Cochrane Database Syst Rev Raphael CK El Hage Chehade NA Khabsa J Akl EA Aouad-Maroun M Kaddoum R 03202310.1002/14651858.CD 011364.pub 3PMC 998329936866968 · doi ↗ · pubmed ↗
- 7Ultrasound-guided arterial cannulation in infants improves success rate Eur J Anaesthesiol Schwemmer U Arzet HA Trautner H Rauch S Roewer N Greim CA 4764802320061651297410.1017/S 0265021506000275 · doi ↗ · pubmed ↗
- 8Effectiveness of ultrasound-guided peripheral arterial cannulation in neonates, including very low birth weight infants who are conventionally difficult-to-cannulate: a case series Eur J Pediatr Okada Y Kido T Takeuchi S 50951218320243793039910.1007/s 00431-023-05320-6 · doi ↗ · pubmed ↗