Applying FRAME-IS to characterize provider-led adaptations to a cervical cancer prevention intervention in Kenya
Harriet Fridah Adhiambo, Katherine Thomas, Megan M. Coe, Lynda Oluoch, Valary Ihaji, Mary Bernadette Kerubo, Alex Kinyua, Sarah Njoroge, Kenneth Ngure, Michelle Shin, Thomas A. Odeny, Bryan Weiner, Nelly Mugo, Sarah Gimbel

TL;DR
This study uses the FRAME-IS framework to track adaptations made to a cervical cancer prevention strategy in Kenya, showing how providers modified the approach over time.
Contribution
The paper demonstrates the application of FRAME-IS to document provider-led adaptations in a cervical cancer prevention intervention in a low-resource setting.
Findings
Most adaptations (70%) occurred in the early phase of implementation.
Educational adaptations were most common, targeting providers delivering screening and treatment services.
Adaptation rates significantly declined over time, from 2.0 per facility in the early phase to 0.80 in the late phase.
Abstract
Implementation strategies that are contextually refined are essential for optimizing the delivery of evidence-based interventions (EBI) to prevent cervical cancer in low-resource settings. This paper reports the application of the Framework for Reporting Adaptations and Modifications to Evidence-based Implementation Strategies (FRAME-IS) to capture and disseminate strategy adaptations made to a single-visit, screen-and-treat approach with thermal ablation (SV-SAT + TA) strategy aimed at establishing sustainable cervical cancer prevention services in Kenya. A FRAME-IS-based tracking spreadsheet was developed to document bundled site-specific implementation strategy adaptations and across 10 facilities. Data was collected during technical assistants' (TAs) site visits, phone calls, and monthly meetings with health providers between March 2023 and September 2024. Sources of adaptation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
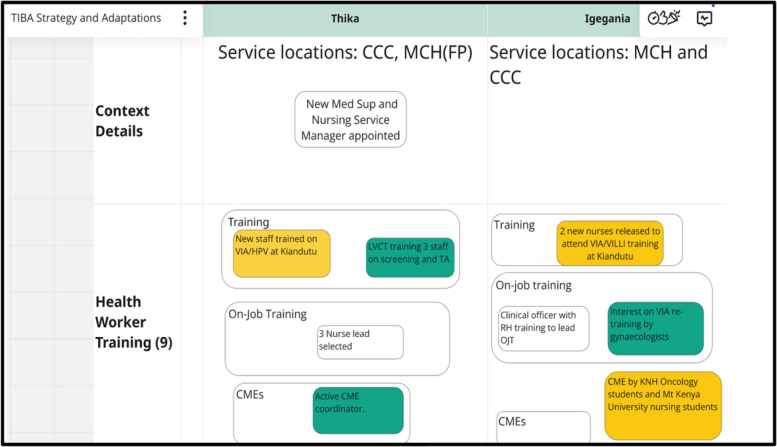 Figure 1
Figure 1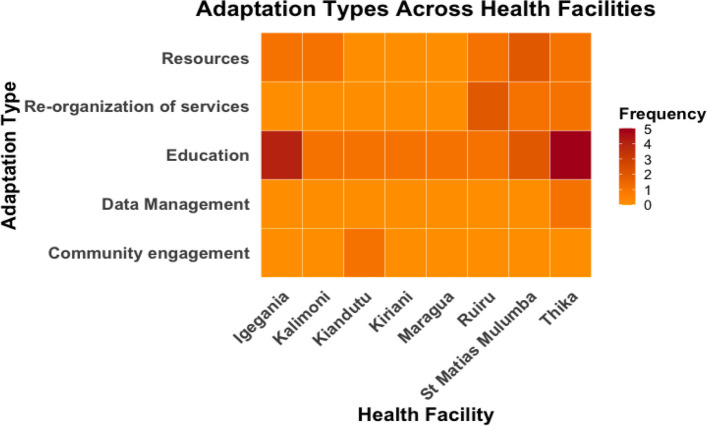 Figure 2
Figure 2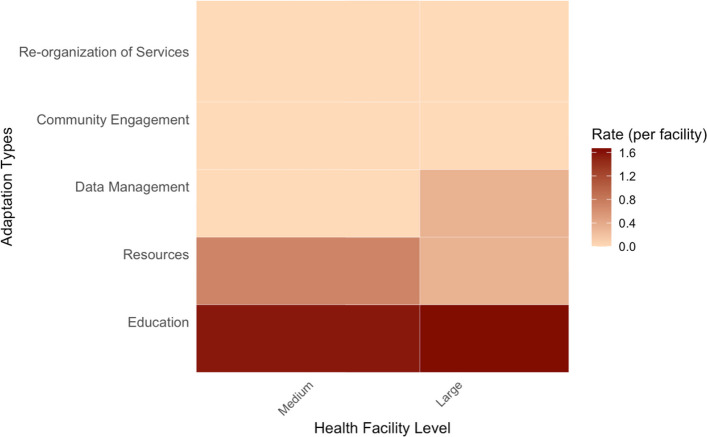 Figure 3
Figure 3- —National Cancer Institute (NCI)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Health Policy Implementation Science · Diabetes Management and Education
Contributions to the literature• We highlight the importance of provider education and resource adaptations in optimizing cervical cancer prevention, contributing to understanding how these factors influence the success of interventions.• We demonstrate the utility of FRAME-IS in systematically documenting and tracking adaptations to evidence-based implementation strategies, offering a structured approach for capturing and disseminating adaptations.• We address critical gaps in adaptation literature by using FRAME-IS to observe how implementation strategies evolve in practice systematically, an area rarely reported. Our study reveals trends and adaptation patterns that offer new insights into the nature of strategy implementation and inform future efforts to scale evidence-based interventions.
Background
Integrating evidence-based implementation strategies in real-world settings characterized by complex contextual realities is often challenging. This complexity is heightened by misaligned organizational priorities and constrained resources, often necessitating modifications or adaptations [1]. Adaptations are deliberate alterations to an intervention or an implementation strategy aiming to achieve fit within a context while maintaining fidelity to the core components [2, 3]. Evidence-based interventions and strategies are often adapted, adopted, or abandoned based on various factors, including indications of low effectiveness, emerging barriers and facilitators, and other multi-level influences [4–6]. Therefore, documenting and reporting strategy adaptations is critical to providing insights into what is more or less important for enhancing strategy effectiveness and sustainability, providing a foundation for replication in similar contexts [1, 7–9].
While we know why adaptations occur, [10, 11] less is understood about their evolution, underlying patterns, and their long-term impact. These knowledge gaps limit our ability to learn from real-world implementation to optimize strategies for scale-up. This challenge is especially evident in cervical cancer prevention. Despite the availability of effective preventive interventions, including primary prevention through Human Papillomavirus (HPV) Vaccination and secondary prevention through screen and treat approaches, which involve identification and immediate treatment of precancerous cervical lesions to prevent progression to cancer [12, 13] the burden of cervical cancer remains on the rise in low- and middle-income countries [14] due to inconsistent implementation of these preventive measures, primarily attributed to limited resources and infrastructure [15, 16]. Although most of these interventions have demonstrated success, for example, the introduction of HPV vaccination, there is limited evidence concerning context-specific adaptations made to enhance their fit and impact on clinical and implementation outcomes. This challenge is not unique to cervical cancer prevention interventions but extends to several effectiveness and implementation trials [2, 17, 18].
Existing tools, such as the Framework for Reporting Adaptations and Modifications to Evidence-based Implementation Strategies (FRAME-IS), among others, provide a structured process for tracking strategy adaptations [2, 17, 19]. FRAME-IS has been used to track adaptations to strategies for implementing mHealth interventions [20–22], pediatric guidelines, and mental health interventions, [7, 8, 20, 23] yet its application remains limited in the context of cervical cancer prevention. This emphasizes the need for more empirical work to understand how strategy adaptations influence implementation.
To address these gaps, we applied FRAME-IS to capture and disseminate adaptations to implementation strategies aimed at promoting the uptake and delivery of the single-visit, screen-and-treat approach with thermal ablation (SV-SAT + TA) for cervical cancer prevention in Kenya. The SV-SAT + TA is a bundled evidence-based intervention (EBI) composed of visual inspection with acetic acid (VIA) and same-day treatment with thermal ablation being implemented through a stepped-wedge cluster randomized trial in 10 health facilities in Kenya [24–27]. Henceforth, "TIBA," a Swahili word for treatment, will represent the single-visit, screen-and-treat approach with thermal ablation. We report how FRAME-IS was used to document bundled strategy adaptations within TIBA, providing insights necessary for its optimization and scale-up within the Kenyan health system.
Methods
Study setting and design
This longitudinal sub-study characterizing adaptations to implementation strategies is nested within a larger hybrid type III implementation trial aiming to develop and test implementation strategies for TIBA to enhance cervical cancer screening and treatment of precancerous lesions in Kenya (NCTO5472311) [28]. TIBA was implemented across 10 health facilities in Kenya, using a three-wave stepped wedge design.
The reproductive health facilities implementing TIBA are medium to larger in size, i.e., Levels four and five [29, 30], which refer to Sub-County and County referral hospitals. Level four provides comprehensive inpatient and outpatient care, while Level 5 offers specialized services, including surgery, oncology, obstetrics/gynecology, and serves as a referral center for lower-level health facilities. The study sites are located in Kiambu, Embu, and Murang'a Counties in the central region of Kenya. Kiambu county borders the capital city, Nairobi, while Embu is situated east of Mount Kenya. Murang’a County is situated between Kiambu and Embu and is renowned for its agricultural activities. These counties offer a mix of urban and rural contexts, with well-established county referral hospitals that provide cancer screening and treatment services. Levels 4 and 5 will hereafter be referred to as medium and larger facilities, respectively.
Conceptual framework
The Framework for Reporting Adaptations and Modifications to Evidence-based Implementation Strategies was employed in this sub-study to assess changes in TIBA implementation over time. FRAME-IS provides a structured, systematic approach to documenting adaptations and modifications to implementation strategies, promoting consistent reporting [31]. The framework is composed of seven modules, four of which are considered core. The core modules cover four main areas: a brief description of the implementation strategy (Module 1), what was modified, such as content, evaluation, content, or training (Module 2), the nature of the modification (Module 3), and the goal and level of the rationale for the modification (Module 4).
Three optional/supplementary modules provide additional details, including modification timing and whether the modification was planned or reactively adopted (Module 5), which participants were involved in the decision to modify (Module 6), and the extent or spread of the modification (Module 7).
We selected FRAME-IS because it is among the first and most widely employed tools developed to track adaptations to implementation strategies. Our data collection tool was informed by FRAME-IS modules 1 to 5, and we included additional sections to capture contextual factors, thus providing a comprehensive understanding of each adaptation.
Data collection
FRAME-IS guided the development of an Excel-based tracking tool for documenting adaptations to TIBA strategies in response to implementation barriers. These barriers to implementing TIBA and potential implementation strategies were identified during a baseline stakeholders' workshop that consisted of healthcare providers, health facility managers, policymakers, and implementing partners offering reproductive health services, as well as through formative qualitative interviews with providers and health facility managers at each of the 10 health facilities. Each health facility was then asked to prioritize three to five key barriers to address during the implementation of TIBA, based on feasibility assessment to ensure the chosen strategies were practical and achievable within their context.
From these discussions, a list of 18 potential strategy options (Supplementary material) was generated collaboratively by the facility representatives and subsequently refined by the research team. Health facilities then applied these strategy options to address the specific barriers prioritized at each site. Table 1 below provides the list of strategies applied to address site-specific barriers across the 10 health facilities. These are the strategies that were subsequently adapted during implementation. Table 1. Site-specific barriers and corresponding implementation strategiesSiteAssociated barrierImplementation StrategiesEmbuLack of trained personnel on cervical cancer screening and treatmentLack of awareness about cervical cancer screening among clients seeking services at Embu level 5 hospitalLack of job aids and algorithmStrengthen mechanisms for health worker training/mentoring and coachingCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentProvision of job aids and similar resources for health workersKirianiLack of trained personnel on cervical cancer screening and treatmentLack of thermal ablation machine, digital wall clock, and white light sourceLimited space in cervical cancer screening roomsLack of job aids (HPV & VIA algorithms) and cervical cancer screening registers (MOH 412 & 745)Lack of awareness about cervical cancer screening among clients seeking services at Kiriaini missionStrengthen mechanisms for health worker training/mentoring and coachingBetter availability and management of essential medications, supplies and equipmentImprovements to the organization of care (e.g., colocation of multiple services in one setting)Provision of job aids and similar resources for health workersCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentMurang’aLack of trained personnel on cervical cancer screening and treatmentLack of awareness about cervical cancer screening among clients seeking servicesLack of essential supplies and equipmentLack of job aidsIncomplete cervical cancer treatment (Patients declining cervical cancer treatment)Strengthen mechanisms for health worker training/mentoring and coachingCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentBetter availability and management of essential medications, supplies and equipmentAvailability of job aids and similar resources for health workersSupport to clients to retain them in system of care (e.g., support for follow up, linkages to other sexual and reproductive health services)St Matias MulumbaLow screening numbersShortage of trained providers on screening and treatmentLack of SOPs, guidelines, algorithms, updated registers, and job aidsFragmented approach to screening and treatment of precancerous lesions (screening done, screen positives scheduled for treatment by gynecologist)Lack of equipment and supplies (speculums, Lugol’s iodine, acetic acid, lack of thermal ablators or LEEP equipment.)Community engagement, service communication, sensitization related to cervical cancer screening and treatmentStrengthen mechanisms for health worker training/mentoring and coachingAvailability of job aids and similar resources for health workersImprovements to the organization of care (e.g., colocation of multiple services in one setting)Better availability and management of essential medications, supplies and equipmentIgeganiaProvider knowledge gaps on screening and treatmentLack of supportive supervision/follow up after trainingLack of essential medication and suppliesUnstructured Clinic flowLow screening numbersStrengthen mechanisms for health worker training/mentoring and coachingImprovements to supervision and quality assuranceBetter availability and management of essential medications, supplies and equipmentStreamlined patient journey (admission to screening, to treatment, to follow up)Community engagement, service communication, sensitization related to cervical cancer screening and treatmentKalimoniLack of trained personnel on screening and treatmentLack of TA equipment, applicator sticks and cotton woolLack of awareness about cervical cancer screening among clients accessing services at Kalimoni hospitalLack of enough rooms for cervical cancer screeningCost of screeningStrengthen mechanisms for health worker training/mentoring and coachingBetter availability and management of essential medications, supplies and equipmentCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentImprovements to the organization of care (e.g., colocation of multiple services in one setting)Other efforts to mitigate financial burden of care-seekingKiandutuLack of trained personnel on screening and treatmentLack of speculums, clean gloves, acetic acid, and cotton wool. Lack of a rotating stool and trolley in the screening roomsLack of awareness about cervical cancer screening among clients seeking services at Kiandutu hospitalLack of job aidsLack of a structured flow of clientsStrengthen mechanisms for health worker training/mentoring and coachingBetter availability and management of essential medications, supplies and equipmentCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentAvailability of job aids and similar resources for health workersStreamlined patient journey (admission to screening, to treatment, to follow up)MaraguaLack of trained personnel on screening and treatmentLack of supplies and equipment for cervical cancer screeningLack of awareness about cervical cancer screening among clients accessing services at Maragua level 4 hospitalLack of structured flow of clients accesing cervical cancer screening services at MCHIncomplete CC treatment (Patients declining treatment)Strengthen mechanisms for health worker training/mentoring and coachingBetter availability and management of essential medications, supplies and equipmentCommunity engagement, service communication, sensitization related to cervical cancer screening and treatmentStreamlined patient journey (admission to screening, to treatment, to follow up)Support to clients to retain them in system of care (e.g., support for follow up, linkages to other SRH services)RuiruPoor linkage to care for clients who are ineligible for ablative treatmentLack of acetic acid, proper gynecological bed, privacy, and biopsy bottleLack of integration of cervical cancer screening services within the maternal and child health clinicSupport to clients to retain them in system of care (e.g., support for follow up, linkages to other sexual and reproductive health services)Better availability and management of essential medications, supplies and equipmentImprovements to the organization of care (e.g., colocation of multiple services in one setting)ThikaLack of trained personnel on screening and treatmentLack of essential medications and supplies (Pain meds, antibiotics, speculums, lugol's iodine, acetic acid, lack of thermal ablators and LEEP equipment.)Lack of SOPs, guidelines, algorithms, and job aidsPoor documentation of cervical cancer servicesLong distance between service points (Comprehensive care centers located far from reproductive health clinic)Incomplete cervical cancer treatment (Patients declining treatment)Strengthen mechanisms for health worker training/mentoring and coachingBetter availability and management of essential medications, supplies and equipmentAvailability of job aids and similar resources for health workersImprovements regarding recording and management of routine health informationImprovements to the organization of care (e.g., colocation of multiple services in one setting)Support to clients to retain them in system of care (e.g., support for follow up, linkages to other SRH services)
Data was collected monthly between March 2023 and September 2024 across the 10 health facilities, with each health facility being observed for six consecutive months during the implementation phase. The data collection occurred during technical assistants' support visits, phone calls, and monthly meetings with health providers and their managers across the three implementation waves. The data was entered into the Excel-based tracking sheet. The data entered entailed whether the strategy component was ultimately adapted, adopted, or abandoned, a description of each adaptation, adaptation type, by whom, when it was initiated, whether it was ad hoc or planned, and the goal of the adaptation. We elicited feedback on adaptations over time through discussions with the providers and health facility managers. Additional data on contextual factors related to the strategy adaptation, barriers, and facilitators were also collected. We created a Miro board (https://miro.com) to synthesize findings and compare site adaptations. This visual whiteboard captures strategy components (clear boxes), site-specific contextual factors (green), and adaptations (yellow) that were updated monthly (Fig. 1). Adaptations were considered adopted if used at two consecutive observation points.Fig. 1. Miro Board. A section of the TIBA Miro board
An extraction tool aligned with the FRAME-IS modules with modifications to module 2 (What was modified-context category) of the framework to expand the categories of the adaptation types (education, resources, data management, communication, service reorganization, and community engagement) was applied by five authors (HAF, VI, BMK, AK, and SN) to systematically extract and organize the data for analysis. During the extraction phase, the five authors convened two brief meetings to assess the consistency and accuracy of their interpretations of their characterization of the adaptations. Additionally, we categorized the adaptations into two periods, i.e., early adaptations (1–3 months after the site initiated the intervention) and late adaptations (from months 4–6).
The extracted data was reviewed by an independent coder (MMC) to assess the consistency and reliability of the coding process. Three discussion meetings were held between the lead author, the independent coder, and one of the project's investigators (SG) to review convergence, reconcile discrepancies, and reach a consensus on the characterization of the adaptations.
Analysis
We used descriptive statistics to summarize the study sites' characteristics and describe trends and patterns in adaptation types over time and across the health facility levels. Adaptation rates were computed per facility per 3 or 6-month period. Due to the small counts of adaptations in our analysis, we used an exact Poisson test to compare whether the adaptation rates varied across the health facility level, which we grouped as medium four vs large. The test produces a rate ratio, a 95% confidence interval, and a p-value. For the same reason, we also applied the exact Poisson test to compare whether the adaptation rates significantly changed across the two time periods (early vs late). However, the exact Poisson test does not take into account the pairing in the data across time points and is, therefore, conservative. Analyses were performed using R version 4.5.0 and "poisson. exact" R package.
Ethical considerations
Ethics approval was granted by the Scientific and Ethical Review Committee of the Kenya Medical Research Institute (SERU-KEMRI No. 4403) in Nairobi, Kenya, and the Human Subjects Institutional Review Board (STUDY00014200) at the University of Washington, Seattle, USA.
Results
Overall, 70% of health facilities were medium level (n = 7), and 30% were larger (n = 3). Most (80%, n = 8) of the health facilities were located in urban areas and were publicly managed (70%, n = 7). Two hundred and sixty health providers, including nurses, clinical officers, and gynecologists, were trained on cervical cancer screening using VIA and treatment with thermal ablation, with 58% (n = 152) of the providers from medium-level health facilities. Approximately 18%(n = 46) of the providers trained offered screening and treatment services during the study period across both site levels. Table 2 provides a summary of the characteristics of the participating health facilities. Table 2. Characteristics of participating clinicsCharacteristicAll (n, %)Medium-level (n, %)Larger(n, %)No. of health facilities10 (100%)7(70%)3(30%)Management TypeGovernment7(70%)4(57%)3(100%)Faith-based3(30%)3(43%)0(0%)LocationUrban8(80%)5(71%)3(100%)Rural2(20%)2(29%)0(0%)No. of providers trained in offering Cervical Cancer screening and treatment (TIBA)260(100%)152(58%)108(42%)No. of providers offering Cervical Cancer screening and treatment (TIBA)46(100%)24(52%)22(48%)We had one lower-level facility, which was grouped with medium-level facilities based on comparable characteristics
Module 1: description of the evidence-based practice and implementation strategies
The SV-SAT + TA is a bundled evidence-based intervention (EBI) composed of visual inspection with acetic acid (VIA) and same-day treatment with thermal ablation for precancerous lesions, aiming to prevent cervical cancer by improving timely access to care. A bundle of site-specific implementation strategies (Table 1) was adapted to address the associated barriers to implementing the SV-SAT + TA across the facilities.
Module 2: what was modified
A total of 28 adaptations were identified, of which two adaptation types were unique. Over half of the adaptations (57%, n = 16) were related to education, targeting patients or providers, followed by resource-related adaptations (21%, n = 6), for example, changes to essential commodity acquisition. There were no differences in adaptation types when comparing urban to rural facilities. Table 3 provides the detailed distribution of the adaptation types, with the education category representing the most significant proportion. Table 3. Summary of adaptation typesFRAME-IS CategoriesAdaptation TypesCountProportionExamples of adaptationsTrainingEducation1657%New staff trained on screening and treatment at nearby health facilityContextResources621%Essential commodities like speculums supplied by implementing partners due to procurement delaysContextService Reorganization414%Services moved from the MCH clinic to the outpatient departmentContextCommunity Engagement14%In-reach activity supported by implementing partnersTrainingData Management14%SOPs developed by implementing partners to guide documentation in the register
Figure 2 visualizes the distribution of adaptation types across t 8 health facilities that made adaptations. Overall, there is a variation in the adaptation types, suggesting that some facilities were more focused on certain adaptations than others.Fig. 2. Heat map visualizing adaptation types across health facilities
Module 3: nature of adaptations
Almost half of the adaptations (46%, n = 13) focused on tailoring provider education related to cervical cancer. For example, new staff who missed training sessions at their own facility were allowed to attend training on cervical cancer screening at nearby health facilities to increase the adoption of the TIBA intervention at their facilities. The training strategy was tailored depending on the staffing challenges at each site. Furthermore, many educational adaptations were enhanced by adding new components (29%, n = 8), including the creation of alternative patient pathways for individuals ineligible for thermal ablation and supplementary resources such as links to the International Agency for Research on Cancer (IARC) that offered in-depth information on cervical cancer to bolster provider competency.
Module 4: goals and levels for modifications
Of the 28 adaptations, 43% (n = 12) aimed to increase the adoption of TIBA by expanding the number of clinicians offering cervical cancer screening with VIA and treatment with thermal ablation through provider training. An additional 36%(n = 10) focused on increasing reach, i.e., the number of patients receiving TIBA. This was achieved by increasing the number of cervical cancer service delivery points, providing essential screening commodities, and targeted in-reach and outreach activities. Eighteen percent (n = 5) targeted improving fidelity through supportive supervision, and one (3%) adaptation aimed to improve clinical effectiveness.
Most adaptations (46%, n = 13) targeted the organizational level, emphasizing the leadership role in resource mobilization to ensure continuity in cervical cancer delivery. Approximately 39% (n = 11) targeted the clinician level, addressing gaps in provider skills, which aligned with the goal of increasing the number of providers implementing TIBA. Adaptation at the patient level were less frequent (14%, n = 4), but those focused on expanding TIBA reach.
Module 5: timing of the modifications and their level of planning
All the adaptations occurred during the implementation phase, and the majority occurred in the early phase (71%, n = 20) Over half of the adaptations (57%, n = 16) were planned. A substantial proportion of unplanned adaptations were mainly implemented in response to clinical training needs among new staff and delays in the procurement of essential commodities. 75% (n = 21) of adaptations were adopted, and none were abandoned. However, given our definition of an adopted adaptation (two consecutive observation points), the majority (seven) of the adaptations not adopted after the first round of implementation were one-time ad-hoc changes mainly intended to address skill gaps among providers of cervical cancer screening and treatment.
Table 4 below provides an illustrative example of how the FRAME-IS was completed to document an adaptation to an implementation strategy used for the SV-SAT + TA. In this example, the implementation strategy of job aid provision was adapted by adding images of the screened cervix showing either a screen-positive or screen-negative finding, which were shared with providers via WhatsApp, along with a link to the International Agency for Research on Cancer (IARC). These additions were intended to support provider understanding and improve fidelity. Table 4FRAME-IS completion exampleFRAME-IS ModuleExampleModule 1Evidenced based intervention being implementedImplementation strategyModification/Adaptations madeReason for the modificationSingle visit, screen and treat approach with thermal abaltion (SV-SAT + TA)Provision of job aidsAdding Images of the screened cervix showing either a screen-positive or screen-negative finding, which were shared with providers via WhatsApp, along with a link to the International Agency for Research on Cancer (IARC) to improve their understanding of the processTo improve fidelityModule 2What was modified?TrainingModule 3What is the nature of the training modification?Adding elementsModule 4What is the goal of the modification?What is the level of the modification?Improve fidelityOrganizational levelModule 5When was the modification initiated?Was the modification planned or unplanned?During implementationPlanned
Change in adaptation rates across time and across health facility levels
Table 5 below summarizes adaptation rates across time and Levels (medium vs large). Table 5. Change in adaptation rates across time and across health facility levelsAdaptation TypesOver TimeBy levelMonth 1–3 (rate per 3-months)Month 4–6(rate per 3-months)Months 1–6 (rate per 6-months)Resources Medium-level1 (0.33)0 (0.00)1 (0.33) Large3 (0.43)2 (0.29)5 (0.72) Total4 (0.40)2 (0.20)6 (0.60)Data Management Medium-level1 (0.33)0 (0.00)1 (0.33) Large0 (0.00)0 (0.00)0 (0.00) Total1 (0.10)0 (0.00)1 (0.10)Education (Provider and Patient) Medium-level2 (0.67)3 (1.00)5 (1.67) Large10 (1.43)1 (0.14)11 (1.57) Total12 (1.20)4 (0.40)16 (1.60)Community Engagement Medium-level0 (0.00)0 (0.00)0 (0.00) Large0 (0.00)1 (0.14)1 (0.14) Total0 (0.00)1 (0.10)1 (0.10)Reorganization of services Medium-level1 (0.33)0 (0.00)1 (0.33) Large2 (0.29)1 (0.14)3 (0.43) Total3 (0.30)1 (0.10)4 (0.40)TotalOver TimeBy levelMonth 1–3Month 4–6Months 1–6Large5 (1.67)3 (1.00)8 (2.67)Medium15 (2.14)5 (0.71)20 (2.85)Total20 (2.0)8 (0.80)28 (2.80)p-value0.020.89Key: n (adaptation rate per clinic per 3 or 6-month period as indicated), n = 10 (total no. of health facilities), n = 7 (no. of medium-level health facilities), n = 3 (no. of larger health facilities)
We observed an overall rate of 2.67 adaptations per facility over a six-month period in larger facilities, compared to 2.85 adaptations per clinic over the same period in medium-level facilities (rate ratio = 0.93 (95% CI = 0.39–2.08, p = 0.89), indicating no statistically significant difference in adaptation rates between the facility levels. Figure 3 visualizes adaptation rates across health facility levels.Fig. 3. Adaptation rates comparing medium-level and larger health facilities
During the early phase, we observed an overall rate of 2.0 adaptations per facility, compared to 0.80 adaptations per facility in the late phase (rate ratio = 2.50, 95% CI = 1.12–6.02, p = 0.02), indicating a statistically significant decrease in adaptations over time.
Discussion
Our study provides key insights into patterns of strategy adaptations necessary to enhance fit and optimize cervical cancer prevention, particularly in LMICs. Guided by FRAME-IS, we identified 28 adaptations, most of which focused on provider and patient education, followed by resource adaptations. The primary goals of these adaptations were to increase provider adoption of TIBA and reach (the number of women being screened and treated for precancerous lesions), with most of the adaptations occurring in the early phase of implementation and being planned. Adaption rates were consistent across health facility levels, though significantly higher in the early implementation phase, highlighting early enthusiasm to enhance strategy fit. Education-related adaptations aimed at tailoring strategies to staff needs and local contexts, and they remained common across the time periods (early and late periods).
We observed an overall rate of 2.0 adaptations per facility in the early phase, compared to 0.80 adaptations per facility in the late phase (rate ratio = 2.50, 95% CI = 1.12–6.02, p = 0.02), indicating a statistically significant decrease in adaptations over time. Early adaptations occur as initial challenges and misalignments with context are more apparent, resulting in proactive adjustments to improve the fit of an intervention or strategy [32]. For example, in our study, challenges such as high provider workload, staff transfers between departments and clinics, and onboarding new staff are findings reported in the literature [33–35] that led to the tailoring of provider education. These adaptations, occurring early in the implementation phase, primarily focused on the action target (health providers) by offering flexible training opportunities at nearby health facilities and additional mentorship from implementing partners to ensure adoption, fidelity to the clinical task, and broader use (reach). Addressing challenges through tailored context-specific adaptations ensures better alignment with the contextual realities, enhancing strategy effectiveness and sustainability [36, 37]. We hypothesize that the frequent adaptations during the early phase were necessary as TIBA fit within the health facility setting. Over time, these adaptations were successfully integrated into the health facility's routine, marking a stabilization phase during the later phase, hence the decline in the adaptation rate over time. It is also possible that there was a decline in organizational enthusiasm.
We found no significant differences in the adaptation rates across the health facility levels. However, following Geng et al.' s 's [38] recommendation to consider the "dose" of an adaptation, tracking both the frequency and intensity of specific adaptations, such as provider education, could offer deeper insights into site-level variation that may otherwise go unrecognized.
Most of our adaptations were planned as recommended in the literature [39] and targeted the organizational level. This allowed the health facilities to maximize the fit of the strategies through collaborative meetings and goal setting among key stakeholders, including frontline staff/implementers, health facility managers, and implementing partners, ensuring aligned priorities and resources. The approach minimized disruptions in service delivery, emphasizing the importance of meaningful stakeholder engagement in ensuring the success of an intervention [8, 40, 41].
Interestingly, two health facilities did not report any adaptations to the implementation strategies. Both were Larger health facilities located in urban areas and did not face challenges with essential commodities for cervical cancer screening, as they received support from larger implementing partners and procured these commodities through their health facilities, unlike the other sites. One of the facilities also provided training on cervical cancer screening and treatment to health providers in peripheral health facilities. This initiative aimed to reduce the number of women referred to their facility for screening and precancer treatment. It sought to increase the broader adoption of TIBA among providers and expand its reach within the region. Additionally, leadership support in these two facilities was evident, and a positive and receptive attitude was observed among providers offering cervical cancer preventive services. Perhaps these two health facilities, in addition to their leadership support, possessed a high level of adaptive capacity [42] and had a functioning system in place, possibly explaining the lack of strategy adaptations. While leaders from all the facilities were involved in the strategy development phase, contributions from these active leaders may have led to the strategy having better fit when introduced, so requiring less adaptation. Further exploration is needed to examine how the clinical and implementation outcomes differed between these facilities and others with strategy adaptations.
Lessons learned when applying FRAME-IS
FRAME-IS was valuable in documenting and tracking adaptations to the TIBA strategy during the implementation phase. It provided a clear view of how TIBA was optimized within the various health facilities.
Determining whether an adaptation occurred was challenging when the original strategy implementation plan lacked sufficient detail. Proctor's recommendation for naming, defining, and operationalizing implementation strategies would help ensure consistency in documenting strategy adoptions and adaptations [43].
FRAME-IS does not provide guidance on adopted strategy adaptations. We defined "adopted adaptations" as those changes that were consistently implemented over two months. We also incorporated a section in the data collection tool to capture emerging barriers and facilitators, providing actionable guidance for strategy adjustments.
FRAME-IS characterizes adaptations into four main categories, i.e., context, content, training, and evaluation, as outlined in module 2. However, during preliminary coding, we encountered challenges applying these categories, as they were not mutually exclusive, and the terminology used was unfamiliar to Technical Assistants and would subsequently be challenging to health providers during dissemination. To address this, we expanded the context and training adaptation types into six categories: community engagement, data management, resources, education, communication, and reorganization of services, which were terminologies familiar and easily interpreted among the health providers in our context. Despite these revisions, we still faced challenges coding certain adaptations. For example, patient education can logically fit under the "community engagement" and "education" categories. Similar challenges have been reported by other authors [8, 18], who addressed these challenges by incorporating additional modules to provide in-depth information on the specific adaptations, implementing a numbering system to map changes to other modules, and adding supplementary coding categories. These refinements can be considered by the authors of FRAME-IS if there is a future update to the framework.
This study had limitations. First, we have not assessed the impact of these adaptations on the implementation and clinical outcomes, which would have provided insights into which adaptations were effective in optimizing TIBA. However, this does not undermine the validity of our findings, as we provided useful information on the adaptation types and examined the trends and patterns of these adaptations during TIBA implementation. Secondly, the study's technical assistants obtained information on the adaptations through monthly conversations with providers and their managers, which may have potentially introduced recall and social desirability biases. Finally, due to time constraints, we could only track adaptations during the active implementation phase, not the maintenance phase. Perhaps tracking adaptations beyond the implementation phase would have provided additional insights into the sustainability patterns of the adaptations.
Strengths
FRAME-IS has previously been applied in Kenya to track adaptations to a mobile health strategy [20]; however, our study is the first to report its application in the context of cervical cancer preventive intervention. We prospectively collected data on these adaptations, offering valuable learning opportunities on optimizing the framework's use while making real-time adjustments to the data collection tool to enhance data quality. We compared adaptation rates across health facility levels and examined how these adaptations evolved. This comparison provided useful information on immediate adaptations needed to support the successful implementation of TIBA.
Conclusion
We demonstrate the capability of FRAME-IS in documenting and tracking strategy adaptations, highlighting the critical role of education adaptations as the most frequently needed modifications to optimize cervical cancer preventive interventions. Over time, we observe a reduction in these adaptation rates, indicating a potential stabilization or strategy fit. Based on our experiences applying the framework, we offer recommendations targeting refinements to module 2 categories, adding new modules to link strategy adaptations to outcomes, and improving data capture of contextual factors influencing the implementation of the adapted strategies.
Future studies should focus on evaluating the impact of these adaptations on both implementation and clinical outcomes, exploring the “dose” of adaptations, and determining an ideal duration for tracking them. Furthermore, establishing an “adaptome,” a knowledge base, or a collection of implementation strategy adaptations [8, 41, 44] would allow the collection of contextualized data that can be easily adapted, facilitating scaling and replication of strategy adaptations in different settings.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith JD, Merle JL, Webster KA, Cahue S, Penedo FJ, Garcia SF. Tracking dynamic changes in implementation strategies over time within a hybrid type 2 trial of an electronic patient-reported oncology symptom and needs monitoring program. Front Health Serv [Internet]. 2022;2. Available from: https://www.frontiersin.org/journals/health-services/articles/10.3389/frhs.2022.983217/full. Cited 2025 Feb 6.10.3389/frhs.2022.983217 PMC 1001268636925901 · doi ↗ · pubmed ↗
- 2Cervical cancer. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer. Cited 2025 Feb 12.
- 3Anticipating Changes That May Affect Intervention Fidelity [Internet]. Rethinking Clinical Trials. Available from: https://rethinkingclinicaltrials.org/chapters/conduct/monitoring-intervention-fidelity-and-adaptations/anticipating-changes-that-may-affect-intervention-fidelity/. Cited 2025 Feb 19.
- 4Stirman SW, Baumann AA, Miller CJ. The FRAME: an expanded framework for reporting adaptations and modifications to evidence-based interventions. Implementation Science : IS. 2019;14. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 6554895/. Cited 2024 Jan 25.10.1186/s 13012-019-0898-y PMC 655489531171014 · doi ↗ · pubmed ↗