Real-world outcomes following PARP inhibitor maintenance in ovarian cancer by BRCA status: a retrospective cohort study
K. Zucker, B. Pickwell-Smith, A. Samani, A. Sujenthiran, H. Pittell, P. Mpofu, G. Hall

TL;DR
This study finds that using PARP inhibitors as first-line treatment for ovarian cancer may reduce the effectiveness of future chemotherapy, regardless of BRCA status.
Contribution
The study provides real-world evidence on the impact of first-line PARP inhibitor use on subsequent treatment outcomes in ovarian cancer.
Findings
Subsequent treatment responses are shorter after first-line PARPi in ovarian cancer.
Shortened responses occur in both second- to third- and third- to fourth-line treatments.
Shortened effects of subsequent treatment occur irrespective of BRCA status.
Abstract
The introduction of poly (adenosine-diphosphate ribose) polymerase inhibitors (PARPis) has significantly improved progression-free survival for patients with ovarian cancer after response to first-line platinum-based chemotherapy. Yet, there are concerns that PARPi may compromise response to further platinum due to cross-resistance mechanisms. This study investigates the clinical effectiveness of chemotherapy post-progression on PARPi maintenance therapy after initial platinum-based treatment for ovarian cancer, regardless of BRCA mutations, using real-world data. Additionally, this study summarises results across randomised trials of PARPi as first-line maintenance. This study used a United States-based electronic health record-derived de-identified database. A retrospective descriptive analysis was conducted on patients with ovarian cancer diagnosed from 1 January 2015 onwards.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
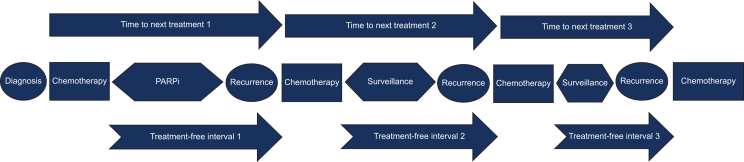 Figure 1
Figure 1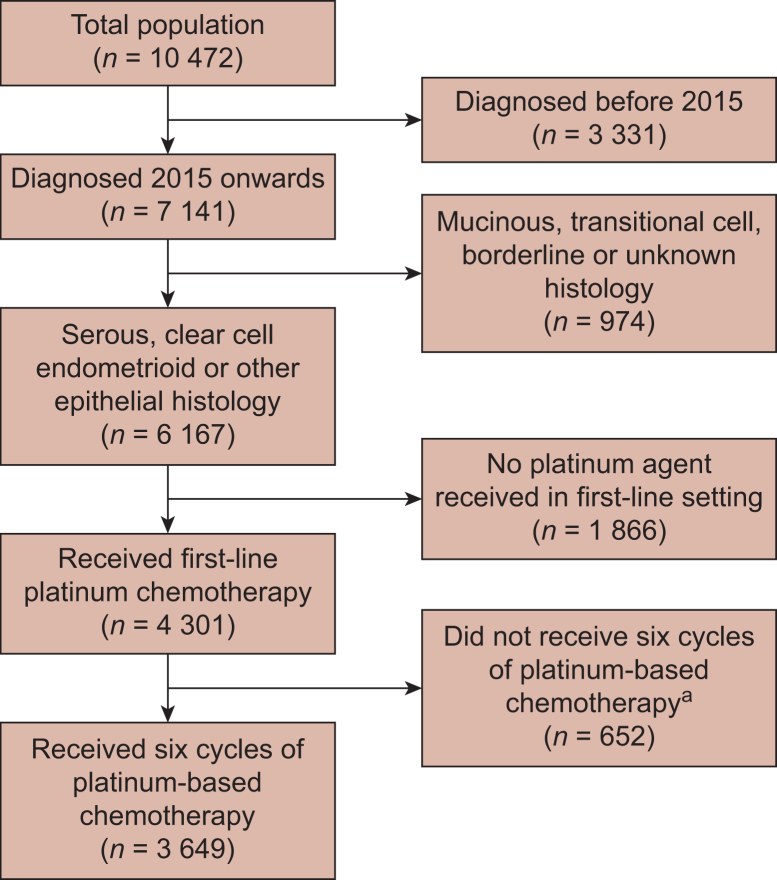 Figure 2
Figure 2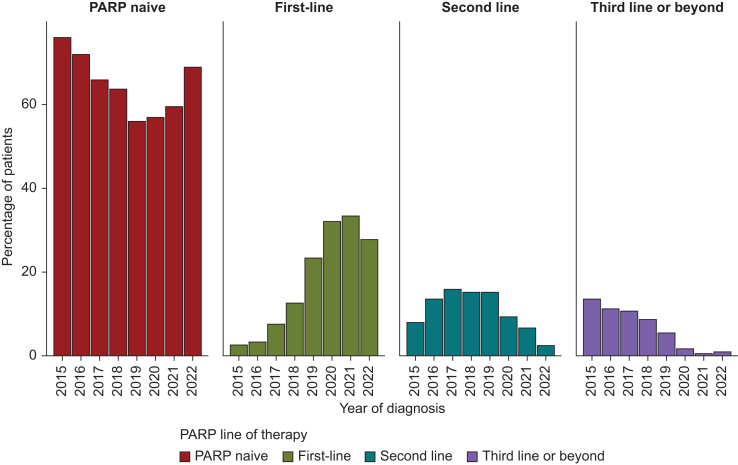 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPARP inhibition in cancer therapy · Ovarian cancer diagnosis and treatment · BRCA gene mutations in cancer
Introduction
Ovarian cancer is the second-highest cause of mortality among gynaecological cancers,1 with 14 000 deaths in the United States and 26 221 in Europe in 2017.2^,^3 Most patients are diagnosed at an advanced stage, with high-grade serous carcinoma (HGSC) being the most prevalent subtype.4 Approximately 50% of HGSC cancers are associated with homologous recombination deficiency (HRD).5 Less common epithelial subtypes include high-grade endometrioid carcinoma, low-grade serous carcinoma, and clear-cell carcinoma.
Despite optimal debulking surgery and platinum-based chemotherapy, many patients relapse within 18 months of first-line treatment.6 Progression-free survival (PFS) captures the interval during and after treatment when cancer remains stable. Poly (adenosine-diphosphate ribose) polymerase (PARP) inhibitors (PARPis) have transformed outcomes, with trials demonstrating significant improvements in PFS through maintenance therapy.7
Initially used in relapsed cases, PARPis benefit patients with BRCA mutations, and HRD-positive and HRD-negative disease. SOLO2 showed significant PFS improvement with olaparib in BRCA-mutated patients after two prior chemotherapy lines.8 The NOVA trial demonstrated PFS benefit with niraparib, irrespective of BRCA or HRD status after two treatment lines.9 Meanwhile, clinical trials have explored the benefits of PARPis following first-line chemotherapy, demonstrating significantly prolonged PFS, particularly in patients with a BRCA mutation (germline or somatic) and in those with BRCA wild-type HRD-positive tumours. Notably, four trials have assessed the efficacy of first-line PARPi as maintenance monotherapy—SOLO-1, PRIMA, VELIA/GOG-3005 and ATHENA-MONO—while one trial has assessed the efficacy of PARPi in combination with bevacizumab as maintenance therapy in the first-line setting (Table 1).10, 12, 14, 15, 16Table 1. Summary of randomised trials of PARPis as first-line maintenanceTrial (year/s)ComparisonProgression-free survival (HRD ± BRCA mutations)Progression-free survival (other analyses)Overall survival (HRD ± BRCA mutations)Overall survival (other analyses)SOLO-110^,^11 (2018, 2022)Olaparib versus placeboBRCA mutation onlyAt 3 years 60% versus 27%HR 0.3, CI 0.23-0.41NABRCA mutation onlyNR versus 75.2 monthsHR 0.55, CI 0.40-0.76NAPRIMA12^,^13 (2019)Niraparib versus placeboBRCA-positive subgroup22.1 versus 10.9 monthsHR 0.40, CI 0.27-0.62HRD-positive subgroup19.6 versus 8.2 monthsHR 0.50, CI 0.31-0.83HRD-negative subgroup8.1 versus 5.4 monthsHR 0.68, CI 0.49-0.94HRD-positive subgroupHR 0.95, CI 0.70-1.29Overall population OSHR 1.01, CI 0.84-1.23VELIA14 (2019)Veliparib versus placeboBRCA-positive subgroup34.7 versus 22.0 monthsHR 0.44, CI 0.28-0.68HRD-positive subgroup31.9 versus 20.5 monthsHR 0.57, CI 0.43-0.76Intention-to-treat15.2 versus 17.3 monthsHR 1.07, CI 0.90-1.29ImmatureImmatureATHENA-MONO15 (2022)Rucaparib versus placeboHRD-positive28.7 versus 11.3 monthsHR 0.47, CI 0.31-0.72HRD-negative12.1 versus 9.1 monthsHR 0.65, CI 0.45-0.95ImmatureImmaturePAOLA-116^,^17 (2019, 2023)Olaparib and bevacizumab versus bevacizumab and placeboBRCA mutation37.2 versus 21.7 monthsHR 0.31, CI 0.20-0.47BRCA-negative HRD-positive28.1 versus 16.6 monthsHR 0.43, CI 0.28-0.66HRD-negative or HRD unknown16.9 versus 16 monthsHR 0.92, CI 0.72-1.17BRCA mutationAt 5 years 73.2% versus 53.8% aliveHR 0.60, CI 0.39-0.93BRCA-negative HRD-positiveAt 5 years 54.7% versus 44.2% aliveHR 0.71, CI 0.45-1.13HRD-negativeAt 5 years 25.7% versus 32.3% aliveHR 1.19, CI 0.88-1.63CI, confidence interval; HR, hazard ratio; HRD, homologous recombination deficiency; NR, not reached; OS, overall survival; NA, not applicable/not available; PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitor.
SOLO-1 randomised patients diagnosed with stage III or IV high-grade serous or endometrioid ovarian cancer with germline BRCA mutations who responded to first-line platinum-based therapy to olaparib or placebo.10 Results indicated a significant improvement in PFS. Overall survival (OS) did not reach statistical significance, though it was clinically meaningful (Table 1).10^,^11
Conversely, the PRIMA trial evaluated the impact of niraparib as maintenance in patients with stage III and IV ovarian cancer after first-line platinum-based chemotherapy without restriction based on HRD status. It revealed a significant PFS benefit with niraparib compared with placebo, irrespective of HRD status. However, the observed benefit was more pronounced in BRCA-mutated or BRCA-wild-type HRD-positive tumours.12 Meanwhile, OS data remain unpublished in peer-reviewed journals but suggest no OS benefit.18^,^13 Similarly, the VELIA/GOG-3005 trial randomised patients with stage III or IV ovarian cancer, regardless of BRCA or HRD status, to receive chemotherapy alone or chemotherapy plus veliparib followed by veliparib maintenance or placebo. While there were significant improvements in PFS for those with BRCA mutations and HRD positivity, the benefit was not statistically significant in the HRD-negative cohort (Table 1).14
Meanwhile, the PAOLA-1/ENGOT-ov25 trial included patients with stage III and IV ovarian cancer, irrespective of BRCA or HRD status, post-initial platinum-based therapy, randomising to maintenance with olaparib plus bevacizumab or placebo plus bevacizumab. In the HRD-positive population, the combination of olaparib and bevacizumab significantly improved PFS and OS. However, these results were not replicated in HRD-negative tumours.16^,^17 Finally, the ATHENA-MONO trial compared rucaparib versus placebo in patients with stage III-IV high-grade cancer following response to first-line platinum-based chemotherapy, stratified by HRD status. Rucaparib improved PFS for patients with and without HRD (Table 1).15
These studies demonstrated PFS benefits in HRD-positive patients receiving first-line PARPi. However, results for HRD-negative patients are mixed, with varying PFS outcomes, and no OS advantage in HRD-negative, BRCA-wild-type HRD-positive, or HRD-positive groups.12^,^17 Substantial OS benefits were seen in BRCA-mutated patients in SOLO1 and PAOLA-1, despite 44.3%-45.7% crossing over in the placebo group.11^,^17
Given the lack of survival benefits in BRCA-negative HRD-positive, or HRD-negative groups, additional evidence is needed to identify who benefits from PARPi treatment and the optimal treatment timing.
Emerging evidence suggests PARPis may drive resistance to subsequent treatment. Cecere et al. reported unexpectedly low response rates after olaparib maintenance therapy.19 Baert et al. reported reduced platinum response in the third-line setting in patients after PARPi.20
The SOLO2 post hoc analysis showed a 7.3-month longer time to second progression in the placebo group.21 Cleveland Clinic data showed significantly worse PFS after PARPi in BRCA-mutated patients in the second- or third-line setting (8.0 months versus 19.1 months).22 Retrospective analysis by Romeo et al. reported that the response rates to subsequent platinum-based chemotherapy were worse among patients with BRCA mutations than patients with BRCA wild-type.23 Collectively, these studies suggest a potential role of PARPis in promoting platinum resistance in the relapsed setting. Suggested mechanisms for this potential cross-resistance have also been postulated.24 These concerns highlight a need for more comprehensive real-world studies to understand the impact of PARPi maintenance, particularly in the first-line setting where the evidence remains scarce.
The current study aims to describe the efficacy of chemotherapy following disease progression on PARPi maintenance therapy in the first-line setting, irrespective of BRCA mutational status, leveraging real-world data sources.
Materials and methods
Study type and dataset
This retrospective observational descriptive real-world data study was delivered utilising the Flatiron Health database, a longitudinal database comprising de-identified patient-level structured and unstructured data curated via technology-enabled abstraction.25^,^26 During the study period, the de-identified data originated from ∼280 United States cancer clinics (∼800 care sites). Most patients in the database originate from community oncology settings; relative community/academic proportions may vary by cohort. The study included patients diagnosed with primary ovarian, fallopian tube, and primary peritoneal cancers from 1 January 2015 to 1 July 2023.
Inclusion criteria and cohort design
As this study relies on the Flatiron Health ovarian dataset, patients were required to meet two sets of inclusion criteria: those that determine inclusion in the original source dataset and a subsequent set of study-specific criteria.
Flatiron Health source data inclusion criteria
The Flatiron datamart-specific inclusion criteria were as follows:
- •Diagnosis with an International Classification of Diseases (ICD) code for ovarian, fallopian tube, or peritoneal cancer (ICD 9: 183x, 158x; ICD 10: C56x, C57.0x, C48x) on or after 1 January 2011.
- •Histology: one of serous, mucinous, clear cell, transitional cell, endometrioid, epithelial not otherwise specified (NOS), borderline, and unknown/undocumented. Note: High- versus low-grade serous distinction was unavailable in this dataset.
- •At least two documented clinical visits, on different days, occurring on or after 1 January 2011. This was a pragmatic decision to ensure sufficient clinical data.
Study-specific inclusion criteria and cohort design
After receiving the data, further inclusion criteria were applied. Patients were limited to those diagnosed from 1 January 2015 to 1 July 2023 with evidence of receiving platinum-based therapy in the first-line (non-maintenance) setting. Patients with borderline, mucinous, transitional cell, or unknown histology were excluded as PARPi is not routinely used in these subtypes. To mitigate issues of immortal time bias, patients were also limited to those receiving at least six cycles of platinum-based chemotherapy in the first-line setting. This issue required addressing due to the use of post-baseline information (use of maintenance PARPi) to classify individuals at baseline.
Sub-cohorts were created based on treatment and molecular status. This first sub-cohort division was based on treatment, and the total study population was divided into two groups:
- 1)A first-line PARPi group, including patients treated with first-line PARPi maintenance therapy (olaparib, niraparib, or rucaparib).
- 2)A non-first-line PARPi group, including all patients with no evidence of maintenance therapy or non-maintenance therapy with a PARPi (olaparib, niraparib, or rucaparib) as part of their first-line treatment.
These cohorts were then subdivided based on molecular status, dividing each group further by BRCA-positive and BRCA-negative status. BRCA positivity was defined as the presence of either a germline or somatic BRCA mutation. Patients with unknown molecular status were excluded from these sub-cohorts, while those with a BRCA variant of unknown significance were treated as BRCA-negative. BRCA positivity was defined as those with recorded evidence of a pathological mutation of BRCA1 and/or BRCA2 in either the germline or somatic testing.
A further tier of subdivision was then applied based on HRD molecular status. This resulted in sub-cohorts based on BRCA status, HRD status, and PARPi treatment.
Baseline characteristics
Summary information relating to baseline characteristics was derived for each patient cohort. This included information on the baseline Eastern Cooperative Oncology Group (ECOG), race/ethnicity, age, socioeconomic status, and International Federation of Gynecology and Obstetrics (FIGO) stage. Where patients had multiple ECOG scores recorded, the score closest in number of days to the date of diagnosis was used. Only ECOG recorded within 30 days before or after diagnosis were included with those patients without an ECOG score recorded within this window marked as ECOG unknown.
Time-to-event analysis
The study focused on describing several time-to-event metrics across the total population and pre-specified sub-populations. These included OS, time to next treatment (TTNT) for the second, third and fourth treatment, and treatment-free interval (TFI) after the first, second and third treatment. OS was defined as the period from diagnosis until the date of death or censoring. The TFI was defined as the time from the last dose of non-maintenance systemic anticancer treatment (SACT) until the next line of systemic anticancer treatment. TTNT one (TTNT1) was defined as the time from starting the first line of non-maintenance SACT until the start of the second subsequent line of SACT (Figure 1). TTNT two (TTNT2) was defined as the time from completion of the second line of chemotherapy to the initiation of third-line chemotherapy. TTNT three (TTNT3) was defined as the time from completion of the third course of chemotherapy to the initiation of fourth-line chemotherapy. A new line of therapy was defined according to Flatiron Health’s oncologist-defined, rule-based lines of therapy.Figure 1Time to next treatment and treatment-free intervals definitions and visual explanations. PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitors.
Because death dates are provided only as month and year (for privacy), the date of death was estimated as the 15th of the death month unless post-death encounters were recorded—in which case the last-seen date was used. This avoided negative time at risk and affected only a few patients. Each time-to-event analysis was conducted using a Kaplan–Meier estimator in the relevant population. All analyses were undertaken using R version 4.2.1 with packages used detailed in Supplementary Table S1, available at https://doi.org/10.1016/j.esmorw.2025.10065.
As the dataset did not contain information relating to the histological grade of each patient’s tumour which is directly related to the likelihood of receiving PARPi, only descriptive analysis was undertaken and no comparative statistical tests have been applied.
Ethical approval
The local institutional ethics panel had granted approval (MREC 23-018). Prior institutional review board (IRB) approval with included waiver of informed consent was obtained. The WCG IRB granted approval. (The Flatiron Health Real-World Evidence Parent Protocol, Tracking # FLI118044). ESMO GROW checklist can be found in the Supplementary Material, available at https://doi.org/10.1016/j.esmorw.2025.10065.
Results
This study involved 280 United States clinics and identified 3649 patients who met the eligibility criteria (Figure 2). The median age at diagnosis was 66 years (interquartile range 57-73 years). Sixty-four percent of patients were white, 8.6% were Latin, 5.7% were black or African American, 3% were Asian, and 9.1% were other specified ethnicities, with 9.5% unknown. Patient demographics, tumour subtypes, and characteristics are summarised in Table 2. The median duration of follow-up was 30 months.Figure 2Flow diagram to show the exclusions applied to the whole cohort.^a^Numbers may reflect that some patients were still receiving treatment at the data cut-off point.Table 2. Patient characteristics, stage, histology, and HRD status grouped by receipt of PARPi use in first-line setting or notCharacteristicAll patients N = 3649First-line PARPi N = 621BRCA-negative first-line PARPi, N = 376BRCA-positive first-line PARPi, N = 202BRCA unknown first-line PARPi, N = 43Non-first-line PARPi, N = 3028BRCA-negative non-first-line PARPi, N = 2093BRCA-positive non-first-line PARPi, N = 297BRCA unknown non-first-line PARPi, N = 638Age at diagnosis, years (range)66 (57-73)65 (57-72)66 (60-73)61 (53-69)64 (57-77)66 (57-74)66 (57-73)61 (54-68)68 (59-77)Deprivation, n (%) 1 (most deprived)464 (13)71 (11)42 (11)19 (9.4)≤10 (23)393 (13)245 (12)45 (15)103 (16) 2570 (16)102 (16)64 (17)30 (15)≤10 (23)468 (15)330 (16)39 (13)99 (16) 3672 (18)112 (18)72 (19)35 (17)≤10 (23)560 (18)379 (18)54 (18)127 (20) 4818 (22)150 (24)89 (24)54 (27)≤10 (23)668 (22)468 (22)73 (25)127 (20) 5 (least deprived)847 (23)141 (23)86 (23)48 (24)≤10 (23)706 (23)500 (24)72 (24)134 (21) Unknown278 (7.6)45 (7.2)23 (6.1)16 (7.9)≤10 (23)233 (7.7)171 (8.2)14 (4.7)48 (7.5)ECOG, n (%) 0557 (15)119 (19)68 (18)45 (22)≤10 (23)438 (14)326 (16)44 (15)68 (11) 1495 (14)89 (14)55 (15)28 (14)≤10 (23)406 (13)264 (13)48 (16)94 (15) 2119 (3.3)22 (3.5)15 (4.0)≤10 (4)≤10 (23)97 (3.2)67 (3.2)≤10 (3)22 (3.4) 334 (0.9)≤10 (2)≤10 (3)≤10 (4)≤10 (23)28 (0.9)18 (0.9)≤10 (3)≤10 (2) 4≤10 (<0.1)≤10 (2)0 (0)≤10 (4)0 (0)0 (0)0 (0)0 (0)0 (0) Unknown≥2434 (67)≥381 (62)≥228 (61)123 (61)27 (63)2059 (68)1418 (68)195 (66)≥444 (70)Race/ethnicity, n (%) Latin312 (8.6)50 (8.1)23 (6.1)19 (9.4)≤10 (23)262 (8.7)163 (7.8)25 (8.4)74 (12) Asian110 (3.0)26 (4.2)17 (4.5)≤10 (4)≤10 (23)84 (2.8)57 (2.7)12 (4.0)15 (2.4) Black or African American208 (5.7)48 (7.7)29 (7.7)15 (7.4)≤10 (23)160 (5.3)93 (4.4)17 (5.7)50 (7.8) Other race333 (9.1)51 (8.2)36 (9.6)13 (6.4)≤10 (23)282 (9.3)198 (9.5)24 (8.1)60 (9.4) White2339 (64)384 (62)227 (60)≥128 (63)26 (60)1955 (65)1385 (66)190 (64)380 (60) Unknown347 (9.5)62 (10.0)44 (12)17 (8.4)≤10 (23)285 (9.4)197 (9.4)29 (9.8)59 (9.2)Stage at diagnosis, n (%) 0403 (11)62 (10.0)38 (10)16 (7.9)≤10 (23)341 (11)228 (11)22 (7.4)91 (14) 1477 (13)17 (2.7)≤10 (2.7)≤10 (4)0 (0)460 (15)297 (14)36 (12)127 (20) 2323 (8.9)31 (5.0)16 (4.3)14 (6.9)≤10 (23)292 (9.6)199 (9.5)29 (9.8)64 (10) 31560 (43)319 (51)197 (52)≥105 (52)14 (33)1241 (41)895 (43)141 (47)205 (32) 4886 (24)192 (31)≥115 (31)57 (28)20 (47)694 (23)474 (23)69 (23)151 (24)Histology, n (%) Clear cell235 (6.4)≤10 (2)≤10 (2.7)≤10 (4)≤10 (23)227 (7.5)165 (7.9)≤10 (3)60 (9.4) Endometrioid288 (7.9)15 (2.4)13 (3.5)≤10 (4)0 (0)273 (9.0)191 (9.1)≤10 (3)72 (11) Epithelial NOS522 (14)84 (14)52 (14)27 (13)≤10 (23)438 (14)294 (14)28 (9.4)116 (18) Serous2604 (71)≥512 (82)≥301 (81)≥151 (76)≥27 (63)2090 (69)1443 (69)257 (87)390 (61)BRCA status, n (%) Negative2469 (68)376 (61)376 (100)0 (0)0 (0)2093 (69)2093 (100)0 (0)0 (0) Positive499 (14)202 (33)0 (0)202 (100)0 (0)297 (10)0 (0)297 (100)0 (0) Unknown681 (19)43 (7)0 (0)0 (0)43 (100)638 (21)0 (0)0 (0)638 (100)HRD, n (%) Negative363 (9.9)63 (10)57 (15)≤10 (4)≤10 (23)300 (9.9)291 (14)≤10 (3)≤10 (2) Positive349 (9.6)156 (25)101 (27)52 (26)≤10 (23)193 (6.4)135 (6.5)53 (18)≤10 (2) Unknown2937 (80)402 (65)218 (58)≥140 (72)29 (67)2535 (84)1667 (80)≥234 (78)625 (98)Where patient numbers where ≤10 data obfuscation has been applied as a privacy preserving measure.ECOG, Eastern Cooperative Oncology Group; HRD, homologous recombination deficiency; NOS, not otherwise specified; PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitor.
Approximately 71% of patients had serous histology, 14% had epithelial NOS, 7.9% endometrioid, and 6.4% had clear-cell histology. The majority of patients (68%) were BRCA-negative, a significant proportion (19%) had an unknown BRCA status, and the remainder (14%) were BRCA-positive. Most patients (80%) had unknown HRD status, 9.9% of patients were negative for HRD, and 9.6% had HRD-positive tumours.
A total of 621 patients (17%) received first-line maintenance PARPi. Of these, 376 (61%) were BRCA-negative, 202 (33%) were BRCA-positive, and 43 (7%) were BRCA unknown. Meanwhile, 3028 patients (83%) did not receive first-line PARPi. Of these, 2093 (69%) were BRCA-negative, 297 (10%) were BRCA-positive, and 638 (21%) were BRCA unknown. Bevacizumab was received within the first line of treatment by 882 patients of whom 219 were in the cohort receiving PARPi and the remaining 663 were in the non-PARPi-receiving cohort.
Overall survival
The reverse Kaplan–Meier-derived median study follow-up time from diagnosis until data cut-off was 55.1 months. The median OS was 60 months [95% confidence interval (CI) 57-64 months]. Median OS was higher in patients receiving a first-line PARPi [68 months (95% CI 62-82 months)] compared with patients not receiving a first-line PARPi [58 months (95% CI 56-62 months)]. This higher estimated survival was seen for patients with BRCA-positive {>100 [95% CI 68-not reached (NR)] versus 90 [95% CI 85-NR]} and -negative disease [66 (95% CI 50-NR) versus 57 (95% CI 54-61)]; however, variation in precision of estimates due to varying patient numbers was also apparent. However, patients with an unknown BRCA status treated with first-line PARPi had a slightly shorter median OS [40 months (95% CI 33 months-NR)] compared with those who did not receive a first-line PARPi [45 months (95% CI 39-54 months)] (Table 3).Table 3. Kaplan–Meier-derived estimates at 1-5 years—results shown for overall survival, time to second, third, and fourth treatment broken down by PARPi and BRCA statusCharacteristicOverall survival, yearsTime to second treatment, yearsTime to third treatment, yearsTime to fourth treatment, years12345123451234512345All patientsAll patients n = 364995% (94-96)82% (81-84)70% (68-71)59% (57-61)50% (47-52)71% (70-73)42% (40-44)33% (32-35)28% (26-30)24% (23-26)39% (36-41)18% (16-20)11% (9.1-13)8.4% (6.9-10)7.1% (5.6-9.0)26% (24-29)8.3% (6.6-10)4.6% (3.2-6.4)2.8% (1.7-4.8)1.4% (0.5-4.3)Receiving first-line PARPi n = 62198% (97-99)87% (85-90)74% (69-78)65% (60-71)57% (51-65)86% (83-89)52% (48-57)40% (35-45)32% (27-38)25% (19-32)24% (19-32)10.0% (5.9-17)7.1% (3.5-14)14% (8.6-23)5.2% (2.0-13)2.6% (0.5-14)2.6% (0.5-14)Not receiving first-line PARPi n = 3.02894% (94-95)81% (80-83)69% (67-71)58% (56-60)49% (46-51)68% (66-70)40% (38-42)32% (30-34)27% (25-29)24% (22-26)41% (38-43)19% (17-21)11% (9.5-13)8.9% (7.3-11)7.5% (5.9-9.5)28% (25-31)8.7% (6.9-11)4.8% (3.4-6.8)2.9% (1.6-5.0)1.4% (0.5-4.4)BRCA-positiveReceiving first-line PARPi n = 202100% (100-100)96% (93-99)87% (82-93)77% (68-86)72% (62-83)95% (91-98)76% (70-83)63% (55-72)49% (40-60)38% (27-53)26% (15-44)14% (5.7-34)14% (5.7-34)22% (9.9-50)Not receiving first-line PARPi n = 29799% (98-100)96% (94-98)90% (86-94)79% (74-85)70% (64-77)79% (74-84)45% (39-52)35% (30-42)30% (25-37)27% (22-34)66% (59-73)40% (33-49)28% (22-37)25% (18-33)21% (14-33)37% (27-49)12% (6.5-22)8.8% (4.1-19)6.6% (2.6-17)BRCA-negativeReceiving first-line PARPi n = 37697% (96-99)85% (81-89)68% (62-74)62% (55-69)52% (44-63)82% (78-86)41% (36-47)30% (25-36)25% (19-32)19% (12-30)24% (18-33)9.5% (5.1-18)4.7% (1.5-15)11% (5.4-21)5.4% (1.9-15)2.7% (0.5-15)2.7% (0.5-15)Not receiving first-line PARPi n = 209395% (94-96)83% (81-84)69% (67-72)57% (55-60)48% (45-51)67% (65-69)38% (36-41)30% (28-32)24% (22-26)21% (19-23)39% (36-42)17% (15-20)8.9% (7.2-11)6.5% (4.9-8.7)5.0% (3.4-7.3)28% (25-32)8.7% (6.6-11)4.9% (3.3-7.3)2.7% (1.3-5.4)1.8% (0.6-5.2)BRCA unknownReceiving first-line PARPi n = 4395% (89-100)71% (58-88)56% (39-79)42% (25-71)31% (14-68)81% (69-94)38% (24-59)14% (5.2-38)14% (5.2-38)21% (6.2-68)30% (6.3-100)Not receiving first-line PARPi n = 63890% (88-93)70% (66-74)56% (52-61)49% (44-54)40% (36-46)67% (63-71)44% (40-48)39% (35-43)35% (31-39)31% (27-36)31% (26-38)12% (8.3-18)9.0% (5.7-14)7.3% (4.3-13)7.3% (4.3-13)19% (13-28)6.0% (2.7-13)HRD, homologous recombination deficiency; PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitor.Expressed as an estimated percentage without the event of interest and the associated 95% confidence interval.
Treatment cross-over
Within the non-first-line PARPi cohort, 633 (21%) patients received later-line PARPi: 391 in the second-line setting, 134 in the third-line setting, 60 in the fourth-line setting, and 48 in the beyond-fourth-line setting (Figure 3).Figure 3Proportion of patients receiving PARPi by year of diagnosis and line of therapy—data only included where complete data for the year are available. PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitors.
Time to next treatment one (TTNT1)
The median TTNT1 for all patients receiving first-line PARPi was 26 months (95% CI 23-29 months), with a median TFI one (TFI1) of 20 months (95% CI 18-24 months). In contrast, patients not receiving first-line PARPi had a median TTNT1 of 18 months (95% CI 17-19 months) and a median TFI1 of 13 months (95% CI 12-14 months). Among patients with a BRCA mutation who received first-line PARPi, the median TTNT1 was 48 months (95% CI 42 months-NR), and the median TFI1 was 44 months (95% CI 36 months-NR), compared with 21 months (95% CI 19-26 months) and 16 months (95% CI 14-20 months) for those who did not receive first-line PARPi. Similarly, BRCA-negative patients receiving first-line PARPi had a median TTNT1 and TFI1 of 20 months (95% CI 19-23 months) and 14 months (95% CI 13-18 months), respectively, compared with 17 months (95% CI 17-18 months) and 12 months (95% CI 11-13 months) for BRCA-negative patients not receiving first-line PARPi. Patients with BRCA unknown status also demonstrated slight difference when treated with first-line PARPi, with a median TTNT1 of 19 months (95% CI 17-28 months) compared with 18 months among those not exposed to a first-line PARPi (95% CI 16-21 months) and a median TFI1 of 14 months (95% CI 8.6-23 months) compared with 13 months among those unexposed to first-line PARPi (95% CI 11-17 months).
Time to next treatment two (TTNT2)
A total of 1878 patients completed second-line therapy. The median TTNT2 for all patients receiving first-line PARPi was 7.8 months (95% CI 7.1-8.8 months), with a median TFI2 of 2.7 months (95% CI 1.8-3.6 months). In contrast, patients not receiving first-line PARPi had a median TTNT2 of 9.7 months (95% CI 9.2-10 months) and a median TFI2 of 3.9 months (95% 3.4-4.4 months). Among patients with a BRCA mutation who received first-line PARPi, the median TTNT2 was 7.6 months (95% CI 6.9-10 months), and the median TFI2 was 2.8 months (95% CI 1.8-5.5 months), compared with 17 months (95% 15-22 months) and 9.7 months (95% CI 7.3-13 months) for those who did not receive first-line PARPi. Similarly, BRCA-negative patients receiving first-line PARPi had a median TTNT2 of 7.8 months (95% CI 6.8-8.7 months) and TFI2 of 2.1 months (95% CI 1.4-3.6 months), respectively, compared with 9.4 months (95% CI 8.8-10 months) and 3.7 months (95% CI 3-4.3 months) for BRCA-negative patients not receiving first-line PARPi. Meanwhile, patients with BRCA unknown seemed to have more extended periods between treatments when receiving first-line PARPi, with a median TTNT2 of 11 months (95% CI 5.6 months-not reached) compared with 7.2 months (95% CI 6-8.6 months) and median TFI2 of 3.8 months (95% CI 2.7 months-not reached) compared with 2.5 months (95% CI 1.7-3.8 months).
Time to next treatment three (TTNT3)
A total of 1132 patients completed third-line treatment. The median TTNT3 for all patients receiving first-line PARPi was 4.9 months (95% CI 3.8-5.9 months), with a median TFI3 of 1.1 months (95% CI 0.9-1.5 months). In contrast, patients not receiving first-line PARPi had a median TTNT3 of 6.2 months (95% CI 5.8-6.9 months) and the median TFI3 was 1.7 months (95% CI 1.6-2.1 months). Among patients with a BRCA-positive mutation who received first-line PARPi, the median TTNT3 was 5.5 months (95% CI 3.9-14 months), and the median TFT3 was 1.1 months (95% CI 0.8-10 months), compared with 8.7 months (95% CI 6.7-12 months) and 2.3 months (95% CI 1.6-3.5 months) for those who did not receive first-line PARPi. Similarly, BRCA-negative patients receiving first-line PARPi had a median TTNT3 and TFI3 of 4.5 months (95% CI 3.2-5.9 months) and 1.1 months (95% CI 0.9-1.6 months), respectively, compared with 6.2 months (95% CI 5.9-6.9 months) and 1.6 months (95% CI 1.5-1.2 months) for BRCA-negative patients not receiving first-line PARPi. Meanwhile, there was a more prolonged clinical benefit seen for patients with BRCA unknown treated with first-line PARPi, with a median TTNT3 of 10 months (95% CI 3.2 months-NR) compared with 5.5 months (95% CI 4.6-6.5 months) and a median TFI3 of 2.2 months (95% CI 1.2 months-NR) compared with 1.6 months (95% CI 1.5-2.2 months).
Results by BRCA and HRD status
Further differences in the length of survival were seen when the population was broken down by HRD and BRCA status, as shown in Table 4.Table 4. Overall survival and median time to next treatment by BRCA and HRD statusCohortOverall survivalFirst to second treatmentSecond to third treatmentThird to fourth treatmentNumberNumber (events)MedianNumberNumber (events)Median time to next treatmentNumberNumber (events)Median time to next treatmentNumberNumber (events)Median time to next treatmentAll patients3649131260 (57-64)3647219019 (18-20)187814349.4 (9.0-9.9)11329226.0 (5.7-6.5)BRCA-positiveReceiving first-line PARPi52862 (46-not reached)521931 (23-not reached)18137.1 (4.2-not reached)1184.9 (1.9-not reached)Not receiving first-line PARPi531289 (89-not reached)533519 (15, 26)352520 (15, 30)22167.4 (5.6, 12)BRCA-negative but HRD-positiveReceiving first-line PARPi887>77 (not reached-not reached)883726 (22-not reached)35227.4 (6.2-23)20135.2 (3.1-10)Not receiving first-line PARPi1294660 (55-74)1299216 (14-20)876810 (8.6-13)63546.7 (5.3-9.5)BRCA-negative and HRD-negativeReceiving first-line PARPi51949 (49-not reached)513215 (13-22)31198.3 (4.9-not reached)17113.8 (2.9-not reached)Not receiving first-line PARPi2796761 (50-78)27915019 (16-23)1348810 (8.6-13)78615.9 (5.1-8.0)HRD, homologous recombination deficiency; PARPi, poly (adenosine-diphosphate ribose) polymerase inhibitor.
Discussion
This descriptive study analysed real-world outcomes in women with ovarian cancer who completed six or more cycles of platinum-based chemotherapy with and without first-line PARPi. While clinical trials have shown PARPi efficacy (olaparib, niraparib, and rucaparib) in improving PFS,10^,^18 these trials involve highly selected patients under strict protocols. Applying these findings to broader populations and determining optimal post-PARPi treatments remains challenging.
Standard care introduces PARPi as maintenance for BRCA-mutant high-grade serous, endometrioid or clear-cell ovarian cancers, followed by chemotherapy upon progression. However, concerns exist about shorter intervals between treatments, platinum resistance, and reduced efficacy, possibly due to overlapping resistance mechanisms between PARPis and platinum-based chemotherapy.19^,^21^,^27^,^28
Cross-resistance may arise from restoration of homologous recombination,29^,^30 secondary mutations restoring BRCA1/2 function,29^,^30 and enhanced DNA replication fork protection enabling tumour survival from either treatment.29 These mechanisms complicate relapse management and emphasise the importance of personalised, genetically informed treatment.
OS is a limited endpoint due to cross-over, post-progression therapy, and attrition. While some trials show OS improvement with PARPis, statistical significance is lacking, especially in some subgroups.11, 16 The PRIMA and PRIME trials showed no OS benefit13^,^30 highlighting the need for alternative endpoints and more nuanced evaluation based on molecular status.
Our study observed differences in OS, median TFI, and TTNT in PARPi-treated patients, predominantly in those with BRCA mutations. TTNT2 and TTNT3 were shorter in BRCA-mutated and wild-type patients receiving first-line PARPi, suggesting potential detriment in subsequent chemotherapy efficacy. Further research into the net benefit of PARPi and its impact on subsequent treatment outcomes is needed.
Results stratified by HRD status were heterogeneous due to the recent adoption of HRD testing and low patient numbers generating uncertain estimates.
Study limitations include missingness in HRD status, small PARPi-treated cohorts, and wide CIs. For example, only 69 out of 202 BRCA-positive patients receiving first-line PARPi had events during the first to second treatment interval, versus 190 out of 297 in the non-PARPi group. BRCA mutation types (BRCA1/BRCA2, somatic/germline) were not distinguished, potentially impacting outcomes. Immortal time bias may also skew results, as PARPi patients entered the cohort only after multiple chemo cycles, excluding early poor outcomes and inflating apparent benefit. We mitigated some of this by restricting the comparators to those receiving six platinum-based cycles through reduced cohort size and increased uncertainty. This study remains descriptive due to heterogeneous cohorts and limited data granularity. Lack of morphological details (e.g. high-grade versus low-grade serous) may explain difference in BRCA mutation prevalence between the PARPi treated group (13.8%) and PARPi untreated group (2.5%).
Real-world progression detection varies from trial protocols, potentially impacting treatment-free intervals and TTNT estimates. Future research should employ target trial type analysis, adjusting for confounders and expanding sample sizes, particularly for non-BRCA patients, to better understand PARPi impact.
Additional resistance factors include timing of progression relative to PARPi therapy and residual disease after surgery. Studies show these influence outcomes reinforcing the need for multi-variable analyses to identify predictors of post-PARPi resistance.31, 32, 33
This study responds to concerns that PARPi may drive platinum resistance, a causal question challenging to answer using observational data. Treatment decisions often reflect patient factors such as fitness, age, and comorbidity, introducing selection bias. Thus, our data cannot definitively explain reduced TTNT and TFI.
Although randomised controlled trials can mitigate bias, cross-over of treatment complicates analysis. This study, the largest real-world evaluation of PARPi-treated ovarian cancer patients to date, found shorter TTNT2, TTNT3, TFI2, and TFI3 in those receiving first-line PARPi. While causality is not proven, the trend is clear and warrants further investigation. We advocate for detailed reporting of post-first-line outcomes in clinical trials to better understand this pattern. Further studies should incorporate broader data including detailed – genetic, biological, and imaging to refine treatment strategies. Multicentre, multinational cohorts will be essential to ensure adequate sample size and representativeness of cohorts.
Conclusion
First-line PARPi patients had shorter TTNT and TFI intervals with differences by BRCA status. The findings suggest PARPi may impact subsequent treatment response and highlight the need for further research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H.Ferlay J.Siegel R.L.Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 71320212092493353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Dalmartello M.La Vecchia C.Bertuccio P.European cancer mortality predictions for the year 2022 with focus on ovarian cancer Ann Oncol 33320223303393509074810.1016/j.annonc.2021.12.007 · doi ↗ · pubmed ↗
- 3Siegel R.L.Miller K.D.Jemal A.Cancer statistics, 2017 CA Cancer J Clin 67120177302805510310.3322/caac.21387 · doi ↗ · pubmed ↗
- 4Peres L.C.Cushing-Haugen K.L.Köbel M.Invasive epithelial ovarian cancer survival by histotype and disease stage J Natl Cancer Inst 1111201960682971830510.1093/jnci/djy 071PMC 6335112 · doi ↗ · pubmed ↗
- 5Konstantinopoulos P.A.Ceccaldi R.Shapiro G.I.D’Andrea A.D.Homologous recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer Cancer Discov 5112015113711542646383210.1158/2159-8290.CD-15-0714 PMC 4631624 · doi ↗ · pubmed ↗
- 6Mc Guire W.P.Hoskins W.J.Brady M.F.Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer N Engl J Med 3341199616749456310.1056/NEJM 199601043340101 · doi ↗ · pubmed ↗
- 7Ledermann J.A.Matias-Guiu X.Amant F.ESGO–ESMO–ESP consensus conference recommendations on ovarian cancer: pathology and molecular biology and early, advanced and recurrent disease Ann Oncol 35320242482663830780710.1016/j.annonc.2023.11.015 · doi ↗ · pubmed ↗
- 8Pujade-Lauraine E.Ledermann J.A.Selle F.Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA 1/2 mutation (SOLO 2/ENGOT-Ov 21): a double-blind, randomised, placebo-controlled, phase 3 trial Lancet Oncol 1892017127412842875448310.1016/S 1470-2045(17)30469-2 · doi ↗ · pubmed ↗