Perioperative immunotherapy for advanced resectable melanoma: a cost-effectiveness analysis
Mingjun Rui, Qiran Wei, Yingcheng Wang, Joyce H.S. You

TL;DR
This study finds that giving immunotherapy before and after surgery for advanced melanoma is more cost-effective than giving it only after surgery.
Contribution
The study introduces a novel cost-effectiveness analysis comparing perioperative and adjuvant immunotherapy strategies for advanced resectable melanoma.
Findings
Perioperative nivolumab plus ipilimumab saved costs and improved quality-adjusted life-years compared to adjuvant nivolumab.
Perioperative pembrolizumab also saved costs and improved quality-adjusted life-years compared to adjuvant pembrolizumab.
Sensitivity analyses confirmed the robustness of the cost-effectiveness results.
Abstract
Recent studies have shown the efficacy of perioperative immunotherapy in improving the event-free survival of patients with advanced resectable melanoma. This study evaluated the cost-effectiveness of different perioperative immunotherapy treatment strategies versus adjuvant immunotherapy treatment strategies from the US payer perspective. Two immunotherapy strategies were each compared with the corresponding standard adjuvant treatment in two Markov models: Model (1) perioperative nivolumab plus ipilimumab versus adjuvant nivolumab for stage III patients; model (2) perioperative pembrolizumab versus adjuvant pembrolizumab for stage IIIB to IVC patients. Primary outcomes included direct costs, life-year gained (LYG), quality-adjusted life-year (QALY), and incremental cost per QALY (ICER). Sensitivity analyses were conducted to evaluate the robustness of the model outcomes. In…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
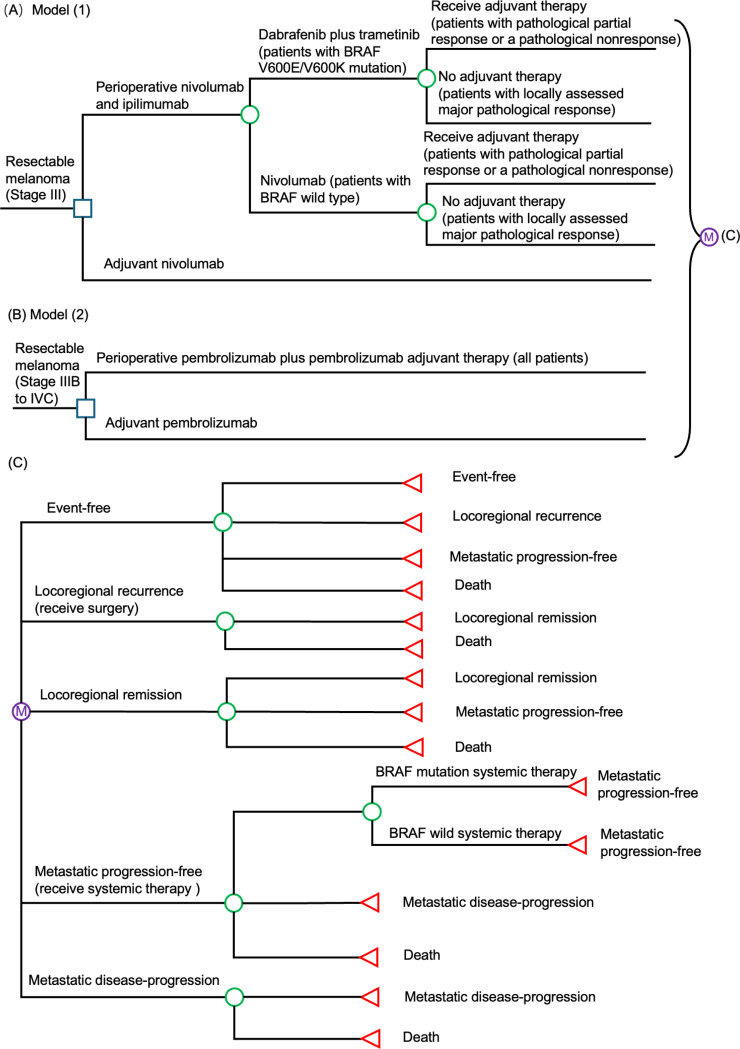 Figure 1
Figure 1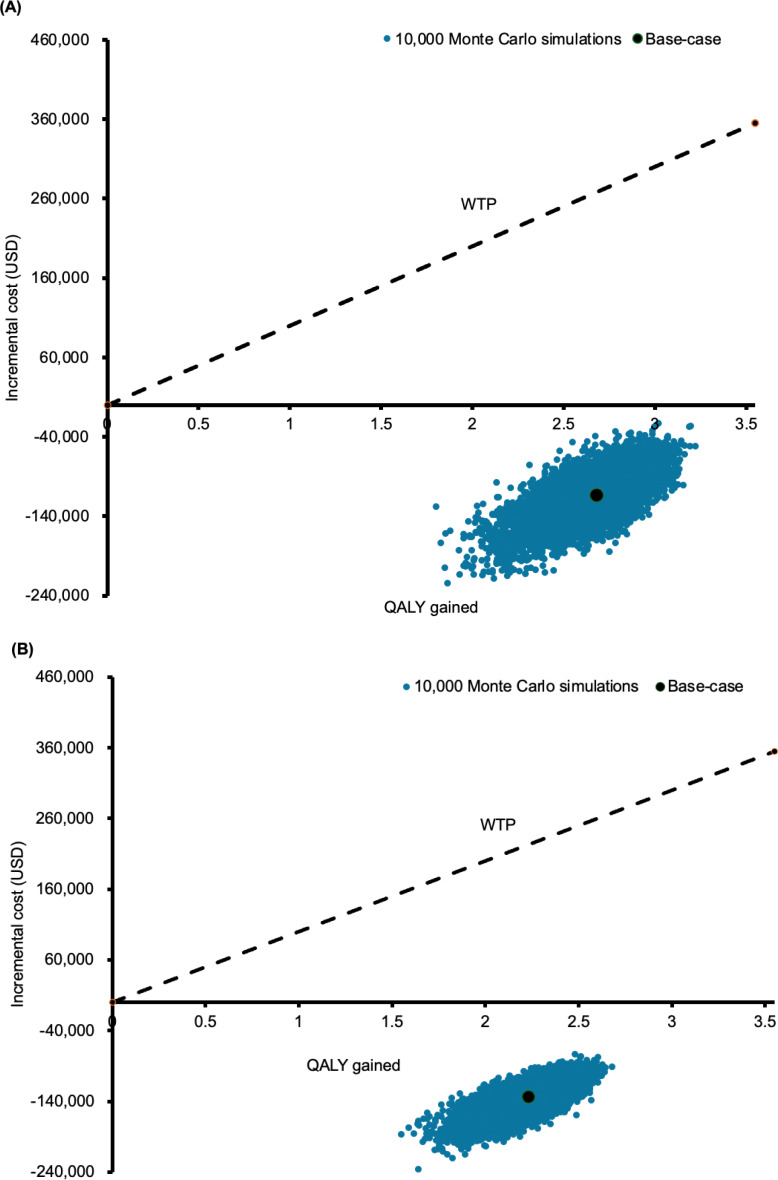 Figure 2
Figure 2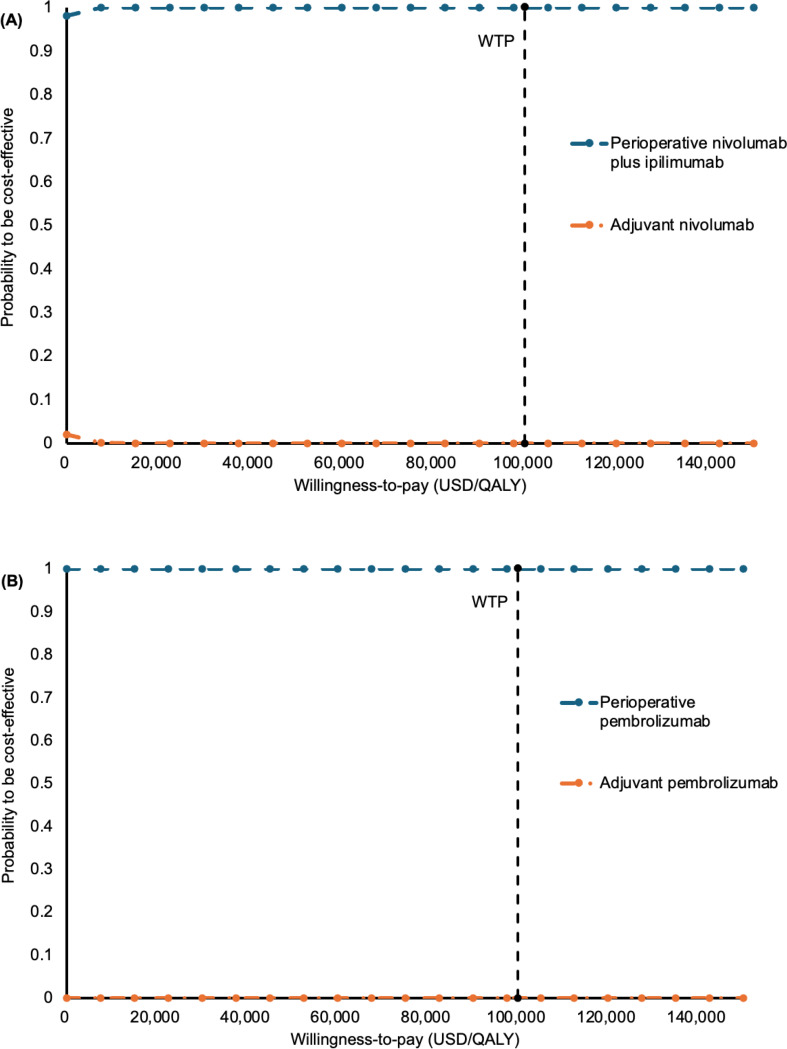 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Cancer Immunotherapy and Biomarkers · Immunotherapy and Immune Responses
Background
Melanoma is a kind of skin cancer that starts in the melanocytes. While stage II-IV melanoma is often treated with surgical resection, the risk of relapse ranges between 30% and 90% after complete resection [1, 2]. Globally, the incidence of melanoma has been rising, particularly among fair-skinned populations in high-income countries such as the United States [3]. The current standard of care for patients with resectable melanoma is complete surgical excision of the primary tumor and involved lymph nodes, plus adjuvant systemic therapy [4, 5]. Adjuvant systemic therapy includes immune checkpoint inhibitors (ICIs) such as anti-programmed cell death protein 1(PD-1) agents (nivolumab and pembrolizumab) and targeted therapy for B-Raf Proto-Oncogene, Serine/Threonine Kinase (BRAF)-mutant tumors (dabrafenib plus trametinib) [4, 6].
Recent studies have explored the role of immunotherapy in the perioperative setting for patients with resectable melanoma [7]. NADINA trial, a multinational phase 3 study conducted in Europe and Australia (n = 423), showed that neoadjuvant ipilimumab plus nivolumab (followed by surgery and response-adapted adjuvant therapy) significantly improved event free survival (EFS) when compared with surgery followed by standard adjuvant therapy in patients with resectable stage III melanoma, with a hazard ratio (HR) for progression recurrence or death of 0.32 (99.9% CI 0.15 to 0.66) [8]. In the SWOG S1801 trial (n = 313) conducted in the US, patients with stage IIIB to IVC melanoma who received neoadjuvant pembrolizumab followed by surgery and continued adjuvant therapy had significantly improved EFS when compared with surgery followed by adjuvant pembrolizumab alone, with a HR of 0.58 (95% CI 0.39 to 0.87) [9]. These findings supported the consideration of perioperative immunotherapy as a component of clinical management for patients with advanced melanoma.
The perioperative immunotherapy strategies with nivolumab plus ipilimumab and with pembrolizumab are associated with improved EFS, but the cost-effectiveness is yet to be investigated. To provide health economics evidence to assist the decision-making process of clinicians and healthcare payers, this study assessed the cost-effectiveness of two perioperative treatment strategies (nivolumab plus ipilimumab, and pembrolizumab) versus the current standard of care (adjuvant therapy) in patients with resectable melanoma from the US payer perspective.
Methods
Model design
Two Markov models (Fig. 1) were developed to simulate the clinical and health economic outcomes of two perioperative treatment strategies (nivolumab plus ipilimumab, and pembrolizumab), each versus the current standard of care (adjuvant therapy) in adult patients with (stage III to IVC) resectable melanoma. The study utilized Markov models to simulate patient progression between mutually exclusive health states. Health outcomes and costs were tallied for each cycle, determined by the specified transition probabilities [10]. The median age of patients with stage III to IVC resectable melanoma in the NADINA trial [8] and SWOG S1801 trial [9] ranged 60–63 years. The present models therefore applied 40 years (with weekly cycle) as the time horizon to allow adequate time for estimation of the lifelong outcome measures, including direct medical cost, life-year gained (LYG) and quality-adjusted life year (QALY) gained by each treatment strategy.
Two immunotherapy were each compared with the corresponding standard adjuvant treatment: Model (1) perioperative nivolumab plus ipilimumab versus adjuvant nivolumab for stage III patients; model (2) perioperative pembrolizumab versus adjuvant pembrolizumab for stage IIIB to IVC patients. Model (1) adopted the treatment regimens of the NADINA trial [8]: Neoadjuvant ipilimumab 80 mg plus nivolumab 240 mg every 3 weeks for 2 cycles, followed by a therapeutic lymph-node dissection. After surgery, those who had a pathological partial response or a pathological nonresponse were further treated with one of the two adjuvant therapies: dabrafenib 150 mg twice daily plus trametinib 2 mg once daily for 46 weeks as adjuvant therapy for patients with BRAF V600E/V600K mutation; nivolumab 480 mg every 4 weeks for 11 cycles in those with BRAF wild type melanoma. The adjuvant nivolumab group underwent a therapeutic lymph node dissection in week 0 followed by 12 cycles of adjuvant 480 mg nivolumab every 4 weeks starting between week 6 and 12. In model (2), the perioperative pembrolizumab group adopted regimens of the SWOG S1801 trial [9]: Neoadjuvant pembrolizumab 200 mg every 3 weeks for 3 cycles, followed by a therapeutic lymph-node dissection and post-surgery adjuvant therapy (pembrolizumab 200 mg every 3 weeks for 15 cycles). In the adjuvant pembrolizumab group, patients underwent surgery without prior neoadjuvant therapy. After surgery, patients received adjuvant therapy with pembrolizumab 200 mg every 3 weeks for 18 cycles [9].
The key health states in both Markov models were: Event-free, locoregional recurrence, locoregional remission, metastatic progression-free, metastatic disease-progression, and death. All patients entered the model at the health status of event-free, and transited to locoregional recurrence, metastatic progression-free, or all-cause death based on the strategy-specific weekly transition probabilities derived from results of clinical trials. One-time salvage surgery was used for those who entered the locoregional recurrence state, and the patients might achieve locoregional remission or die from all causes. Patients with locoregional remission might remain in remission, advance to metastatic progression-free, or die from all causes. When advancement to metastatic progression-free occurred, patients were managed by systemic therapy based upon the BRAF status [11]. Depending on the outcomes of systemic therapy, patients might transit to metastatic disease-progression or cancer-associated death.
Clinical inputs
The clinical model inputs are listed in Table 1. Literature search on MEDLINE (up to 2025) was performed using keywords including “resectable”, “stage III melanoma”, “stage IV melanoma”, “advanced melanoma”, “perioperative”, “neoadjuvant”, “adjuvant”, “event-free survival”, “nivolumab”, “pembrolizumab”, and “immunotherapy”. The selection criteria of clinical trials were: (1) Reports in English language; (2) adult patients with resectable melanoma; and (3) event-free survival was reported. Preferred studies were meta-analyses and randomized controlled trials. When multiple randomized trials were the source for a single model input, the base-case value was set as a weighted average. The upper and lower bounds for the sensitivity analysis were established using the highest and lowest values from these trials.
Table 1. Model inputsParametersBase-case valueRange for sensitivity analysisDistributionReferenceClinical inputsModel (1)Proportion of patients with BRAF V600E/V600K mutation0.450.39–0.66Beta[12]Proportion of BRAF V600E/V600K mutation patients with pathological partial response or pathological nonresponse0.530.42–0.64Beta[13]Proportion of BRAF wild type patients with pathological partial response or pathological nonresponse0.480.38–0.57Beta[13]Perioperative nivolumab and ipilimumab versus adjuvant nivolumabEFS hazard ratio for BRAF V600E/V600K0.290.11–0.79Beta[8]EFS hazard ratio for BRAF wild type0.350.12–1.03Beta[8]Gompertz distribution for EFSAdjuvant nivolumabBRAF V600E/V600K mutationShape-0.02525-0.04224-(-0.00826)Cholesky decomposition[8]Rate0.020620.01343–0.03166[8]BRAF wild typeShape-0.01980-0.03796-(-0.00163)Cholesky decomposition[8]Rate0.013730.00815–0.02313[8]Probability of ADEPerioperative nivolumab and ipilimumabDiarrhea3.8%3.0%-4.6%Beta[8]Rash3.3%2.6%-4.0%Beta[8]Adjuvant nivolumabDiarrhea0.6%0.5%-0.7%Beta[8]Rash2.4%0.0%-0.0%Beta[8]Model (2)Gompertz distribution for EFSPerioperative pembrolizumabShape-0.04236-0.06118-(-0.02355)Cholesky decomposition[9]Rate0.014080.00895–0.02215[9]Adjuvant pembrolizumabShape-0.01515-0.02412-(-0.00618)Cholesky decomposition[9]Rate0.013920.00982–0.01972[9]Probability of ADEPerioperative pembrolizumabDiarrhea0.7%0.6%-0.8%Beta[9]Rash0.9%0.7%-1.1%Beta[9]Vomiting0.9%0.7%-1.1%Beta[9]Adjuvant pembrolizumabDiarrhea0.8%0.6%-1.0%Beta[9]Rash3.1%2.5%-3.7%Beta[9]Vomiting3.1%2.5%-3.7%Beta[9]Models (1) and (2)Transition probability (weekly)From event-free to metastatic progression-freePerioperative nivolumab and ipilimumabBRAF V600E/V600K mutation0.00290.00261–0.00319Beta[8]BRAF wild type group0.00230.00207–0.00253Beta[8]Adjuvant nivolumabBRAF V600E/V600K mutation0.01060.00954–0.01166Beta[8]BRAF wild type group0.00700.00630–0.00770Beta[8]Perioperative pembrolizumab0.00690.00621–0.00759Beta[9]Adjuvant pembrolizumab0.00680.00612–0.00748Beta[9]From locoregional remission to metastatic progression-free0.010620.009558–0.011682Beta[17–19]Death (from event-free)0.000090.000081–0.000099Beta[17–19]Death (locoregional recurrence, or locoregional remission)0.000780.000702–0.000858Beta[17–19]Exponential distribution in patients with metastatic progression-free (rate):Progression-free survival for BRAF V600E/V600K0.002960.00269–0.00326Beta[22–24]Overall survival for BRAF V600E/V600K0.002850.00257–0.00317Beta[22–24]Progression-free survival for BRAF wild type0.004140.00376–0.00456Beta[22–24]Overall survival for BRAF wild type0.002370.00214–0.00264Beta[22–24]Hazard ratio (versus pembrolizumab)PFSDabrafenib + trametinib0.460.30–0.72Beta[22]Nivolumab + ipilimumab0.740.56–0.98Beta[22]OSDabrafenib + trametinib1.090.68–1.85Beta[22]Nivolumab + ipilimumab0.790.56–1.09Beta[22]Proportional for BRAF V600E/V600K patientsDabrafenib + trametinib68%FixedDirichlet[23]Nivolumab + ipilimumab19%[23]Pembrolizumab13%[23]Proportional for BRAF wild type patientsDabrafenib + trametinib0%FixedDirichlet[23]Nivolumab + ipilimumab71%[23]Pembrolizumab29%[23]Utility inputsEvent-free state0.91300.9040–0.9200Beta[26, 27]Locoregional recurrence state0.85800.833–0.884Beta[26, 27]Locoregional remission0.85800.81–0.846Beta[26, 27]Metastatic progression-free0.82800.551–0.629Beta[26, 27]Metastatic disease-progression0.59000.395–0.561Beta[28]Disutility for ADEDiarrhea-0.047-0.038-(-0.056)Beta[29]Rash-0.033-0.026-(-0.040)Beta[29]Vomiting-0.048-0.038-(-0.058)Beta[29]**Cost inputs (USD)**Dabrafenib (per mg)22–2Gamma[31]Trametinib (per mg)378303–454Gamma[31]Nivolumab (per mg)3226–39Gamma[32]Ipilimumab (per mg)180144–216Gamma[32]Pembrolizumab (per mg)5846–69Gamma[32]T-VEC (per mg)7056–84Gamma[31]BRAF testing (per time)463370–555Gamma[30]Disease management cost (per week)Event-free state238191–286Gamma[34, 35]Locoregional recurrence state261209–313Gamma[34, 36]Locoregional remission261209–313Gamma[34, 36]Metastatic progression-free1,102881-1,322Gamma[34, 36, 37]Metastatic disease-progression1,183947-1,420Gamma[34, 36, 37]Surgery (per time)11,1078,886 − 13,329Gamma[34]Systemic therapy (per patient) for BRAF V600E/V600K patients[a]556,052444,842 − 667,262Gamma[23, 34]Systemic therapy (per patient) for BRAF wild type patients[a]378,411302,729 − 454,093Gamma[23, 34]Costs for ADEDiarrhea8,6766,941 − 10,411Gamma[38]Rash3,1782,542-3,814Gamma[38]Vomiting5,2944,235-6,353Gamma[38]T-VEC: talimogene laherparepvec; ADE: adverse drug event; a: Systemic therapy included pembrolizumab, nivolumab, ipilimumab, nivolumab plus ipilimumab, dabrafenib plus trametinib, and encorafenib plus binimetinib. Details of systemic therapy cost estimation for BRAF V600E/V600K patients and BRAF wild type patients are shown in the Supplementary Materials
In model (1), the proportion of V600E/V600K mutation patients with melanoma was approximated from the findings of a US retrospective cohort study (n = 1112) on patients with melanoma [12]. The proportions of pathological partial response and pathological nonresponse for V600E/V600K mutation patients and BRAF wild type patients were approximated from a pooled analysis by the International Neoadjuvant Melanoma Consortium (INMC) which included six clinical trials of anti-PD-1-based immunotherapy or BRAF/MEK targeted therapy [13].
The EFS for each treatment strategy were estimated from the Kaplan-Meier event-free survival curves reported by the NADINA trial for model (1), and SWOG S1801 trial for model (2) [8, 9]. For both models, survival data points were extracted from the survival curves to generate patient-level data [14]. The EFS of all four immunotherapy strategies were extrapolated using Gompertz distribution (as the most appropriate distribution based upon the Bayesian information criterion, a visual inspection of fit, and the cure assumption) [15, 16]. Transition probabilities from the event-free to metastatic progression-free were estimated from reported findings of distant metastasis free survival [8, 9]. The transition from locoregional remission to metastatic progression-free was estimated from findings of the KEYNOTE-054 trial [17–19]. The reported survival of systemic therapy in BRAF-mutated and wild-type patients were not significantly different [20]. Exponential rates for progression-free survival and overall survival of patients with metastatic progression-free treated by systemic pembrolizumab therapy were first estimated from individual patient data from the KEYNOTE-006 trial [21]. Relative effects of nivolumab plus ipilimumab and dabrafenib plus trametinib adopted the HRs of corresponding regimens (versus pembrolizumab) reported by a network meta-analysis for both models [22]. Exponential rates for progression free survival and overall survival for patients with BRAF V600E or V600K mutations and for BRAF wild type patients were then estimated by applying HR from a network meta-analysis to survival rate derived from the KEYNOTE-006 trial and weighting these estimates according to the distribution of systemic therapies reported for each group [23]. Probabilities of adverse drug events (including diarrhea, rash and vomiting) were obtained from NADINA trial [8] (for model 1) and SWOG S1801 trial [9] (for model 2).
All-cause death in event-free, locoregional recurrence, and locoregional remission were approximated using the exponential rate of recurrence-free to death from the KEYNOTE-054 trial [17–19]. The cancer-associated mortality (as weekly probability of death) from metastatic progression-free and disease progression was derived from overall survival of patients receiving systemic therapy as estimated using the weighted and hazard adjusted survival curves [22–24]. Background mortality was incorporated by applying age-specific all-cause mortality rates from the United States population, derived from life table data [25].
Utility inputs
The utility inputs are shown in Table 1. The duration of patient-time spent in each health state and the corresponding utility (or disutility) value were used to determine QALY gained. The health state utilities of event-free, locoregional recurrence, locoregional remission, metastatic progression-free, and metastatic disease-progression were obtained from health-related quality-of-life and health economic evaluations of resected stage III melanoma in the US [26, 27]. The utility of metastatic disease-progression state was sourced from a cross-sectional population-based study on preference value for advanced melanoma health states [28]. Disutility values of adverse drug event (including diarrhea, rash and vomiting) were obtained from a health utility study using standard gamble method to elicit different grade III-IV toxicities commonly associated with chemotherapy treatments [29]. The cumulative QALY was discounted annually at a rate of 3%.
Costs inputs
The cost analysis was conducted on direct medical costs from the perspective of the US payer. Direct costs (Table 1) included drug costs (dabrafenib, trametinib, nivolumab, ipilimumab, pembrolizumab, T-VEC), surgery, BRAF testing, systemic therapy for metastatic progression-free in BRAF V600E/V600K mutation patients and BRAF wild type patients, disease management and adverse event treatment in each health state. The cost of BRAF testing was retrieved from Centers for Medicare & Medicaid Services (CMS) Clinical Laboratory Fee Schedule 2024 [30]. The drug costs of dabrafenib, trametinib and T-VEC were estimated from Medicare Part D Monthly Prescription Drug Plan Formulary and Pharmacy Network Information [31]. The drug costs of nivolumab, ipilimumab, pembrolizumab were estimated from the Medicare Part B Drug Average Sales Price data [32]. The cost of surgery was estimated from the CMS Hospital Outpatient PPS (2022) [33]. The costs of systemic therapy for metastatic progression free disease were estimated separately for patients with BRAF V600E or V600K mutations and for BRAF wild type patients, reflecting differences in available treatment options between the two groups. For BRAF mutated patients, systemic therapy options included pembrolizumab, nivolumab plus ipilimumab, and dabrafenib plus trametinib, whereas BRAF wild type patients were assumed to receive pembrolizumab or nivolumab plus ipilimumab regimens. Treatment specific costs were obtained from US-based cost-effectiveness analyses of metastatic melanoma and combined using weighted averages according to the distribution of systemic therapies reported for each group [23, 34]. Details of the estimation of systemic therapy costs for metastatic disease are showed in Supplementary Materials. Disease management costs for event-free, locoregional recurrence, locoregional remission, metastatic progression-free, and metastatic disease-progression states were derived from the US-based cost-effectiveness analyses and retrospective healthcare database studies [34–37]. The management costs of prominent symptomatic adverse events (including diarrhea, rash and vomiting) were derived from an economic burden study of AEs in cancer care [38]. All cost inputs were converted to year 2025 US dollars using the CCEMG–EPPI Centre Cost Converter v.1.7 [39]. The cumulative costs were discounted with an annual rate of 3%.
Model validation
Internal validation was conducted by comparing modeled EFS for each treatment arm with the Kaplan Meier curves observed in clinical trials. For the comparison of perioperative nivolumab plus ipilimumab versus adjuvant nivolumab in model (1), the EFS Kaplan Meier curves were derived from the NADINA trial [8]. For the comparison of perioperative pembrolizumab versus adjuvant pembrolizumab in model (2), the EFS Kaplan Meier curves were obtained from the SWOG S1801 trial [9]. The results of the internal validation were presented in the Supplementary Materials Figure S1A and Figure S1B. External validation was performed by comparing modeled overall survival outcomes for all arms with predictions reported in three published and validated economic evaluation models [19, 27, 34]. The results of the external validation were presented in Supplementary Materials Figure S2.
Cost-effectiveness and sensitivity analyses
The analyses were performed using TreeAge Pro 2025 (TreeAge Software Inc., Williamstown, MA) and Microsoft Excel 16.9 (Microsoft Corporation, Redmond, WA, USA). A treatment option was considered dominated if it resulted in lower QALY at a higher cost versus an alternative, and the dominated option was excluded from further cost-effectiveness evaluation. When a treatment option yielded higher QALY at an increased cost versus an alternative, the incremental cost-effectiveness ratio (ICER) of the more effective option was calculated by the equation: Δcost/ΔQALY. The present analysis adopted 100,000 USD/QALY as the willingness-to-pay (WTP) threshold in the base-case analysis. A treatment option was cost-effective if (1) it gained higher QALY with cost-saving, or (2) it gained higher QALY at increased cost and the ICER was less than the WTP threshold.
A one-way sensitivity analysis was performed on all model inputs to determine the influence of each parameter and to identify critical threshold values. All the parameters were varied over the upper and lower limits, if available. Otherwise, a 95% confidence interval or a range of variation by ± 20% of the base-case value was used. The probabilistic sensitivity analysis was performed using Monte Carlo simulation. The direct cost and QALY of each study arm were recalculated 10,000 times by randomly drawing each of the model inputs from the probability distribution specified in Table 1. The incremental costs and incremental QALY of the 10,000 simulations were presented in scatter plots, and probability to be the cost-effective alternative was evaluated in acceptability curves over a wide range of WTP from 0 to 150,000 USD/QALY.
Results
Base-case analysis
Expected total direct medical cost (with breakdown costs in perioperative treatment, before recurrence and after recurrence), QALY, LYG, incremental cost and incremental QALY are shown in Table 2. In model (1), perioperative nivolumab plus ipilimumab (versus adjuvant nivolumab) gained higher QALY (by 2.73) with cost-saving (by USD109,157), and were accepted as cost-effective. Compared with adjuvant nivolumab, the breakdown cost of perioperative treatment and cost before recurrence were higher, while the cost after recurrence was lower in the perioperative nivolumab plus ipilimumab arm.
Table 2. Base-case analysis of direct medical cost, QALY and LYG, increment cost, incremental QALY and incremental cost per QALY gained (ICER)StrategyTotal Cost (USD)Cost in perioperative treatment (USD)Cost before recurrence (USD)Cost after recurrence (USD)Total QALYTotal LYGIncremental cost (USD)Incremental QALYICERs (USD per QALY)neoadjuvant treatmentsurgeryadjuvant treatment Stage III resectable melanoma (model 1) Adjuvant nivolumab421,681-6,364149,5046,145259,6688.9010.35---Perioperative nivolumab and ipilimumab312,52545,5576,214138,7339,737112,28411.6213.00-109,1572.73Cost-saving Stage IIIB to IVC resectable melanoma (model 2) Adjuvant pembrolizumab459,633-6,384161,2606,129285,8607.909.33---Perioperative pembrolizumab329,47634,3465,828129,69718,998140,60710.1911.49-130,1572.29Cost-savingLYG: life-year gained; QALY: quality-adjusted life-year
In model (2), perioperative pembrolizumab (versus adjuvant pembrolizumab) gained higher QALY (by 2.29) with cost-saving (by USD130,157), and were accepted as cost-effective. The breakdown cost of perioperative treatment and cost before recurrence were higher, whilst the cost after disease recurrence were lower in the perioperative pembrolizumab group.
Sensitivity analysis
One-way sensitivity analysis found that the base-case results were robust to variation of all model inputs at the WTP threshold 100,000 USD/QALY. The probabilistic sensitivity analysis was performed by 10,000 Monte Carlo simulations. In model (1), the perioperative nivolumab plus ipilimumab (versus adjuvant nivolumab) gained additional 2.6610 QALY (95% CI 2.6571–2.6650 p < 0.01) with a cost-saving of USD 114,826 (95% CI 114,268 − 115,385 p < 0.01). The perioperative nivolumab plus ipilimumab was accepted as cost-effective in 100% of the 10,000 simulations (Fig. 2A). In model (2), the perioperative pembrolizumab (versus adjuvant pembrolizumab) gained additional 2.2461 QALY (95% CI 2.2430–2.2492 p < 0.01) with a cost-saving of USD 133,625 (95% CI 133,220 − 134,030 p < 0.01). The perioperative pembrolizumab was accepted as cost-effective in 100% of the 10,000 simulations (Fig. 2B).
To examine the acceptability of perioperative nivolumab plus ipilimumab versus adjuvant nivolumab (model 1) and perioperative pembrolizumab versus adjuvant pembrolizumab (model 2), the probabilities of each perioperative strategy to be accepted as cost-effective were shown in the acceptability curves over a wide range of WTP (0–150,000 USD/QALY) (Fig. 3A-B).
Discussion
The present cost-effectiveness analysis evaluated two perioperative immunotherapy strategies (each versus adjuvant immunotherapy strategies) for patients with resectable melanoma. Our findings showed perioperative nivolumab plus ipilimumab and perioperative pembrolizumab to gain higher QALY with cost-savings when compared to adjuvant nivolumab and adjuvant pembrolizumab, respectively. Breakdown costs showed that the lower total costs observed in the perioperative nivolumab plus ipilimumab and perioperative pembrolizumab groups were primarily driven by lowering the cost after recurrence. Improved event free survival led to reduced use of subsequent systemic therapies for recurrence. The cost-effectiveness of perioperative nivolumab plus ipilimumab was further enhanced by the response-adapted treatment approach, whereby patients who had achieved pathological complete response did not proceed to receive adjuvant therapy, thus resulted in reduced adjuvant treatment cost. One-way sensitivity analysis found that the base-case results were robust to variation of all model inputs for both perioperative nivolumab plus ipilimumab versus adjuvant nivolumab (model 1) and perioperative pembrolizumab versus adjuvant pembrolizumab (model 2). The probabilistic sensitivity analysis supported the base-case findings to be highly robust that the perioperative nivolumab plus ipilimumab (versus adjuvant nivolumab) and perioperative pembrolizumab (versus adjuvant pembrolizumab) were cost-effective in 100% of times at WTP of 100,000 USD/QALY.
A prior cost-effectiveness study found that pembrolizumab (as adjuvant therapy) was cost-effective for resected stage IIB or IIC melanoma when compared with (observation without adjuvant therapy) in the United States [34]. Another US study evaluated the cost-effectiveness of adjuvant pembrolizumab relative to observation alone following complete resection of high-risk stage III melanoma [27]. The adjuvant pembrolizumab was found to be highly cost-effective versus observation alone. A cost-effectiveness analysis evaluated the cost-effectiveness of pembrolizumab versus other adjuvant treatment strategies (routine observation or ipilimumab in the overall population; dabrafenib + trametinib in the BRAF subgroup) for resected high-risk stage III melanoma in the US, and reported that pembrolizumab was cost-effective [40]. Our findings showed that both perioperative nivolumab plus ipilimumab (versus adjuvant nivolumab) and perioperative pembrolizumab (versus adjuvant pembrolizumab) were accepted as cost-effective, consistent with findings of the prior studies.
Perioperative nivolumab plus ipilimumab strategy avoided overtreatment with adjuvant therapy (thus reducing costs), by using pathological response to determine the need for adjuvant therapy, and V600E/V600K mutation status to guide the use of targeted adjuvant therapy [8, 9]. Pathological response is a strong surrogate marker for long-term benefit, as demonstrated by clinical trials included in the pooled analysis by the INMC [13]. In addition, the OpACIN-neo trial demonstrated that neoadjuvant nivolumab plus ipilimumab provided durable survival benefits without the need for subsequent adjuvant systemic therapy [41, 42]. The PRADO trial also supported the omission of adjuvant therapy in patients achieving a major pathological response without compromising outcomes [43]. Furthermore, in the neoadjuvant nivolumab plus ipilimumab group, patients with V600E/V600K mutations received targeted therapy. Real-world studies have suggested that adjuvant targeted therapy may be associated with better outcomes (comparing to immunotherapy) in patients with V600E/V600K mutated melanoma [44]. Further research is warranted to investigate the role of prognostic markers for guiding adjuvant treatment selection and optimizing long-term outcomes in the future. In model (2), perioperative pembrolizumab was cost-saving versus adjuvant pembrolizumab, primarily due to improved event free survival, thus lower the cost after recurrence. Although response-adapted discontinuation of adjuvant therapy following neoadjuvant pembrolizumab was not evaluated in the SWOG S1801 trial [9], such approach may be considered in clinical practice. Incorporating response-adapted strategies for perioperative pembrolizumab is likely to further improve its cost effectiveness and should be explored in future studies.
This study has several limitations. The present study conducted cost-analysis from a payer’s perspective, indirect costs related to productivity loss or caregiver burden were not considered, and might have underestimated the benefits of the perioperative immunotherapy. The current analysis was limited to within trial comparisons (as network meta-analysis was not conducted due to lacking common comparator). The clinical model inputs were extracted from clinical trials, and the heterogeneity of patient characteristics might affect the generalizability of the model results to clinical practice. Rigorous sensitivity analysis on all model inputs was therefore conducted to examine the robustness of model results, and no influential factor was identified.
Conclusion
Perioperative nivolumab plus ipilimumab and perioperative pembrolizumab appear to gain additional QALY at lower cost when compared with adjuvant immunotherapies for patients with stage III and stage IIIB to IVC resectable melanoma, respectively, from the US payer perspective.
Fig. 1. Simplified model for each strategy; (A) Perioperative nivolumab plus ipilimumab versus adjuvant nivolumab for stage III resectable melanoma; (B) Perioperative pembrolizumab versus adjuvant pembrolizumab for stage IIIB to IVC resectable melanoma; (C) Markov model structure of resectable melanoma
Fig. 2. Scatter plots of incremental cost against QALY gained by (A) perioperative nivolumab plus ipilimumab versus adjuvant nivolumab; (B) perioperative pembrolizumab versus adjuvant pembrolizumab; QALY: quality-adjusted life-year; WTP: willingness-to-pay = 100,000 USD/QALY
Fig. 3. Acceptability curves of (A) perioperative nivolumab plus ipilimumab versus adjuvant nivolumab; (B) perioperative pembrolizumab versus adjuvant pembrolizumab to be cost-effective against willingness-to-pay; QALY: quality-adjusted life-years; WTP: willingness-to-pay
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yushak M, Chapman P, Robert C, Kudchadkar R. Systemic therapy options for patients with unresectable melanoma. Am Soc Clin Oncol Educational Book. 2017;37661–72. 10.1200/edbk_174934.10.1200/EDBK_17493428561662 · doi ↗ · pubmed ↗
- 2Rutherford M, Sweeting M. NICE DSU technical support document 21: flexible methods for survival analysis [Internet]. 2020 [cited 2026 Jan 2]. Available from: http://nicedsu.org.uk/wp-content/uploads/2020/11/NICE-DSU-Flex-Surv-TSD-21_Final_alt_text.pdf.
- 3NICE. NICE DSU technical support document 19. Partitioned survival analysis for decision modelling in health care: A critical review. https://pure.york.ac.uk/portal/en/publications/nice-dsu-technical-support-document-19(4abca 204-a 8a 5-4880-9cce-190049 a 1daf 9).html
- 4Statistics N Cf H. Mortality in the United States. 2023 Dec 16;2024. https://www.cdc.gov/nchs/products/databriefs/db 521.htm
- 524CLABQ 1. Centers for Medicare & Medicaid Services. https://www.cms.gov/medicare/payment/fee-schedules/clinical-laboratory-fee-schedule-clfs/files/24clabq 1. Accessed 01/10, 2024.
- 6Monthly Prescription Drug Plan Formulary and Pharmacy Network Information. Centers for Medicare & Medicaid Services. https://data.cms.gov/provider-summary-by-type-of-service/medicare-part-d-prescribers/monthly-prescription-drug-plan-formulary-and-pharmacy-network-information. Accessed 01/10, 2024.
- 7Medicare Part B. Drug average sales price. https://www.cms.gov/medicare/payment/fee-for-service-providers/part-b-drugs/average-drug-sales-price.
- 8Hospital Outpatient CMS. PPS 2022. https://www.cms.gov/medicare/payment/prospective-payment-systems/hospital-outpatient.