Educating during the COVID-19 Pandemic: An Educator Perspective on Mental Health
Alyssa Schneider Carlson, Zoe Sirotiak, Stephanie Orellana, Emily B. K. Thomas

TL;DR
This paper explores how the pandemic affected educators' mental health and work environments, highlighting increased stress and a lack of decision-making power.
Contribution
The study provides new insights into educators' mental health and occupational challenges during the pandemic through a large-scale survey.
Findings
Educators reported increased stress (38.0%) and feelings of isolation (45.9%).
Many felt increased work responsibilities (34.0%) and unaddressed concerns (28.2%).
A lack of decision-making agency was a systemic issue reported by educators.
Abstract
During the COVID-19 pandemic, educators were impacted across domains of psychological, physical, social, and occupational health. Occupational environments, including classrooms, changed significantly due to COVID-19. This study aimed to characterize the nuanced experience of educators during the COVID-19 pandemic. Participants included 918 United States educators (e.g., teachers, paraeducators, support professionals, and administrators). Educators completed the survey via Qualtrics during November and December of 2020. The survey included eight qualitative questions, and responses were randomized to inductive or deductive datasets for analyses. Our deductive results showed that individuals reported changes in several facets of health, with educators reporting increases in stress (38.0%) and feelings of isolation (45.9%). Our results also showed impacted occupational health, citing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
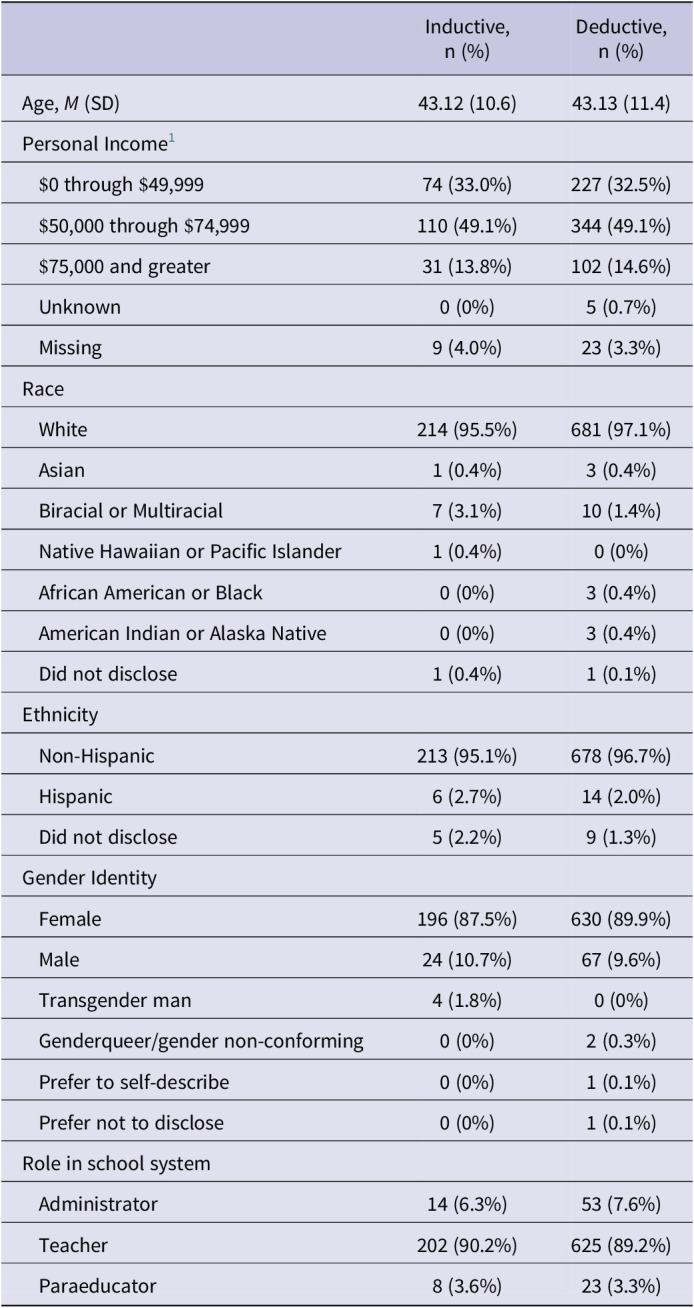 Figure 1
Figure 1 Figure 2
Figure 2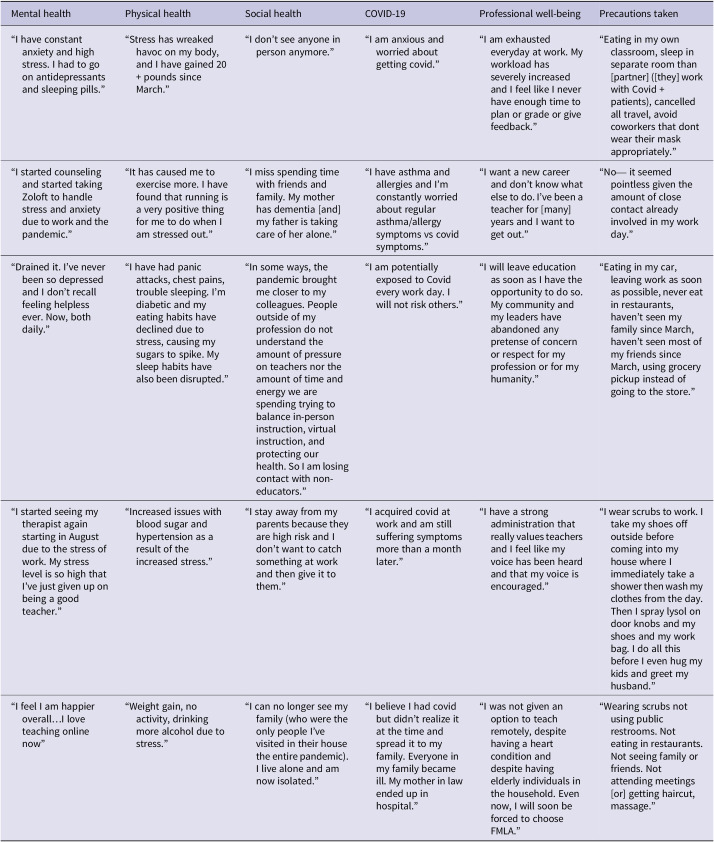 Figure 3
Figure 3- —National Institute of General Medical Scienceshttps://doi.org/10.13039/100000057
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Education, Leadership, and Health Research · Digital Education and Society
Background
The COVID-19 pandemic has adversely impacted global health.1 COVID-19 infections caused widespread mortality, with over 7 million deaths worldwide.2 Symptoms of COVID-19 infection include fever, cough, shortness of breath, fatigue, headache, pain, sore throat, congestion, nausea, and diarrhea.3 Physical symptoms may remain significant and impairing following infection, including fatigue, reduced exercise capacity, and decreased ability to perform physical roles.4 ^,^5 The pandemic has impacted mental health, characterized by increased psychological distress,6 as well as psychiatric symptoms, such as depression, anxiety, and posttraumatic stress disorder.6 ^–^9 Downstream effects of the COVID-19 pandemic, including social isolation, financial stressors, health risk, and lifestyle changes, also impacted mental health.10 ^–^12
The occupational environment has also changed significantly across multiple industries. Workers experienced significant changes, including working from home, face covering implementation, physical barrier assembly, and improved ventilation.13 These changes have been associated with a decrease in life satisfaction.14 Factors associated with occupational environmental stressors include fear of infection or infecting others, job strain, periods of quarantine or isolation, perception of worker rights exploitation, and uncertainty.15
The mental health impacts of the COVID-19 pandemic have not been uniform across occupational groups. Essential workers, defined as those whose jobs necessitated in-person work, reported significant fear, stress, anxiety, depression, insomnia, burnout, and distress.16 ^–^18 In addition to being more likely to become infected and die from COVID-19,19 ^,^20 essential workers faced other adversities, such as a lack of personal protective equipment, staff shortages, challenges with enforcing regulations, and delays.17 ^,^19 ^,^21 ^,^22 Moreover, when lockdowns were enforced in the USA, testing was largely available to symptomatic or exposed individuals, contributing to stress about asymptomatic spread among essential workers.23 Essential health care workers reported high levels of fear, anxiety, depression, and trauma related to the pandemic, leading to burnout and feeling unable to ensure patient safety.24 A qualitative study performed with health care workers identified inadequate preparedness, emotional challenges, insufficient equipment and information, and work burnout as related to the pandemic.24
Educators are a group of essential workers who were significantly impacted throughout the COVID-19 pandemic. Educators are defined as teachers, administrators, paraeducators, and support professionals. Research has demonstrated that teachers reported high rates of anxiety, depression, stress, and burnout related to the COVID-19 pandemic.25 ^–^28 Many educators were expected to continue teaching, and the struggles of USA educators were outlined in an American Psychological Association (APA) technical report,29 which indicated that many educators desired to transfer or quit education, received verbal threats of violence, and experienced physical aggression from students. A related policy brief emphasized that investigating psychological symptoms among educators has never been more timely.30
Factors that contribute to the development of psychological distress and disorder have been identified among educators. Lack of collegial support, fear of verbal or physical abuse, significant workload, student behavior, and poor employment conditions were associated with depression, anxiety, and poor mental health.31 ^–^33 Among USA educators, increased stressors during the COVID-19 pandemic were related to poorer mental health, and poor mental health was associated with increased difficulty coping and teaching.34 Additionally, most Wisconsin, USA, educators reported clinically significant depressive and anxiety symptoms.35 Moreover, schoolteachers in Australia reported worsened mental health, citing contributors including increased responsibilities, changes in ways of working, and difficult working conditions.16 In Poland, educators reported at least mild levels of stress, anxiety, and depression, noting contributing factors including blurred professional and personal boundaries and isolation.36 The transition from in-person to remote teaching contributed to poorer mental health, with remote teaching associated with higher levels of distress than in-person37; however, other work has demonstrated high depressive and anxiety symptoms that did not differ based on teaching modality.38 Increased workload due to lockdown was suggested as a potential cause of worsened educator mental health.39 Uncertainty, increased workload, negative perception of the profession, concern for the well-being of others, health struggles, and juggling multiple roles were related to poor mental health among educators in England.40
Although quantitative research offers distinct advantages, qualitative and mixed methods research provides nuanced perspectives and context regarding individual experiences of collective events. Specifically, qualitative research methods can clarify the lived experience of individuals.41 Qualitative research may be particularly helpful in characterizing the lived experience of mental health difficulties.42 COVID-19 and the mental health challenges that it poses may be particularly conducive to qualitative investigation.43 Even though educators were among the essential workers faced with significant changes and dangers related to COVID-19, qualitative research investigating the effects of the COVID-19 pandemic on educators is limited. Given that many individual and societal experiences secondary to COVID-19 are novel, qualitative investigations are critical to provide contextual nuance. The APA policy brief30 and technical brief29 included both qualitative and quantitative data, further emphasizing the importance of both methods to capture educator experiences more fully during the COVID-19 pandemic. In response to the APA reports and the gap in the current literature, this study aims to understand how the COVID-19 pandemic has impacted mental, physical, occupational, and social health among educators.
Method
Participants
Participants (n = 918) were English-reading/speaking adults in the USA who identified as an educator (e.g., teacher, paraeducator, administrator) from kindergarten through college. The average age of the sample was 43 years (SD = 11.3). Most identified as White (96.6%) and female (87.8%). At least one person participated from 46 states of the USA. To be included in the qualitative analyses, a response to one of the 8 qualitative questions was required. There were 145 participants who were excluded due to lack of qualitative response, leaving a sample of 925. Participant responses were randomized into 2 samples for analyses: inductive and deductive. See the demographic characteristics of the two samples in Table 1.Table 1.Descriptive characteristics of the inductive(n = 224) and deductive samples (n = 701)Inductive, n (%)Deductive, n (%)Age, M (SD)43.12 (10.6)43.13 (11.4)Personal Income1 49,99974 (33.0%)227 (32.5%) 74,999110 (49.1%)344 (49.1%) $75,000 and greater31 (13.8%)102 (14.6%) Unknown0 (0%)5 (0.7%) Missing9 (4.0%)23 (3.3%)Race White214 (95.5%)681 (97.1%) Asian1 (0.4%)3 (0.4%) Biracial or Multiracial7 (3.1%)10 (1.4%) Native Hawaiian or Pacific Islander1 (0.4%)0 (0%) African American or Black0 (0%)3 (0.4%) American Indian or Alaska Native0 (0%)3 (0.4%) Did not disclose1 (0.4%)1 (0.1%)Ethnicity Non-Hispanic213 (95.1%)678 (96.7%) Hispanic6 (2.7%)14 (2.0%) Did not disclose5 (2.2%)9 (1.3%)Gender Identity Female196 (87.5%)630 (89.9%) Male24 (10.7%)67 (9.6%) Transgender man4 (1.8%)0 (0%) Genderqueer/gender non-conforming0 (0%)2 (0.3%) Prefer to self-describe0 (0%)1 (0.1%) Prefer not to disclose0 (0%)1 (0.1%)Role in school system Administrator14 (6.3%)53 (7.6%) Teacher202 (90.2%)625 (89.2%) Paraeducator8 (3.6%)23 (3.3%)
Procedures
Potential participants clicked a link to the survey, which directed them to the survey at qualtrics.com. Congruent with the institutional review board (IRB)-approved protocol, the first page of the survey was a consent letter notifying participants that clicking to the next page indicated consent to participate. The consent specified that participation was voluntary, that the data would be stored on a secure computer drive, and that information provided by participants would not be identifiable. This protocol was approved by the University of Iowa IRB, approval #202007406. Both recruitment and data collection procedures are further detailed alongside quantitative findings.38 The qualitative questions that were included are listed below.
- How has your role as an educator during the pandemic impacted your ability to do your job day-to-day?
- How has your role as an educator during the pandemic impacted your professional advancement and career goals?
- How has your role as an educator during the pandemic impacted your mental health?
- How has your role as an educator during the pandemic impacted your physical health?
- How has your role as an educator during the pandemic impacted your social health?
- Do you feel that your school community was receptive and/or responsive to your preferences for educating during the COVID-19 pandemic?
- Were your preferences solicited by a school board, administrative body, county governance, or state governance, and if so, did these preferences appear to be considered in decision-making processes?
- Please feel free to speak to the degree to which you felt your voice as an educator was valued during the pandemic.
Data Analysis
The dataset was divided into an inductive and deductive cohort, using random assignment with a 1:3 scheme (inductive: deductive). In the inductive phase, randomly selected participants were utilized for coding. The purpose of this phase was to develop codes, identify themes, and identify representative data to support codes and themes.44 The deductive phase utilized the inductive codes for deductive coding of the data. The purpose was to allow for a structured, systemic analysis to enhance the validity of codes and themes.45 Four coders were involved in analyses. Each coder reviewed all responses to qualitative questions in the inductive dataset. A thematic discussion resulted in the development of relevant codes. Responses to each question were reviewed sequentially to ensure independent consideration for thematic extraction.
The data analytic plan and hypotheses were pre-registered through Open Science Framework (OSF) prior to randomization of responses.46
Thematic Analysis and Codebook Formation
The themes were formulated based on responses to the 8 qualitative questions, and codes were formed across questions. After identification of themes and the codebook, the inductive dataset was coded by all coders. All codes were reviewed iteratively for accuracy, clarity, and agreement.
Inductive data analyses
In code generation, coders noted themes of interest.47 Individual extractions were collated into themes, ensuring that all data relevant to a theme were included.47 Coders reviewed codes and themes for coherence, accuracy, and refinement.47
Deductive data analyses
Responses were randomly assigned to coders. The deductive codes are reported for interpretation. In addition to random assignment, 30% of each coders’ data were randomly selected for double coding to ensure agreement between coders. All discrepancies were resolved through discussion until agreement was reached.45 ^,^48
Results
The results demonstrate that this sample reported declines in physical, mental, and social health, as well as challenges in their professional environment. Educators reported not feeling that their voices were being heard regarding implemented workplace policies. Educators reported taking precautionary measures personally and professionally to prevent infection or spread of COVID-19.
When individuals were recorded as having “not reported” a code, this means that it was not mentioned explicitly. When a participant was recorded as having “reported” a code, this experience was explicitly mentioned and was available for coding. See Table 2 for theme frequencies in each phase.Table 2.Frequencies of inductive and deductive codesInductive, n (%)Deductive, n (%)Fear of COVID–19 infection53 (24.0%)82 (11.6%)Fear of spreading COVID–1951 (14.4%)93 (13.1%)COVID–19 exposure Exposed through work9 (2.5%)29 (4.1%) Exposed to COVID–19, unspecified origin4 (1.1%)6 (0.8%)COVID–19 infection Contracted COVID–19 at work4 (1.1%)4 (0.6%) Infected with COVID–19, unspecified origin5 (1.4%)6 (0.8%)Limited social interaction271 (76.8%)510 (72.0%)Family time Less time with family64 (18.1%)106 (15.0%) More time with family2 (0.6%)3 (0.4%)Lack of connection or feeling isolated65 (18.4%)197 (27.8%)Forgoing activities Choosing not to attend a general category of activities176 (49.9%)325 (45.9%) Not attending specific events9 (2.5%)19 (2.7%)Virtual activity (i.e., engaged in virtual activity, e.g., Zoom)113 (32.0%)211 (29.8%)Exercise or physical activity Decreased63 (17.8%)116 (16.4%) Increased15 (4.2%)35 (4.9%)Increased sedentary behavior43 (12.2%)64 (9.0%)Increased alcohol consumption6 (1.7%)5 (0.7%)Increased self-care16 (4.5%)14 (2.0%)Weight changes Weight gain43 (12.2%)88 (12.4%) Weight loss4 (1.1%)17 (2.4%)Diet changes Negative changes in diet33 (9.3%)69 (9.7%) Positive changes in diet1 (0.3%)11 (1.6%)Sleep changes Sleeping less21 (5.9%)27 (3.8%) Sleeping more3 (0.8%)3 (0.4%) Sleep change, unspecified direction3 (0.8%)9 (1.3%)Somatic symptoms Exacerbation of prior somatic symptoms4 (1.1%)4 (0.6%) New onset somatic symptoms34 (9.6%)84 (11.9%)Fatigue Exhaustion42 (11.9%)66 (9.3%) Tiredness or fatigue23 (6.5%)69 (9.7%)Exacerbation of physical illness6 (1.7%)22 (3.1%)Lack of access to health behavior facilitators14 (4.0%)20 (2.8%)Chronically ill8 (2.3%)15 (2.1%)Anxiety76 (21.5%)148 (20.9%)Stress122 (34.6%)269 (38.0%)Depression38 (10.8%)93 (13.1%)Grief/nostalgia18 (5.1%)34 (4.8%)Guilt15 (4.2%)21 (3.0%)Uncertainty58 (16.4%)91 (12.9%)Frustration72 (20.4%)170 (24.0%)Post-traumatic symptoms5 (1.4%)10 (1.4%)Feeling imprisoned8 (2.3%)23 (3.2%)Suicidality5 (1.4%)4 (0.6%)Exacerbation of mental health difficulties15 (4.2%)20 (2.8%)New onset of mental health difficulties76 (21.5%)169 (23.9%)Medications Increased medication4 (1.1%)6 (0.8%) Started new medication10 (2.8%)13 (1.8%)Therapy New pandemic therapy4 (1.1%)7 (1.0%) Current therapy, unclear if existent prior to pandemic5 (1.4%)11 (1.6%) Desire to start but unable to access therapy3 (0.8%)4 (0.6%)Helpless or hopeless38 (10.8%)131 (18.5%)Lack of time for self4 (1.1%)19 (2.7%)Alone49 (13.9%)153 (21.6%)Solitude appreciation5 (1.4%)13 (1.8%)Self-reflection35 (9.9%)30 (4.2%)Falling short of professional self-expectations49 (13.9%)113 (16.0%)Inadequate education for students45 (12.7%)124 (17.5%)Overworked42 (11.9%)124 (17.5%)Increased responsibility84 (23.8%)245 (34.6%)Nature of job changed43 (12.2%)149 (21.0%)Positivity34 (9.6%)16 (2.3%)Unsafe policies or spaces47 (13.3%)163 (23.0%)Student issues14 (4.0%)50 (7.1%)Parental disrespect15 (4.2%)18 (2.5%)Resentment towards profession72 (20.4%)191 (27.0%)Financial concerns27 (7.6%)25 (3.5%)Professional instability16 (4.5%)36 (5.1%)District-level administrative support Less support65 (18.4%)142 (20.1%) More support5 (1.4%)29 (4.1%)Building-level administrative support Less support17 (4.8%)28 (4.0%) More support24 (6.8%)39 (5.5%)Administrative support, level unspecified Less support46 (13.0%)109 (15.4%) More support15 (4.2%)19 (2.7%)Voiced concerns Voiced concerns, not heard91 (25.8%)200 (28.2%) Voiced concerns, heard30 (8.5%)70 (9.9%) Told what they would be doing, not asked59 (16.7%)71 (10.0%) Told what they would be doing, not asked and voice not heard9 (2.5%)25 (3.5%)State influence on decision-making30 (8.5%)80 (11.3%)Parental influence on decision-making18 (5.1%)41 (5.8%)Other organizational influence on decision-making School board32 (9.1%)60 (8.5%) Union22 (6.2%)22 (3.1%)Family-work responsibilities4 (1.1%)16 (2.3%)Work satisfaction Dissatisfaction with work41 (11.6%)97 (13.7%) Satisfaction with work10 (2.8%)14 (2.0%)Career change Desire to shift careers39 (11.0%)78 (11.0%) Plan to shift careers9 (2.5%)7 (1.0%) Shifted careers due to pandemic7 (2.0%)6 (0.8%) Pursuing early retirement12 (3.4%)18 (2.5%) Retired early0 (0.0%)2 (0.3%)Educational pursuits Declined to pursue additional education36 (10.2%)41 (5.8%) Pursued additional education11 (3.1%)34 (4.8%) Desire to pursue additional education but no action reported5 (1.4%)10 (1.4%)Career advancement No opportunity for career advancement22 (6.2%)9 (1.3%) Experienced career advancement4 (1.1%)39 (5.5%)Technology20 (5.7%)76 (10.7%)Lack of resources, internet3 (0.8%)3 (0.4%)Lack of resources, cleaning supplies4 (1.1%)2 (0.3%)Lack of resources, personal protective equipment (PPE)4 (1.1%)13 (1.8%)Parental academic support Less support15 (4.2%)10 (1.4%) More support9 (2.5%)1 (0.1%)Personal protective behaviors, seeking increased air flow37 (10.5%)51 (7.2%)Personal protective behaviors, disinfecting surfaces72 (20.4%)131 (18.5%)Personal protective behaviors, social distancing93 (26.3%)122 (17.2%)Personal protective behaviors, requesting students to mask37 (10.5%)41 (5.8%)Personal protective behaviors, personal PPE use63 (17.8%)138 (19.5%)Personal protective behaviors, parental safety support1 (0.3%)3 (0.4%)Personal protective behaviors, altering eating behaviors148 (41.9%)314 (44.4%)Personal protective behaviors, altering shopping behaviors80 (22.7%)130 (18.4%)Personal protective behaviors, increased cleaning of self44 (12.5%)90 (12.7%)Personal protective behaviors, travel Limiting travel10 (2.8%)15 (2.1%) No travel12 (3.4%)27 (3.8%)Personal protective behaviors, isolating65 (18.4%)226 (31.9%)Personal protective behaviors, altering living arrangements8 (2.3%)5 (0.7%) Note. Data represent the frequency (n) and percentage (%) of participants in the inductive (n = 224) and deductive (n = 701) samples endorsing each code. Definitions for abbreviated or specific codes are as follows: Alone indicates feeling alone or uncared for; Job change indicates feeling as though the nature of the job has changed (e.g., feeling like a babysitter); Positivity indicates having to stay positive for the kids or behaving incongruent with emotions; Student issues indicates an increase in student behavioral issues; Technology indicates new technology as a factor; and Unsafe policies or spaces indicates policies or physical spaces do not feel safe at work or are not following CDC guidelines.
Themes
COVID-19. Codes observed included: fear of COVID-19 infection, fear of spreading COVID-19, COVID-19 exposure, and COVID-19 infection. Exposure was defined by coders as a known exposure, and infection as a positive test.
Social health. Given the numerous changes in public health recommendations that may have necessitated changes in social behaviors, these themes included responses such as social distancing, lockdowns, isolation, or minimization of contact with others. Codes in this section included limited social interaction, increase or decrease in family time, forgoing activities, virtual activities, and lack of connection or feeling isolated.
Physical health. Derived codes included changes in exercise or physical activity, weight, and/or diet changes, sleep changes, somatic symptoms, fatigue, and lack of access to health behavior facilitators (e.g., gyms or health care visits). Because of the regulations that varied by state, some of these activities were forbidden or strongly recommended against. Others reported forgoing activities to minimize risk.
Mental health. Derived codes included psychological experiences, including depression, anxiety, suicidality, and helplessness. This section highlights changes to existing psychiatric medications or starting new psychiatric medication. Themes of seeking new psychotherapeutic services or desire but inability to seek therapy were observed. This section included stress, grief, uncertainty, self-reflection, and appreciation of solitude.
Professional well-being. Derived codes included a sense that the education being provided was inadequate. A theme of having unsafe policies or physical spaces, such as classrooms being unfit for social distancing guidelines, was observed. Themes regarding student issues, parental disrespect, financial concerns, and either the presence or lack of administrative support were observed. Educators reported feeling overworked and having increased responsibilities. Educators reported insufficient personal protective equipment (PPE) to safely work in-person. Themes of career dissatisfaction and plans for career change were present. Some reported having shifted careers. On the other hand, some reported feeling validated in their career choice and had an increased sense of belonging. Another theme was having one’s voice heard by administrators; some reported having a role in decision-making processes, whereas others voiced opinions and were ignored. Others were not asked for feedback and were informed of plans.
Precautions taken. Derived codes highlighted the precautions that educators were taking to avoid becoming infected with or spreading COVID-19. Themes included disinfecting surfaces, social distancing, and altering eating and shopping behaviors.
Deductive Findings
Participants reported fear of spreading (13.1%) or becoming infected with (11.6%) COVID-19, with some reporting a known exposure or infection at work (0.6%). When connected with CDC county-level data, most participants who also completed the quantitative data portion of this study (88.0%) reported living in an area with a “high” rate of COVID-19 transmission.38 Most reported limiting social interactions (72.0%), and 27.8% reported feeling lack of connection or isolation. Moreover, 49.5% chose not to attend certain activities, and 29.8% reported virtual engagement in activities. Changes in mental and physical health were also reported. New-onset symptoms were reported, with 11.9% of participants reporting new-onset somatic symptoms and 23.9% reporting new-onset mental health symptoms. Less often noted were exacerbations of physical illness (3.1%) or mental health difficulties (2.8%). Participants reported decreased physical activity (16.4%), weight gain (12.4%), and negative changes in diet (9.7%). Others reported positive health behavior changes (e.g., positive changes in diet [1.6%], increased self-care [2.0%], and increased exercise or physical activity [4.9%]).
Alongside mental health difficulties, many specific emotions and symptoms were reported, including anxiety (20.9%), stress (38.0%), frustration (12.9%), and uncertainty (12.9%). Many reported feeling helpless or hopeless (18.5%) and alone (21.6%). Several personal protective behaviors were reported, including altering eating behavior (44.4%) and personal PPE use (19.5%). Many reported a lack of administrative support across district-level (20.1%), building-level (4.0%), and unspecified levels of administrative support (15.4%). Others reported administrative support (district-level: 4.1%; building-level: 5.5%). Many reported their concerns were not heard when voiced (28.2%), while others reported feeling heard (9.9%). Others were told of plans, not asked (10.0%). Some reported being told of plans, not asked for their concerns, and their voice was not heard (3.5%).
Underscoring the competing demands that educators faced, 34% reported increased work responsibility, and 21% reported that the nature of their job changed. Some participants felt overworked (17.5%), and others reported that expectations had increased in a way that was unachievable (16.0%). Some participants reported feeling that they were delivering an inadequate education, and almost one-quarter reported unsafe policies or spaces at work (23.0%). Some participants reported work dissatisfaction (13.7%), and participants reported feeling work-related resentment (27.0%).
Discussion
The purpose of this study was to understand how the COVID-19 pandemic impacted domains of health (mental, physical, and social), day-to-day functioning, and career satisfaction among educators in the USA. Although research detailed the physical and psychological health impacts of COVID-19 on educators worldwide, limited work has focused on educators’ lived experiences. The present study sought to derive themes inductively and apply the derived codes to the deductive dataset. The authors describe educator experiences across domains of health as detailed by educators in November and December of 2020.
The findings demonstrated deleterious mental and physical health impacts, where participants reported feeling demoralized and distressed. Participants endorsed occupational changes, including planning or desiring to leave the profession, in part due to new responsibilities and insufficient time. Educators reported increased expenses for work supplies, such as cleaning supplies and PPE. Many educators reported isolation in service of protecting others, with some living separately from family or not seeing relatives, limiting access to supports. See Table 3 for deidentified quotes sampled from educators in the deductive phase of analyses.Table 3.Deidentified quotes from participants in the deductive phase, grouped by themesMental healthPhysical healthSocial healthCOVID-19Professional well-beingPrecautions taken“I have constant anxiety and high stress. I had to go on antidepressants and sleeping pills.”“Stress has wreaked havoc on my body, and I have gained 20 + pounds since March.”“I don’t see anyone in person anymore.”“I am anxious and worried about getting covid.”“I am exhausted everyday at work. My workload has severely increased and I feel like I never have enough time to plan or grade or give feedback.”“Eating in my own classroom, sleep in separate room than [partner] ([they] work with Covid + patients), cancelled all travel, avoid coworkers that dont wear their mask appropriately.”“I started counseling and started taking Zoloft to handle stress and anxiety due to work and the pandemic.”“It has caused me to exercise more. I have found that running is a very positive thing for me to do when I am stressed out.”“I miss spending time with friends and family. My mother has dementia [and] my father is taking care of her alone.”“I have asthma and allergies and I’m constantly worried about regular asthma/allergy symptoms vs covid symptoms.”“I want a new career and don’t know what else to do. I’ve been a teacher for [many] years and I want to get out.”“No— it seemed pointless given the amount of close contact already involved in my work day.”“Drained it. I’ve never been so depressed and I don’t recall feeling helpless ever. Now, both daily.”“I have had panic attacks, chest pains, trouble sleeping. I’m diabetic and my eating habits have declined due to stress, causing my sugars to spike. My sleep habits have also been disrupted.”“In some ways, the pandemic brought me closer to my colleagues. People outside of my profession do not understand the amount of pressure on teachers nor the amount of time and energy we are spending trying to balance in-person instruction, virtual instruction, and protecting our health. So I am losing contact with non-educators.”“I am potentially exposed to Covid every work day. I will not risk others.”“I will leave education as soon as I have the opportunity to do so. My community and my leaders have abandoned any pretense of concern or respect for my profession or for my humanity.”“Eating in my car, leaving work as soon as possible, never eat in restaurants, haven’t seen my family since March, haven’t seen most of my friends since March, using grocery pickup instead of going to the store.”“I started seeing my therapist again starting in August due to the stress of work. My stress level is so high that I’ve just given up on being a good teacher.”“Increased issues with blood sugar and hypertension as a result of the increased stress.”“I stay away from my parents because they are high risk and I don’t want to catch something at work and then give it to them.”“I acquired covid at work and am still suffering symptoms more than a month later.”“I have a strong administration that really values teachers and I feel like my voice has been heard and that my voice is encouraged.”“I wear scrubs to work. I take my shoes off outside before coming into my house where I immediately take a shower then wash my clothes from the day. Then I spray lysol on door knobs and my shoes and my work bag. I do all this before I even hug my kids and greet my husband.”“I feel I am happier overall…I love teaching online now”“Weight gain, no activity, drinking more alcohol due to stress.”“I can no longer see my family (who were the only people I’ve visited in their house the entire pandemic). I live alone and am now isolated.”“I believe I had covid but didn’t realize it at the time and spread it to my family. Everyone in my family became ill. My mother in law ended up in hospital.”“I was not given an option to teach remotely, despite having a heart condition and despite having elderly individuals in the household. Even now, I will soon be forced to choose FMLA.”“Wearing scrubs not using public restrooms. Not eating in restaurants. Not seeing family or friends. Not attending meetings [or] getting haircut, massage.” Note. Quotes that include [bracketed text] were altered to remove any potentially identifying information.
Our results align with literature noting worsened physical and mental health during the COVID-19 pandemic among educators worldwide.6 ^–^9 ^,^49 Decreased physical activity, increased sedentary behavior, weight gain, negative dietary changes, and sleeping less were noted among our sample, fitting with literature noting a decrease in healthy lifestyle behaviors during the COVID-19 pandemic.49 ^,^50 Somatic symptom burden was also significant, fitting with literature noting increased somatic symptom burden during the COVID-19 pandemic.51 Anxiety, stress, depression, uncertainty, and feeling hopeless or helpless were reported in our sample, aligning with extant research.6 ^–^9 ^,^49 Some participants noted increased self-reflection, fitting with research observing improved self-concept, autonomy, and psychological well-being among some during COVID-19 lockdowns.52 As with a significant proportion of the world’s population,11 our sample reported limiting social interaction and forgoing activities. Although concerns about developing or spreading COVID-19 were frequently noted among our sample, confirmed exposure and infection were relatively low, though infection was not directly assessed herein.
Past literature has noted educators as essential workers affected by the pandemic with reports of lack of colleague support, increased workload, and poor employment conditions.25 ^,^29 ^,^31 ^,^32 ^,^53 ^–^55 Our results further illustrate the lived experience of educators during this time. The participants noted increased responsibility, with failure to meet professional self-expectations, perception of providing inadequate education, being overworked, and feeling that the nature of the job had changed. These reports mirror wider literature noting increased responsibilities, juggling multiple roles, and the blurring of professional-personal boundaries.16 ^,^36 ^,^39 ^,^40 ^,^55 The APA technical report highlighted concerns regarding the safety of educators regarding physical violence, verbal abuse, and risk of COVID-19 infection.29 The present findings describe unsafe policies and physical spaces at work related to the infectious nature of COVID-19, further highlighting educator distress.
Educators noted varied experiences regarding support in the workplace. Building-level administrative support was reported more frequently than district-level administrative support, indicating that those in closer proximity to our sample (primarily teachers) provided more support. Several participants voiced concerns to superiors about the occupational environment with varying levels of success. The highest proportion who voiced concerns did not feel those concerns were heard. The perception of difficult working conditions has been associated with mental health difficulties among educators,16 ^,^31 ^,^32 ^,^56 and occupation-related concerns and lack of administrative support noted among some in our sample mirror this finding. Perhaps associated with these issues, resentment of employers was observed. Some educators noted desire or plan to shift away from educational careers, whereas others intended to pursue early retirement. These findings were also demonstrated by the APA, with 49% of US educators surveyed having a desire to leave the profession.29
Finally, pandemic precautions were reported during early stages of the COVID-19 pandemic,57 and our sample also endorsed protective behaviors. The most common protective behaviors were increasing ventilation, disinfecting surfaces, social distancing, using PPE, and altering shopping behaviors, fitting with findings in the wider population from this time.58 ^–^60 However, other precautions seemed specific to the occupational environment, such as monitoring masking among students and altering eating behaviors (e.g., not eating in classroom or break room).
Limitations
There are several limitations to this research. The sample was primarily White, non-Hispanic females. Even though this aligns with the population of USA educators, our sample lacks diversity in race, ethnicity, and gender.29 ^,^61 The study advertisement was posted on Facebook and Reddit. This may have resulted in a lack of responses from educators who did not use social media. The study was cross-sectional; therefore, no longitudinal conclusions can be drawn. The data did not capture duration or intensity of experiences. Data were collected via survey to maximize participant ease, but no follow-up or clarifying questions were asked.
As our study involved educator responses during 2020, our findings do not apply to educators’ experiences during other phases of the pandemic. Longitudinal work could be utilized to assess the experience of educators over time. While our work analyzed written qualitative responses, other qualitative interviews or focus groups may allow follow-up and in-depth understanding of the educator experience. Future work could assess long-term implications of the COVID-19 pandemic on educators.
Implications
Given the expressed mental health concerns, systemic emphasis on utilization of mental health care resources may be a helpful future direction. Providing resources in the workplace would improve access. One study in Colorado demonstrated workplace integration, with eight schools providing social-emotional competencies workshops in the workplace, and demonstrated benefit.62
Beyond individual-level interventions, systems-level interventions should also be considered. School psychologists are often confused as resources for the students and teachers, which is typically not the case. School psychologists serve as an invaluable resource for students struggling with issues related to learning and school, but oftentimes there are few (if any) resources for educator mental health within the school system.63 However, when providing a mental health care specialist for educators has been tested, mindfulness has improved, and stress has decreased.64 Although this research is promising, it does not address the needs of educators in areas that are not well-resourced. Districts that cannot provide an on-site mental health care specialist for educators should consider providing low-cost, virtual mental health care for employees.
The “Supporting the Mental Health of Educators and Staff Act of 2023” highlights the incorporation of mental health care services in the workplace and proposes substantial funding to support this type of programming at a policy level within the USA.65 Including mental health care screenings in employee health screenings would further the goal of normalizing checking in about mental health and well-being.66 Having referral options following screening is of critical importance.
At the systemic level, lack of agency or voice was described by educators in our sample. Many wrote about decisions being made on their behalf at the building and district levels. Encouraging representation of educators as key stakeholders in these choices would increase agency. Increasing spending for educator health would allow for identification of predictors of workplace satisfaction among educators.67 ^,^68 This would elucidate problem areas and improve teacher retention, leading to fiscal benefits and downstream improved student achievement.67 ^,^68
Conclusion
In summary, the present study examined USA educators’ experiences. Many of the themes aligned with issues that have been highlighted in media and policy beyond the COVID-19 pandemic, including lack of perceived support by administration and inadequate time allotted for responsibilities. Our findings demonstrated negative impacts on educators’ physical and psychological health, as well as a desire to feel heard in decision-making. Further intervention research is needed to address educator mental and physical health at different levels of intervention (individuals, systems, policies). As educators shape the future of students and communities worldwide, it is imperative that their well-being is a top priority.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19. WHO. Published 2020. Accessed [03/11/2020]. https://www.who.int/news-room/speeches/item/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020
- 2World Health Organization. WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. WHO. Published 2024. Accessed [01/21/2026]. https://covid 19.who.int/
- 3Centers for Disease Control and Prevention. Symptoms of COVID-19. CDC. Published October 26, 2022. Accessed [08/2023]. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
- 4Davis HE, Mc Corkell L, Vogel JM, et al. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s 41579-022-00846-236639608 PMC 9839201 · doi ↗ · pubmed ↗
- 5Shanbehzadeh S, Tavahomi M, Zanjari N, et al. Physical and mental health complications post-COVID-19: scoping review. J Psychosom Res. 2021;147:110525. doi:10.1016/J.JPSYCHORES.2021.11052534051516 PMC 8133797 · doi ↗ · pubmed ↗
- 6Thompson EJ, Stafford J, Moltrecht B, et al. Psychological distress, depression, anxiety, and life satisfaction following COVID-19 infection: evidence from 11 UK longitudinal population studies. Lancet Psychiatry. 2022;9(11):894–906. doi:10.1016/S 2215-0366(22)00307-836244359 PMC 9560745 · doi ↗ · pubmed ↗
- 7Jia H, Guerin RJ, Barile JP, et al. National and state trends in anxiety and depression severity scores among adults during the COVID-19 pandemic — United States, 2020–2021. MMWR Morb Mortal Wkly Rep. 2021;70(40):1427–1432. doi:10.15585/MMWR.MM 7040 E 334618798 PMC 12364538 · doi ↗ · pubmed ↗
- 8Liu CH, Zhang E, Wong GTF, et al. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for U.S. young adult mental health. Psychiatry Res. 2020;290:113172. doi:10.1016/J.PSYCHRES.2020.11317232512357 PMC 7263263 · doi ↗ · pubmed ↗