Retinal imaging in pre‐eclamptic pregnancy: systematic review
D. Kitmiridou, I. Mitrogiannis, M. Charakida, K. H. Nicolaides

TL;DR
This review examines retinal changes in pregnant women with pre-eclampsia, finding inconsistent results across studies.
Contribution
The paper provides a systematic review of retinal imaging in pre-eclamptic pregnancies, highlighting the lack of consensus and need for further research.
Findings
Retinal imaging methods showed mixed results in detecting structural changes in pre-eclamptic pregnancies.
Most studies found no significant differences in retinal thickness and vessel density between pre-eclamptic and non-pre-eclamptic groups.
The review emphasizes the need for large-scale prospective studies to clarify retinal changes in pre-eclampsia.
Abstract
To explore potential changes in retinal structures in pregnant women with pre‐eclampsia (PE). This was a systematic review of the literature on retinal assessment in pregnancies complicated by PE. PubMed, EMBASE via Ovid, The Cochrane Library and Scopus databases were searched in July 2025 using an a‐priori‐designed protocol for studies examining the retina of pregnant women with an established diagnosis of PE or those who developed PE following retinal assessment. Randomized controlled trials and prospective and retrospective cohort, case–control and population‐based studies were eligible. Risk of bias was assessed using the Risk Of Bias In Non‐randomized Studies of Interventions version 2 (ROBINS‐I V2) tool. Due to substantial heterogeneity observed between studies in the methods of retinal assessment, retinal parameters studied and gestational age at retinal examination, a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
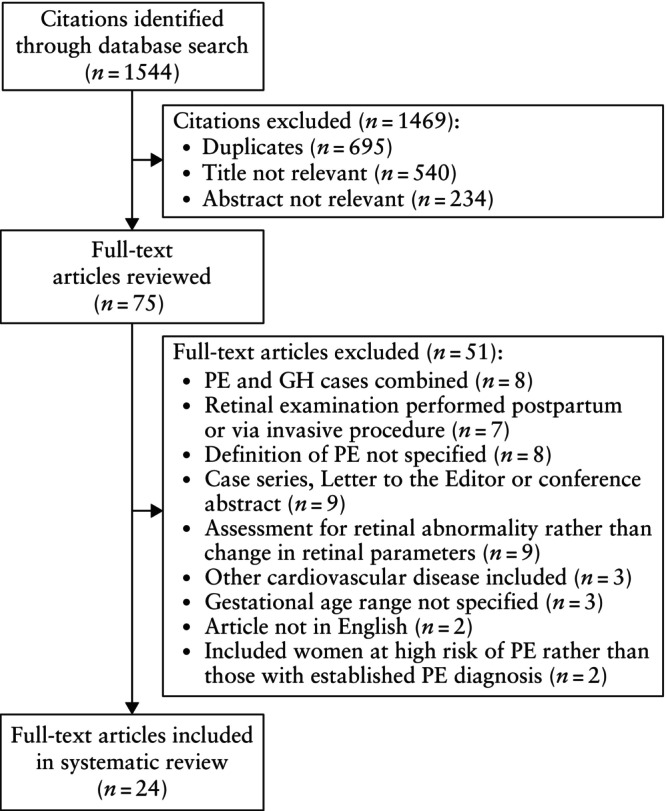 Figure 1
Figure 1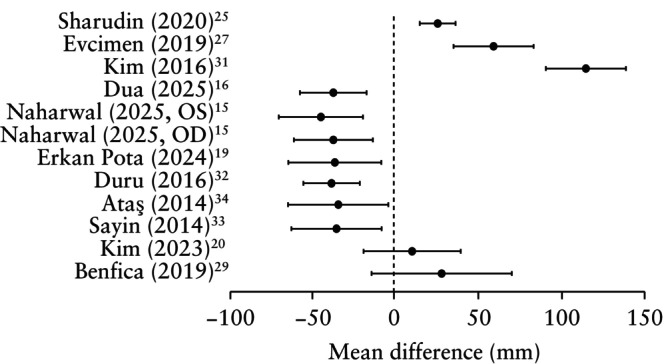 Figure 2
Figure 2| Study | Women with PE ( | Women without PE ( | Retinal examination | GA at examination | Retinal parameter(s) examined |
|---|---|---|---|---|---|
| Dua (2025) | 42 | 42 | OCT | 32–37 w | Choroidal and retinal thickness |
| Naharwal (2025) | 30 | 30 | OCT | 20–39 w | Choroidal thickness |
| Erkan Pota (2024) | 27 | 30 | OCTA/OCT | 28–34 w | Choroidal, retinal, RNFL and GCL thickness; SCP, DCP and choriocapillaris vessel density; FAZ parameters |
| Lee (2024) | 66 | 0 | OCT | 26–41 w | Choroidal thickness and vascularity index |
| Tang (2024) | 64 | 63 | OCTA/OCT | 29–39 w | Retinal thickness; SCP vessel density; perfusion density; FAZ parameters |
| Fayed (2023) | 15 | 15 | OCTA | Third trimester | Adjusted flow index |
| Kim (2023) | 46 | 7 | OCT | 32–36 w | Choroidal thickness and choroidal vessel density |
| Özcan (2022) | 50 | 50 | OCTA/OCT | 22 w to term | Macular and RNFL thickness; SCP and DCP vessel density; FAZ parameters; choriocapillaris blood flow area |
| Lee (2021) | 52 | 0 | OCTA/OCT | 21–39 w | Choroidal and GCL thickness; SCP and DCP vessel density; FAZ area |
| Sharudin (2020) | 50 | 50 | OCT | 28–41 w | Choroidal and macular thickness |
| Tok (2020) | 28 | 28 | OCT | 26–40 w | Macular, RNFL and GCL thickness |
| Benfica (2019) | 47 | 27 | OCT | 28–39 w | Choroidal thickness |
| Ciloglu (2019) | 55 | 43 | OCTA/OCT | 26–43 w | RNFL thickness; SCP and DCP vessel density; FAZ area |
| Evcimen (2019) | 52 | 54 | OCT | 20–39 w | Choroidal and macular thickness |
| Urfalıoglu (2019) | 27 | 26 | OCTA | 26–40 w | SCP and DCP vessel density; choriocapillaris and retinal blood flow area |
| Arab (2018) | 105 | 44 | OCT | 28–41 w | RNFL thickness |
| Duru (2016) | 32 | 41 | OCT | 28–37 w | Choroidal thickness |
| Kim (2016) | 7 | 14 | OCT | 28–37 w | Choroidal and retinal thickness |
| Ataş (2014) | 27 | 25 | OCT | 28–42 w | Choroidal, macular and RNFL thickness |
| Sayin (2014) | 33 | 46 | OCT | 16–36 w | Choroidal thickness |
| Lupton (2013) | 9 | 83 | Fundus photography | 13, 19, 29, 38 w | Central retinal arteriolar and venular equivalent |
| Gooding (2012) | 20 | 20 | OCT | 27–35 w | Retinal thickness and volume |
| Onaran (2012) | 20 | 21 | Central retinal artery Doppler | 24–38 w | PSV, EDV and RI of central retinal artery |
| Jaffe (1987) | 31 | 25 | Fundus photography | Third trimester | Arteriole‐to‐vein ratio |
| Parameter/Study | Design | Finding |
|---|---|---|
| Choroidal thickness | ||
| Sharudin (2020) | PE | Higher |
| Evcimen (2019) | PE | Higher |
| Kim (2016) | PE | Higher |
| Dua (2025) | PE | Lower |
| Naharwal (2025) | PE | Lower (OD); lower (OS) |
| Erkan Pota (2024) | PE | Lower |
| Duru (2016) | PE | Lower |
| Ataş (2014) | PE | Lower |
| Sayin (2014) | PE | Lower |
| Kim (2023) | PE | Similar |
| Benfica (2019) | PE | Similar |
| Lee (2024) | PE | Associated directly with urine PCR |
| Lee (2021) | PE | Associated inversely with sFlt‐1/PlGF ratio |
| Retinal thickness | ||
| Dua (2025) | PE | Higher |
| Erkan Pota (2024) | PE | Similar |
| Tang (2024) | PE | Similar |
| Kim (2016) | PE | Similar |
| Gooding (2012) | PE | Similar |
| Retinal nerve fiber layer thickness | ||
| Özcan (2022) | PE | Lower |
| Erkan Pota (2024) | PE | Similar |
| Tok (2020) | PE | Similar |
| Ciloglu (2019) | PE | Similar |
| Arab (2018) | PE | Similar |
| Ataş (2014) | PE | Similar |
| Macular thickness | ||
| Özcan (2022) | PE | Lower |
| Sharudin (2020) | PE | Similar |
| Tok (2020) | PE | Similar |
| Evcimen (2019) | PE | Similar |
| Ataş (2014) | PE | Similar |
| Ganglion cell layer thickness | ||
| Erkan Pota (2024) | PE | Similar |
| Tok (2020) | PE | Similar |
| Lee (2021) | PE | Similar in women with high |
| Choroidal vessel density | ||
| Kim (2023) | PE | Similar |
| Choroidal vascularity index | ||
| Lee (2024) | PE | Similar in women with high |
| Total retinal volume | ||
| Gooding (2012) | PE | Similar |
| Parameter/Study | Design | Finding |
|---|---|---|
|
| ||
| Foveal avascular zone area | ||
| Tang (2024) | PE | Similar |
| Erkan Pota (2024) | PE | Similar |
| Özcan (2022) | PE | Similar |
| Ciloglu (2019) | PE | Similar |
| Lee (2021) | PE | Similar in women with high |
| Deep capillary plexus vessel density | ||
| Erkan Pota (2024) | PE | Lower |
| Deep foveal vessel density | ||
| Özcan (2022) | PE | Lower |
| Ciloglu (2019) | PE | Similar |
| Deep parafoveal vessel density | ||
| Ciloglu (2019) | PE | Similar |
| Urfalıoglu (2019) | PE | Similar |
| Deep perifoveal, parafoveal and foveal vessel density | ||
| Lee (2021) | PE | Similar in women with high |
| Superficial capillary plexus vessel density | ||
| Erkan Pota (2024) | PE | Similar |
| Superficial foveal vessel density | ||
| Özcan (2022) | PE | Lower |
| Ciloglu (2019) | PE | Similar |
| Superficial parafoveal vessel density | ||
| Özcan (2022) | PE | Similar |
| Ciloglu (2019) | PE | Similar |
| Urfalıoglu (2019) | PE | Similar |
| Superficial perifoveal, parafoveal and foveal vessel density | ||
| Tang (2024) | PE | Lower |
| Lee (2021) | PE | Similar in women with high |
| Retinal perfusion density/blood flow area (perifoveal, parafoveal, foveal) | ||
| Perfusion density | ||
| Tang (2024) | PE | Lower |
| Retinal superficial blood flow area | ||
| Urfalıoglu (2019) | PE | Similar |
| Retinal deep blood flow area | ||
| Urfalıoglu (2019) | PE | Similar |
| Choriocapillaris blood flow | ||
| Adjusted flow index | ||
| Fayed (2023) | PE | Lower |
| Blood flow area | ||
| Özcan (2022) | PE | Lower |
| Urfalıoglu (2019) | PE | Lower |
| Vessel density | ||
| Erkan Pota (2024) | PE | Similar |
|
| ||
| Corrected central retinal arteriolar equivalent | ||
| Lupton (2013) | PE | Lower |
| Corrected central retinal venular equivalent | ||
| Lupton (2013) | PE | Lower |
| Arteriole‐to‐vein ratio | ||
| Jaffe (1987) | sPE | Lower |
|
| ||
| Peak systolic velocity | ||
| Onaran (2012) | PE | Similar |
| End‐diastolic velocity | ||
| Onaran (2012) | PE | Similar |
| Resistance index | ||
| Onaran (2012) | PE | Higher |
| Study | Confounding | Classification of intervention | Selection of participants | Deviation from intended intervention | Missing data | Measurement of outcome | Selection of reported results | Overall risk |
|---|---|---|---|---|---|---|---|---|
| Dua (2025) | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Naharwal (2025) | Serious | Low | Moderate | Low | Low | Low | Low | Serious |
| Erkan Pota (2024) | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Lee (2024) | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Tang (2024) | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Fayed (2023) | Serious | Low | Low | Low | Low | Low | Low | Serious |
| Kim (2023) | Serious | Low | Moderate | Moderate | Moderate | Moderate | Low | Serious |
| Özcan (2022) | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Lee (2021) | Low | Low | Low | Moderate | Low | Moderate | Low | Moderate |
| Sharudin (2020) | Serious | Low | Low | Low | Low | Low | Low | Serious |
| Tok (2020) | Moderate | Low | Low | Low | Low | Moderate | Low | Moderate |
| Benfica (2019) | Serious | Low | Moderate | Low | Low | Low | Low | Serious |
| Ciloglu (2019) | Serious | Low | Low | Low | Low | Low | Low | Serious |
| Evcimen (2019) | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
| Urfalıoglu (2019) | Serious | Low | Moderate | Moderate | Low | Moderate | Low | Serious |
| Arab (2018) | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Duru (2016) | Serious | Low | Moderate | Low | Low | Low | Low | Serious |
| Kim (2016) | Serious | Low | Moderate | Low | Low | Moderate | Low | Serious |
| Ataş (2014) | Serious | Low | Low | Low | Low | Low | Low | Serious |
| Sayin (2014) | Low | Low | Moderate | Low | Low | Low | Low | Moderate |
| Lupton (2013) | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
| Gooding (2012) | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Onaran (2012) | Serious | Low | Moderate | Low | Low | Moderate | Low | Serious |
| Jaffe (1987) | Serious | Low | Low | Low | Low | Low | Low | Serious |
- —Fetal Medicine Foundation10.13039/501100003123
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Neurological Complications and Syndromes · Retinopathy of Prematurity Studies
INTRODUCTION
Pre‐eclampsia (PE) is a major cause of maternal−fetal morbidity and mortality, affecting approximately 5% of pregnancies1. Women with PE are at an increased risk of future cardiovascular complications; they are twice as likely to develop ischemic heart disease and have a higher chance of cardiovascular mortality compared with women who were normotensive during pregnancy2, 3. This is likely a consequence of PE acting as a marker of chronic underlying susceptibility to future disease, rather than PE causing harm which eventually leads to clinically apparent maternal cardiovascular and metabolic sequelae4, 5.
Retinal assessment has been proposed as an accessible way to examine the systemic microcirculation, with the potential to predict the development of hypertension and identify individuals at higher cardiovascular risk6, 7. Narrowing of the retinal arterioles has been identified as a potential marker for developing hypertension, which is hypothesized to be a result of increased vascular resistance8. Changes in the small vessels of the retina are thought to precede gross vascular changes, thus allowing for earlier detection of individuals at risk9. Assessment of the retinal microvasculature can also provide information on cumulative changes, rather than a snapshot of the circulatory status at the time of assessment10. Optical coherence tomography (OCT) has been used to study the choroid, a vascular network that provides oxygen and nutrients to the retina. Outside of pregnancy, changes in choroidal thickness have been associated with cardiovascular disease11. In pregnancy, there is emerging evidence that various cardiovascular indices can be used for the prediction of PE12. However, there is no consensus within the currently available evidence on the retinal changes associated with PE13.
The aims of this study were to conduct a systematic review of the available literature regarding retinal assessment in pregnancies complicated by PE and to assess the feasibility of a meta‐analysis. We aimed to explore potential changes in retinal structures in pregnant women with PE and determine whether specific retinal parameters can serve as early biomarkers of PE.
METHODS
This systematic review adhered to the Preferred Reporting Items for Systematic reviews and Meta‐Analyses (PRISMA) checklist14 and followed an a‐priori‐designed search protocol, which was registered prospectively on PROSPERO (ID: CRD420251010666).
Data sources and search strategy
We performed an electronic search of PubMed, EMBASE via Ovid, The Cochrane Library and Scopus databases on 6 July 2025, using a combination of the following keywords and medical subject heading (MeSH) terms: ‘optical coherence tomography’, ‘retina’, ‘fundus photography’, ‘retinal imaging’, ‘retinal vasculature’, ‘retinal vessels’, ‘choroidal thickness’, ‘pre‐eclampsia’, ‘preeclampsia’, ‘pregnancy‐induced hypertension’ and ‘HELLP syndrome’. The reference lists of other systematic reviews and the selected studies were screened manually to identify additional eligible studies that were missed by the aforementioned search.
Eligibility criteria and study selection
We included studies examining the retina of pregnant women with an established diagnosis of PE or those who developed PE following retinal assessment. Randomized controlled trials and prospective and retrospective cohort, case–control and population‐based studies were eligible for inclusion. We included studies utilizing any kind of non‐invasive retinal imaging, as well as those in which pregnant women without PE were used as controls. We excluded the following studies: review articles, case reports, case series, Letters to the Editor, conference abstracts, retracted articles and study protocols; studies not written in English; studies that did not specify the definition used for PE; studies including women with gestational or pre‐existing hypertension or cardiovascular disease; studies assessing retinal abnormalities rather than changes in retinal parameters; studies that did not define the gestational age range at retinal examination; and studies in which retinal assessment was performed only postpartum.
Study selection was performed independently by two reviewers (D.K., I.M.), who screened titles and abstracts to identify potentially eligible studies. Full‐text articles were then reviewed to select studies suitable for inclusion. Discrepancies were discussed and, if consensus could not be achieved between the two reviewers, a third senior reviewer (K.H.N.) was consulted.
Data extraction
For each study, we populated a predefined data extraction form, which included the title, year and journal of publication, name of the first author, details of the study population (including whether non‐PE or non‐pregnant controls were also examined), number of participants, gestational age range at the time of retinal assessment, method of retinal assessment and retinal parameters studied.
We reported the mean ± SD or median (interquartile range) of the retinal parameters examined. Studies considered for inclusion were assessed carefully to avoid duplicates and overlapping samples. If overlapping samples were detected, the study with the largest sample size was selected for data extraction.
Assessment of risk of bias
The risk of bias was assessed independently by two reviewers (D.K., I.M.) using the Risk Of Bias In Non‐randomized Studies of Interventions version 2 (ROBINS‐I V2) tool. We examined the risk of bias across seven domains: presence of and adjustment for confounding factors, classification of interventions, participant selection criteria, any deviations from the intended intervention, reporting and management of missing data, outcome measurement, and selection of the reported results. We combined the level of risk assigned to each of these domains (low, moderate, serious or critical) to calculate an overall risk of bias for each included study.
Synthesis of results
Due to the substantial heterogeneity in the methods of retinal assessment, retinal parameters studied and gestational age at retinal examination observed between the studies included in this systematic review, a meta‐analysis was not performed.
RESULTS
Database search results
The electronic database search yielded 1544 results (Figure 1). Following the removal of duplicates, 849 citations underwent title and abstract screening, of which 774 were excluded. A total of 75 articles were eligible for full‐text review, of which 24 met the inclusion criteria and were ultimately included in the systematic review15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38.
Flowchart summarizing inclusion of studies in systematic review, according to predefined criteria. GH, gestational hypertension; PE, pre‐eclampsia.
Characteristics of included studies
Characteristics of the 24 included studies, including the number of PE and non‐PE cases, the method of retinal assessment, the gestational age range at retinal assessment and the retinal parameters examined, are presented in Table 1, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38. The methods of retinal assessment used in the included studies were OCT, optical coherence tomography angiography (OCTA), retinal fundus photography and central retinal artery Doppler.
Grouping studies according to gestational age at retinal examination could not be performed accurately, because the original articles collected data over broad gestational age ranges, and the small study populations did not allow for meaningful comparisons between studies.
Outcomes
Optical coherence tomography
Choroidal thickness, assessed using OCT, was the most commonly examined retinal parameter, reported in 13 studies (Table 2). In women with PE, compared to those without PE, the choroid was thinner in six studies15, 16, 19, 32, 33, 34, thicker in three studies25, 27, 31 and not significantly different in two studies20, 29. The mean difference, with corresponding 95% CI, in choroidal thickness between women with and those without PE in each study is shown in Figure 2. Two studies did not include normotensive controls18, 23. One such study reported that, in women with PE, an increased soluble fms‐like tyrosine kinase‐1 to placental growth factor (sFlt‐1/PlGF) ratio was associated with a decrease in choroidal thickness23. In the other study, an increase in the urine protein‐to‐creatinine ratio was associated with an increase in choroidal thickness in women with PE18.
Forest plot of mean difference (95% CI) in choroidal thickness between women with vs those without pre‐eclampsia. Only first author is given for each study. OD, oculus dexter; OS, oculus sinister.
When examining all other OCT parameters (retinal thickness, retinal nerve fiber layer thickness, macular thickness, ganglion cell layer thickness, choroidal vessel density and total retinal volume), the majority of studies did not find significant differences between women with and those without PE.
Optical coherence tomography angiography
Foveal avascular zone area was examined in five studies; measurements were similar in women with and those without PE17, 19, 22, 28, and among PE pregnancies, measurements were similar in women with high and those with low sFlt‐1/PlGF ratio23 (Table 3). Vessel density in the deep and superficial capillary plexuses was found to be either reduced or not significantly different in women with PE compared to normotensive controls17, 19, 22, 26, 28; no study demonstrated an increase in capillary plexus vessel density in women with PE. One study examined only women with PE and found that vessel density in the deep and superficial capillary plexuses was not associated with the sFlt‐1/PlGF ratio23.
Measures of choriocapillaris blood flow were found to be lower in women with PE compared to normotensive controls in three out of four studies19, 21, 22, 26. Retinal perfusion density was lower in women with PE compared to those without PE in one study17, whereas in another study, retinal blood flow area did not differ significantly between groups26.
Other imaging modalities
In the two studies that used retinal fundus photography, retinal vascular changes were identified in women with PE35, 38 (Table 3). One study reported an overall reduction in corrected central retinal arteriolar and venular equivalents in women with PE compared to those without35. The other study reported a reduced arteriole‐to‐vein ratio in women with severe PE compared to normotensive controls, but there was no significant difference between cases with mild PE and those without PE38.
One study used Doppler to assess the central retinal artery and reported that there was a significantly higher resistance index, but similar peak systolic velocity and end‐diastolic velocity, in those with PE compared to normotensive controls36.
Assessment of quality and risk of bias
The ROBINS‐I V2 tool was used to assess the risk of bias in the included studies (Table 4). In eight studies, there was an overall moderate risk of bias16, 17, 18, 23, 24, 27, 33, 35 and in the other 16, the overall risk of bias was serious15, 19, 20, 21, 22, 25, 26, 28, 29, 30, 31, 32, 34, 36, 37, 38.
DISCUSSION
Main findings and interpretation
The studies included in this systematic review present conflicting findings regarding the effects of PE on the retina and its relevant structures. The discrepancies in choroidal thickness measurements likely reflect differences in disease severity, timing of assessment, imaging protocols and population characteristics. Thinning may indicate choroidal vasoconstriction and hypoperfusion, whereas thickening could represent inflammation, vascular leakage or impaired autoregulation17, 39, 40. Choroidal thinning was also associated with a higher sFlt‐1/PlGF ratio in women with PE in one study23, which could indicate progressive choroidal changes according to disease severity. Despite evidence of functional microvascular alterations in PE, other OCT‐derived parameters remained largely unchanged, suggesting that the gross retinal structure remains relatively preserved, at least in mild‐to‐moderate disease stages.
A higher level of agreement between studies was observed in the OCTA‐based findings. Measurements of choriocapillaris blood flow provided more consistent evidence of microvascular dysfunction, as it was found to be decreased in women with PE in three out of four studies19, 21, 22, 26. This reflects the lack of robust autoregulation of the choroidal vasculature, when compared with the retina, as it is a high‐flow, low‐resistance vascular bed and is highly sensitive to blood pressure alterations41. The possible reduction in vessel density in the superficial and deep capillary plexuses, along with decreased choriocapillaris perfusion, in women with PE likely reflects widespread endothelial dysfunction and impaired vascular autoregulation characteristic of PE pathophysiology.
Furthermore, foveal avascular zone parameters and retinal perfusion density metrics were unchanged in most studies17, 22, 26, 28, highlighting the need to determine which OCTA parameters are most sensitive to PE‐related changes. The lack of correlation between angiogenic markers (e.g. the sFlt‐1/PlGF ratio) and OCTA parameters reported by one study23 suggests that retinal microvascular changes may occur independently of biochemical profiles or may not be captured by current imaging thresholds.
Other modalities offered complementary insights. Retinal fundus photography, utilized by two studies35, 38, revealed reduced retinal vessel calibers in women with PE, particularly in severe cases, consistent with systemic vasoconstriction. A Doppler study of the central retinal artery identified a higher resistance index in women with PE36, supporting the notion of increased downstream vascular resistance, a common feature in hypertensive pregnancies.
It is important to highlight that different imaging modalities provide different information. OCT offers structural insights, whereas OCTA and retinal fundus photography help to visualize blood flow and the retinal vessels, respectively. Despite methodological heterogeneity, the emerging consensus suggests that PE is associated with subtle yet detectable alterations in the retinal microvasculature.
Clinical perspectives
Retinal imaging is appealing in obstetric care due to its non‐invasive and repeatable nature. Zhou et al.42 demonstrated that fundus scores, generated from retinal fundus images obtained before 20 weeks' gestation, can be of value in predicting the subsequent development of PE. Wu et al.43 examined retinal vascular characteristics before 14 weeks as a biomarker for PE screening and predictor of adverse outcome when combined with maternal risk factors and mean arterial pressure. It is therefore possible that, when integrated with maternal cardiovascular assessment and uterine artery Doppler, which was surprisingly not attempted in any of the included studies, retinal imaging could enhance prediction models for PE and potentially guide personalized antenatal care. It is also worth exploring whether the addition of ophthalmic artery Doppler could further strengthen this approach. By detecting early hemodynamic changes, even before overt clinical symptoms of PE appear, ophthalmic artery Doppler could work synergistically with retinal imaging to provide a multimodal, multisystem screening strategy44, 45, 46, 47. Such a model, especially when combined with biomarkers like the sFlt‐1/PlGF ratio, could improve diagnostic precision, enable earlier intervention and reduce maternal−fetal morbidity48.
In addition, there is a large body of evidence examining retinal changes as a precursor of cardiovascular disease in non‐pregnant populations. Retinal imaging could, therefore, help identify those at highest risk of cardiovascular sequelae following the development of PE1, 49, 50.
Future research should aim to address key methodological limitations observed in the current literature. There is a need for prospective, longitudinal studies that assess retinal parameters at multiple timepoints throughout gestation and postpartum, to determine whether these changes precede, accompany or follow the clinical onset of PE. Large multicenter studies should incorporate well‐matched control groups and adjust for relevant confounders such as gestational age, pre‐existing hypertension, maternal body mass index and comorbidities. Finally, correlations with clinical outcomes, including maternal complications, fetal growth restriction and timing of delivery, will be crucial to establish the predictive value and clinical utility of retinal biomarkers.
Strengths and limitations
Although there have been other systematic and narrative reviews on retinal assessment in pregnancies complicated by PE, this is the first to include studies regardless of the method of retinal assessment used and parameters examined, and to do so in a systematic manner. It highlights the variation in retinal imaging findings and possible pathophysiological explanations, ultimately drawing attention to the lack of consensus on the expected effect of PE on the retina.
A limitation of this review, and of the primary literature it encompasses, is the heterogeneity in study design, imaging protocols and population characteristics. Studies were varied in their definition and classification of PE, timing of imaging relative to disease onset, and selection of retinal parameters. Most studies were cross‐sectional, precluding assessment of causality or temporal progression. Lupton et al.35 were the only group that examined the retina in pregnant women from the first trimester onwards, with examinations performed at four different timepoints, and compared the findings between women who subsequently developed PE and those who remained normotensive throughout pregnancy. Their findings suggested that retinal arteriolar narrowing and an increase in peripheral vascular resistance may precede the clinical onset of PE. All other studies included in this systematic review examined women with established PE.
Furthermore, few studies adjusted for important confounders, such as gestational age, maternal body mass index, pre‐existing hypertension or diabetes mellitus — factors that may independently influence retinal vascular parameters51, 52. The small sample sizes and predominance of single‐center studies further limit generalizability and the potential for a meta‐analysis.
Conclusions
Retinal imaging offers a promising, non‐invasive method for assessing microvascular health during pregnancy, and there is emerging evidence of its utility in identifying vascular dysfunction in PE. While findings remain inconsistent, key patterns support the biological plausibility of retinal involvement in PE.
Integration of retinal assessment into obstetric care, especially when combined with Doppler studies and angiogenic markers, could enable a multisystem screening strategy that supports early identification of PE, monitoring of disease progression and tailored intervention. Realizing this potential will require rigorous, standardized research to validate retinal biomarkers as meaningful, predictive tools in maternal health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rolnik DL , Nicolaides KH , Poon LC . Prevention of preeclampsia with aspirin. Am J Obstet Gynecol. 2022;226:S 1108‐S 1119.32835720 10.1016/j.ajog.2020.08.045 · doi ↗ · pubmed ↗
- 2Ahmed R , Dunford J , Mehran R , Robson S , Kunadian V . Pre‐eclampsia and future cardiovascular risk among women: a review. J Am Coll Cardiol. 2014;63:1815‐1822.24613324 10.1016/j.jacc.2014.02.529 · doi ↗ · pubmed ↗
- 3Tooher J , Thornton C , Makris A , et al. Hypertension in pregnancy and long‐term cardiovascular mortality: a retrospective cohort study. Am J Obstet Gynecol. 2016;214(722):e 721‐e 726.10.1016/j.ajog.2015.12.04726739795 · doi ↗ · pubmed ↗
- 4Sibai BM , Ewell M , Levine RJ , et al. Risk factors associated with preeclampsia in healthy nulliparous women. The Calcium for Preeclampsia Prevention (CPEP) Study Group. Am J Obstet Gynecol. 1997;177:1003‐1010.9396883 10.1016/s 0002-9378(97)70004-8 · doi ↗ · pubmed ↗
- 5Dimopoulou S , Neculcea D , Papastefanou I , Galan A , Nicolaides KH , Charakida M . Long‐term cardiovascular assessment of women who had a pregnancy complicated by a hypertensive disorder. Ultrasound Obstet Gynecol. 2024;64(3):308‐313.38437524 10.1002/uog.27632 · doi ↗ · pubmed ↗
- 6Emfietzoglou M , Terentes‐Printzios D , Kotronias RA , et al. The spectrum and systemic associations of microvascular dysfunction in the heart and other organs. Nat Cardiovasc Res. 2022;1:298‐311.39196132 10.1038/s 44161-022-00045-5 · doi ↗ · pubmed ↗
- 7Mayor M , Camafort M , Estruch R . Retinal microvasculature assessment: useful to refine cardiovascular risk. Eur Heart J. 2024;45(33):3086‐3088.39016158 10.1093/eurheartj/ehae 422 · doi ↗ · pubmed ↗
- 8Wong TY , Klein R , Sharrett AR , et al. Retinal arteriolar diameter and risk for hypertension. Ann Intern Med. 2004;140:248‐255.14970147 10.7326/0003-4819-140-4-200402170-00006 · doi ↗ · pubmed ↗