An Unexpected Culprit: Nocardia Pericarditis Leading to Cardiac Tamponade in an Immunocompetent Host With Congenital Heart Disease
Devendra K Jain, Sandeep Seth, Gagandeep Singh, Angitha K Parambath, Shitij Chaudhary

TL;DR
A woman with a heart defect and diabetes developed a rare Nocardia infection causing heart complications, which was successfully treated with antibiotics.
Contribution
This case highlights Nocardia as a rare but important cause of pericarditis in immunocompetent individuals with congenital heart disease.
Findings
Nocardia was identified as the causative agent in a case of pericardial effusion with cardiac tamponade.
Treatment with trimethoprim-sulfamethoxazole led to clinical improvement and resolution of the effusion.
The case emphasizes the need for microbiological testing to avoid misdiagnosis in endemic regions.
Abstract
We report the case of a woman in her 40s with type II diabetes mellitus and a known ostium secundum atrial septal defect (23 mm, left-to-right shunt) diagnosed one year back. The patient presented with progressive dyspnea on exertion for the last three months, along with low-grade fever and fatigue. Clinical and echocardiographic evaluation revealed massive pericardial effusion with features of cardiac tamponade. Pericardial drainage via a pigtail catheter yielded 650 mL of exudative fluid. Pericardial effusion was negative for fungal culture, malignant cytology, and tubercular workup. Adenosine deaminase was negative, and the effusion was predominantly neutrophilic and exudative in nature. The bacterial culture showed the presence of Nocardia. The patient was started on trimethoprim-sulfamethoxazole, following which there was significant improvement in clinical status over the next…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2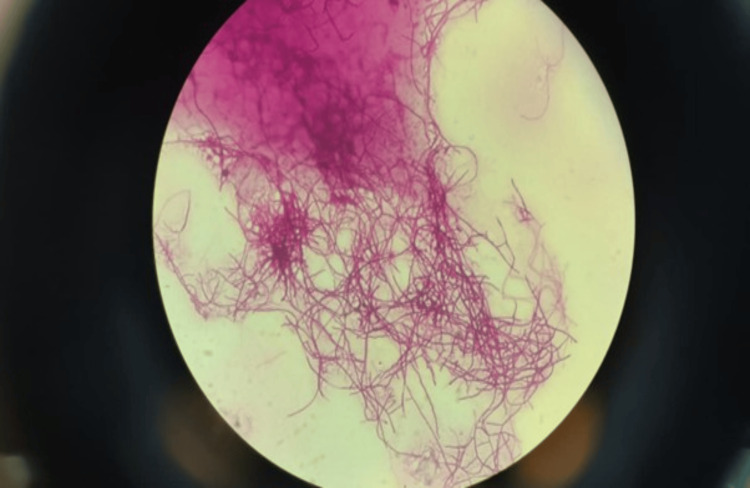 Figure 3
Figure 3| Immunocompromised patients | ||||||
| Age | Gender | Cardiac tamponade | Therapy | Outcome | Underlying condition | Reference |
| 52 | Male | No | IV TMP/SMX + ceftriaxone + amikacin oral amoxicillin/clavulanate + TMP/SMX | Recovered | HIV/AIDS |
[ |
| 32 | Male | No | IV TMP/SMX | Recovered | HIV/AIDS |
[ |
| 34 | Male | No | IV TMP/SMX | Died | HIV/AIDS |
[ |
| 34 | Male | Yes | IV TMP/SMX oral sulfadiazine | Recovered | HIV/AIDS |
[ |
| 42 | Male | No | IV TMP/SMX (allergic) + IV ceftriaxone + minocycline | Recovered | HIV/AIDS |
[ |
| 24 | Female | Yes | Oral TMP/SMX | Recovered | HIV/AIDS |
[ |
| 44 | Male | No | IV TMP/SMX + oral TMP/SMX | Recovered | HIV/AIDS |
[ |
| 35 | Female | Yes | IV TMP/SMX + ceftriaxone + doxycycline + oral TMP/SMX + doxycycline | Recovered | HIV/AIDS |
[ |
| 37 | Male | Yes | IV imipenem/cilastatin + TMP/SMX + oral TMP/SMX | Recovered | HIV/AIDS |
[ |
| 32 | Male | Yes | IV imipenem/cilastatin + TMP/SMX | Died | HIV/AIDS |
[ |
| Immunocompetent patients | ||||||
| 65 | Female | No | IV imipenem/ceftriaxone/linezolid + oral TMP/SMX/doxycycline + oral TMP/SMX | Recovered | - |
[ |
| 60 | Male | Yes | Imipenem/cilastatin + linezolid + TMP/SMX | Recovered | Heavy alcohol use |
[ |
| 63 | Male | No | TMP/SMX | Recovered | - |
[ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Actinomycetales infections and treatment · Lung Cancer Diagnosis and Treatment
Introduction
Pericardial effusion and cardiac tamponade are potentially life-threatening complications that can occur secondary to a wide spectrum of etiologies, including infections, malignancy, autoimmune disorders, and metabolic causes. Among the infectious etiologies, Mycobacterium tuberculosis remains a leading cause of pericarditis in developing countries such as India [1]. Due to a lack of diagnostic facilities, very often, pericardial effusion is attributed to tuberculosis due to its high prevalence.
However, Nocardia species, filamentous, gram-positive and weakly acid-fast aerobic bacteria, represent an exceedingly rare cause of pericardial infection, typically occurring in immunocompromised hosts, such as those with human immunodeficiency virus (HIV) infection, organ transplantation, or long-term corticosteroid use [2]. Due to the similarities in staining characteristics (partially acid-fast) and morphology with Mycobacterium tuberculosis, nocardiosis is frequently misdiagnosed as tuberculosis [3]. In immunocompetent individuals, nocardial pericarditis is exceptionally uncommon, with only isolated cases described in the literature. The clinical presentation often mimics tuberculous pericarditis, leading to diagnostic delays and inappropriate therapy [3]. Microbiological confirmation through prolonged culture and modified Ziehl-Neelsen staining remains the cornerstone of diagnosis [2].
We report a rare case of massive pericardial effusion in a middle-aged woman with a background of atrial septal defect (ASD), where Nocardia species was isolated from pericardial fluid. The patient was immunocompetent and initially treated empirically for tuberculous pericarditis. This case highlights the importance of maintaining a high index of suspicion for atypical organisms such as Nocardia, even in immunocompetent hosts, especially in endemic settings where tuberculosis is the default diagnosis for exudative pericardial effusions.
Case presentation
A woman in her 40s, a known case of type II diabetes mellitus and congenital heart disease with ostium secundum ASD (23 mm in size, with left-to-right shunt), presented with progressive dyspnea over one year, worsening during the preceding three months, associated with low-grade fever and fatigue for two weeks. There was no prior history of tuberculosis or immunosuppressive drug use.
On admission, the patient was afebrile, with a blood pressure of 110/70 mm Hg, heart rate of 125 beats/minute, respiratory rate of 30 breaths/minute, and oxygen saturation of 98% on room air. Jugular venous pressure was elevated, and heart sounds were muffled. There was no pedal edema, hepatomegaly, or pulsus paradoxus. The electrocardiogram demonstrated right bundle branch block with right-axis deviation. Transthoracic echocardiography revealed a large circumferential pericardial effusion with right atrial diastolic collapse, preserved left ventricular systolic function, and a 23-mm ostium secundum ASD with left-to-right shunt, consistent with impending pericardial tamponade. Chest radiograph showed an enlarged cardiac silhouette and clear lung fields (Figure 1).
Chest radiograph (anteroposterior view) showing an enlarged cardiac silhouette (“water-bottle” sign of pericardial effusion).
An emergency ultrasound-guided pericardiocentesis was performed, yielding approximately 650 mL of blood-tinged, exudative fluid, and a pigtail catheter was left in situ for drainage. Pericardial fluid analysis revealed an albumin of 2.7 g/dL (serum albumin: 3.8 g/dL), total protein of 5.5 g/dL (serum protein: 7.2 g/dL), lactate dehydrogenase (LDH) of 486 U/L (serum LDH: 526 U/L), glucose of 164 mg/dL (blood glucose: 182 mg/dL), and amylase of 42 U/L. Cytology did not show any evidence of malignancy. The total leukocyte count was 10,000/mm³ with 80% polymorphonuclear and 20% mononuclear cells. The patient was initially started on empiric antitubercular therapy (isoniazid 300 mg + rifampin 600 mg + pyrazinamide 1,500 mg + ethambutol 1,200 mg) once daily. Acid-fast bacilli stain, GeneXpert, and KOH mount were all negative, and adenosine deaminase (ADA) was 13 U/L (normal value <30 U/L). Gram staining showed filamentous, branching, gram-positive bacilli. Modified Ziehl-Neelsen staining showed weakly acid-fast bacilli. After seven days of incubation on blood agar, chalk-white, dry colonies appeared, confirming Nocardia spp. (Figures 2, 3). During this time, the patient continued to have low-grade fever with the pericardial catheter draining hemorrhagic fluid.
Blood agar plate showing dry, pitting colonies of Nocardia spp.
Thin, branching, filamentous acid-fast bacilli (magnification: 1,000×) grown on culture suggestive of Nocardia spp.
Species-level identification with matrix-assisted laser desorption/ionization with tandem time-of-flight analysis revealed Nocardia brasiliensis. The patient was immunocompetent. HIV enzyme-linked immunosorbent assay, anti-hepatitis C virus, and hepatitis B surface antigen were negative. HbA1c was 6.8%, thyroid-stimulating hormone was within the normal range, erythrocyte sedimentation rate (ESR) was 52 mm/hour, and total leukocyte count was normal. Based on the culture result, the diagnosis of nocardial pericarditis with tamponade was established. Infectious disease consultation advised discontinuation of antitubercular therapy and initiation of therapy with trimethoprim-sulfamethoxazole (TMP-SMX) (160 mg/800 mg two tablets twice daily) and linezolid 600 mg twice daily. Subsequently, antimicrobial susceptibility testing showed sensitivity to imipenem, linezolid, minocycline, amoxicillin-clavulanate, ceftriaxone, and ciprofloxacin, and resistance to TMP-SMX. The patient was continued on linezolid 600 mg twice daily along with amoxicillin-clavulanate (500 mg/125 mg one tablet thrice daily), with a planned duration of six months. A CT scan of the chest and abdomen showed subcentimetric mediastinal lymph nodes with no other focus of Nocardial infection. The patient’s dyspnea improved steadily over the next seven days, with no recurrence of effusion on repeat echocardiography. She remained afebrile, hemodynamically stable, and inflammatory markers normalized (ESR: 15 mm/hour). The pericardial catheter was subsequently removed once the drainage was less than 50 mL for two consecutive days, and the patient was discharged. Follow-up after three days of discharge showed clinical stability and no evidence of re-accumulation on echocardiography. At one-month review, she remained asymptomatic (New York Heart Association Class I) with normal left ventricular function and no pericardial collection. Long-term follow-up was planned to monitor for relapse or medication toxicity.
Discussion
Nocardial pericarditis is an exceedingly rare entity, particularly in immunocompetent individuals, and poses a significant diagnostic challenge due to its nonspecific presentation and slow-growing nature, requiring selective culture media. Nocardial infections can be acquired through various routes, including inhalation, ingestion, and direct inoculation of the skin. Nocardia species can hematogenously disseminate and involve multiple organ systems, with pulmonary-limited infection reported in approximately 39% of cases, central nervous system involvement in 9%, cutaneous disease in 8%, and disseminated infections in 32%; pericardial involvement is very rare and can occasionally present as purulent effusions requiring drainage [4]. While Nocardia species leading to infective endocarditis in congenital heart disease is well-known, nocardial pericarditis in congenital heart disease has not been previously documented [5]. Among pathogenic species, N. asteroides accounts for the majority of respiratory and disseminated infections, whereas N. farcinica is more virulent, prone to antibiotic resistance, and has a higher propensity for dissemination [6].
Most nocardial infections occur in immunocompromised hosts, such as those with HIV infection, organ transplantation, or other conditions impairing cell-mediated immunity [7]. Diabetes may confer a subtle predisposition even when well-controlled, as in our patient [8]. Table 1 summarizes cases of Nocardia pericarditis reported in the literature in immunocompromised and immunocompetent patients [9-20]. Clinically, nocardial pericarditis can closely mimic tuberculous pericarditis, especially in endemic regions, with massive pericardial effusions, blood-tinged exudates, and elevated inflammatory markers [9]. Differentiating features include polymorphonuclear predominance in pericardial fluid, normal ADA levels, partial acid-fastness on modified Ziehl-Neelsen staining, and a negative GeneXpert, highlighting the importance of microbiological confirmation before initiating long-term empiric therapy [9]. Prompt pericardial drainage combined with prolonged targeted antibiotic therapy, typically TMP-SMX, is essential to prevent tamponade and ensure favorable outcomes. Alternative drugs, such as linezolid, meropenem, imipenem, amikacin, ceftriaxone, and amoxicillin-clavulanate, can also be used alone or in combination, based on local epidemiology and susceptibility profiles [8,9]. Our patient, an immunocompetent middle-aged woman with a congenital ASD, demonstrated gradual clinical improvement and near-complete resolution of pericardial effusion following drainage and linezolid and amoxicillin-clavulanate therapy, underscoring the need for high clinical suspicion for atypical organisms such as *Nocardia *even in patients without classic risk factors, as well as the value of early intervention and careful follow-up to ensure complete recovery.
Conclusions
While tuberculosis remains the most common diagnosis for exudative effusions in tuberculosis-endemic countries, it must not be assumed without microbiological confirmation. *Nocardia *pericarditis can mimic tubercular pericarditis. Therefore, a high index of suspicion must be maintained for atypical microorganisms in the diagnosis of pericardial effusion. Early microbiological diagnosis and targeted antimicrobial therapy are the key to optimal patient response and outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Demographic, clinical and etiological profile of pericardial effusion in India: a single centre experience Indian J Tuberc Pradhan A Vishwakarma P Bhandari M 2202266920223537940510.1016/j.ijtb.2021.08.023 · doi ↗ · pubmed ↗
- 2Nocardiosis: risk factors, clinical characteristics and outcome Iran Red Crescent Med J Alavi Darazam I Shamaei M Mobarhan M Ghasemi S Tabarsi P Motavasseli M Mansouri D 4364391520132434973510.5812/ircmj.2384 PMC 3838657 · doi ↗ · pubmed ↗
- 3Pulmonary nocardiosis in suspected tuberculosis patients: a systematic review and meta-analysis of cross-sectional studies Ethiop J Health Sci Mehrabadi SM Taraghian M Pirouzi A Khaledi A Neshani A Rashki S 2933003020203216581910.4314/ejhs.v 30i 2.17PMC 7060384 · doi ↗ · pubmed ↗
- 4Nocardia and Actinomyces Medicine (Baltimore) Henderson NM Sutherland RK 06452017
- 5Infective endocarditis by Nocardia species: a systematic review J Chemother Velidakis A Degaitis F Tsorbatzoglou G Ioannou P 1731803520233578715110.1080/1120009 X.2022.2095154 · doi ↗ · pubmed ↗
- 6Nocardia farcinica infection presenting as a solitary bronchial neoplasm in an immunocompetent adult: a case report Front Med (Lausanne) Tan Y Yang M Wan C Tang S Liu L Chen L 13373031020233827445410.3389/fmed.2023.1337303 PMC 10809415 · doi ↗ · pubmed ↗
- 7Nocardia infections in the immunocompromised host: a case series and literature review Microorganisms Palomba E Liparoti A Tonizzo A 11201020223574463810.3390/microorganisms 10061120 PMC 9229660 · doi ↗ · pubmed ↗
- 8Invasive nocardiosis: disease presentation, diagnosis and treatment - old questions, new answers?Infect Drug Resist Lafont E Conan PL Rodriguez-Nava V Lebeaux D 460146131320203337636610.2147/IDR.S 249761 PMC 7764858 · doi ↗ · pubmed ↗