Impact of COVID-19 on national health screening participation and chronic disease detection: evidence from South Korea’s NHIS database
Sunyoung Kim, Hyejin Lee, Jungha Park, Sujeong Han, Hye Yeon Koo, Eunbyul Cho, Haeung Song, Bumjo Oh

TL;DR
The study found that despite a drop in health screenings during the pandemic in South Korea, more chronic diseases were still detected, showing the health system's resilience.
Contribution
The paper provides new evidence on how reduced health screening participation during the pandemic did not lead to fewer chronic disease diagnoses.
Findings
Health screening participation dropped from 75.4% in 2019 to 68.7% in 2020.
New diagnoses of chronic diseases increased by 550,000 cases in 2020 compared to 2019.
Chronic disease detection increased despite lower screening rates, indicating alternative diagnostic pathways.
Abstract
The COVID-19 pandemic disrupted preventive healthcare services worldwide, raising concerns about missed diagnoses of chronic diseases. South Korea’s national health screening program experienced a substantial decline in participation during 2020. This study investigated how changes in screening rates influenced chronic disease detection and what these shifts reveal about the resilience of the national health system. Using the Korea Disease Control and Prevention Agency-National Health Insurance Service (K-COV-N) database, we analyzed trends in national health screening participation (2010–2020) and new diagnoses of hypertension, diabetes mellitus, and dyslipidemia before (2019) and during (2020) the COVID-19 pandemic. Analyses were stratified by sex and 10-year age groups to partially control for confounding factors. Relative risks (RRs) and 95% confidence intervals (CIs) for newly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
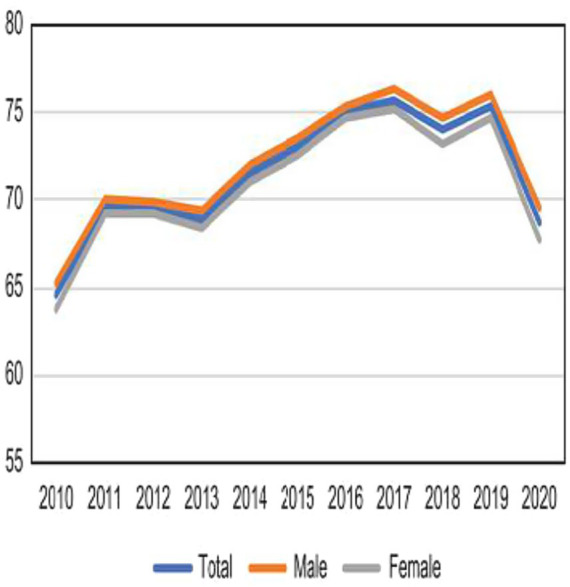 Figure 1
Figure 1| Age (years) | 2010, N (%) | 2011, N (%) | 2012, N (%) | 2013, N (%) | 2014, N (%) | 2015, N (%) | 2016, N (%) | 2017, N (%) | 2018, N (%) | 2019, N (%) | 2020, N (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | All | 7,671,714 (64.59) | 8,019,396 (69.65) | 8,464,871 (69.59) | 8,634,169 (68.87) | 9,486,352 (71.52) | 10,238,371 (73.1) | 10,724,742 (75.02) | 10,995,640 (75.75) | 11,219,154 (73.96) | 11,592,643 (75.39) | 10,392,121 (68.72) |
| 40–49 | 2,893,186 (63.25) | 2,987,807 (68.59) | 3,038,660 (68.55) | 3,139,333 (68.58) | 3,338,836 (72) | 3,562,858 (74.06) | 3,640,093 (76.41) | 3,646,628 (77.47) | 3,530,415 (76.71) | 3,633,855 (77.54) | 3,124,468 (70.69) | |
| 50–59 | 2,478,099 (67.33) | 2,631,127 (72.47) | 2,830,566 (71.87) | 2,833,405 (70.35) | 3,144,926 (72.76) | 3,379,521 (73.81) | 3,494,580 (75.92) | 3,567,171 (76.71) | 3,643,103 (75.57) | 3,711,838 (76.44) | 3,350,420 (70.77) | |
| 60–69 | 1,470,560 (71.27) | 1,482,665 (76.18) | 1,594,604 (75.45) | 1,620,317 (74.99) | 1,836,196 (76.37) | 2,050,946 (77.75) | 2,238,568 (78.99) | 2,348,001 (79.41) | 2,485,591 (77.64) | 2,638,830 (78.4) | 2,512,142 (71.8) | |
| ≥70 | 829,869 (53.25) | 917,797 (58.08) | 1,001,041 (59.59) | 1,041,114 (58.81) | 1,166,394 (61.38) | 1,245,046 (62.94) | 1,351,501 (64.51) | 1,433,840 (65.15) | 1,560,045 (61.3) | 1,608,120 (65.11) | 1,405,091 (56.88) | |
| Male | All | 3,948,541 (65.35) | 4,079,129 (70.14) | 4,328,723 (69.9) | 4,380,086 (69.36) | 4,840,238 (72.05) | 5,227,472 (73.62) | 5,435,966 (75.38) | 5,550,927 (76.32) | 5,684,963 (74.78) | 5,840,617 (76.04) | 5,307,281 (69.6) |
| 40–49 | 1,576,828 (63.86) | 1,619,383 (69.15) | 1,647,060 (69.07) | 1,698,117 (69.57) | 1,807,877 (72.89) | 1,921,254 (74.96) | 1,955,776 (77.22) | 1,954,705 (78.49) | 1,921,820 (78.01) | 1,963,973 (78.96) | 1,734,492 (72.65) | |
| 50–59 | 1,269,410 (66.25) | 1,316,175 (70.83) | 1,452,881 (70.37) | 1,423,442 (68.72) | 1,612,856 (71.57) | 1,730,669 (72.41) | 1,771,386 (74.36) | 1,791,118 (75.31) | 1,837,779 (74.15) | 1,856,608 (75.17) | 1,690,115 (69.36) | |
| 60–69 | 728,561 (71.01) | 731,667 (75.66) | 779,207 (74.4) | 792,334 (73.89) | 901,031 (75.27) | 1,010,923 (76.75) | 1,098,299 (77.67) | 1,152,770 (78.24) | 1,217,817 (76.15) | 1,282,265 (76.94) | 1,219,527 (70.37) | |
| ≥70 | 373,742 (59.21) | 411,904 (63.49) | 449,575 (64.57) | 466,193 (63.8) | 518,474 (65.86) | 564,626 (68.03) | 610,505 (69.19) | 652,334 (70.04) | 707,547 (66.69) | 737,771 (69.74) | 663,147 (62.08) | |
| Female | All | 3,723,173 (63.81) | 3,940,267 (69.16) | 4,136,148 (69.27) | 4,254,083 (68.38) | 4,646,114 (70.98) | 5,010,899 (72.57) | 5,288,776 (74.65) | 5,444,713 (75.19) | 5,534,191 (73.13) | 5,752,026 (74.74) | 5,084,840 (67.82) |
| 40–49 | 1,316,358 (62.52) | 1,368,424 (67.93) | 1,391,600 (67.95) | 1,441,216 (67.45) | 1,530,959 (70.97) | 1,641,604 (73.03) | 1,684,317 (75.49) | 1,691,923 (76.32) | 1,608,595 (75.21) | 1,669,882 (75.94) | 1,389,976 (68.4) | |
| 50–59 | 1,208,689 (68.5) | 1,314,952 (74.2) | 1,377,685 (73.52) | 1,409,963 (72.07) | 1,532,070 (74.07) | 1,648,852 (75.33) | 1,723,194 (77.59) | 1,776,053 (78.18) | 1,805,324 (77.07) | 1,855,230 (77.75) | 1,660,305 (72.26) | |
| 60–69 | 741,999 (71.52) | 750,998 (76.69) | 815,397 (76.48) | 827,983 (76.08) | 935,165 (77.46) | 1,040,023 (78.76) | 1,140,269 (80.32) | 1,195,231 (80.57) | 1,267,774 (79.14) | 1,356,565 (79.82) | 1,292,615 (73.21) | |
| ≥70 | 456,127 (49.18) | 505,893 (54.32) | 551,466 (56.07) | 574,921 (55.31) | 647,920 (58.22) | 680,420 (59.26) | 740,996 (61.11) | 781,506 (61.57) | 852,498 (57.44) | 870,349 (61.64) | 741,944 (52.92) |
| Diagnosis | Total | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2019, N (%) | 2020, N (%) | Change | 2019, N (%) | 2020, N (%) | Change | 2019, N (%) | 2020, N (%) | Change | |
| Total | 28,995,763 (100) | 29,548,301 (100) | 552,538 | 14,039,493 (100) | 14,315,625 (100) | 276,132 | 14,956,270 (100) | 15,232,676 (100) | 276,406 |
| Hypertension | 9,735,495 (33.58) | 10,068,281 (34.07) | 332,786 (0.49) | 4,879,765 (34.76) | 5,082,321 (35.5) | 202,556 (0.74) | 4,855,730 (32.47) | 4,985,960 (32.73) | 130,230 |
| Diabetes mellitus | 6,470,991 (22.32) | 6,714,221 (22.72) | 243,230 (0.4) | 3,285,561 (23.4) | 3,427,355 (23.94) | 141,794 (0.54) | 3,185,430 (21.3) | 3,286,866 (21.58) | 101,436 |
| Dyslipidemia | 10,806,197 (37.27) | 11,279,735 (38.17) | 473,538 (0.9) | 5,045,544 (35.94) | 5,294,398 (36.98) | 248,854 (1.04) | 5,760,653 (38.52) | 5,985,337 (39.29) | 224,684 |
| Angina | 1,562,856 (5.39) | 1,549,149 (5.24) | −13,707 | 848,406 (6.04) | 855,393 (5.98) | 6,987 | 714,450 (4.78) | 693,756 (4.55) | −20,694 |
| Myocardial infarction | 730,146 (2.52) | 725,233 (2.45) | −4,913 | 445,954 (3.18) | 453,322 (3.17) | 7,368 | 284,192 | 271,911 (1.79) | −12,281 |
| Heart failure | 786,684 (2.71) | 827,528 (2.8) | 40,844 (0.09) | 382,853 (2.73) | 408,363 (2.85) | 25,510 (0.12) | 403,831 | 419,165 (2.75) | 15,334 |
| Cerebral hemorrhage | 153,574 (0.53) | 150,564 (0.51) | −3,010 | 76,752 (0.55) | 75,216 (0.53) | −1,536 | 76,822 | 75,348 (0.49) | −1,474 |
| Cerebral infarction | 859,352 (2.96) | 845,262 (2.86) | −14,090 | 443,109 (3.16) | 442,445 (3.09) | −664 | 416,243 (2.78) | 402,817 (2.64) | −13,426 |
| Osteoarthritis | 7,029,165 (24.24) | 6,795,735 (23) | −233,430 | 2,503,485 (17.83) | 2,464,697 (17.22) | −38,788 | 4,525,680 (30.26) | 4,331,038 (28.43) | −194,642 |
| Osteoporosis | 2,827,884 (9.75) | 2,831,915 (9.58) | 4,031 | 310,827 (2.21) | 314,046 (2.19) | 3,219 | 2,517,057 (16.83) | 2,517,869 (16.53) | 812 |
| Total | Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 2019, N (%) | 2020, N (%) | RR | 2019, N (%) | 2020, N (%) | RR | 2019, N (%) | 2020, N (%) | RR | |
| Hypertension | 31,771 | 32,615 | 1.0266 | 34,262 | 35,345 | 1.0316 | 29,242 | 29,766 | 1.0179 |
| Diabetes mellitus | 21,480 | 22,440 | 1.0447 | 22,930 | 23,879 | 1.0414 | 20,007 | 20,938 | 1.0465 |
| Dyslipidemia | 39,957 | 42,167 | 1.0553 | 38,767 | 40,874 | 1.0543 | 41,165 | 43,517 | 1.0571 |
| Angina | 4,775 | 4,661 | 0.9761 | 5,496 | 5,446 | 0.9907 | 4,043 | 3,843 | 0.9504 |
| Myocardial infarction | 2,121 | 2079 | 0.9806 | 2,753 | 2,741 | 0.9958 | 1,479 | 1,389 | 0.9392 |
| Heart failure | 2020 | 2085 | 1.0323 | 2,159 | 2,262 | 1.0476 | 1879 | 1901 | 1.0117 |
| Cerebral hemorrhage | 316 | 294 | 0.9287 | 319 | 294 | 0.9194 | 314 | 294 | 0.9383 |
| Cerebral infarction | 1995 | 1865 | 0.9349 | 2,220 | 2,106 | 0.9488 | 1767 | 1,614 | 0.9134 |
| Osteoarthritis | 24,808 | 24,040 | 0.969 | 18,504 | 18,167 | 0.9818 | 31,209 | 30,169 | 0.9667 |
| Osteoporosis | 9,746 | 9,873 | 1.013 | 1985 | 2003 | 1.0095 | 17,627 | 18,086 | 1.0261 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Promotion and Cardiovascular Prevention · Data-Driven Disease Surveillance · COVID-19 Digital Contact Tracing
Introduction
1
During the coronavirus disease 2019 (COVID-19) pandemic, some form of lockdown was implemented across almost every country in the world. In South Korea, despite the absence of an official government lockdown, many individuals refrained from going outside because of the fear of contracting SARS-CoV-2. This apprehension was particularly pronounced in relation to visiting hospitals, as individuals expressed concerns about potential contamination by the virus. Access to healthcare services for health promotion and prevention has decreased during the COVID-19 epidemic (1).
In South Korea, national health checkups have been performed since 1980; they have affected health promotion, diagnosis, and treatment of chronic diseases and cancer (1). The target population comprises individuals aged ≥20 years in South Korea (2). According to 2018 data from the Korean National Health Insurance Service (NHIS), 23.5% of those who underwent health checkups were diagnosed with diseases, and 30.4% were suspected of having diseases, emphasizing the importance of comprehensive examinations to identify potential health problems (3).
Before the COVID-19 pandemic, because of proactive promotion of health checkups by the government and hospitals, the national health checkup rate had been steadily increasing. However, with the onset of the COVID-19 pandemic in 2020, the national health checkup rate plummeted (Figure 1).
Trends in national general health screening participation, 2010–2020 announced by Statistics Korea.
According to mortality statistics reported by Statistics Korea, the leading causes of death remained largely consistent between 2019 and 2020, with cancer, heart disease, and pneumonia topping the list (4, 5). Despite the COVID-19 pandemic, the rankings and mortality rates of causes of death showed no significant difference, except for sepsis. In addition to mortality, these chronic diseases significantly challenge daily functioning and have a considerable economic impact (6).
Studies investigating the association between health checkups and chronic disease diagnoses have consistently demonstrated that national health examinations reduce the incidence and mortality rates of stroke and myocardial infarction (MI) (7, 8). Recent studies have also highlighted the challenges in post-pandemic screening recovery (9) and the importance of maintaining preventive services (10). Moreover, public health researchers support the claim that routine general healthcare screening can effectively reduce the incidence and mortality rates of chronic diseases (7, 10–14).
Therefore, whether during a pandemic or not, early detection and management of chronic diseases help reduce mortality rates. This study aims to answer the following research question: How did the pandemic-induced decline in screening rates influence the detection of major chronic diseases? We hypothesized that while screening participation decreased, alternative diagnostic pathways would mitigate the impact on disease detection. We analyzed the health checkup rate and number of newly diagnosed cases of chronic diseases in 2019, before the COVID-19 pandemic, and during the period corresponding to the COVID-19 pandemic in 2020.
Methods
2
National screening program in South Korea
2.1
South Korea operates a national health checkup program. The target population comprised adults aged ≥20 years, allowing for a health checkup every 2 years. The tests include medical examination, blood pressure measurement, fasting blood glucose testing, and lipid profile testing. The NHIS oversees the national health screening program and repeatedly encourages individuals who have not undergone screening to do so.
Study design and population
2.2
This study employed a retrospective cohort design that focused on adults aged ≥40 years. This study used data encompassing the national general checkup rates from January 2010 to December 2020 and the incidence rates of chronic diseases from January 2019 to December 2020. The primary objectives were to assess fluctuations in health examination rates and analyze the rates of new diagnoses of chronic diseases before and after the onset of the COVID-19 pandemic.
Data collection
2.3
Data from the Korea Disease Control and Prevention Agency-COVID-19-National Health Insurance Service (K-COV-N) were used. Chronic diseases were classified into categories including HTN, DM, DL, cardiovascular disease, cerebrovascular disease, and joint diseases. The diagnostic codes used were based on KCD-7 and ICD-10. Specific codes included HTN (I10–15), DM (E10–14), and DL (E78) (11).
To ensure the identification of new diagnoses, if the diagnostic code for a chronic disease was previously recorded at least once, it was excluded from the analysis. We included adults aged ≥40 years who had at least one NHIS record between 2019 and 2020. Missing or duplicate entries (<0.3%) were removed according to NHIS data-validation procedures.
Participants were categorized as “screened” if they completed a health checkup in the given year and “not screened” otherwise. Furthermore, the calculations included only individuals with examination records for a given year.
Ethical approval
2.4
All procedures in this study were conducted in compliance with relevant laws and institutional guidelines and were approved by the Institutional Review Board (IRB) of Kyung Hee University Hospital. The privacy rights of all human subjects were strictly protected, and data were handled in accordance with institutional and regulatory guidelines.
Statistical analysis
2.5
Using percentages, the proportion of individuals who underwent health checkups was determined. We calculated relative risks (RRs) and 95% confidence intervals (CIs) to quantify the difference in new diagnosis rates between the screened and non-screened groups. RRs were calculated using the formula RR = [a/(a + b)] / [c/(c + d)], and 95% CIs were derived using the Wald method. Analyses were stratified by sex and 10-year age groups to partially control for confounding factors.
All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Two-tailed p-values < 0.05 were considered statistically significant. Due to the anonymized nature of the K-COV-N dataset, detailed socioeconomic status (SES) and regional variables were unavailable for analysis; this limitation is further addressed in the Discussion section.
Results
3
General health screening from 2010 to 2020
3.1
The number of health checkups increased from 2010 (7.7 million cases, 64.6%) to 2019 (11.6 million cases, 75.54%) but decreased in 2020 (11.4 million cases, 68.7%) during the COVID-19 pandemic. Except for 2018 and 2019, most examinees were in their 40s, and there were more male examinees than female examinees in all years (Figure 1 and Table 1).
New diagnoses and changes in the diagnoses of chronic diseases
3.2
In 2020, new diagnoses of chronic diseases increased by 552,538 compared with the previous year (2019). As shown in Table 2, the diagnosis rates of HTN, DM, and DL increased by 0.49, 0.4, and 0.9%, respectively. Among cardiovascular diseases, the diagnosis rates of angina (−0.15%) and MI (−0.07%) decreased. Among cerebrovascular diseases, the diagnosis rates of CH (−0.02%) and cerebral infarction (−0.1%) decreased. Detailed stratifications by age and sex are provided in Supplementary Table S1.
Relative risks of new diagnoses among screened vs. non-screened individuals
3.3
Compared with the period before the COVID-19 pandemic, the relative risk (RR) for new diagnoses following the pandemic was >1 for HTN, DM, and DL among those who underwent screenings. As detailed in Table 3, the RRs (95% CI) were 1.0266 (1.0253–1.0278) for HTN, 1.0447 (1.0431–1.0464) for DM, and 1.0553 (1.0543–1.0564) for DL.
Conversely, cardiovascular diseases showed RRs of 0.9761 (95% CI, 0.9724–0.9798) for angina and 0.9806 (95% CI, 0.975–0.9862) for MI. Among cerebrovascular diseases, the RRs were 0.9287 (95% CI, 0.9147–0.9429) for CH and 0.9349 (95% CI, 0.9294–0.9405) for cerebral infarction.
Discussion
4
This study identified the association between health checkups and new diagnoses of chronic diseases. Whether the COVID-19 pandemic increased or decreased the prevalence of chronic diseases remains controversial. Several studies have reported conflicting findings (15).
However, before and after the COVID-19 pandemic, the number of new diagnoses of chronic diseases, such as HTN, DM, and DL, increased. Notably, the RR of a new chronic disease diagnosis for the 2 years before and after COVID-19 was consistently higher among those who underwent health checkups than among those who did not (16).
In Korea, the steadily increasing health checkup rates from 2010 to 2019 can be attributed to the concerted efforts of the government. However, the impact of the COVID-19 pandemic has been significant and rapidly decreased the number of individuals undergoing health checkups. This decline can be attributed to reduced hospital visits and postponement of scheduled examinations because of the pandemic (16). Behavioral barriers, including fear of infection and reduced willingness to participate in preventive health screenings, have also been documented during the pandemic (19–21).
Despite the decrease in health screening rates, we observed more newly diagnosed chronic diseases. This finding suggests a behavioral and systemic shift rather than a direct causal contradiction. The expansion of telemedicine and pharmacy-based monitoring partially compensated for reduced screening access, allowing for the continued identification of symptomatic cases. Although the overall hospital utilization rate decreased, awareness of individual health increased, which may have increased new diagnoses of certain chronic diseases through alternative diagnostic pathways.
Comparing internationally, South Korea’s rapid resumption of preventive services contrasts with countries like the United Kingdom, where screening backlogs persisted longer. Similar to Japan, Korea’s universal health insurance system provided a resilient foundation, although disparities remained.
The numbers of new diagnoses of cardiovascular diseases other than HF, particularly angina, MI, and cerebrovascular disease, were similar before and after the COVID-19 pandemic. These diseases are often diagnosed after emergency room treatment rather than routine examinations. Previous studies have reported reduced emergency department visits and decreased in-person outpatient care utilization during the COVID-19 pandemic (16–18). Thus, their new diagnosis may not have been closely related to a checkup or clinic visit.
Limitations
4.1
This study has several limitations. First, the observation period was limited to 2 years (2019–2020), which may not capture the long-term effects of the pandemic. Second, due to the nature of the K-COV-N database, we could not control for detailed socioeconomic status or regional variations (urban vs. rural), which are known confounders in healthcare access. Third, there is a potential selection bias, as individuals who are more health-conscious may have been more likely to undergo screening during the pandemic, potentially skewing the detection rates. Finally, our findings represent associations and should be interpreted with caution regarding causality.
Conclusion
5
The COVID-19 pandemic disrupted preventive healthcare but did not eliminate chronic disease detection in South Korea. The findings suggest that while population-level screening decreased, healthcare systems and individuals adapted through alternative diagnostic routes.
To strengthen health system resilience against future public health emergencies, we recommend integrating digital health strategies and ensuring equity-oriented screening programs. As noted by recent studies, the digital transformation of preventive services is crucial for maintaining continuity of care. These findings underscore the importance of resilient yet uneven health systems that maintain continuity of essential services during public health crises.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kang HT. Current status of the national health screening programs in South Korea. Korean J Fam Med. (2022) 43:168–73. doi: 10.4082/kjfm.22.0052, 35610963 PMC 9136500 · doi ↗ · pubmed ↗
- 2Lee H Cho J Shin DW Lee SP Hwang SS Oh J . Association of cardiovascular health screening with mortality, clinical outcomes, and health care cost: a nationwide cohort study. Prev Med. (2015) 70:19–25. doi: 10.1016/j.ypmed.2014.11.007, 25445334 · doi ↗ · pubmed ↗
- 3Corporation NHI. 2018 National Health Screening Statistical Yearbook National Health Insurance Service (2018).
- 4Noh H Seo J Lee S Yi N Park S Choi YJ . Cause-of-death statistics in 2020 in the Republic of Korea. J Korean Med Assoc. (2023) 66:132–42.
- 5Noh H Seo J Lee S Yi N Park S Huh S. Statistical analysis of the cause of death in Korea in 2019. J. Korean Med. Assoc. (2022) 65:748–57.
- 6Prince MJ Wu F Guo Y Gutierrez Robledo LM O'Donnell M Sullivan R . The burden of disease in older people and implications for health policy and practice. Lancet. (2015) 385:549–62. doi: 10.1016/S 0140-6736(14)61347-7, 25468153 · doi ↗ · pubmed ↗
- 7Cho JH Han KD Jung HY Bond A. National health screening may reduce cardiovascular morbidity and mortality among the elderly. Public Health. (2020) 187:172–6. doi: 10.1016/j.puhe.2020.08.010, 32992163 · doi ↗ · pubmed ↗
- 8Krogsbøll LT Jørgensen KJ Grønhøj Larsen C Gøtzsche PC. General health checks in adults for reducing morbidity and mortality from disease: Cochrane systematic review and meta-analysis. BMJ. (2012) 345:e 719123169868 10.1136/bmj.e 7191 PMC 3502745 · doi ↗ · pubmed ↗