Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's disease
Shanshan Huang, Yunyun Guo

TL;DR
This study compares nine drugs for Alzheimer's disease and finds no strong evidence that they improve cognitive function more than a placebo.
Contribution
The study provides a network meta-analysis ranking nine Alzheimer's drugs based on cognitive outcomes.
Findings
No drug showed statistically significant superiority over placebo in primary cognitive outcomes.
Semorinemab and tilavonemab had the highest rankings but no significant pairwise advantage.
Aducanumab showed a modest benefit on MMSE, but results may be biased by publication bias.
Abstract
Alzheimer's disease (AD) remains a global challenge, and the comparative cognitive efficacy of emerging pharmacotherapies is still unclear. To compare and rank nine pharmacological agents against placebo in AD with respect to key cognitive outcomes using a network meta-analysis. We systematically searched randomized controlled trials published up to May 2025 that evaluated aducanumab, lecanemab, donanemab, gosuranemab, semorinemab, tilavonemab, zagotenemab, masupirdine, or sodium oligomannate in AD. The primary outcomes were Clinical Dementia Rating–Sum of Boxes (CDR-SB) and Alzheimer's Disease Assessment Scale–Cognitive Subscale (ADAS-cog); Mini-Mental State Examination (MMSE) was a secondary outcome. Treatments were ranked using the Surface Under the Cumulative Ranking curve (SUCRA). Fifteen randomized trials encompassing 33 treatment arms were included. No drug demonstrated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
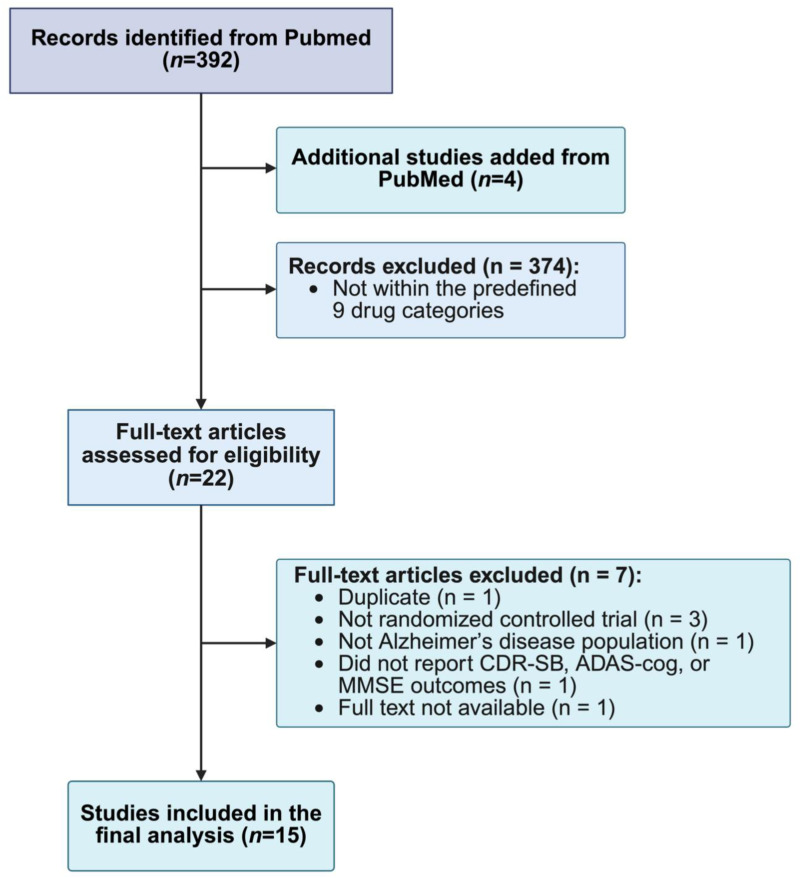 Figure 1
Figure 1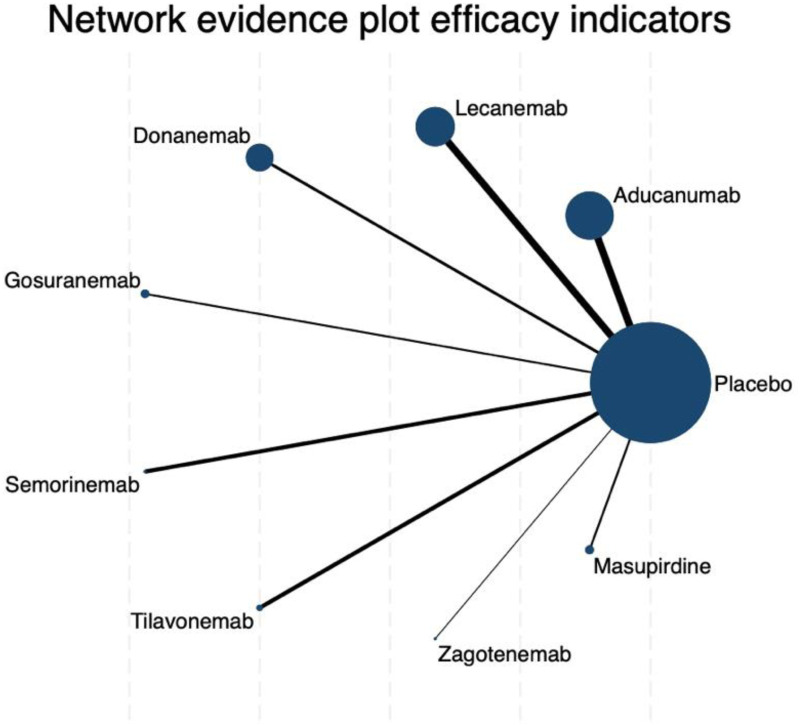 Figure 2
Figure 2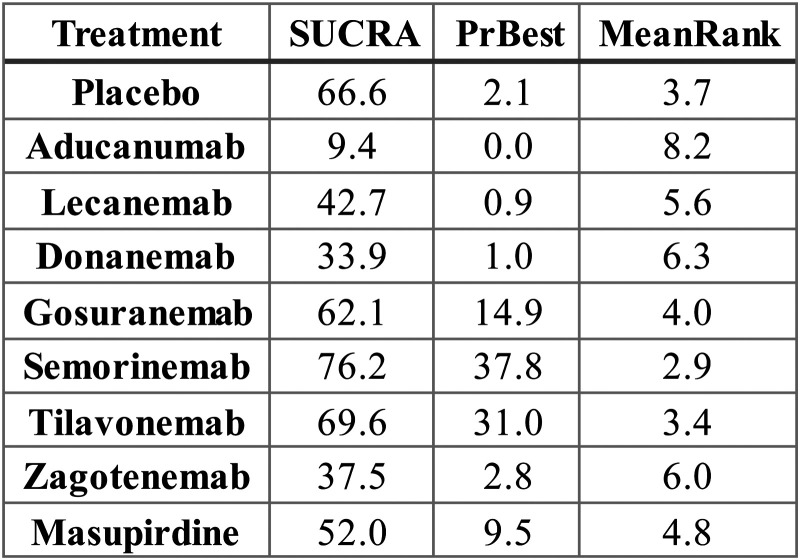 Figure 3
Figure 3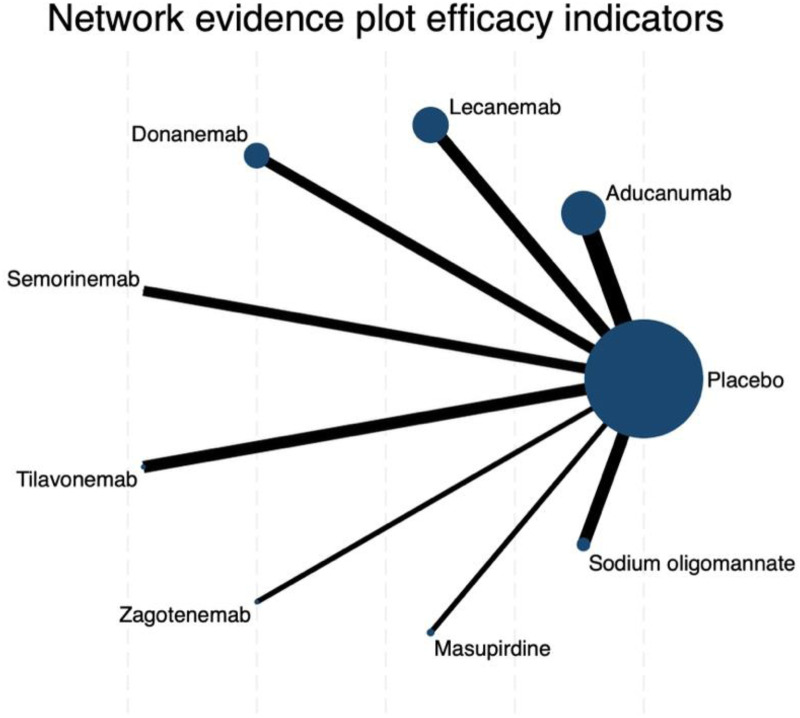 Figure 4
Figure 4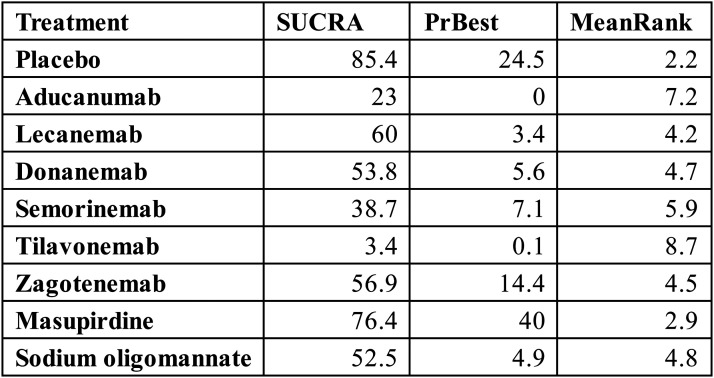 Figure 5
Figure 5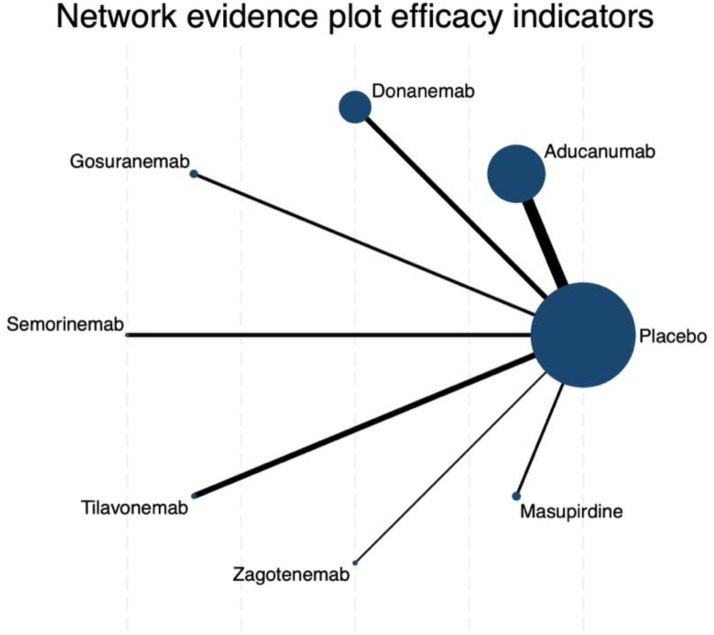 Figure 6
Figure 6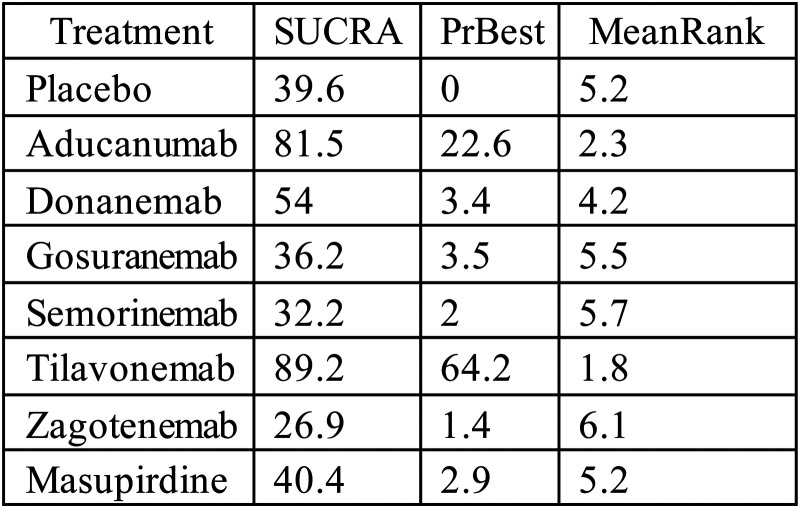 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Alzheimer's disease research and treatments · Cholinesterase and Neurodegenerative Diseases
Introduction
Alzheimer's disease (AD) is the most common cause of dementia and represents a major global health burden in aging populations. Despite decades of research, effective pharmacological options remain scarce. Current investigational approaches target mechanisms such as tau protein hyperphosphorylation, whereas approved therapies primarily modulate neurotransmission or promote amyloid clearance. Despite these advances, their overall clinical benefits remain modest.^1??????????????????????????????–32^ In recent years, novel biological agents such as aducanumab,^ 2 ^ lecanemab,^ 3 ^ and donanemab^ 1 ^ have been investigated in late-phase clinical trials. While lecanemab and donanemab have demonstrated relatively consistent efficacy profiles and received regulatory approvals in several regions,^1,3^ aducanumab has generated considerable controversy due to conflicting trial outcomes and regulatory decisions.^ 2 ^?
Table 1.: Characteristics of included studies.
Traditional pairwise meta-analyses are limited to direct, head-to-head comparisons and cannot assess the comparative efficacy of multiple competing interventions simultaneously. In contrast, network meta-analysis (NMA) integrates both direct and indirect evidence, enabling a comprehensive comparison and probabilistic treatment ranking of different treatments within a single analytical framework.^4,5^
The present study applies a NMA to assess the comparative efficacy and safety of nine active pharmacological treatments—aducanumab, lecanemab, donanemab, gosuranemab, semorinemab, tilavonemab, zagotenemab, masupirdine, and sodium oligomannate—against placebo in patients with AD. Specifically, we focus on cognitive outcomes measured by the Clinical Dementia Rating–Sum of Boxes (CDR-SB), Alzheimer's Disease Assessment Scale–Cognitive Subscale (ADAS-cog), and the Mini-Mental State Examination (MMSE) with the aim of providing an integrated ranking of interventions and clarifying their relative therapeutic potential.^6?–8^
Methods
Literature search strategy
A systematic literature search was conducted using the MEDLINE (via PubMed) database, covering studies from database inception to May 2025. We used a combination of Medical Subject Headings (MeSH) and free-text keywords, including “Alzheimer's disease”, “randomized controlled trial”, “CDR-SB”, “ADAS-cog”, “MMSE”, and “network meta-analysis”. Additional records were identified by manually screening the reference lists of relevant reviews and included articles. No restrictions were placed on language or publication status. The full, replicable search strategy for PubMed is provided in the Supplemental Material.
Inclusion and exclusion criteria
Population
We included studies enrolling adults diagnosed with AD based on established clinical criteria (e.g., NIA-AA, DSM, or similar), with no restrictions on disease severity or duration.
Intervention
We included studies evaluating novel, mechanism-based pharmacological therapies for AD that have advanced to late-stage (Phase 2 or 3) randomized controlled trials (RCTs) as of May 2025. We focused on agents beyond traditional symptomatic treatments (e.g., cholinesterase inhibitors). This rationale led to the inclusion of nine specific agents representing the primary emerging therapeutic classes: Anti-amyloid (Aβ) monoclonal antibodies (aducanumab, lecanemab, donanemab); Anti-tau monoclonal antibodies (gosuranemab, semorinemab, tilavonemab, zagotenemab); Other novel mechanisms (masupirdine [a 5-HT6 antagonist] and sodium oligomannate [a gut-brain axis modulator]). Although mechanistically diverse, these interventions are considered “exchangeable” for this NMA because they (a) target the same broad patient population (mild-to-moderate AD), (b) are frequently tested against a common placebo comparator, and (c) are assessed using the same standardized cognitive outcomes (CDR-SB, ADAS-cog, MMSE), making them clinically relevant competitors in the current therapeutic development landscape.
Comparator
Comparisons with placebo or head-to-head evaluations between two or more of the eligible interventions were included.
Outcomes
To be eligible, studies were required to report at least one of the following cognitive measures: CDR-SB, ADAS-cog, or MMSE. Outcome data needed to be extractable in the form of mean, standard deviation (SD), and sample size for each treatment arm.
Study design
Only randomized controlled trials (RCTs) were eligible, including parallel, crossover, or factorial designs.
Exclusion criteria
Studies were excluded if they were non-randomized, investigated combination therapies without isolating the effects of individual agents, lacked key outcome data (including where data could not be obtained from authors), were duplicate publications, conference abstracts, or had critical methodological flaws such as undefined interventions or comparators.
Outcome indicators
This network meta-analysis focused on three standardized cognitive outcomes commonly assessed in AD clinical trials. These were: (1) CDR-SB, evaluating cognitive and functional performance in daily life; (2) ADAS-cog, assessing memory, language, and praxis functions; (3) MMSE, reflecting global cognitive status.
Only change from baseline outcome scores were considered. When multiple time points were reported, data from the final follow-up or from the prespecified primary endpoint were extracted.
Data extraction and quality assessment
Two reviewers independently screened titles and abstracts assessed full texts for eligibility and extracted data using a predefined extraction form. Extracted information included study characteristics (author, publication year, design), details of intervention and control groups, sample size, treatment duration, and change from baseline outcome scores (mean, standard deviation, and sample size). Discrepancies were resolved through discussion or third-party adjudication. When outcome data were missing or unclear, study authors were contacted for clarification.
The methodological quality of included studies was evaluated using the Cochrane Risk of Bias tool (RoB 2.0). Each study was assessed across seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other potential biases. Each domain was rated as low, high, or unclear risk of bias.
Statistical analysis
All statistical analyses were performed using Stata version 17.0 with the net meta package. A network plot was first constructed to visually represent the geometry of the evidence, illustrating how different interventions were compared across studies. Fixed- or random-effects models were applied depending on the degree of heterogeneity, quantified using the I^2^ statistic; values >50% were considered indicative of substantial heterogeneity, prompting the use of a random-effects model.
Consistency within the network was assessed by conducting node-splitting analyses, allowing for the comparison of direct and indirect evidence on specific treatment comparisons. If significant inconsistencies were detected (e.g., p < 0.1 from the node-splitting test), we planned to explore potential sources of heterogeneity by examining key trial-level characteristics, such as differences in baseline population severity or study duration. To rank the relative efficacy of the interventions, we calculated the Surface Under the Cumulative Ranking (SUCRA) values, with higher SUCRA scores indicating a greater likelihood of being the most effective treatment. Additionally, the probability of each treatment being ranked best (PrBest) was estimated from the ranking model. Sensitivity analyses were performed by excluding studies deemed at high risk of bias, thereby testing the stability of the primary findings. Finally, publication bias was evaluated through visual inspection of funnel plots, supplemented by Egger's regression test to statistically assess asymmetry.
Results
Identification of relevant studies
A total of 392 articles were initially collected according to the searching strategy on PubMed. After adding 4 additional studies from PubMed, 396 studies remained. Following title and abstract screening, 374 articles were excluded for clearly not meeting the inclusion criteria. A total of 22 were retained for full-text review. After detailed assessment, 7 articles were excluded for the following reasons: duplicate publication (n = 1), not randomized controlled trial (n = 3), not AD population (n = 1), absence of CDR-SB, ADAS-cog, or MMSE outcomes (n = 1), and full text not available (n = 1) (Figure 1).
PRISMA flow diagram of the study selection process. A total of 392 records were identified from PubMed, with 4 additional studies added. After exclusions, 22 full-text articles were assessed for eligibility. Seven articles were excluded for reasons including duplicate records, not randomized controlled trials, non-AD population, lack of relevant cognitive outcomes (CDR-SB, ADAS-cog, MMSE), or unavailable full text. Finally, 15 studies were included in the analysis.
Ultimately, 15 articles met the eligibility criteria and were included in the final network meta-analysis (Table 1). The literature screening process and results are presented in the Supplemental Material (Excel file).
Risk of bias assessment and certainty of evidence
Risk of bias assessment showed that overall methodological quality was variable across the included studies. Specifically, two trials were judged to be at high risk of bias due to selective outcome reporting (domain D5). In addition, 7 studies were rated as having some concerns**,** while 5 studies were judged to be at low risk of bias across all assessed domains**.**
Regarding the certainty of evidence, treatment comparisons involving well-connected interventions such as aducanumab and lecanemab were supported by trials with low to moderate risk of bias. In contrast, comparisons involving zagotenemab and masupirdine were based on a small number of studies with methodological limitations. Overall, the quality of evidence was judged to be moderate for most primary outcomes, but lower for the MMSE-based secondary outcome.
Additional results, including SUCRA rankings, ranking probability distributions, and pairwise comparisons, are provided in the Supplemental Material (Supplemental Figures 1–6, Supplemental Tables 1–9).
Network meta-analysis primary outcomes
CDR-SB score
The network meta-analysis of changes in CDR-SB revealed a well-connected evidence network, with placebo serving as the central node directly compared to all investigated interventions (Figure 2). The connections linking aducanumab and lecanemab to placebo were notably thicker, reflecting a greater number of direct comparisons and thus lending relatively more stability to their estimates. In contrast, the edges corresponding to zagotenemab and masupirdine were markedly thinner.
Network evidence plot of efficacy indicators for CDR-SB outcomes. Each node represents a treatment, with the node size proportional to the number of patients randomized to that treatment. The thickness of the connecting lines reflects the number of trials directly comparing the two connected treatments. Placebo is the most connected node, serving as the reference comparator for all other drugs.
Based on SUCRA values, semorinemab ranked highest among all treatments for improving CDR-SB scores, with a SUCRA of 76.2, followed by tilavonemab (69.6), placebo (66.6), and gosuranemab (62.1) (Figure 3). It is noteworthy that placebo itself was positioned surprisingly high in the hierarchy, ranking third. Masupirdine (52.0), lecanemab (42.7), and donanemab (33.9) occupied intermediate positions, whereas zagotenemab (37.5) and aducanumab (9.4) were ranked lowest. Indeed, aducanumab demonstrated a virtually negligible probability of being the most effective treatment (PrBest = 0.0%) and was most frequently assigned to the eighth or ninth position across ranking iterations. In contrast, semorinemab and tilavonemab emerged as the most promising candidates, with probabilities of being ranked best of 37.8% and 31.0%, respectively. The cumulative rank probability distributions further underscored this pattern, showing that these two agents, along with placebo, were consistently concentrated in the top three ranks, while aducanumab's distribution clustered at the bottom (Supplemental Figure 1, Supplemental Table 1).
SUCRA values, probability of being best treatment (PrBest), and mean rank of each intervention for CDR-SB outcomes. Higher SUCRA values and lower mean rank indicate more favorable performance.
Despite the favorable ranking probabilities observed for semorinemab and tilavonemab, traditional pairwise meta-analyses painted a more cautious picture (Supplemental Table 2). The forest plots comparing mean differences in CDR-SB scores versus placebo indicated that, for nearly all treatments, the 95% confidence intervals crossed zero. Consequently, while the network rankings point toward a potential relative advantage for semorinemab and tilavonemab, the overall uncertainty remains considerable when viewed through the lens of traditional meta-analytic contrasts.
Sensitivity analyses and assessments of the model's underlying assumptions lent additional context to these findings. The funnel plot of effect sizes displayed a slight leftward asymmetry but remained broadly symmetrical, with Egger's regression tests yielding p-values of 0.054 (A versus C) and 0.066 (A versus B) (Supplemental Table 3), neither of which met conventional thresholds for statistical significance. These results do not provide strong evidence for the presence of publication bias, though the mild asymmetry warrants cautious interpretation (Supplemental Figure 2). Furthermore, node-splitting analyses for consistency revealed non-significant p-values, supporting the assumption of coherence between direct and indirect evidence within the network.
Taken together, these results show that among the pharmacologic agents evaluated, semorinemab and tilavonemab may hold relative promise for attenuating cognitive decline as measured by CDR-SB. Nevertheless, the lack of statistically significant differences in direct pairwise comparisons and the elevated placement of placebo within the ranking schema highlight the persistent uncertainty surrounding these interventions. Further large-scale, rigorously conducted randomized trials will be essential to more definitively ascertain their comparative efficacy.
ADAS-Cog score
The network meta-analysis for changes in ADAS-cog scores revealed a star-shaped structure highly similar to that observed in the CDR-SB analysis. Placebo functioned as the central comparator node, directly connected to all nine active interventions, with particularly thick links to aducanumab, lecanemab, semorinemab, sodium oligomannate, and tilavonemab. This reflects the relatively larger evidence base for these treatments in placebo-controlled trials (Figure 4).
Network evidence plot of efficacy indicators for ADAS-cog outcomes. Node size represents the sample size per treatment and line thickness indicates the number of direct comparisons.
In terms of treatment ranking, placebo unexpectedly achieved the highest SUCRA value (85.4%), with a probability of being the best treatment (PrBest) of 24.5% and a mean rank of 2.2. Among active agents, masupirdine emerged as the most favorable intervention (SUCRA: 76.4%; PrBest: 40.0%; mean rank: 2.9), followed by lecanemab (SUCRA: 60.0%; PrBest: 3.4%) and zagotenemab (SUCRA: 56.9%; PrBest: 14.4%). By contrast, tilavonemab consistently ranked lowest (SUCRA: 3.4%), with an 82.1% probability of being the worst treatment, while aducanumab also demonstrated poor performance (SUCRA: 25.0%; PrBest: 0%; mean rank: 7.0). These findings highlight a striking divergence in relative efficacy probabilities, favoring placebo and masupirdine while reinforcing the unfavorable standing of tilavonemab and aducanumab (Figure 5).
Surface under the cumulative ranking curve (SUCRA), probability of being the best treatment (PrBest), and mean rank of each intervention for ADAS-cog outcomes.
The rank probability plots further substantiated these patterns. Placebo showed the highest overall likelihood of occupying top positions (rank 1–3), whereas tilavonemab had a dominant probability of being ranked last (Supplemental Figure 3). Masupirdine displayed the greatest probability of achieving rank 1 (40.0%), albeit with wide distribution across intermediate ranks (Supplemental Table 4).
Pairwise comparisons largely confirmed these observations. Most active interventions versus placebo yielded wide confidence intervals crossing zero, indicating a lack of statistically significant superiority. Notably, however, placebo demonstrated statistically significant advantages over certain active drugs. For instance, placebo was superior to tilavonemab (mean difference: 7.40; 95% CI: 2.66 to 12.14) and aducanumab (mean difference: 3.51; 95% CI: 1.63 to 5.39). These results account for the unusually high ranking of placebo in SUCRA analysis and underscore the limited efficacy of several monoclonal antibodies within this outcome domain (Supplemental Table 5).
Assessment of small-study effects revealed potential concerns. Funnel plots exhibited mild asymmetry, and Egger's tests detected significant publication bias for one comparison (A versus B, p = 0.0081), though other contrasts were not statistically significant (Supplemental Figure 4).
Furthermore, inconsistency analyses identified discrepancies between direct and indirect evidence, suggesting that the network's transitivity assumption may not be fully satisfied. These limitations indicate that the probabilistic rankings should be interpreted with caution (Supplemental Table 6).
In conclusion, the ADAS-cog analysis did not demonstrate robust superiority of any pharmacological intervention over placebo. Instead, placebo and masupirdine achieved the most favorable rankings, whereas tilavonemab and aducanumab consistently performed worst. These findings contrast with earlier results for other scales, highlighting both the heterogeneity of cognitive outcome measures and the substantial challenges in achieving reliable efficacy signals across AD clinical trials.
Secondary outcome
For the secondary outcome assessing changes in MMSE scores, the network geometry retained a star-shaped structure, with placebo serving as the central comparator directly connected to all active interventions. The thickest connections were observed between placebo and aducanumab as well as tilavonemab (Figure 6).
Network evidence plot of efficacy indicators for MMSE outcomes. Node size reflects the number of patients randomized to each treatment, while edge thickness represents the number of trials directly comparing connected interventions.
Based on SUCRA values and ranking probabilities, the treatment hierarchy differed significantly from the primary outcomes. The most highly rated intervention was tilavonemab (SUCRA: 89.2%; PrBest: 64.2%; mean rank: 1.8), which was closely followed by aducanumab (SUCRA: 81.5%; PrBest: 22.6%; mean rank: 2.3). Donanemab's performance was intermediate (mean rank: 4.2; SUCRA: 54.0%) (Figure 7). On the other hand, all active medications, such as zagotenemab, gosuranemab, semorinemab, and masupirdine, as well as a placebo, were consistently found in the lower ranks. The rank-probability plots, which displayed the probability distribution for aducanumab peaking at rank two and for tilavonemab peaking at rank one, further corroborated these trends (Supplemental Figure 5, Supplemental Table 7).
Surface under the cumulative ranking curve (SUCRA), probability of being the best treatment (PrBest), and mean rank of each intervention for MMSE outcomes.
The pairwise comparisons (Supplemental Table 8) revealed a more complex and subtle perspective. The only active treatment that demonstrated a statistically significant advantage over a placebo was aducanumab (mean difference −1.99, 95% CI – 3.68 to −0.3). The fact that tilavonemab failed to produce a statistically significant outcome even though it was the drug with the highest SUCRA ranking was particularly significant. Actually, compared to a placebo, its negative mean difference (mean difference −3.20, 95% CI −6.88 to 0.48) indicated a trend of worse performance. The confidence intervals for all other active interventions crossed zero, indicating no meaningful differences from placebo.
The model diagnostics, on the other hand, showed serious problems that make these efficacy findings very questionable. The funnel plot for the MMSE analysis exhibited significant asymmetry (Supplemental Figure 6), indicating that smaller studies generally reported larger effect sizes. Egger's test confirmed this finding by showing a statistically significant intercept (p = 0.016), which strongly suggested either publication bias or small-study effects (Supplemental Table 9). This discovery significantly affects the trustworthiness of the entire MMSE analysis and raises considerable doubt regarding the purported efficacy of aducanumab.
In summary, although an initial examination of the MMSE analysis indicated that tilavonemab and aducanumab were the most promising agents, with aducanumab displaying a relatively significant advantage, these conclusions lack credibility. The robust statistical evidence of publication bias strongly indicates that the observed positive effects, particularly for aducanumab, are likely a statistical artefact. Consequently, these findings must be regarded with extreme caution.
Publication bias
Publication bias assessment revealed heterogeneous findings across different cognitive outcomes. For the primary outcome (CDR-SB) and the secondary outcome (ADAS-cog), funnel plots appeared largely symmetrical, and Egger's test did not identify statistically significant small-study effects (p > 0.05). These results suggest that the risk of publication bias for these measures is minimal, lending greater confidence to the pooled estimates.
In contrast, the MMSE outcome exhibited clear evidence of bias. The funnel plot showed marked asymmetry, with smaller studies disproportionately reporting larger treatment effects. This was corroborated by Egger's test (p = 0.0159), indicating significant small-study effects or selective reporting. Importantly, aducanumab—the only drug showing nominal statistical superiority over placebo on MMSE—may have had its apparent benefit exaggerated due to this bias. Moreover, MMSE is inherently less sensitive to subtle cognitive changes in early-stage AD and is prone to ceiling effects, further limiting the robustness of these findings.
Taken together, while the CDR-SB and ADAS-cog results appear methodologically reliable, the MMSE findings should be interpreted with caution. These observations underscore the need for more rigorous trial reporting, prospective registration, and larger-scale studies to mitigate selective publication and improve the reliability of cognitive outcome assessments in AD research.
Discussion
In this network meta-analysis comparing nine pharmacological treatments for AD with placebo, no active drug demonstrated a robust or statistically significant cognitive benefit over placebo on the primary outcomes (CDR-SB and ADAS-cog). While two experimental therapies, semorinemab and tilavonemab (both targeting tau protein pathology), ranked highest in terms of probability of being the best treatment, their advantages were modest and not statistically significant in direct comparisons. The placebo showed unexpectedly strong performance, ranking near the top across multiple outcomes and even achieving the highest SUCRA value on ADAS-cog, exceeding all active treatments. This finding underscores the modest and uncertain efficacy signals of current agents. In contrast, aducanumab produced inconsistent results. It ranked lowest on CDR-SB and ADAS-cog but appeared near the top on MMSE, where it was the only drug demonstrating nominal statistical superiority over placebo. However, this apparent advantage is undermined by evidence of publication bias (Egger's test p = 0.0159), casting doubt on the reliability of MMSE-derived findings. Taken together, these results highlight the limited and inconsistent cognitive benefits of available therapies, the pronounced role of placebo responses in AD trials, and the methodological vulnerabilities of different cognitive assessment tools.
Several explanations may account for these findings. First, most active drugs do not outperform placebo in statistically significant ways, largely due to small or non-significant effect sizes. Their confidence intervals frequently crossed zero, thereby weakening their ranking. Second, certain interventions were evaluated in only a limited number of trials, often with large standard errors and heterogeneous results, further reducing confidence in their estimated benefits. Third, placebo performance remained consistent despite the absence of active pharmacological effects. In a probabilistic ranking model, such consistency of performance may result in a higher rank when other treatments perform poorly or inconsistently.
An additional methodological limitation across several included trials relates to the use and reporting of placebo comparators. Future AD trials may benefit from comparing investigational agents against optimized standard-of-care therapy rather than placebo alone, in line with best practices in clinical trial design, to improve interpretability and clinical relevance of efficacy estimates.
Meanwhile, the relative success of tau-targeting antibodies (semorinemab and tilavonemab) is highly supported by the accumulating evidence that AD tau pathology correlates more closely with cognitive decline than amyloid burden.^ 19 ^ Nonetheless, the small, non-significant effect sizes observed here suggest that current tau antibodies may not yet achieve sufficient target engagement or brain penetration to translate into robust clinical benefits.^ 20 ^
More critically, our analysis detected a statistically significant Egger's test result for the MMSE outcome (p = 0.0159), providing strong evidence of publication bias or small-study effects. This elevates the concern from a methodological limitation to a direct challenge to the validity of the observed aducanumab result. The observed “benefit” is likely a statistical artifact, not a true clinical effect, amplified by selective reporting or an overrepresentation of smaller, positive studies. This conclusion aligns with the broader scientific and regulatory controversy surrounding the drug. The European Medicines Agency (EMA) initially refused marketing authorization for aducanumab, citing conflicting trial results and an unproven link between its biomarker effect (amyloid reduction) and meaningful clinical improvement.^ 2 ^ More recently, the EMA has approved other anti-amyloid monoclonal antibodies, including lecanemab and donanemab, following additional evidence of modest clinical benefit. Importantly, however, this regulatory change does not resolve the specific concerns surrounding aducanumab. In our analysis, the apparent MMSE benefit of aducanumab coincides with clear evidence of publication bias and the known limitations of MMSE as a cognitive outcome measure. Taken together, the convergence of a flawed instrument, evidence of statistical bias from our analysis, and a negative regulatory review builds an overwhelming case to interpret aducanumab's apparent MMSE benefit with extreme uncertainty.
Methodologically, this study highlights the value of NMA for comparing multiple interventions when head-to-head trials are scarce. By integrating direct and indirect evidence, NMA enables comprehensive treatment ranking, though several limitations remain. NMA findings are typically presented using statistical metrics like SUCRA, indicating the likelihood of each treatment being the most favorable option.^ 21 ^ It is important to note that an SUCRA number nearing 100% indicates a higher likelihood of the therapy ranking highly in efficacy, but it does not necessarily correlate with more significant clinical benefits or more robust evidence.^ 22 ^ A high ranking does not indicate a definitive superiority in effectiveness nor suggest an especially high level of confidence.^ 23 ^ Therefore, when treatment effects are just slightly distinct or the quality of evidence is insufficient, relying only on SUCRA rankings for decision-making may be misleading.^ 24 ^ Such assessments should be augmented by a thorough examination that includes real effect magnitude and variability.
First, the evidence network was uneven. Certain treatment nodes, such as zagotenemab and masupirdine, were supported by only a small number of trials, reducing the precision and reliability of their estimated effects. Second, the MMSE outcome appeared particularly vulnerable to bias. Funnel plot asymmetry and a statistically significant Egger's test (p = 0.0159) indicated the presence of publication bias or small-study effects. This strongly undermines confidence in the apparent benefit of aducanumab, which was largely driven by MMSE findings. Third, consistency tests indicated significant inconsistency between the aducanumab and semorinemab comparison groups, cautioning against overinterpretation of MMSE results. Additionally, heterogeneity in cognitive outcomes and inconsistencies in trial duration across studies may introduce unmeasured variability.
Beyond the statistical limitations of the NMA, the interpretation of efficacy in the included trials requires caution due to fundamental design shortcomings highlighted in recent critical reviews. The treatment of adverse events may induce enrichment bias. Patients with low antibody tolerance, generally due to amyloid-related imaging abnormalities (ARIA), may be excluded from efficacy assessments or discontinue treatment early. This favors a ‘super-responder’ population that tolerates the treatment, perhaps increasing efficacy relative to the general AD population.^ 25 ^ Additionally, most trials did not strictly control for changes in conventional background therapy, making it difficult to isolate the true pharmacological effect of the investigational agents from variations in standard care.^ 25 ^
Taken together, these limitations highlight the need for cautious interpretation of treatment rankings and underscore the importance of larger designed trials with standardized cognitive endpoints.
Consistent with previous meta-analyses, our results show that the active interventions investigated did not show statistically significant benefits over placebo on the primary outcomes (CDR-SB and ADAS-cog), highlighting the limited effectiveness of existing pharmacotherapies for AD. The relatively high rankings of the tau-targeting antibodies semorinemab and tilavonemab in our analysis align with reports suggesting that showing both agents offer comparable or superior cognitive improvement to placebo with favorable safety profiles. The incidence of adverse events (AEs), serious adverse events (SAEs), falls, and urinary tract infections was lower in the tilavonemab group than in the placebo group, and the differences were statistically significant.^ 4 ^ The favorable ranking of semorinemab in our network meta-analysis may reflect its target engagement and downstream pharmacodynamic effects, as supported by recent biomarker studies. In particular, Schauer et al.^ 26 ^ demonstrated that semorinemab reduced cerebrospinal fluid levels of tau-related pathology markers, including phosphorylated tau and neurogranin, which may underlie its potential to slow cognitive decline in AD. These findings suggest that the high SUCRA rankings of semorinemab and tilavonemab in our analysis may reflect modest but genuine clinical effects of tau-targeted approaches.
Interestingly, our secondary analysis of MMSE revealed a markedly improved ranking for aducanumab, in contrast to its poor performance on CDR-SB and ADAS-cog. Mechanistically, aducanumab has been shown to distinguish monomers from oligomers or fibrillar aggregates based on its weak monovalent affinity, rapid binding kinetics, and strong affinity for epitope-rich aggregates.^27,28^ Despite this pharmacological rationale, regulatory evaluations have raised substantial concerns. The U.S. Food and Drug Administration (FDA) has reported significantly higher incidences of ARIA-edema and ARIA-hemorrhage, collectively referred to as ARIA, in patients treated with aducanumab.^ 25 ^ Beyond these acute events, emerging evidence suggests a paradoxical ‘therapeutic’ consequence: accelerated brain volume loss.^ 29 ^ Long-term assessment of patients treated with anti-amyloid immunotherapies has revealed significant whole-brain atrophy and ventricular enlargement compared to placebo.^ 30 ^ These structural changes raise critical questions about whether the clearance of amyloid plaques comes at the cost of neuronal integrity.^31,32^ At the time of earlier regulatory assessments, the European Medicines Agency (EMA) has stated that aducanumab has not yet demonstrated clear clinical efficacy or an acceptable safety profiles patients with early-stage AD.^ 33 ^ Since then, the EMA has approved other anti-amyloid monoclonal antibodies, including lecanemab and donanemab, following the availability of additional trail data indicating modest clinical benefit. Biogen's ENVISION study, a validation study assessing the safety and efficacy of long-term treatment after discontinuation, is expected to be completed by 2026.^ 33 ^ In this study, due to the relatively small number of studies included in our MMSE analysis, funnel plot asymmetry and a significant Egger's test suggest the possibility of small-study or publication bias. Egger regression is commonly used to assess funnel plot asymmetry, but its accuracy decreases when fewer than 10 trials are available. Thus, the favorable ranking of aducanumab on MMSE should be interpreted with caution, and more robust, adequately powered randomized trials are needed to clarify its true effect.
Although this may seem counterintuitive, high placebo scores in our analysis are not unprecedented in AD trials. Recent meta-analyses of trials targeting AD and mild cognitive impairment have confirmed strong placebo responses, which are typically attributed to expectation effects,^ 34 ^ researcher-participant interaction, regression to the mean effects, and repeated cognitive testing.^ 35 ^ These findings suggest that the unexpected placebo effects observed in this study likely reflect inherent factors inherent to the trial itself rather than genuine therapeutic benefits.
This study, along with most of the included trials, used PET imaging markers (such as changes in cerebral amyloid or tau burden) as a surrogate endpoint. However, a decrease in the imaging signal of pathological burden does not indicate a complete absence of the disease pathology, and a definitive causal relationship between imaging enhancement and clinical benefit for patients remains unestablished. Prior research has demonstrated that a simple decrease in cerebral amyloid beta burden is insufficient to significantly prevent cognitive decline over follow-up periods.^ 36 ^ Furthermore, the reliance on structural MRI and amyloid-PET as primary biomarkers fails to capture the functional metabolic state of the brain following treatment.^ 37 ^ There is a notable scarcity of data utilizing fluorodeoxyglucose-positron emission tomography (FDG-PET) to assess regional metabolic activity in areas affected by ARIA or atrophy.^ 29 ^ Currently, no interventions targeting amyloid beta have shown significant improvements in clinical efficacy.^38,39^ This indicates that efficacy evidence derived mainly from PET surrogate endpoints requires careful analysis.
Despite encouraging changes in biomarkers, several tau-targeting monoclonal antibodies, including semorinemab, have failed to demonstrate significant clinical benefits in late-stage clinical trials. The limited efficacy of tau-targeting antibodies, such as semorinemab and tilavonemab, likely stems from fundamental mechanistic barriers.^40,41^ Pathological tau tangles are primarily located intracellularly, posing a significant challenge for conventional monoclonal antibodies. Due to their substantial molecular size, these antibodies cannot readily penetrate the neuronal cell membrane to access and clear intraneuronal aggregates.^ 42 ^ Current approaches largely rely on the hypothesis of intercepting extracellular ‘seed’ tau (the “interceptor” Hypothesis) to prevent cell-to-cell propagation.^ 43 ^ However, as our results indicate, targeting this extracellular fraction alone may be insufficient to halt clinical decline once intracellular pathology is established. This highlights a critical limitation in the current design of passive immunotherapies: without effective intracellular delivery mechanisms, antibodies may fail to engage the most relevant pathological targets. Additionally, recent quantitative systems pharmacology modelling suggests that semorinemab has relatively low target binding rates in cerebrospinal fluid, which may be related to its lower affinity and shorter half-life in extended dosing regimens.^ 44 ^ To be more specific, antibodies targeting the N-terminal region of tau protein may successfully bind to soluble tau protein in cerebrospinal fluid but fail to affect pathological tau protein or intracellular aggregates in the brain.^ 44 ^ Future studies should consider alternative tau antigen epitopes, improve antibody pharmacokinetic properties, or adopt delivery strategies that enhance brain penetration.
Meanwhile, current animal and in vitro models may not adequately predict the functional efficacy of antibodies targeting tau protein. Induced pluripotent stem cell (iPSC)-derived neurons and brain organoids offer promising human-relevant platforms for preclinical evaluation.^ 45 ^ These models can be used to test antigen-specific binding, cellular uptake, and downstream tau protein clearance efficiency under conditions similar to those in humans.^ 46 ^ Future research should combine human neuronal models derived from iPSCs with pharmacokinetic analysis to design more effective tau immunotherapies that can penetrate the blood-brain barrier.^ 47 ^
Conclusion
This network meta-analysis of nine AD drugs found that none provided a clinically meaningful cognitive benefit over a placebo.
Tau-targeting antibodies showed only marginal, statistically insignificant potential. The apparent benefit of another drug, aducanumab, was found to be highly unreliable due to strong evidence of publication bias and limitations of the cognitive test used.
Overall, these findings underscore the limitations of the current AD therapeutic landscape and highlight the significant influence of the placebo response in clinical trials. Future research should include larger, high-quality randomized controlled trials to validate these comparative efficacy trends and detect any meaningful treatment effects. Additionally, greater use of advanced human neuronal models, such as induced pluripotent stem cell (iPSC)-derived neurons and brain organoids, is recommended to better elucidate the mechanistic efficacy of tau-targeting therapies. Such approaches will help inform the development of more effective treatments for AD and ensure that promising therapeutic strategies are rigorously evaluated before clinical adoption.
Supplemental Material
sj-docx-2-alr-10.1177_25424823261422205 - Supplemental material for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's diseaseSupplemental material, sj-docx-2-alr-10.1177_25424823261422205 for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's disease by Shanshan Huang and Yunyun Guo in Journal of Alzheimer's Disease Reports
sj-xlsx-3-alr-10.1177_25424823261422205 - Supplemental material for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's diseaseSupplemental material, sj-xlsx-3-alr-10.1177_25424823261422205 for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's disease by Shanshan Huang and Yunyun Guo in Journal of Alzheimer's Disease Reports
sj-xlsx-4-alr-10.1177_25424823261422205 - Supplemental material for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's diseaseSupplemental material, sj-xlsx-4-alr-10.1177_25424823261422205 for Network meta-analysis of the efficacy of nine drugs for cognitive function in patients with Alzheimer's disease by Shanshan Huang and Yunyun Guo in Journal of Alzheimer's Disease Reports
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mintun MA Lo AC Duggan Evans C , et al. Donanemab in early Alzheimer’s disease. N Engl J Med 2021; 384: 1691–1704.33720637 10.1056/NEJ Moa 2100708 · doi ↗ · pubmed ↗
- 2Budd Haeberlein S Aisen PS Barkhof F , et al. Two randomized phase 3 studies of aducanumab in early Alzheimer’s disease. J Prev Alzheimers Dis 2022; 9: 197–210.35542991 10.14283/jpad.2022.30 · doi ↗ · pubmed ↗
- 3van Dyck CH Swanson CJ Aisen P , et al. Lecanemab in early Alzheimer’s disease. N Engl J Med 2023; 388: 9–21.36449413 10.1056/NEJ Moa 2212948 · doi ↗ · pubmed ↗
- 4Cai W Zhang H Wu Y , et al. Comparative the efficacy and safety of gosuranemab, semorinemab, tilavonemab, and zagotenemab in patients with Alzheimer’s disease: a systematic review and network meta-analysis of randomized controlled trials. Front Aging Neurosci 2025; 16: 1465871.39945003 10.3389/fnagi.2024.1465871 PMC 11814219 · doi ↗ · pubmed ↗
- 5Monteiro C Toth B Brunstein F , et al. Randomized phase II study of the safety and efficacy of semorinemab in participants with mild-to-moderate Alzheimer disease: lauriet. Neurology 2023; 101: e 1391–e 1401.10.1212/WNL.0000000000207663 PMC 1057314137643887 · doi ↗ · pubmed ↗
- 6Straten G Saur R Laske C , et al. Influence of lithium treatment on GDNF serum and CSF concentrations in patients with early Alzheimer’s disease. Curr Alzheimer Res 2011; 8: 853–859.21875410 10.2174/156720511798192754 · doi ↗ · pubmed ↗
- 7Ballard C Banister C Khan Z , et al. Evaluation of the safety, tolerability, and efficacy of pimavanserin versus placebo in patients with Alzheimer’s disease psychosis: a phase 2, randomised, placebo-controlled, double-blind study. Lancet Neurol 2018; 17: 213–222.29452684 10.1016/S 1474-4422(18)30039-5 · doi ↗ · pubmed ↗
- 8Chen C Katayama S Lee J-H , et al. Clarity AD: Asian regional analysis of a phase III trial of lecanemab in early Alzheimer’s disease. J Prev Alzheimers Dis 2025; 12: 100160.40189473 10.1016/j.tjpad.2025.100160 PMC 12184022 · doi ↗ · pubmed ↗