Clinical spectrum and management outcomes of acute febrile illness Among children attending health facilities in northwestern Tanzania, 2020–2021
Neema M. Kayange, Oliver Ombeva Malande, Stephan Gehring, Silvia Scialabba, Britta Groendahl, Philip Koliopoulos, Stephen E. Mshana

TL;DR
This study examines how children with fevers are diagnosed and treated in Tanzania, finding high rates of unnecessary antibiotic and antimalarial use.
Contribution
The study provides insights into clinical management and prescription patterns of acute febrile illness in low-resource settings.
Findings
Acute respiratory infections and malaria were the most common initial diagnoses among children with febrile illness.
Over 29% of children received unnecessary antibiotics, and nearly 40% received antimalarials without confirmed malaria.
Fever resolved in 96% of children by day 28, but complications like anemia and dehydration were common among hospitalized children.
Abstract
The diagnostic challenges of febrile illness in children in low-resource settings and the risks of empirical overtreatment. We evaluated the range of clinical presentations and management outcomes in a cohort of children with acute febrile illness, building on our previous examination of the etiology of these illnesses. This prospective cohort study enrolled children aged 1 to ≤12 years who were cared for by attending clinicians across primary, secondary, and tertiary healthcare settings. Management decisions were based on clinical presentation and laboratory and radiographic findings available on the day of enrollment. Outcomes were measured on days 7, 14, and 28. The study also analyzed prescription patterns for antibiotics and antimalarials in relation to established guidelines. In this cohort of 434 children with acute febrile illness, the most common initial diagnoses were acute…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
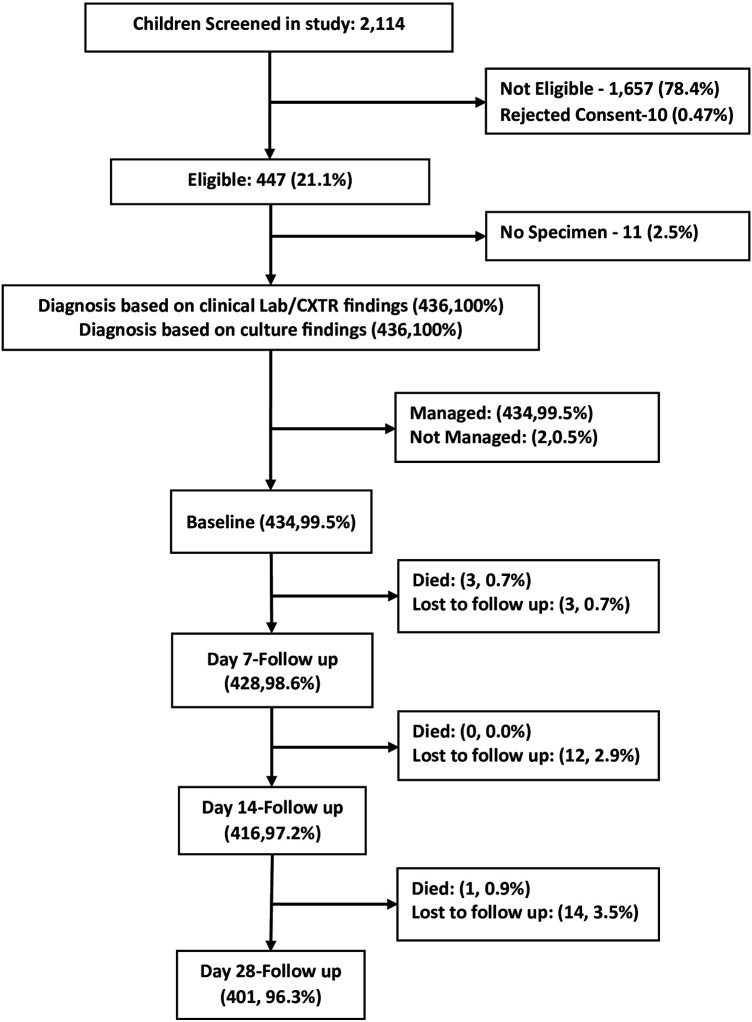 Figure 1
Figure 1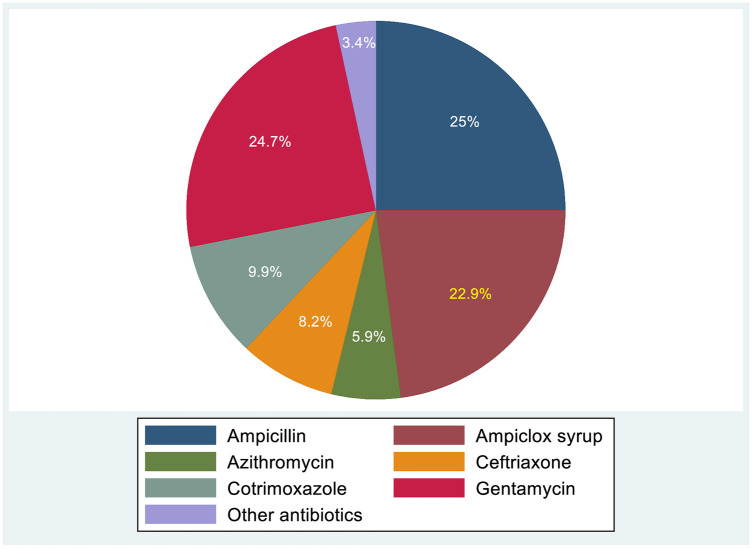 Figure 2
Figure 2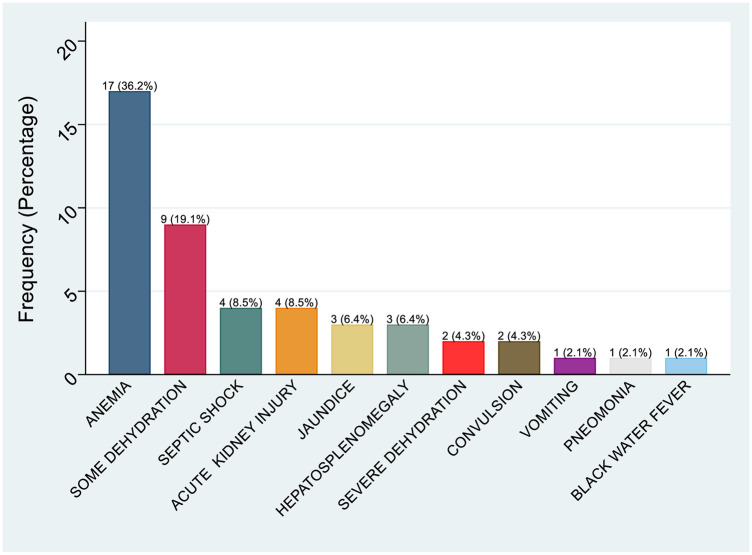 Figure 3
Figure 3| Condition | Definition |
|---|---|
| Fever | Core body temperature of ≥38 °C |
| Malaria | A positive result from any of the following: malaria rapid diagnostic test (RDT), slide microscopy, or genus-specific malaria PCR at baseline and follow up |
| Presumptive acute arboviral infection | Positive RDT [e.g., Dengue Non-structural protein 1 (NS1) antigen] |
| Confirmed arboviral infection | Positive PCR results for arboviruses such as Dengue, Chikungunya, Yellow Fever, Zika, West Nile, Rift Valley, or O’nyong-nyong, or positive anti-arbovirus Immunoglobulin M (IgM) ELISA. |
| Bloodstream infections (bacteremia/candidemia) | Positive blood culture with pathogenic bacteria or yeast |
| Urinary tract infections (UTI) | Urine culture showing significant bacteriuria (≥105 colony-forming units/mL). |
| Acute respiratory infection | Presentation with at least one respiratory sign or symptom lasting ±7 days and confined to the respiratory tract (upper or lower). |
| Pneumonia | History of cough and/or difficulty breathing, along with one or more of these signs: tachypnea, chest abnormalities, abnormal auscultation, or radiographic findings suggestive of pneumonia. |
| Sepsis | Systemic inflammatory response syndrome with suspected or confirmed infection, or signs of organ dysfunction. |
| Anemia | Hematocrit below age-specific cut-off (age: 2 months: <28%; 3–6 months: <29%; 7–24 months: <33%; 25 months-6 years: <34%; 7–12 years: <35%) |
| Meningitis | Clinical signs (e.g., stiff neck, meningeal signs) and/or cerebrospinal fluid abnormalities consistent with meningitis confirmed by clinicians |
| Acute gastroenteritis | Presentation with diarrhea, defined as ≥3 loose or liquid stools per day, lasting less than 7 days, reported at any time within the 7 days before enrollment. |
| Undifferentiated fever | No source of fever was identified following clinical assessment and all available laboratory tests. |
|
|
|
| Resolved Fever | No fever observed for 2 consecutive days before day 7 (± 1), day 14 (± 1), and day 28 (± 1), as reported by caregivers or with a measured temperature ranging from 36.4 °C to 37.5 °C. |
| Persistent Fever | Fever episode within the 2 days prior to day 7 (± 1), day 14 (± 1), 28 (±1) as reported by caregivers or confirmed by a measured temperature of ≥38 °C |
| Relapse | Fever was reported on day 14 (± 1) in a child who had previously experienced fever resolution around day 7 (± 1), possibly linked to the initial febrile illness. |
| Hospitalization | Hospital admission for treatment linked to the febrile illness presented. |
| Death | Mortality within 28 days (± 1 day) of follow-up, considered potentially related to the initial febrile illness, as evaluated by the attending clinicians. |
| Clinical diagnosed infections (chart record clinic & wards) | Health Facility | Total | ||||
|---|---|---|---|---|---|---|
| Bugando | Sekou Toure | Buzuruga | Nyamagana | Sengerema | ||
| 43 | 38 | 31 | 30 | 27 | 169 | |
| 11 | 7 | 15 | 16 | 9 | 58 | |
| 9 | 11 | 15 | 17 | 21 | 73 | |
| URTI | 14 | 12 | 10 | 1 | 21 | 77 |
| Unspecified LRTIs | 11 | 1 | 1 | 0 | 5 | 18 |
| 14 | 0 | 1 | 1 | 1 | 17 | |
| 4 | 2 | 0 | 4 | 3 | 13 | |
| 4 | 5 | 0 | 2 | 2 | 13 | |
| 0 | 0 | 0 | 2 | 0 | 2 | |
| 1 | 1 | 0 | 0 | 0 | 2 | |
| Undifferentiated fever | 5 | 1 | 3 | 2 | 7 | 18 |
| 14 | 18 | 21 | 22 | 23 | 98 | |
| Pneumonia | 10 | 18 | 10 | 8 | 13 | 59 |
| Clinical diagnosed infections (chart record clinic & wards) | Health facility | Total | ||||
|---|---|---|---|---|---|---|
| Bugando | Sekou Toure | Buzuruga | Nyamagana | Sengerema | ||
| 11 | 7 | 15 | 16 | 9 | 58 | |
| 11 | 1 | 1 | 0 | 5 | 18 | |
| 14 | 0 | 1 | 1 | 1 | 17 | |
| 4 | 2 | 0 | 4 | 3 | 13 | |
| 4 | 5 | 0 | 2 | 2 | 13 | |
| Otitis Media | 0 | 0 | 0 | 2 | 0 | 2 |
| 1 | 1 | 0 | 0 | 0 | 2 | |
| 5 | 1 | 3 | 2 | 7 | 18 | |
| 10 | 18 | 10 | 8 | 13 | 59 | |
| Total | 200 | |||||
| Clinical Diagnosed Infections (Chart record Clinic & Wards) | Health Facility | Total | ||||
|---|---|---|---|---|---|---|
| Bugando | Sekou Toure | Buzuruga | Nyamagana | Sengerema | ||
| Laboratory Diagnosed (by Study Tests) | ||||||
| 6 | 4 | 7 | 9 | 7 | 33 | |
| 7 | 13 | 11 | 9 | 7 | 47 | |
| 22 | 20 | 11 | 5 | 9 | 66 | |
| 7 | 5 | 8 | 11 | 5 | 36 | |
| 6 | 4 | 8 | 6 | 2 | 26 | |
| 12 | 3 | 3 | 6 | 10 | 34 | |
| 0 | 0 | 0 | 0 | 0 | 0 | |
| Pearson | ||||||
| Characteristics | Health Facility | Total | |||||
|---|---|---|---|---|---|---|---|
| Initial Management | Bugando ( | Sekou Toure ( | Buzuruga ( | Nyamagana ( | Sengerema ( | ||
| Managed as inpatients | 79 (85.9) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 79 | |
| Managed as outpatient | 13 (14.1) | 67 (95.7) | 73 (84.9) | 72 (84.7) | 97 (96.0) | 322 | 0.001 |
| Referred to higher-level care | 0 (0.0) | 3 (4.3) | 13 (15.1) | 13 (15.3) | 4 (4.0) | 33 | |
| Prescriptions and adherence with guidelines | |||||||
| Antibiotic Prescriptions | |||||||
| 86 (93.5) | 48 (68.6) | 51 (59.3) | 51 (60.0) | 48 (47.5) | 284 | 0.001 | |
| Prescribed antibiotic with empirical clinical indication | 59 (29.5) | 26 (44.7) | 39 (56.3) | 37 (53.5) | 39 (43.4) | 200 | 0.001 |
| 27 (52.0) | 22 (47.0) | 12 (47.2) | 14 (48.4) | 9 (47.2) | 84 | 0.001 | |
| Antimalarial Prescriptions | |||||||
| Prescribed antimalarials | 43 (46.7) | 38 (54.3) | 31 (36.1) | 30 (35.3) | 27 (26.7) | 169 | 0.102 |
| Prescribed antimalarials with clinical indication | 25 (24.3) | 23 (22.3) | 19 (18.4) | 19 (18.4) | 17 (16.5) | 103 | |
| 18 (28.8) | 15 (22.7) | 12 (18.2) | 11 (16.7) | 10 (13.6) | 66 | 0.055 | |
| Follow-up variable | Day 7, | Day 14, | Day 28, |
|---|---|---|---|
| Follow-up Status | |||
| Completed | |||
| Lost to follow up | 3 (0.3%) | 12 (3.0) | 14 (3.5) |
| Child status | |||
| Alive | |||
| Died | 3 (0.7) | 0 | 1 (0.3%) |
| Fever Status | |||
| Resolved | 398 (93%) | 400 (96%) | 386 (96%) |
| Persistent | 30 | 9 | 0 |
| Relapsed | 0 | 8 | 0 |
| Hospitalization | |||
| Hospitalized at first visit | 78 (18.0%) | 0 | 0 |
| Hospitalized on follow-up | 4 | 16 | 13 |
| Not hospitalized | 356 | 0 | 0 |
| Readmission | 0 | 2 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Hematological disorders and diagnostics · Antibiotic Use and Resistance
Introduction
1
Improvements in malaria diagnosis and management, such as the introduction of malaria rapid diagnostic tests and artemisinin combination therapy, have had a significant impact in resource-limited settings, leading to a reduction in irrational use of antimalarial drugs (1, 2). However, diagnostic tools for other infectious conditions that present with similar symptoms, such as viral respiratory infections and mosquito-borne viral infections, continue to pose a significant challenge to implementing effective guidelines and managing cases of acute febrile illness (3, 4). The World Health Organization and the Integrated Management of Childhood Illness (IMCI) program recommend that children with non-severe fever and negative malaria tests should be observed and monitored without the use of antibiotics (2, 5). In many low- and middle-income countries, following guidelines is challenging due to the lack of reliable diagnostic tools to determine the cause of fever in children. Healthcare providers must navigate various pressures, such as caregiver expectations, limited clinical infrastructure, and the concern of missing serious bacterial infections (5–7). Consequently, antimalarials and antibiotics are often prescribed without necessity, leading to the development of antimicrobial resistance (8–10).
A recent large multicenter study conducted across 7 sites in Sub-Saharan Africa and South Asia identified common causes of death in children below five years of age with infection reported be part of the causal chain in 549 of 632 deaths (86.9%) (11). These acute infections can be treated effectively when supported by targeted case management, accurate diagnosis, and proper follow-up. Effective case management is essential for reducing mortality and morbidity and for improving the survival of this vulnerable population (12–14). Management and treatment of AFI depend on various factors, including the patient's clinical condition and the underlying cause of the disease, which can range from bacterial and viral infections to zoonotic diseases such as mosquito-borne viral infections, as well as the challenges posed by limited treatment options (9, 15). The complexity of various cause categories leads to different treatment approaches. These approaches include reviewing clinical history, conducting physical examinations, and performing tests such as blood tests, urine and stool analyses, and specialized laboratory tests, including serology and molecular diagnostics for specific pathogens (16–18. Studies of AFI etiology found that acute respiratory viral infections were the major cause of fever and therefore treatment with antimalarials and antibiotics would not have been necessary (16). The World Health Organization recommended the use of supportive therapy while awaiting results in patients with uncomplicated acute febrile illness (2). These therapies include maintaining adequate rehydration, managing fever and pain, and ensuring rest, which are more specific for viral infections. Patients with AFI need to be monitored closely for any worsening symptoms such as difficulty breathing and persistent vomiting (17, 18). As this may be a sign of a serious illness and can lead to further complications if left untreated, prompt intervention may be needed (17, 19). Guidelines for managing common Severe AFI, such as localizing infections like acute gastroenteritis, pneumonia, urinary tract infections, and malaria, are well outlined in a step-by-step approach. However, management of other causes of acute febrile illness remains less clear, leading to diagnostic and clinical management uncertainties. As a result, clinicians in low and middle-income countries often prescribe empirical antibiotics that may be unnecessary or ineffective. A study in Mwanza reported that approximately 76% of pediatric patients were overprescribed antimalarials. This study aimed to evaluate the clinical spectrum and management outcomes of acute febrile illnesses in children presenting to five health facilities in Mwanza, Tanzania.
Methods
2
Study design and population
2.1
A prospective cohort study was conducted across five health facilities in Northwestern Tanzania, as previously described (20), children were eligible if they had a fever (≥38 °C) and at least one of the following symptoms: 1) fever lasting less than 7 days; 2) vomiting; 3) headache; 4) rash; or 5) joint pain. Patients with incomplete data or in critical condition requiring intensive care (such as trauma or acute injury) were excluded from the study.
Study setting/region
2.2
Part of this cohort has been described in a our previously publication titled “non-malarial etiology of acute febrile episodes in children attending five healthcare facilities in Mwanza, Tanzania years 2020–2021” (20). The five sites in which data were collected includes Bugando Medical Centre (BMC), Sekou Toure Region Referral Hospital (STRRH); BHC, Buzuruga Health Centre (BHC), Nyamagana District Hospital NDH and SDDH, Sengerema Designated District Hospital (SDDH). According to the 2022 national census, the region had a population of 3,699,872, compared to 2,772,509 in the 2012 census. Mwanza Region is the second most populous region in Tanzania, and all five health facilities are located within it (Tanzania Health Data Survey 2022) (21).
Follow-up and outcomes
2.3
All children with acute febrile illness were followed to determine the management outcome. Clinical disease spectrum, diagnostic practices, prescribing practices in relation to antibiotics and antimalarials, and clinical outcomes at weeks 1, 2, and 4 were assessed. All participants were followed by phone, in addition to hospital chart reviews. Informed written consent was obtained from caregivers, and assent was additionally sought from children aged 7 years and above.
Data collection
2.4
During the data collection period, research team from all five health facilities was trained on protocol standard operating procedures focused on data collection procedures and patient documentation of the baseline clinical management on the day of enrollment. Data were collected using a structured questionnaire during enrollment, follow-up, and retrospective hospital chart reviews.
Data collected on the day of enrollment included sociodemographic details (age, sex), signs and symptoms, treatments before and during presentation, illness duration, physical examination findings, immunization history, laboratory results, type of imaging and their results and clinical diagnoses.
During follow-up, data collected included the child's status, fever resolution or persistent readmissions, and any reported complications inpatients. The study team, in collaboration with caregivers, gathered clinical outcome data through mobile phone interviews. Retrospective medical records were collected at the facility level, covering patients' characteristics, admission status, medications given, duration of hospital stays, clinical observations, and referrals to higher-level facilities. This data was documented in paper forms at district and health centers (extracted from patient books) and electronic health records at tertiary and regional hospitals, in accordance with the study protocol.
Clinical and laboratory investigations
2.5
The research team conducted a history and physical examination. Laboratory investigations were performed according to specific hospital standard operating procedures. Routine investigations that were performed on children presenting with acute fever at a tertiary-level hospital (BMC) and a secondary-level hospital (STRRH) included: malaria rapid test, malaria microscopy, complete blood count (CBC), human immunodeficiency virus (HIV) testing, stool microscopy, and urinalysis (both dipstick and microscopy). Blood and urine cultures were performed subject to the availability of the reagents and consumables and at the clinician's discretion, based on the case presentation. The decision to perform Chest radiography (CXR) followed the indications prescribed in the national Standard Treatment guidelines subject to the availability of radiological services. For primary-level hospital districts and health centers, routine investigations included malaria rapid tests, malaria microscopy, human immunodeficiency virus (HIV), stool microscopy, and urinalysis (both dipstick and microscopy) when available.
Diagnostic investigations conducted for each participant, according to the study protocol, included a rapid malaria test, a rapid dengue test, malaria microscopy, CBC, urinalysis, blood and urine cultures, and multiplex PCR targeting arboviral infections (blood). Additionally, singleplex PCR for dengue was performed. For participants with flu-like symptoms, multiplex PCR to detect respiratory pathogens was also performed using throat swabs sample.
Diagnosis and management
2.6
The diagnosis and clinical management of the study participants were outlined in accordance with the case management protocol detailed in Table 1.
All participants' laboratory results except multiplex PCR for arboviral infections, urine and blood cultures, and PCR for Nasopharyngeal swabs, were provided to the attending clinicians on the day of enrollment to assist patients' management. Children were seen as either outpatient or inpatients. Initial treatments, including types of antibiotics, antimalarials, antipyretics, and pain relief, were documented by the study team. Antibiotic use as indicated by positive urinalysis, a full blood count suggesting sepsis (elevated WBC count above the normal range of 4.0–11.0 × 10^9^/L, with a high neutrophil count >9 × 10^9^/L) or a clinical diagnosis such as acute tonsillitis, otitis media, or pneumonia, following Tanzania national guidelines, WHO standards, and IMCI protocols was considered appropriate (21–23).
All enrolled children were followed up; children who were not admitted were followed via phone calls on days 7 (± 1), 14, and 28, depending on clinical and laboratory findings. Participants with positive culture results were asked to return to the facility for further management. The study considered the clinical conditions listed in Table 1, these conditions were defined according to the Tanzania Ministry of Health's Standard Treatment guidelines (2021) (21), adapted from World Health Organization (WHO) guidelines for the management of common childhood illnesses (2013) (23). Laboratory confirmation was required for study-specific definition of malaria, bloodstream infections, urinary tract infections (UTIs), and anemia. Febrile participants with no identifiable source of infection based on available clinical and laboratory investigations were classified as having undifferentiated fever.
Data analysis
2.7
Data were double-entered into Microsoft Excel and analyzed with STATA version 15 (24). Categorical variables, including sociodemographic characteristics and clinical diagnoses, treatments, and outcomes, were summarized using frequencies and percentages. Quantitative data, including child age, sex, duration of illness, and hospital stay, were summarized using the median and interquartile range (IQR). Differences in demographic and clinical characteristics, diagnoses, prescribed treatments (per Tanzania guidelines), and outcomes between lower-tier (health centers) and higher-tier (tertiary hospital) facilities were evaluated using the Pearson Chi-square test or Fisher's exact test, as appropriate. A p-value < 0.05 was considered statistically significant.
Results
3
Sociodemographic characteristics of study participants
3.1
During the study period, a total of 2,114 children were screened, and 527 met the eligibility criteria. Of those, 21 were excluded. A total of 436 were included in the final analysis (Figure 1). Of the 436 participants, 56.4% were male. Detailed sociodemographic and clinical characteristics were described previously (20). Of the enrolled children, 335(76.8%) were from four urban hospitals (BMC, SRRH, NDH, BHC) and 101(23.2%) were from one rural hospital (SD).
Flow chart of the study participants to health facilities in Mwanza, Tanzania (2020–2021).
Spectrum of clinical presentations
3.2
The study's definitions indicated that the primary diagnoses among enrolled children, based on outpatient and inpatient charts, were malaria, acute respiratory infections, urinary tract infections, and acute gastroenteritis. According to WHO criteria, 31.2% (136/436) of children were diagnosed with acute respiratory infections, with 56.6% (77/136) having upper respiratory tract infections and 43.4% (59/136) diagnosed with pneumonia. Malaria was identified in 45% (197/436) of cases. Additional clinical diagnoses are detailed in Table 2, and some conditions requiring empirical antibiotics are listed in Table 3.
Laboratory diagnosis and confirmatory diagnosis
3.3
Among the 103 patients with a diagnosis of malaria, 67 (65.0%) tested positive with MRDT, while 36 (35.0%) had a positive malaria blood smear, with a mean parasite count of ± SD (30.8 ± 40.2). Overall, PCR testing detected Plasmodium falciparum in 12.0% (52/436) of the study participants (Table 4). Among the 59 patients with pneumonia, 22.0% (13/56) showed indications for chest x-rays, and 61.5% (8/13) of these x-rays were performed. Blood cultures were positive in 6.7% (4/59) of pneumonia cases. No participant tested PCR-positive for any arboviral pathogens, as previously noted (20).
Clinical management
3.4
The management was done by specialists at BMC and SRRH while in district hospitals (SD and NDH), and Health centre (BHC) patients were managed by medical officers an clinical officers. Of the 436 children enrolled, 356 were treated as inpatients and 78 as outpatients. Two children left before receiving initial treatment. Among these patients, 27.8% received pre-medication prior to hospital arrival, with antipyretics/analgesics (Paracetamol, Ibuprofen and Diclofenac) being the most frequently reported medications. Details on medications, clinical management, and prescription patterns are summarized in Table 5. Antimalarial drugs were prescribed to 38.9% (169/434) of the patients, with 103 diagnosed with malaria based on a positive MRDT or blood smear. Additionally, 66 patients (39.0%) who received antimalarial treatment tested negative on both MRDT and blood smear. The malaria management protocol across all study sites for uncomplicated malaria was outpatient-based, prescribing artemether-lumefantrine twice daily for three days. In case of complicated malaria, artesunate was administered intravenously in three doses within 24 h (at admission, 12-hour and 24 h). With improvement, treatment was then switched to oral artemether-lumefantrine twice daily for three more days, as recommended in the Tanzania and WHO guidelines (21, 22).
In total, 76.3% (333/434) of patients had examinations that ruled out malaria as the cause of the current fever, so they were classified as having non-malarial febrile illness. Diagnostic clarification of the clinical picture and the pathogen causing the fever was usually carried out by history and physical examination, with MRDT at the district hospital (NDH, SDDH) and the Health Center (BHC). In some cases, additional laboratory tests, such as urine or stool microscopy, were performed. At the tertiary hospital (BMC), laboratory tests included blood smear, MRDT, urine, stool, culture, and complete blood counts (CBC). At the regional hospital (SRRH), laboratory tests included MRDT, CBC, urine and stool, with occasional blood culture and urine culture.
Antibacterial agents were prescribed to 284 (65.4%%) of 434 patients. Among inpatients, 75 of 78 (96.4%, 95%CI: 92.3–100) received antibiotics compared to 209 of 356 (57.6%, 95%CI: 52.4–62.7) of those treated as outpatients (P < 0.001). At enrollment, 46.0% (200/434) of children were prescribed antibiotics empirically. Indications for empirical use of antibiotic in the study sites included positive urinalysis, elevated blood count (White blood cells) suggesting sepsis, or clinical diagnosis with signs and symptoms requiring empirical treatment such as acute tonsillitis, otitis media or pneumonia. Around 29.6% (84/284) were prescribed antibiotics without clear clinical indication; including children with WHO clinical diagnosis of upper respiratory tract infection and acute gastroenteritis. Among patients who received antibiotics only 9.2% (26/284) had a positive blood culture. A total of 136 of the participants were diagnosed with respiratory infections. All participants diagnosed with pneumonia were treated with antibiotics using intravenous ampicillin and gentamicin, and ceftriaxone for the uncomplicated upper respiratory. Children with upper respiratory tract infections were also treated with antibiotics (including Ampiclox syrup, Cotrimoxazole, and Azithromycin).
Distribution of antibiotics prescribed
3.5
Among children with acute febrile illness across the five health facilities, 65.7% (284/434) received antibiotics at the initial antibiotic prescription; the medications varied between health facilities. Most children received only one antibiotic agent 65.5% (186/284), while 32.7% (93/284) received a combination of two antibiotics, and 2.1% (6/284) received a combination of three antibiotics. The most commonly prescribed antibiotics were ampicillin (25.0%), gentamicin (24.7%), and ceftriaxone (8.2%) (Figure 2). Additional antibiotics administered to inpatients after culture and sensitivity results included ciprofloxacin, meropenem, vancomycin, and piperacillin-tazobactam.
Distribution of antibiotics prescribed among children presenting to health facilities in Mwanza, Tanzania (2020–2021) Key: “Others Antibiotics” include: ciprofloxacin, meropenem, vancomycin, piperacillin-tazobactam and amoxicillin-clavulanic acid.
Clinical outcomes and follow-up
3.6
All patients were followed by scheduled phone calls on day 7, 14 and 28 after discharge. However, to capture the patients complications for inpatients, patients were followed up at their respective hospitals till discharge. Data was collected by the research team, and additional clinical information, such as complications and blood transfusion records (Figure 3) were retrieved from the hospital electronic records system for patients admitted to tertiary and regional hospitals. A total of 428 participants (98.2%) completed the 7-day follow-up. A total of 7.6% (33/434) of study participants were referred to a higher level of care. Of the 428 participants whose status was known by day 7, 0.7% (3/428) died in hospital. Two died from pneumonia, and one died secondary to acute gastroenteritis complicated with shock and anemia. Three outpatient participants could not be reached and were considered lost to follow-up. Fever had resolved in 398 participants (93.0%). Fever persisted beyond day 7 in only 30 patients. Of the patients contacted on day 14, 416 (95.4%) completed the follow-up, while 12 were not reached; all were outpatients. Fever had resolved in all patients contacted, but 2 patients were readmitted (Table 6).
Distributions of complications retrieved from patients records among children attended in health facilities in Mwanza, Tanzania (2020–2021).
Of the 401 participants who completed the day 28 follow-up, one patient died. The cause of death could not be clearly determined; however, according to the parents, the child had persistent fever and continued treatment with traditional medicine. A retrospective review of laboratory results showed that the child tested positive for bocavirus via PCR from a nasopharyngeal swab, but this could not be definitively linked as the cause of death. Overall, there were 4 deaths out of 401 participants (1%) by day 28. Among children with presumed dengue infection based on IgG/IgM serology, fever had resolved in all cases. Out of 434 patients followed, 10.8% (47/434) developed complications, as shown in the Figure 3.
Predictors of hospitalization
3.7
Adjusted analysis indicated that children presenting with headaches (OR: 12.97, 95% CI 2.33–72.23, P < 0.003), hepatosplenomegaly (OR: 29.17, 95% CI 1.35–630.91, P = 0.032), and those clinically diagnosed with meningitis have higher odds of admission (OR: 41.33, 95% CI 2.38–718.12, P < 0.011). In the initial analysis, sociodemographic factors such as age 1–5 years, female gender, and symptoms such as fever lasting less than 3 days, along with muscle and joint pain, were associated with admission, but these associations became non-significant after adjusting for other variables (see Supplementary Table S2).
Discussion
4
This prospective study analyzed the clinical differential diagnosis patterns and management outcomes of children presenting with acute febrile illness at five healthcare facilities in Tanzania (four urban and one rural). The study found that overprescription of antibiotics and antimalarials occurred in about 29.6% and 39% of cases, respectively. The most common diagnoses were acute respiratory infections, including upper respiratory infections and pneumonia, followed by malaria. Malaria was evenly distributed across all sites but confirmed Plasmodium falciparum cases detected through microscopy and PCR were more frequent at Nyamagana District Hospital and Buzuruga Health Centre. The rate of positive Plasmodium falciparum tests was lower at tertiary and secondary hospitals, likely because patients first seek care at primary facilities where they may have already received treatments, including antimalarials. None of the children were diagnosed with arboviral infections, possibly due to limited awareness among health workers about dengue and chikungunya in Tanzania, despite reports of outbreaks and studies indicating their presence (25, 26).
Common complications observed in admitted children included anemia (36.0%), dehydration (9.1%), shock (8.5%), and acute kidney injury (8.5%). These were especially frequent in patients diagnosed with malaria and septicemia. It was noted that children with uncomplicated malaria can quickly develop into severe or complicated malaria due to immature immunity. The pathophysiology of severe malaria involves erythrocyte destruction, reduced production, anemia, and sequestration of parasitized red blood cells (pRBCs) in blood vessels (27). Observed complications of malaria in this study, highlighting the importance of emphasizing ongoing primary preventive strategies, such as use of insecticide-treated bed nets and malaria vaccination for all children in moderate and high endemic areas as per WHO recommendation. In addition, secondary measures to prevent severe illness, that include appropriate malaria diagnosisis and effective treatment of uncomplicated cases should be sustained. Additionally, there is a need to improve healthcare workers' understanding regarding monitoring and follow-up of children with high risk of worsening and ensuring strict compliance with protocols guidelines (27–29).
Approximately 39% of children were prescribed antimalarial drugs without diagnostic confirmation by a rapid diagnostic test or microscopy. This is lower than in a previous study conducted in the same area, where a single center reported extensive antimalarial overprescription of about 76.6% among children (4). The findings reported herein are higher, however, than those reported by Kazaura et al. in a study conducted in the Lake Victoria region that found an overprescription rate of 7.0% in 2016, 10 years ago (30). The frequency of prescribing antimalarials without a diagnostic indication may stem from healthcare workers' uncertainty in trusting negative microscopy or MRDT results, as well as the patient's clinical condition (30, 31). Other studies in Ethiopia and Mozambique have reported antimalarial overprescription rates ranging from 7.0% to 72%, respectively (31, 32). The 2021 Tanzania National Guidelines and WHO Guidelines highlighted that malaria testing should be performed with an MRDT before treatment in all health facilities without access to the quality gold-standard malaria slide microscopy (21, 22). This challenge is worsened by the scarcity of diagnostic tools for children with undifferentiated fever, which hampers clinicians' ability to identify causes other than malaria. Moreover, in resource-limited settings, clinicians treating febrile children showing malaria-like symptoms might be more prone to empirically prescribe antimalarials (5, 33). Overprescription of antimalarials raises concerns about the long-term efficacy of malaria treatment and the emergence of drug resistance. Artemisinin resistance markers have been reported in various areas in Tanzania (34), including a recent publication that reported the detection of the Pfk13 R561H mutation, associated with partial artemisinin resistance, in 2 patients enrolled in 2022 in Mwanza, Tanzania (35). This finding is particularly of concerning as it may compromise first-line treatment.
The main indication for prescribing antimicrobials at the initial visit in tertiary and regional hospitals was an elevated white blood cell count, urinalysis findings, and illness severity while awaiting culture results. At the primary health care level, the indication to start antibiotics depended on the clinical presentation of patients and clinicians' judgment, as most investigations were not available, especially in outpatient clinics. Cultures and complete blood count was were not part of routine investigations, therefore, overprescription of antibiotics of 29.6% in this cohort should be interpreted with caution, particularly in light of the above challenges, especially in district hospitals and health centers. Antibiotic prescriptions without indication were most often noted in children with a clinical diagnosis of upper respiratory tract infection and acute gastroenteritis (Supplementary Table S1). As observed in previously, this trend of overprescription was more evident among inpatients at tertiary hospitals (32, 36). Notably, most febrile children who did not receive antimalarials or antibiotics still recovered, suggesting that their illnesses were likely due to other causes, more likely viral infections, which do not respond to antimicrobial or antimalarial therapy (37, 38). This underscores the need for adherence to clinical guidelines, improved diagnostic capacity, better healthcare education, and trust in laboratory results in order to ensure adequate and high-quality care for this vulnerable population.
Fever management remains a major challenge for most clinicians, especially in settings where diagnostic tools are limited. In this study, fever resolved in 92.3% of participants on day 7 of follow-up and in 96.0% by day 28. Children with negative malaria often experienced spontaneous fever resolution supporting obversion from other African studies (34, 37, 38). These findings indicated that there is room to wait before starting antimalarials and antibiotics for children with uncomplicated febrile illness. The mortality rate observed in the current study was 1%. This is consistent with the findings of another study conducted in Ethiopia, which reported a mortality rate of 1.5%. Prompt case detection and appropriate management coupled with follow-up of patients are essential to achieving the Sustainable Development Goal of reducing under-five mortality to less than 25 deaths per 1,000 live births by 2030, particularly for preventable diseases (39, 40).
Strength and limitation
4.1
A key strength of the present study is the integration of clinical and laboratory data reported in a previous study using WHO diagnostic algorithms, along with robust follow-up on outcomes. This provides a solid foundation for future qualitative research into the root causes of overprescription of antimalarials and antibiotics and for quality improvement initiatives focused on the more rational use of antibiotics and antimalarials. Nevertheless, the current analysis has potential limitations; i) during follow-up, recall bias and chart review may have affected the reliability of the data, especially for caregiver-reported outcomes, ii) laboratory and diagnostic testing did not cover all known potential infections limiting the information needed to improve overall fever management guidelines, iii) patients' prior treatment history, local antimicrobial resistance patterns, and medication costs could have influenced clinicians' treatment decisions and iv) participants were enrolled in five health facilities; sampling was not random across the region, and other clinical settings were not included. Therefore, selection bias related to facility choice was possible, limiting the generalizability of the findings.
Conclusion and recommendation
5
The high rate of children with acute respiratory tract infections (ART) and pneumonia underscores the need for intensified ART management, particularly by promoting early care-seeking behaviour and treatment to reduce hospitalizations. The varying malaria transmission levels across study sites underscore the need to strengthen interventions in high-risk areas, and efficiently allocate resources toward malaria elimination. Notably, about 29.6% of antibiotic prescriptions lacked clinical justification, and 39.0% of children with febrile illnesses received antimalarial drugs despite negative rapid diagnostic tests (MRDT) or blood microscopy results. This underscores the need to improve antimicrobial use by incorporating diagnostic tools to identify common pathogens coupling with antimicrobial stewardship programmes and improved healthcare workers' adherence to guidelines across health facilities at all levels.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Escadafal C Geis S Siqueira AM Agnandji ST Shimelis T Tadesse BT Bacterial versus non-bacterial infections: a methodology to support use-case-driven product development of diagnostics. BMJ Glob Health. (2020) 5(10):e 003141. 10.1136/bmjgh-2020-00314133087393 PMC 7580043 · doi ↗ · pubmed ↗
- 2World Health Organization. WHO informal consultation on fever management in peripheral health care settings: a global review of evidence and practice).
- 3D'Acremont V Malila A Swai N Tillya R Kahama-Maro J Lengeler C Withholding antimalarials in febrile children who have a negative result for a rapid diagnostic test. Clin Infect Dis. (2010) 51(5):506–11. 10.1086/65568820642354 · doi ↗ · pubmed ↗
- 4Huth PF Addo M Daniel T Groendahl B Hokororo A Koliopoulos P Extensive antibiotic and antimalarial prescription rate among children with acute febrile diseases in the lake Victoria region, Tanzania. J Trop Pediatr. (2021) 67(1):fmaa 135. 10.1093/tropej/fmaa 13533575804 · doi ↗ · pubmed ↗
- 5Wiedenmayer K Ombaka E Kabudi B Canavan R Rajkumar S Chilunda F Adherence to standard treatment guidelines among prescribers in primary healthcare facilities in the Dodoma region of Tanzania. BMC Health Serv Res. (2021) 21:272. 10.1186/s 12913-021-06257-y 33761948 PMC 7990379 · doi ↗ · pubmed ↗
- 6Reñosa MD Dalglish S Bärnighausen K Mc Mahon S. Key challenges of health care workers in implementing the integrated management of childhood illnesses (IMCI) program: a scoping review. Glob Health Action. (2020) 13(1):1732669. 10.1080/16549716.2020.173266932114968 PMC 7067189 · doi ↗ · pubmed ↗
- 7Green C Krafft H Guyatt G Martin D. Symptomatic fever management in children: a systematic review of national and international guidelines. P Lo S One. (2021) 16(6):e 0245815. 10.1371/journal.pone.024581534138848 PMC 8211223 · doi ↗ · pubmed ↗
- 8Versporten A Bielicki J Drapier N Sharland M Goossens H Project Group ARPEC The worldwide antibiotic resistance and prescribing in European children (ARPEC) point prevalence survey: developing hospital-quality indicators of antibiotic prescribing for children. J Antimicrob Chemother. (2016) 71(4):1106–17. 10.1093/jac/dkv 41826747104 · doi ↗ · pubmed ↗