Long-term follow up of malignant transformation of epidermoid cyst at the cerebellopontine angle based on serial imaging findings; A case report and literature review
Koji Saito, Akihiko Teshigawara, Miku Maeda, Nei Fukasawa, Yasuharu Akasaki, Yuzuru Hasegawa, Masayuki Shimoda, Yuichi Murayama, Toshihide Tanaka

TL;DR
A case report describes a rare malignant transformation of an epidermoid cyst after over 10 years, highlighting imaging changes and treatment challenges.
Contribution
This case report adds to the limited literature on malignant transformation of epidermoid cysts, emphasizing imaging features and treatment considerations.
Findings
Malignant transformation of an epidermoid cyst was confirmed after 10 years of follow-up.
Neuroradiological changes on imaging, such as contrast enhancement and edema, indicated malignancy.
Postoperative radiotherapy did not prevent carcinomatous meningitis in this case.
Abstract
We report a case of malignant transformation of epidermoid cysts during long-term follow up more than 10 years with literature review. Epidermoid cysts are benign congenital tumors, accounting for 0.2–1.8% of intracranial tumors. Malignant transformation is extremely rare, with limited reports describing the imaging features and prognosis. A 69-year-old woman had presented with a tumor exhibiting hyperintensity on diffusion-weighted imaging at the left cerebellopontine angle and had been followed-up for the past decade. After 10 years, she developed left facial paralysis and hearing impairment. Contrast-enhanced lesions appeared within the tumor, accompanied by edema. Intraoperative findings revealed a tumor with two distinct components of pearly tumor and hematoma invading the cranial nerves. The pathological diagnosis was squamous cell carcinoma without primary malignancies,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
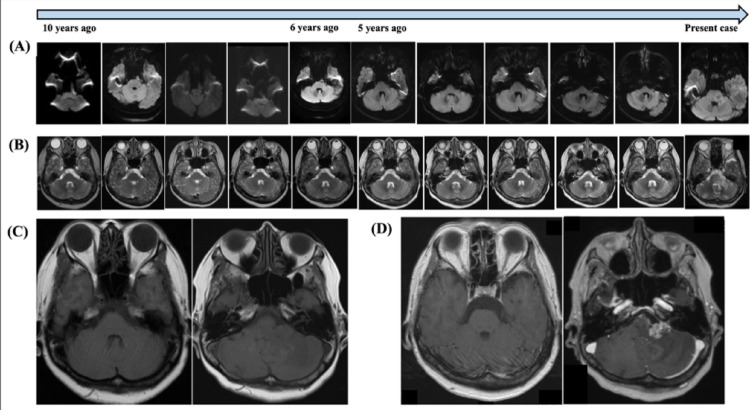 Figure 1
Figure 1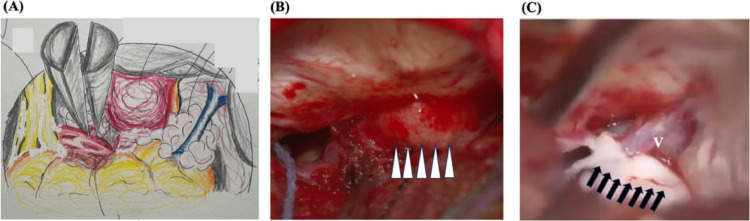 Figure 2
Figure 2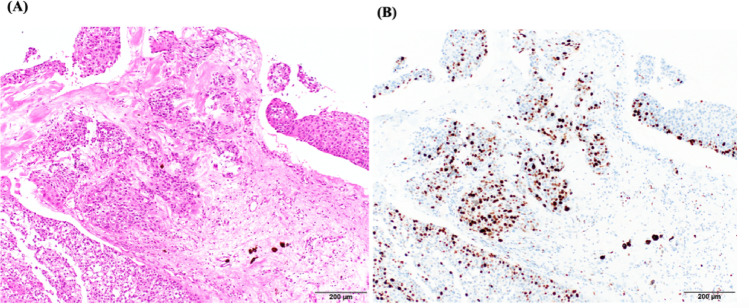 Figure 3
Figure 3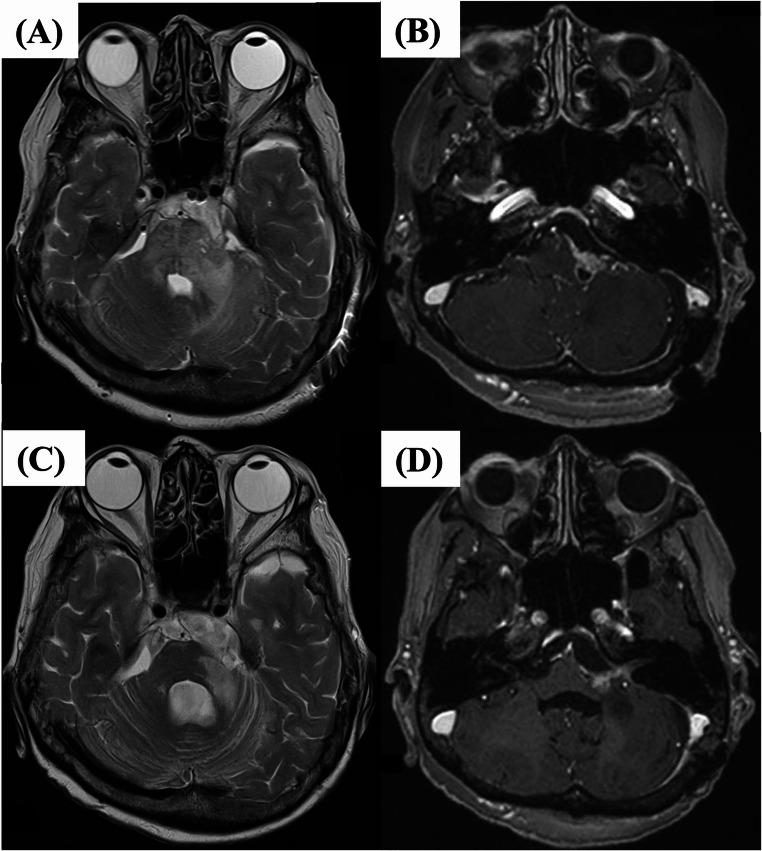 Figure 4
Figure 4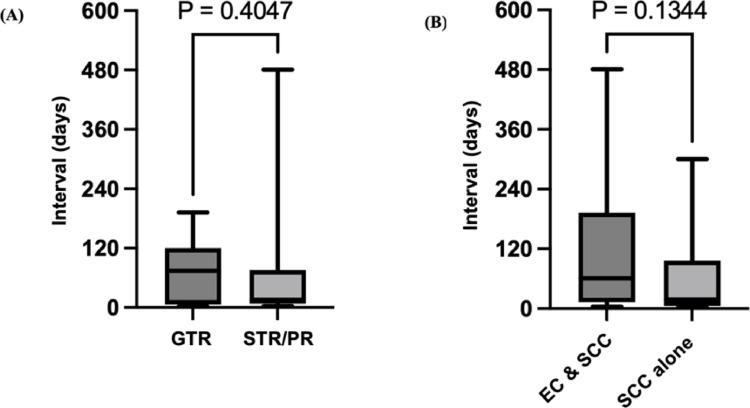 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTeratomas and Epidermoid Cysts · Meningioma and schwannoma management · Facial Nerve Paralysis Treatment and Research
Introduction
Epidermoid cyst (EpiC) is generally considered a benign tumor arising from remnant fetal tissue (0.2–1.8% of intracranial tumor) [1]. And cholesteatoma is also known as epidermoid cyst especially in involving the petrous bone and the intracranial region. Malignant transformation is extremely rare and few reports have described its imaging characteristics and prognosis. We present a case showing malignant transformation of EpiC in the left cerebellopontine angle that showed rapid progression 10 years after the initial diagnosis, necessitating craniotomy. Malignant transformation of EpiC was confirmed by pathological examination and whole-body imaging. Based on the present case, we reviewed previously reported cases of malignant transformation of EpiC, identifying 101 cases in the literature. We summarized key aspects such as pathology, extent of resection, postoperative adjuvant therapy, and duration from initial diagnosis to malignant transformation.
Case report
A 69-year-old woman presented with tinnitus that had developed one month earlier. A tumor at the left cerebellopontine angle had been incidentally discovered on magnetic resonance imaging (MRI) a decade earlier, exhibiting high intensity on diffusion-weighted imaging (DWI) and T2-weighted imaging (T2WI) without enhancement on gadolinium-enhanced T1-weighted imaging (T1Gd); these findings were consistent with the typical imaging characteristics of an epidermoid cyst. DWI was performed at the referring hospital with a b-value of 1000 s/mm². Information regarding the MRI scanner manufacturer and magnetic field strength was not available. The case had been followed-up for 10 years with non-contrast MRI during “tumor dormancy status” (Fig. 1a and b). Therefore, we assumed this tumor was benign.
Fig. 1. Serial imaging results, a,** b)** Serial images from diffusion-weighted imaging (DWI) (a) and T2-weighted imaging (T2WI) (b) on magnetic resonance imaging (MRI) during 10-year follow-up. Representative slices were selected to best demonstrate the lesion on each imaging study. c,** d)** Axial T1-weighted MRI at initial detection (c) and just before surgery 10 years later (d) (left panels: without Gd enhancement; right panels: with Gd enhancement)
On this presentation, she displayed left facial paralysis and hearing impairment. MRI with gadolinium enhancement was re-investigated, since we suspected that the tumor became malignant progression. Contrast-enhanced lesions appeared within the tumor and left pons, accompanied by edema involving the middle cerebellar peduncle and cerebellar hemisphere (Fig. 1b). In addition, the previously observed hyperintensity on DWI had disappeared (Fig. 1a). There were no tumors in the chest and abdomen CT with serum tumor markers were within normal limits (data not shown).
Due to the rapid symptom progression and the need for pathological confirmation to guide postoperative therapy, surgical resection was performed.
Intraoperative findings
Craniotomy was performed via a retrosigmoid approach. Intraoperatively, two distinct components were observed at the left cerebellopontine angle (Fig. 2a). The first component was a red-white hemorrhagic tumor wrapped in a membrane adherent to the cerebellum, located near the acoustic meatus and lower cranial nerves (Fig. 2b). The second component was a pearly tumor situated around the petrosal vein, invading the internal acoustic canal and adjacent facial and acoustic nerves (Fig. 2c). The facial and acoustic nerves could not be clearly detached from the tumor, so surgery was ended with partial resection.
Fig. 2. Intraoperative findings for gross appearance of the tumor. Schematic drawing of intraoperative findings of the tumor at the cerebellopontine angle (a). A red component (arrowhead) appears attached to the dura along the petrous bone (b) and a pearly tumor (arrow) appears adherent to the petrous vein (V) (c)
Pathological findings
Atypical epithelial cells with loss of polarity were observed within the membranous structures. In the main tumor mass, nests of squamous cell carcinoma (SCC) cells were found densely proliferating against a background of fibrous stroma, with minimal keratinization but evident necrosis. Typical findings of keratinization for EpiC were not observed (Fig. 3a). The MIB-1 index was 50.8% (Fig. 3b).
Fig. 3. Pathological findings of the tumor at the cerebellopontine angle. a) Hematoxylin and eosin staining. Typical squamous cell lineage and keratinization was obsereved. b). Immunohistochemistry for MIB-1. Tumor cells in recurrent tumors were strongly positive for MIB-1 of which labeling index was 50.8%
Postoperative clinical course
Based on the pathological findings as described above, whole-body computed tomography (CT) was performed and tumor marker levels were examined. No primary cancers were identified elsewhere. Given the long-term clinical course detected by radiographic findings along with histological and serological findings, the final diagnosis was SCC representing malignant transformation of EpiC. The patient underwent postoperative local radiotherapy (54 Gy in 27 fractions) to the residual tumor identified on postoperative MRI (Fig. 4a and b). After treatment, the contrast-enhanced lesion and associated edema tended to regress without further progression (Fig. 4c and d). However, 4 months later, the patient gradually developed immobility and was diagnosed with carcinomatous meningitis from lumbar puncture, although no new abnormalities were detected on MRI. The patient was transferred to another facility for palliative care.
Fig. 4. Postoperative magnetic resonance imaging (MRI). T2-weighted (a) and T1-weighted imaging with gadolinium enhancement (b) showing the residual tumor with high-intensity signal at the middle cerebellar peduncle (a) and tumor along the facial nerve (b). MRI after radiotherapy. T2- (c) and T1-weighted imaging with gadolinium enhancement (d) show regression of the perifocal edema (c) and residual tumor (d)
Discussion
We considered two possible mechanisms for the malignant transformation of the EpiC: malignant transformation of residual tumor tissue, or de novo emergence of a malignant tumor. An issue of interest was whether any difference in overall survival exists between cases in which surgery was performed after the development of new symptoms or imaging changes, as in the present case, and cases in which surgery was performed at the time of initial diagnosis. The problem of the present case to diagnose the malignant transformation of EpiC was the lack of initial pathological specimen. We judged by neuroradiological alteration from the non-enhanced tumor to the enhanced tumor with deteriorated clinical symptom.
Review of EpiC with malignant transformation (Table;1)
Table 1. Characteristics of literature included in the review (n=103). In this review, mean age at diagnosis was 54 years, and the most common location was the posterior cranial fossa, including the cerebellopontine angle (76.5%). Mean interval from initial diagnosis to malignant transformation was 105.5 months. Among the 48 reported cases, 38 underwent radiotherapy, 4 underwent chemotherapy alone, and 6 received chemoradiotherapyParametern (%)MeanAge, years10154Sexmale54 (53.5)female47 (46.5)Locationcerebellopontine angle57 (56.4)other posterior fossa19 (18.8)supratentorial23 (22.8)Interval between initial & salvage surgery, months48 (47.5)106.1Postoperative adjuvant therapyradiation38 (37.6)chemotherapy4 (4.0)chemoradiation6 (5.9)Pathological samples obtainedinitial surgery94 (93.1)salvage surgery/autopsy40 * (39.6)* Diagnosis determined by CSF cytology (n=2)
We reviewed previously reported cases of malignant transformation of EpiC, identifying 103 cases in the literature (Tables 1 and 3). To review previously reported cases of malignant transformation of epidermoid cysts, we investigated a literature search in PubMed using the keywords “epidermoid cyst” and “malignant transformation.” Additional cases changing from EpiC to malignant transformation were identified through manual screening of the reference lists of relevant articles. In this review, mean age at diagnosis was 54 years, and the most common location was the posterior cranial fossa, including the cerebellopontine angle (76.5%). Mean interval from initial diagnosis to malignant transformation was 106.1 months, with the longest reported interval being 480 months [2]. The present case showed a relatively long period of follow-up compared to previous reports. In addition, the true interval in this case may have exceeded 120 months, as the patient was asymptomatic at the time of initial diagnosis.
Consideration of latent period between initial diagnosis and malignant transformation
Forty-nine cases were included in the comparative analysis of the latent period of malignant transformation, stratified by extent of resection. This included 20 cases classified as gross total resection (GTR) and 29 cases classified as STR or PR. Among these 49 cases, analysis was performed on those cases with a clearly documented interval to recurrence. Mean interval from initial diagnosis to malignant transformation was 79.9 months in the GTR group and 82.1 months in the STR/PR group (GTR, n = 11 or STR] or [PR] [n = 17]), showing no significant difference (p = 0.423; Fig. 5A). Statistical analysis was performed using the Mann–Whitney test. Due to the small number of reported cases and the presence of a few STR/PR cases with exceptionally long intervals, these results should be interpreted with caution [2–4].
Fig. 5. Comparison of interval between initial surgery and salvage surgery for recurrence**. (a)** The interval (in months) tended to be longer for the group with gross total resection (GTR) (n = 11) than in the group with subtotal resection (STR) or partial resection (PR) (n = 17), although the difference was not significant (p = 0.423). (b) The interval tended to be longer in the group with concomitant epidermoid cyst and squamous cell carcinoma (EpiC + SCC) (n = 19) than in the group with SCC alone (n = 14), although the difference was not significant (p = 0.120)
Imaging changes suggestive of malignant transformation
Previous reports have suggested that rapid progression of clinical symptoms, changes in tumor appearance on DWI and T2WI, appearance of contrast-enhanced lesions, and development of peritumoral edema are indicative of malignant transformation [1]. In the present case, a change in DWI findings—specifically, the disappearance of lesion hyperintensity—was observed between 5 and 6 years before surgery, despite the asymptomatic status of the patient (Fig. 1a). No significant changes were observed on T2WI during the same period (Fig. 1b). In the present case, malignant transformation might have occurred during this period, but accurate timing of the malignant transformation was difficult since the patient remained asymptomatic and contrast-enhanced MRI had not been performed during this period. If contrast-enhanced MRI had been conducted, the malignant transformation might have been detected earlier.
Pathological diagnosis of initial and recurrent tumors (Table 2)
Table 2. Pathological diagnoses of initial and recurrent tumors (n = 94). Ninety-four cases included information about pathological diagnosis. Among these, 40 cases were diagnosed as EpiC alone, 48 cases as EpiC with SCC (including 10 autopsy cases), and 6 cases as SCC alone. Of these, recurrent tumor samples were available for only 39 casesPathological diagnosis n Initial sampleRecurrent sampleEpiC alone400EpiC and SCC48*20SCC alone620 * *
Ninety-four cases included information about pathological diagnosis (Table 2). Among these, 40 cases were diagnosed as EpiC alone, 48 cases as EpiC with SCC (including 10 autopsy cases), and 6 cases as SCC alone. Of these, recurrent tumor samples were available for only 40 cases, as the other cases already diagnosed with malignant transformation had proceeded directly to postoperative therapy. Among the recurrent cases, two were diagnosed by lumbar puncture [5, 6], and no initial pathological specimens were available in two other cases; the initial diagnoses in these cases were based on MRI findings, similar to the present case [7, 8]. We analyzed the difference in mean interval from initial diagnosis to second operation between samples of recurrence comprising EpiC with SCC and SCC alone. The mean interval was 121 months in the EpiC with SCC group and 60 months in the SCC alone group (EpiC with SCC [n = 19] or SCC alone [n = 14]), again showing no significant difference (p = 0.120). Statistical analysis was performed using the Mann–Whitney test. This finding may suggest that the ratio of benign to malignant components is associated with the latent period of malignant transformation. Further investigation is required to validate these results (Fig. 5B).
Significance of concomitant EpiC and SCC (Table 3) [1–102]
To verify malignant transformation of EpiC precisely and rule out the possibility of SCC from occult primary cancers, intraoperative findings might be useful for diagnosing tumors and clarifying whether benign and malignant components co-exist. Only four cases have been reported in which tumors exhibited two distinct components—a red-white hemorrhagic mass and a pearly tumor—similar to the present case. All of these were pathologically diagnosed as EpiC with SCC. Although the coexistence of two components does not establish a direct causal relationship, these findings suggest the possibility of malignant transformation of EpiC. Pathological diagnosis is essential for understanding the biological characteristics of a tumor and evaluating the growth potential, both of which are critical for predicting overall survival and making decisions regarding postoperative adjuvant therapy.
Table 3. Lists of patients with epidermoid cyst with malignant transformation in the literature review (n = 103). CPA, cerebellopontine angle; EpiC, epidermoid cyst; F, female; GTR, gross total resection; M, male, n.d; not described; RT, radiotherapy; SCC, squamous cell carcinoma; STR, subtotal resectionReferenceSexAge (Years)Histopathology at initial surgeryInterval from initial surgery to recurrence (months)Histopathology at surgery for recurrenceExtent of resectionLocationAdjuvant therapyFollow-upImmunohistochemistry, MIB-1 indexNarasimhaiah D et al. 2023 [11]M39EpiC5SCCGTRCPAn.d.n.d.p63(+), MIB-1 40%Gabay S et al. 2022 [37]M61EpiC+SCCn.d.n.d.STRCPART, remission at 2 months13 monthsn.d.Mliyh L et al. 2023 [70]F80EpiC+SCCn.d.n.d.STRCPAn.d.n.d.p16(-)Zhang X et al. 2023 [102]M58EpiC+SCCn.d.n.d.GTRsupratentorialRT, no recurrence at 11 monthsn.d.n.d.Yang T et al. 2024 [14]M61EpiC+SCCn.d.−GTRCPAchemoradiation11 monthsCK (AE1/AE3)(+),GATA3(+), vimentin(+),MIB-1 20%Dey S et al. 2024 [28]F52SCCn.d.−STRdorsal midbrainRTn.d.n.d.Fox H et al. 1965 [35]M50EpiC84EpiC+SCCSTRtemporal loben.d.n.d.n.d.Toglia JU et al. 1965 [98]F53EpiC12EpiC+SCCSTRskull basen.d.died at 1 dayn.d.Goldman SA et al. 1987 [3]F59EpiC396EpiC+SCCSTRlateral ventricleRT36 monthsn.d.Salazar et al. 1987 [87]M49EpiC3EpiC+SCCGTR or STRCPAn.d.nonen.d.Abramson RC et al. 1989 [15]M37EpiC60SCCGTRCPAn.d.9 monthsn.d.Nishiura I et al. 1989 [78]M38EpiC6EpiC+SCCSTRCPAchemotherapystable at 24 monthsn.d.Knorr JR et al. 1991 [55]M74EpiC13EpiC+SCCGTR or STRCPAn.d.n.d.n.d.Tognetti F et al. 1991 [97]F67EpiC372−Nfrontotemporaln.d.n.d.n.d.Bayindir C et al. 1996 [20]F67EpiC10SCCSTRlateral ventriclenone36 monthsn.d.Murase S et al. 1999 [73]F40EpiC120SCCGTRCPAchemotherapystable at 60 monthsn.d.Asahi T et al. 2001 [9]F55EpiC156EpiC+SCCGTRCPAn.d.died at 3 monthsEMA(+), MIB-1 30%Link M et al. 2002 [64]F57EpiC12EpiC+SCCSTRCPARTdied immediatelyn.d.Akar Z et al. 2003 [18]FEpiC18SCCSTRCPAn.d.died at 5 monthsn.d.Hamlat A et al. 2005 [44]F62EpiC+SCC10−Ntemporal lobechemotherapydied at 7 monthsn.d.Tamura K et al. 2006 [96]F56EpiC96SCCGTRCPART18 monthsn.d.Ge P et al. 2009 [39]M50EpiC74EpiC+SCCGTRtemporal loben.d.Nn.d.Kano T et al. 2010 [4]F64EpiC192SCCSTRCPARTdied at 36 monthsn.d.Nakao Y et al. 2010 [75]F74EpiC240EpiC+SCCGTR or STRCPART17 monthsn.d.Hao S et al. 2010 [7]F61EpiC72EpiC+SCCSTRCPAn.d.died at 1.5 monthsn.d.Lakhdar F et al. 2011 [61]M52EpiC6EpiC+SCCGTRCPARTn.d.n.d.Chon K et al. 2012 [24]M43EpiC5SCCSTRCPARTnonen.d.Vellutini E et al. 2014 [100]F42EpiC24EpiC+SCCSTRCPAn.d.n.d.n.d.Pikis and Margolon 2016 [83]M77EpiC9EpiC+SCCSTRCPAchemoradiationdied at 6 monthsn.d.Ding S et al. 2016 [29]F55EpiC7SCCSTRtemporal loben.d.nonen.d.Solanki S et al. 2017 [92]F47n.d.36−NCPAn.d.n.d.n.d.Sakamoto H et al. 2021 [1]F59EpiC108EpiC+SCCGTRCPART7 monthsp53(+), p16(+)Ernst P et al. 1912 [32]M52EpiC+SCCn.d.−autopsyCPAn.d.n.d.n.d.Hug O et al. 1942 [48]M42EpiC+SCCn.d.−autopsyparapontinen.d.n.d.n.d.Henkel H et al. 1951 [46]M49EpiC+SCCn.d.−autopsyparapontinen.d.n.d.n.d.Yamanaka A et al. 1955 [101]M57EpiC+SCCn.d.−autopsyskull basen.d.n.d.n.d.Landers J et al. 1960 [62]F73EpiC+SCCn.d.−autopsycerebellumn.d.n.d.n.d.Kömpf D et al. 1977 [58]F57EpiC+SCCn.d.−autopsyparapontinen.d.n.d.n.d.Scully R et al. 1977 [89]M59EpiC+SCCn.d.−GTR or STRCPARTn.d.n.d.Dubois P et al. 1981 [30]M53EpiC+SCCn.d.−STRCPARTdied at 2 monthsn.d.Takado M et al. 1982 [95]F54EpiC+SCCn.d.−biopsyparapontinen.d.n.d.n.d.Lewis A et al. 1983 [63]F53EpiC+SCCn.d.−STRparasellarn.d.died at 1.2 monthsn.d.Bondeson L et al. 1984 [21]F56EpiC+SCCn.d.−biopsyCPAn.d.n.d.n.d.Giangaspero F et al. 1984 [42]M45SCCn.d.−STRparietooccipital lobeRTn.d.n.d.Gi H et al. 1990 [41]M39EpiC+SCCn.d.−GTRCPARTn.d.n.d.Mori Y et al. 1995 [72]M41EpiC+SCCn.d.−STRCPART11 monthsn.d.Nishio S et al. 1995 [77]M57EpiC+SCCn.d.−STRCPART30 monthsn.d.Kahn E et al. 1955 [52]F37EpiC+SCCn.d.n.d.n.d.frontal loben.d.n.d.n.d.Davidson S et al. 1960 [26]M46EpiC+SCCn.d.n.d.GTRfrontal lobeRTnonen.d.Komjatszegi S et al. 1964 [57]F45EpiC+SCCn.d.n.d.autopsybasaln.d.n.d.n.d.Nosaka Y et al. 1979 [79]M46EpiC+SCCn.d.n.d.STRCPAn.d.died at 7 monthsn.d.Maffazoni D et al. 1986 [65]M45EpiC+SCCn.d.−nonebasaln.d.n.d.n.d.Ishimatsu T et al. 1988 [50]M40EpiC+SCCn.d.−noneCPAn.d.n.d.n.d.Mohanty V et al. 1996 [71]M20EpiC+SCCn.d.−noneposterior fossan.d.n.d.n.d.Ishikawa S et al. 2000 [49]M65EpiC+SCCn.d.−autopsyCPAn.d.n.d.n.d.Khan R et al. 2001 [53]M53EpiC+SCCn.d.−autopsyprepontinen.d.n.d.n.d.Shirabe T et al. 2003 [91]M49EpiCn.d.SCCbiopsybrainstemn.d.died at 24 monthsn.d.Kodama H et al. 2007 [56]M67EpiC2SCCSTRCPARTdied at 13 monthsn.d.Pagni F et al. 2007 [81]F65EpiC+SCCn.d.SCC (CSF)biopsypinealn.d.nonen.d.Ozuneiz C et al. 2017 [8]M64EpiC(neuroimage)276SCCNlateral ventriclen.d.3 monthsn.d.Michael L et al. 2005 [68]M45EpiC+SCCn.d.−STRposterior fossaRTdied immediatelyn.d.Nagata K et al. 2019 [74]F77SCC +(EC? )n.d.−STRCPARTn.d.n.d.Feng R et al. 2014 [33]M42EpiC+SCCn.d.−GTRCPART6 monthsn.d.Garcia C et al. 1981 [38]M61SCCn.d.EpiC+SCC (autopsy)biopsyCPARTdied at 6 monthsn.d.Fuse T et al. 1995 [36]F74n.d.n.d.−GTR or STRCPARTn.d.n.d.Uchino A et al. 1995 [99]M57EpiC+SCCn.d.−STRCPART4 monthsn.d.Park and Park et al. 2003 [82]M65EpiC+SCCn.d.−STRCPARTnonen.d.Guan L et al. 2004 [43]F42EpiC204−GTR or STRtemporal lobeRTn.d.n.d.Kim and Kim et al. 2008 [54]F72EpiC+SCCn.d.−STRCPART12 monthsn.d.Roh T et al. 2017 [86]F53EpiC+SCCn.d.−GTRCPARTn.d.n.d.Chen Z et al. 2019 [23]M43EpiC+SCCn.d.−STRCPART24 monthsAE1/3(+)Fereydonyan N et al. 2019 [34]30EpiC60EpiC+SCCGTRCPART24 monthsn.d.Gerges M et al. 2019 [40]F65EpiC+SCCn.d.−GTRpinealRT6 monthsn.d.Badat N et al. 2018 [19]70n.d.n.d.−NCPAn.d.n.d.n.d.Kadashev B et al. 2003 [51]F47EpiC+SCCn.d.−GTR or STRtemporal loben.d.n.d.n.d.Sawan B et al. 2000 [88]M66EpiC+SCCn.d.−autopsyprepontinen.d.n.d.n.d.Chourmouzi D et al. 2015 [25]F39EpiC+SCCn.d.−GTRCPAn.d.nonen.d.Seif B et al. 2017 [90]M83EpiC2SCCGTRCPAn.d.nonen.d.Alsadi H et al. 2025 [5]M59EpiC168SCC (CSF)n.d.CPAchemotherapydied at 2 monthsn.d.Agarwal S et al. 2007 [17]M45EpiC+SCCn.d.−Nposterior fossaRTlostn.d.Elsarraj H et al. 2025 [6]M61EpiC156SCC (CSF)STRCPAchemotherapyn.d.n.d.Michenet P et al. 1989 [69]M56EpiC192EpiC+SCCGTRn.d.n.d.n.d.n.d.Hoeffel C et al. 1997 [47]M43EpiC+SCCn.d.−Nparietal and occipital bonechemoradiationn.d.n.d.Raheja A et al. 2016 [85]F54EpiC+SCCn.d.−STRprepontinen.d.n.d.n.d.Raheja A et al. 2016 [85]F37EpiC+SCCn.d.−biopsyprepontinen.d.n.d.n.d.Mascarenhas A et al. 2017 [66]F35EpiC60EpiC+SCCSTRCPAn.d.n.d.n.d.Cuoco J et al. 2019 [2]M71EpiC480EpiC+SCCSTRCPARTnoneCK5/6(+)Radhakrishnan V et al. 1994 [84]M53EpiC372EpiC+SCCGTR or STRfrontaln.d.n.d.n.d.Song Z et al. 2024 [12]F47EpiC+SCCn.d.−GTRbasal ganglia and thalamuschemoradiationn.d.CK5/6(+), P63(+),β-catenin(+), MIB-1 40%Acciari N et al. 1993 [16]SCC+(EC? )n.d.−Nchiasmatic-parasellarn.d.n.d.n.d.Bretschneider T et al. 1999 [22]F71EpiC+SCCn.d.−STRoccipital boneRTdied at 13 monthsn.d.Eatz T et al. 2023 [31]F43n.d.n.d.n.d.n.d.CPAn.d.n.d.n.d.Kubokura T et al. 1986 [59]F60EpiC+SCCn.d.n.d.STRsuprasellar and temporaln.d.died at 6 daysn.d.Matsuno A et al. 1987 [67]M43EpiC7n.d.STRCPAchemoradiationn.d.n.d.Delangre T et al. 1992 [27]F72EpiC+SCCn.d.n.d.n.d.CPAn.d.n.d.n.d.Nawashiro H et al. 2001 [76]M46n.d.n.d.n.d.n.d.temporal loben.d.n.d.n.d.Hatem O et al. 2002 [45]M40n.d.n.d.n.d.n.d.frontotemporal prepontineRTn.d.n.d.Kwon S et al. 2019 [60]M71n.d.n.d.n.d.STRn.d.n.d.n.d.n.d.Ou A et al. 2018 [80]F71EpiC300SCCGTR or STRCPARTn.d.n.d.Suematsu Y et al. 2018 [94]M54EpiC24SCCGTR or STRCPAn.d.n.d.n.d.Monaco R et al. 2003 [10]M36EpiC+SCCn.d.−GTRposterior fossan.d.24 monthsAE1/3(+), MIB-1 80%Sun T et al. 2016 [13]F22EpiC+SCCn.d.SCCSTRCPARTreoperation at 19 months,CK5/6(+), MIB-1 60%died at 41 monthsSterner R et al. 2024 [93]F63EpiC6SCCGTR or STRorbitn.d.n.d.n.d.CPA, cerebellopontine angle; EpiC, epidermoid cyst; F, female; GTR, gross total resection; M, malen.d., not described; RT, radiotherapy; SCC, squamous cell carcinoma; STR, subtotal resection
In six cases, the MIB-1 labeling index was found to be high (range, 20–80%) [13, 67, 72, 90, 93, 101]. In the present case, consistent with previous reports, the MIB-1 index was 50.8%, suggesting a high proliferative potential of the tumor cells. Despite a lack of histological confirmation of EpiC during the clinical course of the present case, we assumed the tumor represented a malignant transformation from EpiC rather than SCC metastasis from an unknown primary cancer, as evidenced by serial MRI during long-term follow-up, especially the first 5 years of dormancy as shown in T2WI and DWI (Fig. 1a and b). Even during the most recent five years when radiological findings from T2WI and DWI changed, growth potential was not rapid, representing an obvious difference from the typical behavior of SCC metastasis.
Role of postoperative adjuvant therapy for SCC at recurrence (Table 3)
In cases of malignant transformation, the issue of whether to perform radiotherapy or chemotherapy in addition to surgery is important. However, no standard treatment strategy has been established. Among the 48 reported cases, 38 underwent radiotherapy, 4 underwent chemotherapy alone, and 6 received chemoradiotherapy. In addition, follow-up periods remain short and treatment regimens have not been standardized or clearly described in detail. In the present case, the contrast-enhanced lesion disappeared following local radiotherapy, suggesting that radiotherapy may be effective. Malignant transformation of EpiC is extremely rare, making a definitive algorithm for postoperative therapy difficult to establish. EpiC is recognized as a benign tumor and malignant transformation is rare, so long-term follow-up is essential for identifying malignant transformation through imaging and pathological evaluation.
Limitations
In the present case, whether the tumor consisted solely of EpiC in the initial stage was unclear, as no initial surgery was performed. In addition, pathological examination revealed only SCC, despite the intraoperative observation of a pearly tumor. Ultimately, malignant transformation was diagnosed based on the initial imaging and intraoperative findings. If pathological changes had been captured through multiple surgeries performed at the time of initial diagnosis and during malignant transformation, or if surgery had been performed immediately after malignant transformation was suspected and features of the transition from EpiC to SCC had been identified, the exact timing of malignant transformation might have been able to be determined. In addition, in the present case, only partial resection was performed, which may have contributed to the inability to detect EpiC components in the submitted specimens. Although no disease progression was observed for 4 months after radiotherapy, the period of follow-up for postoperative therapy remains short, similar to previous reports. Further accumulation of postoperative therapy cases and long-term follow-up are required to validate these observations.
Conclusions
We experienced malignant transformation of EpiC during the clinical course. Long-term follow-up is essential for identifying such changes, as malignant transformation typically requires an extended period. In particular, if high intensity on DWI disappears or a contrast-enhanced lesion appears, malignant transformation of EpiC should be considered. Postoperative radiotherapy may be effective for controlling residual tumor, but clear evidence remains lacking.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alsadi H, Dahlstrom K, Summers K et al (2025) Intracranial epidermoid cyst with malignant degeneration and leptomeningeal carcinomatosis: illustrative case. J Neurosurg Case Lessons 9. 10.3171/CASE 2473810.3171/CASE 24738 PMC 1179165239899849 · doi ↗ · pubmed ↗
- 2Chen Z, Araya M, Onishi H (2019) Proton beam therapy for malignant transformation of intracranial epidermoid cyst. BMJ Case Rep 12. 10.1136/bcr-2019-22938810.1136/bcr-2019-229388 PMC 666316731320371 · doi ↗ · pubmed ↗