Pregnancy after fertility preservation and multimodal therapy including intensity-modulated radiotherapy for recurrent vulvar cancer: A case report
Kosuke Murakami, Kiko Yamamoto, Takuya Uehara, Yukinori Matsuo, Noriomi Matsumura

TL;DR
A 36-year-old woman with recurrent vulvar cancer successfully preserved fertility through embryo cryopreservation and later achieved pregnancy despite undergoing radiotherapy.
Contribution
This case report demonstrates the potential for fertility preservation and partial uterine function retention after intensity-modulated radiotherapy in recurrent vulvar cancer.
Findings
Embryo cryopreservation before cancer treatment enabled subsequent pregnancy.
IMRT may reduce scatter radiation to the uterus, preserving partial uterine function.
Hormone replacement allowed endometrial regrowth after ovarian function loss.
Abstract
Advanced or recurrent vulvar cancer in women of reproductive age is extremely rare, and the effects of radiotherapy (RT) on uterine and ovarian function in such cases remain poorly understood. Here, we report the case of a 36-year-old woman with recurrent vulvar cancer after initial surgery. She strongly desired fertility preservation, so before undergoing resection of the recurrent lesion and inguinal lymphadenectomy, she underwent ovarian stimulation using a random-start progestin-primed ovarian stimulation (PPOS) protocol, and embryos were cryopreserved. Because of the high risk of recurrence, the patient underwent adjuvant intensity-modulated radiotherapy (IMRT) postoperatively. Three months after irradiation, ovarian function was lost; however, endometrial regrowth and withdrawal bleeding were observed with oral administration of norgestrel and ethinylestradiol. Despite significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1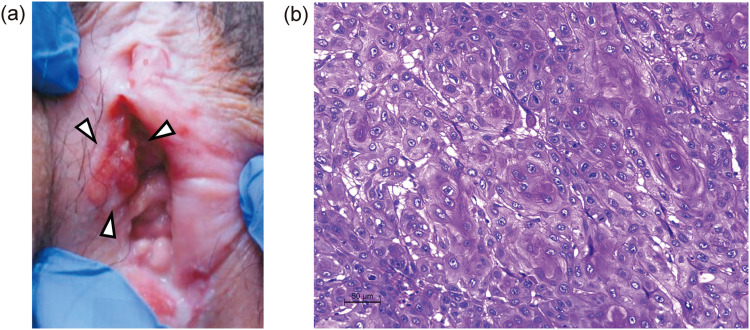 Figure 2
Figure 2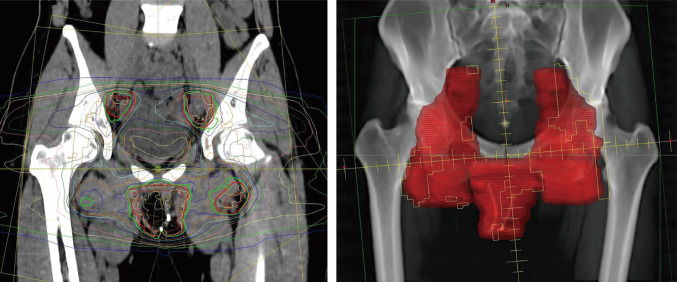 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Cancer Risks and Factors · Ovarian cancer diagnosis and treatment
Introduction
Vulvar cancer is a rare malignancy, accounting for approximately 5% of all gynecologic cancers [1]. However, the incidence of advanced or recurrent cases in women of reproductive age is on the rise [2]. For advanced vulvar cancer, standard treatment includes radical vulvectomy, and in cases with a high risk of recurrence, adjuvant radiotherapy (RT) may be added [1]. However, the impact of such treatment on uterine and ovarian function in reproductive-age women has not been fully elucidated.
With an increasing number of young women expected to survive long-term after cancer treatment, the effects of therapy on fertility have become a critical issue. Pelvic RT poses risks such as depletion of the primordial follicle pool and premature ovarian insufficiency [3]. In addition, impaired uterine blood flow can lead to endometrial atrophy and decreased uterine volume and elasticity, resulting in reduced fertility [3, 4]. Therefore, efforts are being made to minimize radiation exposure to reproductive organs in young female patients receiving RT. Technological advancements, including intensity-modulated RT (IMRT) and image-guided RT (IGRT), have enabled more precise control of the irradiation field and reduced unnecessary radiation to surrounding normal tissues [5, 6]. With these techniques, in cases of diseases that do not directly involve the uterus, such as vulvar, anal, or rectal cancer, it is theoretically possible to minimize scatter radiation to the uterus. However, there is a lack of clinical evidence on how much these methods contribute to preserving uterine function, and detailed evaluations from the perspective of fertility preservation remain scarce.
In this report, we present a rare case of recurrent vulvar cancer treated with multimodal therapy including surgery and IMRT. Although ovarian function was lost, endometrial proliferation was achieved with oral administration of norgestrel and ethinylestradiol, and pregnancy was successfully established by frozen-thawed embryo transfer.
Case report
The patient was a nulligravid, nulliparous woman. She was 147 cm tall and weighed 55 kg, with a body mass index (BMI) of 25.5 kg/m^2^. She had no notable medical history. At the age of 32, she noticed a 1.5 cm mass on her left labia majora. A biopsy confirmed vulvar squamous cell carcinoma (Fig. 1). She underwent wide local excision and left inguinal lymph node biopsy. Postoperative pathological diagnosis was International Federation of Gynecology and Obstetrics (FIGO) stage IA (pT1aN0M0) squamous cell carcinoma with negative margins, and no adjuvant therapy was given. She was followed up without recurrence.Fig. 1. Vulvar tumor at initial presentation. A 1.5 cm mass is observed on the left labia majora (white arrowhead)
At age 35, she got married and began standard infertility treatment six months later. However, at age 36, a recurrent vulvar mass was observed, which gradually enlarged (Fig. 2a). A biopsy confirmed recurrence of vulvar squamous cell carcinoma. At this time, the patient strongly desired fertility preservation, and ovarian stimulation using a progestin-primed ovarian stimulation (PPOS) protocol was initiated. Anti-Müllerian hormone (AMH) level was 5.22 ng/mL. Although a random-start stimulation protocol was initially considered, the patient’s menstrual period started just before treatment initiation, allowing conventional stimulation to begin on day 3 of menstruation. After 10 days of recombinant follicle-stimulating hormone (rFSH) 150 IU administration per day, follicular growth was observed, and ovulation was triggered using 5,000 IU of human chorionic gonadotropin (hCG). Transvaginal oocyte retrieval was performed 34 hours later, yielding 9 mature oocytes. Fertilization was achieved through conventional insemination, resulting in cryopreservation of two blastocysts and one morula.Fig. 2. Recurrent vulvar tumor. A. A mass is observed on the right labia (white arrowhead). B. Histopathological image of the resected tumor. Hematoxylin and eosin staining; scale bar: 50 µm
Subsequently, the patient underwent radical vulvectomy and bilateral inguinal lymphadenectomy for the recurrent lesion. Pathological examination again confirmed recurrent vulvar squamous cell carcinoma (Fig. 2b). Metastasis was found in the right inguinal lymph nodes, indicating a high risk of further recurrence. Adjuvant IMRT was administered. The irradiation field included the vulva, bilateral inguinal lymph nodes, and pelvic lymph node regions as the clinical target volume, adding set-up margins of 5.0 mm for the planning target volume (PTV), with a total dose of 50.4 Gy (1.8 Gy × 28 fractions) (Fig. 3). Four full arcs of volumetric modulated arc therapy technique were applied with 6 MV flattening filter-free photon beams using Halcyon linac (Varian Medical Systems Inc., Palo Alto, CA). The prescribed dose was normalized as 50.4 Gy to 50% of the PTV. To minimize radiation exposure to the uterus, the bladder was filled before each session. Dose–volume histogram (DVH) parameters for the uterus were evaluated using D_max_, D_mean_, V_14Gy_, and V_20Gy_. Dmax was defined as the maximum dose, and Dmean as the mean dose. V_14Gy_ and V_20Gy_ were defined as the volumes of the uterus receiving ≥14 Gy and ≥20 Gy, respectively. The D_max_, D_mean_, V_14Gy_, and V_20Gy_ of the uterus were 25.1 Gy, 5.9 Gy, 1.8 cc, and 0.1 cc, respectively. DVH parameters for the ovaries were evaluated using D_max_, D_mean_, V_5Gy_, and V_14Gy_, where V_5Gy_ was defined as the volume receiving ≥5 Gy. The D_max_, D_mean_, V_5Gy_, and V_14Gy_ of the ovaries were 6.7 Gy, 3.9 Gy, 1.3 cc, and 0 cc, respectively. Radiation-induced vulvitis occurred and was managed with topical steroids and petroleum jelly. Severe vaginal atrophy was also observed, and topical estrogen cream was applied.Fig. 3. Radiation plan using intensity-modulated radiotherapy. The irradiation fields included the vulva, bilateral inguinal lymph nodes, and pelvic lymph node areas
Three months after the completion of RT, hormonal assessment revealed serum estradiol below the detection limit (<10 pg/mL), FSH of 99.3 mIU/mL, and AMH below the detection limit (<0.1 ng/mL), indicating complete ovarian failure. Although uterine function was presumed impaired, oral administration of norgestrel and ethinylestradiol induced endometrial proliferation (up to 9.5 mm) and withdrawal bleeding. Despite severe vaginal and cervical atrophy, transcervical tubing was possible. Frozen-thawed embryo transfer was attempted during a hormone replacement cycle using estradiol patches (2.88 mg every other day). The first blastocyst transfer did not result in pregnancy, but the second attempt led to a confirmed intrauterine gestational sac (Fig. 4). Unfortunately, at 5 weeks of gestation, the patient was diagnosed with acute myeloid leukemia (AML). Although a causal link with RT was suspected, it remained unproven. Pregnancy could not be continued, and termination was performed at 6 weeks.Fig. 4. Intrauterine gestational sac
Discussion
This is an extremely rare case in which fertility preservation therapy was performed in a patient with recurrent vulvar cancer, and following IMRT, endometrial proliferation was achieved with oral norgestrel–ethinylestradiol administration, ultimately resulting in pregnancy through frozen-thawed embryo transfer. We reviewed previous reports of pregnancies occurring after RT for non-uterine pelvic malignancies such as rectal, anal, or vulvar cancer. Case reports extracted using the PubMed search formula ((rectal cancer) OR (anal cancer) OR (vulvar cancer)) AND ((pregnancy) OR (fertility preservation)) AND ((radiation) OR (radiotherapy)) are summarized in Table 1 [7–17]. While three cases of pregnancy after RT for vulvar cancer have been reported previously [7, 9, 13], to our knowledge, this appears to be the first reported case of recurrent vulvar cancer treated with RT following fertility preservation therapy.Table 1. Pregnancy after pelvic radiotherapy in patients with vulvar, rectal, and anal cancersYearCancerAge at RTType of RTRT field and doseEffective dose to the uterusAge at pregnancy Spontaneous or ARTPregnancy outcomeReference12002Vulvar19EBRTRight hemipelvis 45 Gy & right inguinal 10.8 GyNA25 SpontaneousPreterm birth at 29 weeks[7]22007Rectum24EBRTTwo lateral pelvis 50.4 GyNA26 SpontaneousIntrauterine fetal death at 21 weeks[8]32010Vulvar33EBRT & brachytherapyPerineum brachytherapy 20 Gy & EBRT 50 GyNA35 SpontaneousNA[9]42012Anal25EBRTWhole pelvis 50 Gy30 Gy (cervix; 50 Gy)26 SpontaneousNA[10]52016Rectum33EBRTPrimary tumor 50 Gy & pelvic lymph nodes 40 GyNA36 SpontaneousTwin, preterm, one baby died during delivery[11]62016Anal36IMRTPelvis 59.4 GyNA39ARTCesarean section at term[12]72016Vulvar17EBRTVulvar and inguinal 45 GyNA26SpontaneousCesarean section at term[13]82017Rectum28EBRTRectum 30.6 Gy22.5 Gy29SpontaneousDelivery at term[14]92020Rectum28EBRTNANA30SpontaneousCesarean section at 32 weeks[15]102021Rectum32EBRT & brachytherapyWhole pelvis EBRT 48.6 Gy & anal canal brachytherapy 10 Gy16 Gy (cervix; 35 Gy)42ART (donation)Twin, cesarean section at term[16]112024Rectum26IMRTPrimary tumor 50 Gy & pelvic lymph nodes 45 GyUterine fundus; 20-25 Gy, cervix; 45–47.5 Gy33ARTCesarean section at term[17]12 Our case Vulvar (recurrent)36IMRTVulvar, inguinal and pelvic lymph nodes 50.4 GyNA36ARTArtificial abortion at 6 weeks −RT; radiotherapy, EBRT; external beam radiotherapy, IMRT; intensity modulated radiotherapy, ART; assisted reproductive technology, NA; not available
Regarding uterine function after RT, pelvic irradiation can lead to fibrosis of the myometrium, reduced uterine volume and blood flow, and loss of the basal endometrium [3, 4]. However, Barnhill et al. reported that 7 out of 16 patients who received RT for cervical cancer exhibited endometrial proliferation following estrogen therapy [18]. De Hullu et al. observed hematometra in 2 of 4 young women who had received approximately 80 Gy for cervical cancer, suggesting partial preservation of endometrial function [19]. Furthermore, Rozen et al. reported a case of rectal cancer in which the endometrium became markedly thinned and unresponsive after RT, but thickened to a transferable level following high-dose estrogen therapy, leading to successful pregnancy and delivery [17].
These findings suggest that the endometrium is not always completely destroyed by RT. If partially functional endometrial tissue remains, regeneration may be stimulated through exogenous hormone therapy, even when spontaneous regrowth is limited. However, even if pregnancy is achieved after RT, the risk of obstetric complications due to impaired uterine function remains high, and careful perinatal management in a high-level medical facility is essential [20, 21].
In malignancies that do not directly involve the uterus, such as rectal, anal, or vulvar cancers, it is technically feasible to spare the uterus from radiation exposure (Table 1). In recent years, the introduction of IMRT has enabled precise control of the irradiation field and substantial reduction of scatter radiation to surrounding normal tissues [5]. Lee et al. reported a case in which successful pregnancy was achieved by minimizing radiation exposure to the uterine corpus during RT for cervical cancer [22]. Milgrom et al. noted that although complete avoidance of scatter radiation to the uterus is challenging, dose optimization and shaping can enhance the possibility of preserving uterine function [23]. Moreover, bladder filling during RT is commonly used to shift the uterus ventrally and out of the irradiation field [24], as was also performed in this case.
As a more challenging approach, uterine transposition prior to RT for non-gynecologic malignancies has been reported, and in one study, natural conception and live birth were achieved in 2 of 8 cases after repositioning the uterus post-treatment [25]. However, the feasibility of this technique for vulvar cancer remains unclear. There have been reports of successful natural pregnancies after ovarian transposition prior to RT [11, 15]. However, in the present case, ovarian transposition was not performed because it was anticipated that sufficient protection of the ovaries from scatter radiation would be difficult to achieve, and the surgical approach would have been more invasive due to a different operative field. Since scatter radiation to the ovaries cannot be fully predicted even with IMRT, embryo cryopreservation prior to treatment was considered the most practical and effective fertility preservation strategy.
The timing of embryo transfer should be carefully considered in light of the risk of disease recurrence. Although clear evidence regarding the second recurrence risk of vulvar cancer is lacking, previous studies have reported cumulative incidences of local recurrence after primary treatment of 5.9% at 2 years and 14.7% at 5 years [26]. Taking these data into account, together with the age-related decline in fertility, early embryo transfer after completion of treatment may be reasonable. In the present case, however, AML developed shortly after embryo transfer. Radiation-induced leukemia is recognized as a late complication of radiotherapy, but its incidence is very low. Large cohort studies of pelvic radiotherapy have shown a 72% increase in post-treatment leukemia; however, the peak incidence usually occurs 5–10 years after exposure, and the cumulative incidence remains 0.0022% [27]. In this case, AML occurred only a few months after completion of IMRT, which does not match the typical latency of radiation-induced leukemia. Therefore, while a causal relationship with radiotherapy cannot be excluded entirely, the temporal course suggests that the association is unclear and could not have been predicted.
In conclusion, this case provides a valuable clinical experience in which partial preservation of uterine function and successful pregnancy were achieved through technical modifications in IMRT and the use of hormone therapy. Given the nature of the disease, fertility preservation is often considered to be unfeasible. However, with thorough pre-treatment counseling and appropriate strategy, the possibility of preserving fertility can be maximized.