Sarcomatoid carcinoma of the common bile duct: A case report and review of the literature
Sedat Alp Pinar, Mari-Claire McGuigan, Fraser Duthie, Abinaya Ezhil, David Holroyd, Nigel B. Jamieson

TL;DR
This case report describes a rare type of bile duct cancer called sarcomatoid carcinoma and highlights the diagnostic and treatment challenges associated with it.
Contribution
The paper presents a new case of sarcomatoid carcinoma of the common bile duct and reviews the limited existing literature on this rare malignancy.
Findings
The patient was diagnosed with sarcomatoid carcinoma after histopathology and immunohistochemical staining confirmed epithelial markers.
The patient underwent pancreaticoduodenectomy and remained recurrence-free for 16 months without adjuvant chemotherapy.
The paper emphasizes the importance of tissue confirmation and immunohistochemical analysis for accurate diagnosis.
Abstract
Sarcomatoid carcinoma of the common bile duct is an exceptionally rare malignancy, with only eight cases previously reported in the English literature. We present the case of a 72-year-old Caucasian male who presented with obstructive jaundice and abnormal liver function tests, but without elevated tumour markers CA19-9 and CEA. Imaging with CT and MRCP revealed a polypoid mass in the common bile duct, and two ERCP attempts were unsuccessful. The patient underwent a pancreaticoduodenectomy without adjuvant chemotherapy and has remained recurrence-free for 16 months. Histopathology revealed sarcomatoid spindle cells negative for the expression of sarcomatous markers but positive for epithelial markers CAM5.2 and AE1/3, as well as MNF focally, along with chronic cholecystitis. Sarcomatoid carcinoma is a rare and challenging diagnosis that requires tissue confirmation and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2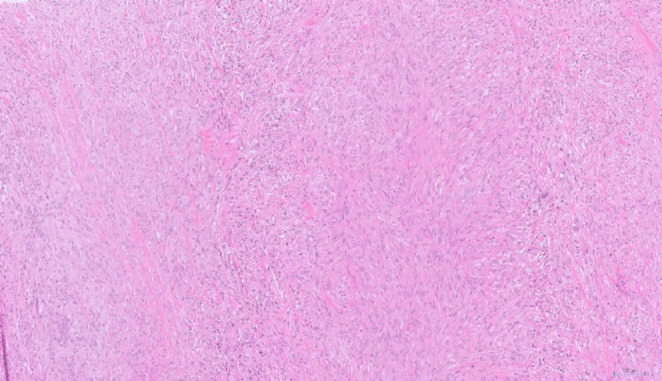 Figure 3
Figure 3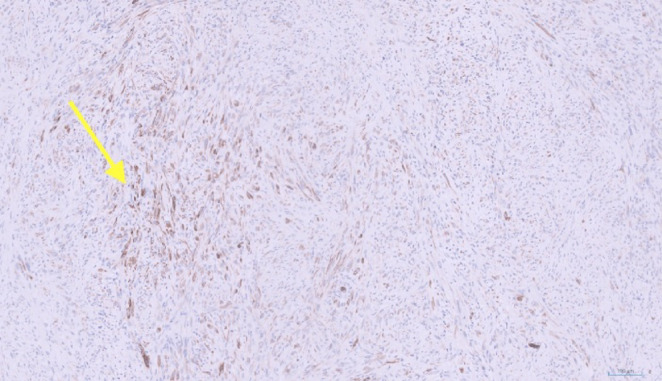 Figure 4
Figure 4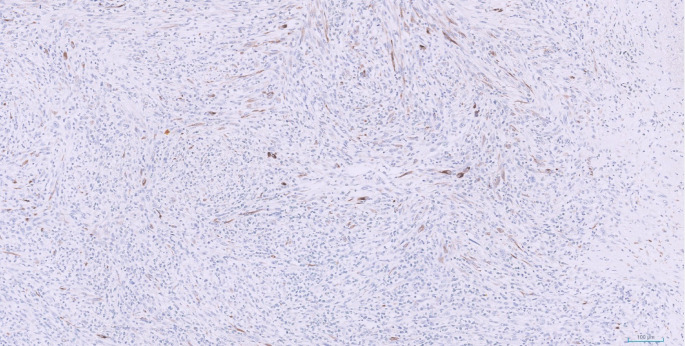 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Metastasis and carcinoma case studies · IgG4-Related and Inflammatory Diseases
Background
Sarcomatoid carcinoma is an exceptionally rare and aggressive tumour affecting the hepato-pancreato-biliary system, characterized by the presence of giant cells/spindle cells with sarcomatous morphology with an epithelial origin [1, 2].
Sarcomatoid carcinoma has been reported in the liver [3], gallbladder [4], pancreas [5], and ampulla of Vater [6]. However, occurrences in the common bile duct are exceptionally rare. This rarity poses a significant challenge in studying these tumours and establishing a standardized treatment protocol.
The origin of sarcomatoid carcinoma is not well understood, though three main theories have been proposed [6]. According to Kench and Frommer (1997), sarcomatoid carcinoma may develop through a metaplastic transformation of carcinomatous cells into sarcomatous cells [6]. Another possibility is that it arises from a single multipotent reserve cell that has the ability to differentiate in various ways [6]. A third theory suggests that sarcomatoid carcinoma results from the simultaneous malignant growth of both epithelial and stromal cells [6].
While these tumours are generally regarded as highly aggressive with a tendency for high recurrence and poor survival, the limited literature provides mixed survival outcomes, underscoring the need for more comprehensive research and case studies [7]. We believe the aggressive nature of these tumours may be associated with a high proportion of metastatic disease at the time of diagnosis, contributing to very low rates of pancreaticoduodenectomy resection, and therefore low rates of tissue diagnosis.
Despite its aggressive nature, there remains a gap in the understanding of sarcomatoid carcinoma of the common bile duct with only a few documented cases. There is a lack of robust data on its clinical presentation, optimal management strategies, and prognostic factors, highlighting the need for additional case reports and future studies.
The aim of this case report is to provide insight into the aggressive behavior of sarcomatoid carcinomas and to emphasize the critical importance of early diagnosis and timely surgical management. Our case specifically highlights the importance of the lack of elevated tumour markers such as CA19-9 and CEA which may initially lead clinicians away from considering malignancy. Additionally, it highlights the necessity of advancing molecular characterization of these rare tumours to improve diagnostic precision and inform the development of more effective, targeted therapeutic strategies.
Case presentation
A 72-year-old Caucasian male was admitted to the general surgery ward as an emergency to a district general hospital, presenting with four weeks of painless obstructive jaundice. The patient has previously been healthy with no diagnosed health conditions, no routine medications, no relevant family history and had not previously undergone any previous operations.
A thoraco-abdominopelvic computed tomography (CT) scan revealed a 15 mm filling defect within the distal common bile duct, accompanied by dilatation of both intrahepatic and extrahepatic biliary ducts (Fig. 1). There was no pancreatic duct dilation or evidence of a pancreatic mass. No other significant abnormalities were found on the CT scan.
Magnetic resonance cholangiopancreatography (MRCP) confirmed biliary duct dilatation, revealing a solid mass measuring 19 mm longitudinally and 13 mm transversely, raising suspicion for malignancy (Fig. 2). An endoscopic retrograde cholangiopancreatography (ERCP) was attempted twice but was unsuccessful due to the inability to cannulate the common bile duct due to tumour involvement. Following this, the patient was transferred to our unit at Glasgow Royal Infirmary, after 10 days from initial admission at the district general hospital.
Fig. 1. Coronal portal venous phase CT showing abrupt truncation of the distal CBD with 2.4cm stricture/intraluminal soft tissue which extends to the level of the ampulla, as indicated by the arrow. Associated moderate upstream intra and extrahepatic biliary tree dilatation is present
Fig. 2. Coronal T2 SPACE MRI confirming distal CBD stricture as indicated by the arrow, with upstream biliary tree dilatation. Normal calibre main pancreatic duct suggests the mass originates within CBD rather than from the pancreas or ampulla
Laboratory tests on admission revealed significant abnormalities: alkaline phosphatase was elevated at 215 U/L, total bilirubin was markedly increased at 439 µmol/L, AST was 140 U/L, ALT was 164 U/L, and albumin was low at 27 g/L. Serum levels of carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9 were within the reference range. The amylase level was mildly elevated at 157 U/L, and C-reactive protein (CRP) was raised at 39 mg/L. These results are presented in Table 1.
Table 1. Laboratory and tumour marker results obtained upon the patient’s admission to our unit, prior to stentingTestResultNormal RangeAbnormalityAlkaline Phosphatase215 U/L40–150 U/LElevatedTotal Bilirubin439 µmol/L< 21 µmol/LMarkedly ElevatedAST140 U/L8–33 U/LElevatedALT164 U/L4–36 U/LElevatedAlbumin27 g/L35–55 g/LLowCarcinoembryonic Antigen (CEA)1.9 ug/L0.0–5.0.0ug/LWithin Normal RangeCarbohydrate Antigen (CA) 19-916 kU/L< 37 kU/LWithin Normal RangeAmylase157 U/L40–140 U/LMildly ElevatedC-Reactive Protein (CRP)39 mg/L< 10 mg/LElevated
Consequently, an endoscopic ultrasound-guided stenting of the bile duct was performed using a lumen opposing selfexpanding Metal Stent (SEMS), resulting in the complete resolution of bilirubin levels and a marked improvement in albumin levels to 33 g/L. We conclude that the improvement in serum albumin levels following stenting is attributable to the resolution of the temporary acute phase response caused by obstruction by the polypoid mass, which had previously contributed to the mildly low albumin levels. The patient clinically improved following stenting and was discharged from our unit 6 days after admission. He did not develop renal impairment, coagulopathy, or change in neurological status throughout his admission.
Magnetic Resonance Imaging (MRI) of the liver showed no evidence of metastasis. Given the high suspicion of malignancy and without tissue diagnosis, the patient underwent a classic Whipple resection (pancreaticoduodenectomy), 6 weeks post-discharge of his acute admission. During the operation, no metastasis was identified, but extensive inflammation of the portal structures and intrahepatic biliary tree stones were noted. The surgery had proceeded without the use of neoadjuvant chemotherapy or radiotherapy following multi-disciplinary team (MDT) decision, as the tumour was perceived resectable, and the patient was deemed fit and healthy with no comorbidities.
Pathological evaluation of the specimen demonstrated a Whipple pancreaticoduodenectomy specimen comprising stomach (40 mm along the greater curvature and 30 mm along the lesser curvature), small bowel (190 mm), pancreatic head (100 × 55 × 20 mm), attached common bile duct (40 mm), and cystic duct (25 mm). A separate gallbladder measuring 75 × 30 × 30 mm and omentum measuring 330 × 95 × 15 mm were also submitted.
On sectioning, a pale tumor was identified centered in the distal common bile duct, measuring 34 × 10 × 25 mm, with focal extension into the pancreas. A metallic lumen stent was present within the proximal common bile duct. The tumor exhibited a nodular configuration with solid architecture, demonstrating exophytic growth into the bile duct lumen and extension into the bile duct wall to a depth of 7.4 mm. Gross photographs of the resected specimen were unavailable due to institutional archiving limitations.
Histological examination revealed large, pleomorphic, spindle-shaped cells, along with angulated glands lined by biliary epithelium, exhibiting nuclear enlargement and prominent nucleoli (Fig. 3). Distinguishing between areas of glandular differentiation and entrapped background epithelium proved challenging. Specimen confirmed an R0 resection. A total of 18 regional lymph nodes were retrieved and histologically examined, including a separately submitted station 8 A lymph node. No metastatic carcinoma was identified in any of the examined nodes (0/18), corresponding to pN0 disease.
Fig. 3. This micrograph demonstrates a tumour predominantly composed of spindle cells with pleomorphic hyperchromatic nuclei. The architecture indicates sarcomatoid differentiation, with regions showing ambiguous glandular structures that are challenging to distinguish from entrapped background epithelium
Immunohistochemical staining showed patchy expression of AE1/3 (Fig. 4) and CAM5.2 (Fig. 5), with focal cytokeratin MNF16 positivity, while all other markers; including CD34, CD56, Desmin, DOG1, MyoD1, S100, smooth muscle actin (SMA), STAT6, synaptophysin, anaplastic lymphoma kinase (ALK), CD1a, CD68, and langerin were negative.
Fig. 4. Immunohistochemical staining for AE1/3 demonstrates expression of the gene by spindle cells, confirming epithelial origin. The arrow points at a group of spindle cells that show strong expression of AE1/3
Fig. 5. Immunohistochemical staining for CAM 5.2 demonstrates expression of the gene by spindle cells, confirming epithelial origin
The extended immunohistochemical panel was employed to exclude important differential diagnoses. Negative ALK staining ruled out inflammatory myofibroblastic tumor [8], while STAT6 negativity excluded solitary fibrous tumor [9]. The absence of CD1a and langerin expression argued against histiocytic or dendritic cell neoplasms [10, 11], and negative lymphoid markers excluded lymphoma. Retained epithelial marker expression, including AE1/3 and CAM5.2, in combination with the histomorphological features, supported the diagnosis of sarcomatoid carcinoma. The lack of sarcomatous markers on staining directed us towards excluding carcinosarcoma as a diagnosis. The immunohistochemistry staining results are shown in Table 2.
Table 2. Immunohistochemical (IHC) staining profile of the resected specimen, summarising the expression of various markers, including cytokeratins, mesenchymal markers, neural markers, and other lineage-specific markers, detailed along with the corresponding antibody clone, manufacturer, heat-induced epitope retrieval (HIER) method, and dilution usedMarker (Kit/Company)ExpressionAntibodyCloneManufacturerHIERDilutionAE1/3Positive (Patchy)NCL-L-AE1/AE3-601AE1/AE3LEICAER2(20)1:200CAM5.2Positive (Patchy)452 M-98CAM5.2CELL MARQUEER1(20)RTUCytokeratin MNF16Positive (Focal)M0821MNF-116DAKOER2(20)1:400CD34NegativeNCL-L-ENDQBEN10LEICAER1(20)1:50CD56NegativeNCL-L-CD56-504504LEICAER2(20)1:75DesminNegativeNCL-L-DES-DER11DE-R-11LEICAE1(10)1:500DOG1NegativeNCL-L-DOG-1K9LEICAER2(20)1:100MyoD1NegativeM35125.8 ADAKOER2(20)1:25S100NegativeNCL-L-S100-167EP32LEICAER2(20)1:800SMANegativePA0943ASM-1LEICAER2(5)RTUSTAT6NegativeSC-374,021D-1SANTA CRUZER2(20)1:800SynaptophysinNegativeM7315DAK-SYNAPDAKOER1(20)1:100ALKNegativeNCL-L-ALK5A4LEICAER1(20)1:100CD1aNegativeNCL-L-CD1A-235MTB1LEICAER2(20)1:40CD68NegativeM0876PGM1DAKOER2(20)1:200LangerinNegativeNCL-L-LANGERINPOLYLEICAER2(20)1:200Key- ALK: anaplastic lymphoma kinase; DOG: discovered on gastrointestinal stromal tumour; SMA: Smooth Muscle Actin
The patient was diagnosed with Grade 3 sarcomatoid carcinoma, reflecting poor histologic differentiation, and stage T2 according to the TNM staging system of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC), 8th edition, for extrahepatic cholangiocarcinoma [12]. Chronic cholecystitis was observed in the gallbladder, along with a focal pancreatic intraepithelial neoplasia in the background pancreas.
The patient experienced no significant postoperative complications and was discharged 18 days post-surgery. As of the 16-month follow-up, there has been no recurrence of the disease, with the patient having returned to normal activities.
Discussion
For our article, we performed a targeted literature review. To refine our approach, we utilized key references from two review papers: Lee et al. (2016) [13] and incorporated more recent articles from Yao et al. (2023) [14]. Although these articles were describing cases of carcinosarcoma, they included cases of sarcomatoid carcinoma in their reviews; we suspect due to their clinical and prognostic similarity. From these articles, we excluded fourteen specific papers: two were not available in English, one focused on sarcomatoid carcinoma arising from the intrahepatic bile duct, one was a case of sarcomatoid carcinoma of the intrapancreatic duct, and ten were carcinosarcomas. The previous eight cases of common bile duct sarcomatoid carcinoma we identified are presented in Table 3.
Table 3. Past cases of sarcomatoid carcinoma of the common bile duct described in the literature, including patient details, tumour characteristics, treatments, and outcomesAuthor (year) (country)Gender/agePresentationInvestigation/tumour markersGross/sizeSurgery(C)RTPathologyIHC- stainPrevious HPB disease/interventionPrognosisYoon et al. (2004) (Korea) [15]Male, 78Abdominal pain and obstructive jaundiceCT, PTCInfiltrative, 40 mmPDNot usedBiphasic pattern of carcinomatous and sarcomatous components merging into anotherPositive: CEA; Cytokeratin; NSE; PCNA; p53; SMA; VimentinNegative: Bcl-2; Chromogrnin; Desmin; HMB45; Ki-67; Neurofilament; Synaptophysin; S100None reportedDied at 5 days post-operatively due to cardiac complicationsJang et al. (2005) (Korea) [16]Female, 68Abdominal pain, anorexia, and weight lossCT, EUS. Raised CA19-9. CEA and AFP within reference rangePolypoidal, 35 mmPDNot usedBiphasic pattern of predominantly sarcomatous and focally carcinomatous componentsPositive: CEA; Cytokeratin; VimentinNegative: C-kit; Desmin; Myoglobin; S100; SMANone reportedAlive and “doing well” at 1 year post-operativelyZhang et al. (2017) (China) [17]Female, 51Abdominal pain, obstructive jaundice, and weight lossCT, EUSInfiltrative, 38 mmPD3 cycles of Cisplatin and Gemcitabine chemotherapyBiphasic pattern of carcinomatous and sarcomatous components and necrotic regionsPositive: AE1/AE3; CEA; CK18; CK19; CK7; VimentinNegative: Desmin; Myoglobin; SMA; S100Chronic hepatitis B3 years disease-freeKim et al. (2019) (Korea) [18]Female, 65Jaundice and abdominal painCT, ERCP, raised CA19-9. CEA and AFP within reference rangeInfiltrative, 35 mmPDNot usedBiphasic pattern of predominantly sarcomatous and focally carcinomatous componentsPositive: Pan-cytokeratin; vimentinNegative: Desmin; SMANone reportedDied at 23 days post-operatively due to hepatic failure secondary to metastasisChan et al. (2023) (Canada) [19]Female, 70s (unspecified)Painless jaundice, decreased appetite, and fatigueCT, MRCP/ERCPNa, 47 mmPDNot usedBiphasic pattern of carcinomatous and sarcomatous components as well as squamous differentiation and sarcomatoid malignant peripheral nerve sheath tumour like areasPositive: AE1/AE3; Calretinin; CD34; CD117; CK5; CK8/18; EMA; p63; synaptophysin; VimentinNegative: ALK5A4; CDX2; CK7; CK20; CK19; Claudin; DOG; H3K27me3; MDM2; SOX10; S100; WT1Open cholecystectomyDied at 14 weeks post-operatively from perforated viscus, gastroduodenal leak and diffuse bowel ischaemiaMarques et al. (2023) (Portugal) [20]Male, 79Abdominal discomfort and obstructive jaundiceCT, MRCP, raised CA 19-9, CEA within reference rangeInfiltrative, 12 mmPDNot usedBiphasic pattern of diffuse sheets of poorly differentiated carcinomatoid and sarcomatous componentsPositive: CK7None reported2 years disease freeNagata et al. (2024) (Japan) [21]Male, 72Obstructive jaundiceEUS, CT, MRI, ERCP, CEA and CA19-9 within reference rangeInfiltrative, 32 mmPDNot usedBiphasic patten of sarcomatous and carcinomatous components, with a focus of adenocarcinoma near the CBD lumen. Slight infiltration into the pancreatic parenchyma, ki-67 index exceeded 80%Positive: AE1/AE3; CAM 5.2; CK19; VimentinNegative: CD34; Desmin; Myoglobin; S100; SMANone reportedIntra-abdominal lymph node recurrence at 2 months, hepatic metastasis at 3 months; died at 7 monthsYao et al. (2024) (China) [22]Male, 70Obstructive jaundiceCT, raised CA19-9, raised CEANa, 10 mmPDCarelizumab immunotherapy with 6 cycles of Gemcitabine and CisplatinBiphasic pattern with predominant moderately differentiated adenocarcinoma component and some sarcomatous regionsPositive: CKpan; SMARCA4; VimentinNegative: MyoD1 antibody; Myogenin; SMARCB1None reportedAlive at 6 months post-operativelyKey- AFP: Alpha-fetoprotein; CDX: caudal type homeobox; DOG: discovered on gastrointestinal stromal tumor EMA: Epithelial Membrane Antigen; EUS: Endoscopic Ultrasound; MDM: mouse double minute; NSE: Neuron-Specific Enolase; PCNA: Proliferating cell nuclear antigen; PD: Pancreaticoduodenectomy; PTC: Percutaneous Transhepatic Cholangiography; SMA: Smooth Muscle Actin; SOX: SRY-related HMG-box; WT1: Wilms tumour gene
To ensure adequate literature saturation, we performed a PubMed search using the term “sarcomatoid carcinoma bile duct”; identifying Nagata et al. (2024) [21] and Yao et al. (2024) [22] as the only relevant recent publications, as included in our table. The remaining results predominantly covered pancreatic and gallbladder cases.
Carcinosarcomas were excluded from our review because they are pathologically distinct from sarcomatoid carcinoma. Sarcomatoid carcinoma is a malignant epithelial tumor exhibiting sarcomatoid (spindle cell) features while retaining epithelial marker expression (e.g., AE1/3, CAM5.2, MNF16). In contrast, carcinosarcoma is a biphasic malignant neoplasm composed of both epithelial (carcinomatous) and mesenchymal (sarcomatous) components. As such, sarcomatoid carcinoma of the bile ducts is a rare subtype of cholangiocarcinoma that exhibits mesenchymal molecular and histopathological features.
Incorporating our case into the existing literature, sarcomatoid carcinoma of the common bile duct appears to have an even distribution between genders, with no clear sex predilection; as 55.6% of reported cases have occurred in males. All described cases involve adults, with the youngest patient reported at 51 years and the oldest at 79 years. Notably, 88.9% of cases have been observed in patients over the age of 65. Additionally, 66.7% of cases originated from Asia. We suggest that this is more indicative of variations in surgical and academic practices rather than a true difference in prevalence [23]. The extremely limited number of reported cases underscores the rarity of this entity and highlights the difficulty in establishing definitive epidemiologic patterns.
Additionally, all the cases, including ours, tested positive for epithelial markers AE1/3 and vimentin when stained, highlighting the value of using these stains for tumours that exhibit sarcomatoid features in histology. Moreover, pancreatoduodenectomy was the primary treatment approach in all cases, with only 22.2% incorporating adjuvant chemotherapy. As such, the MDT, taking the patient’s wishes into account, felt that the evidence base for adjuvant chemotherapy was lacking.
Based on the relevant literature, historically, the primary treatment approach for this condition has been surgical resection, either with or without (neo)adjuvant chemoradiotherapy. Reported disease-free survival (DFS) times have shown significant variability, ranging from as short as 23 days post-operatively [18] to over 3 years, with no follow-up beyond that point [17].
Evidence from gallbladder sarcomatoid carcinoma may provide insight into its potential relevance for common bile duct pathology. A study conducted at Sichuan University reviewed five cases of advanced gallbladder sarcomatoid carcinoma (stage III or higher) treated over a 20-year period [24]. Among these patients, the longest survival was observed in the one who underwent adjuvant chemotherapy after surgery, with an overall survival of 15 months and 12 months without disease progression [24]. In contrast, the remaining patients, who did not receive chemotherapy, had a maximum survival of only 2.6 months [24]. This highlights the importance of reporting additional cases of this exceedingly rare malignancy with the aim of better characterising patterns of (neo)adjuvant therapy use and associated outcomes.
In addition to contributing to the limited literature on sarcomatoid carcinoma of the common bile duct, our case also illustrates the limitations of ERCP in achieving a tissue diagnosis of malignancy. Our case is a common example of failure to achieve tissue diagnosis following ERCP due to the narrowing of the bile duct, which accounts for the very low sensitivity of both cytological brush (45%) and forceps biopsy (67%) [25, 26]. In such situations, endoscopic ultrasound-guided biliary drainage has emerged as a minimally invasive alternative with high technical and clinical success rates, and was therefore selected in this case [27].
Lastly, we acknowledge that the extreme rarity of sarcomatoid carcinoma of the common bile duct and the narrative nature of our review represent significant limitations of this study, restricting the ability to draw robust conclusions regarding prognosis and optimal management. Further accumulation of cases and long-term follow-up are required to better understand the behavior and outcomes of this tumor type.
Conclusion
Sarcomatoid carcinoma of the common bile duct is an exceptionally rare and aggressive malignancy that poses significant diagnostic and therapeutic challenges. Accurate diagnosis depends on careful histopathological assessment supported by immunohistochemical confirmation of epithelial differentiation. Surgical resection remains the cornerstone of management for localized disease and offers the best opportunity for disease control. However, due to the extreme rarity of this entity, prognostic factors and the role of (neo)adjuvant therapy remain poorly defined. The limited number of reported cases demonstrates considerable variability in clinical outcomes, underscoring the need for continued case reporting, longer follow-up, and collaborative efforts to better characterize disease behavior and guide future management strategies.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chan R et al (2023) Sarcomatoid carcinoma of the common bile duct presenting as painless jaundice. BMJ Case Rep, 16(11)10.1136/bcr-2023-257167 PMC 1064972037945274 · doi ↗ · pubmed ↗
- 2Navaneethan U et al (2015) Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: a systematic review. Gastrointest Endosc, 82(4): p. 608 – 14.e 2.10.1016/j.gie.2015.04.030PMC 482603226071061 · doi ↗ · pubmed ↗