Resection of the entire first rib for a malignant tumor via the transclavicular approach: a case report and literature review
Zhiqing Zhao, Xinli Sun, Bing Wang, Taiqiang Yan

TL;DR
A rare case of a malignant tumor in the first rib was successfully removed using a transclavicular surgical approach, offering a new method for similar challenging procedures.
Contribution
The paper presents a novel transclavicular surgical approach for complete resection of first rib tumors with neurovascular protection.
Findings
The transclavicular approach enabled safe and complete resection of the first rib tumor.
The patient experienced no neurological deficits and had symptom resolution post-surgery.
Histopathology confirmed the tumor was lymphoma.
Abstract
Malignant tumors of the first rib are extremely rare. Resection of the entire first rib is surgically challenging and requires an ingenious approach due to the complex anatomical characteristics. Currently, there is no standardized surgical approach. We herein report a case requiring resection of the entire first rib for a malignant tumor via the transclavicular approach and review relevant literature. A 43-year-old Chinese male suffered from right-sided neck and back pain for 1 month. Imaging studies (chest computed tomography, magnetic resonance imaging, and positron emission tomography-computed tomography) revealed an osteolytic lesion with pathological fracture in the right first rib, suggestive of malignancy. Due to the lesion's proximity to critical neurovascular structures, percutaneous biopsy was not feasible. The patient underwent en bloc resection of the entire first rib via…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
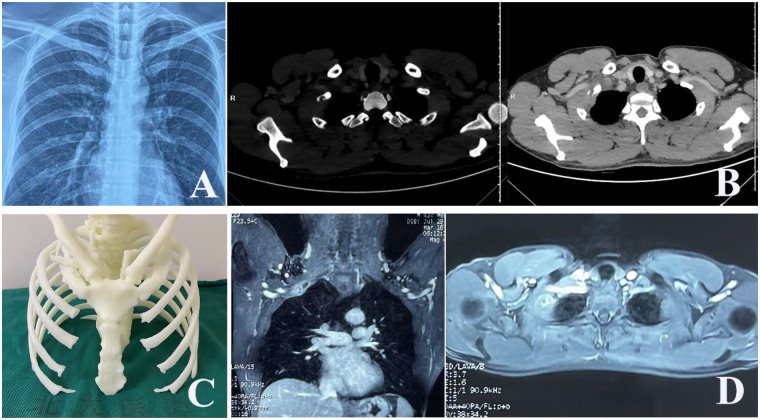 Figure 1
Figure 1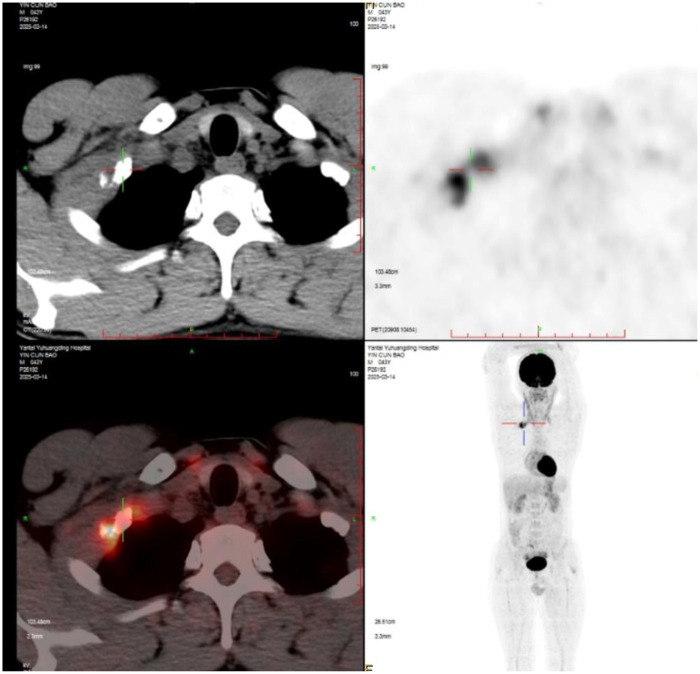 Figure 2
Figure 2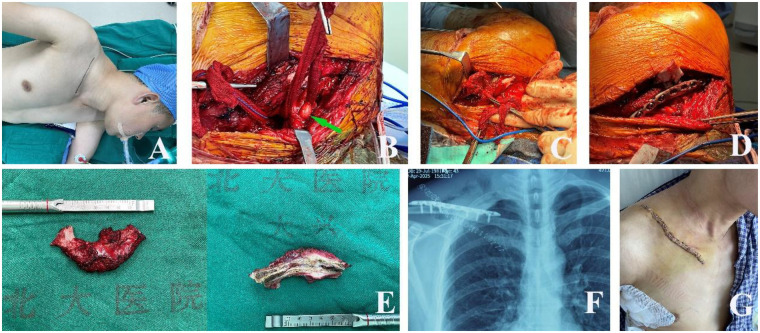 Figure 3
Figure 3| Author(s), year | Sex | Age | Tumor | Approach | Entire rib resection | Complication |
|---|---|---|---|---|---|---|
| Yeow and Hsieh, 2001 ( | 50 | F | Hemangioma | Transaxillary, infraclavicular, and supraclavicular approaches | No | Subclavian vessels compressed by hematoma formation |
| Cheng et al., 2007 ( | 21 | F | Aneurysmal bone cyst | Transmanubrial approach | No | None |
| 42 | M | Aneurysmal bone cyst | Transmanubrial approach | None | ||
| Masahiro Kitada et al, 2009 ( | 56 | M | Chondrosarcoma | Anterior approach (severing the clavicle), thoracoscope, and thoracotomy | No | None |
| O’Brien et al., 2010 ( | 12 | F | Osteochondroma | Supraclavicular and infraclavicular approach | No | Acute thrombosis of the subclavian vein |
| Kemp et al., 2012 ( | 41 | F | Fibrous dysplasia | Transaxillary approach and posterolateral thoracotomy | No | None |
| Furukawa et al., 2012 ( | 27 | F | Fibrous dysplasia | Combined posterior-transmanubrial approach | Yes | None |
| Medina and Paul, 2016 ( | M | 17 | Aneurysmal bone Cyst | Anterior approach (Transclavicular: clavicle was resected and reimplanted) | No | None |
| Matsunobu et al., 2021 ( | 27 | F | Giant cell tumor in the bone | Transmanubrial approach | No | None |
| Tvedten et al., 2021 ( | 5 | F | Osteochondroma | NA | NA | NA |
| Peng et al., 2023 ( | 26 | F | Osteoblastoma | Robotic-assisted wire saw resection | NA | None |
| 51 | M | Epithelioid malignant tumor | None | |||
| 21 | M | Fibro-osseous lesion | None | |||
| Chen et al., 2024 ( | 18 | M | Osteochondroma | Trans manubrial approach (L-shaped skin incision) | Yes | Brachial plexus injury |
| Buero et al., 2025 ( | 18 | M | Hemangiomas | Combined approach (video-assisted thoracoscopy and posterior access) | Almost | Asystole |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Shoulder and Clavicle Injuries · Head and Neck Cancer Studies
Background
Tumors of the ribs are uncommon, with those arising from the first rib being exceptionally rare. Resection of first rib tumors poses significant challenges due to limited exposure and the proximity of vital neurovascular structures, including the subclavian vessels and brachial plexus (1). The clavicle overlies the first rib, further complicating surgical access. Owing to the rarity of these tumors, there is no consensus on the optimal surgical approach (2–5). Various techniques have been described, including the transaxillary, transmanubrial, supraclavicular, and combined approaches, each with its own advantages and limitations (6–10). This report presents a case of successful entire first rib resection for a malignant tumor using the transclavicular approach (anterior approach with clavicular transection and reconstruction) and provides a comprehensive review of the literature.
Case presentation
A 43-year-old, previously healthy man experienced right-sided neck and back pain for 1 month. The physical examination was unremarkable. Laboratory investigations showed no abnormalities. A plain chest radiograph revealed a lytic lesion with an associated fracture in the right first rib (Figure 1A). Subsequent contrast-enhanced chest computed tomography (CT) demonstrated an osteolytic, expansile lesion in the mid-portion of the right first rib with cortical destruction and adjacent soft tissue swelling (Figure 1B). A three-dimensional (3D) printed model based on the CT scan illustrated the first rib lesion and its relationship with the subclavian vessels (Figure 1C). Magnetic resonance imaging (MRI) showed heterogeneous, high signal intensity on T2-weighted sequences within the lesion (Figure 1D). Fluorodeoxyglucose positron emission tomography-computed tomography (PET-CT) identified a solitary hypermetabolic focus in the same location [standardized uptake value maximum (SUVmax) of 11.1] with no other lesions (Figure 2). Given the imaging characteristics suggestive of malignancy and the lesion's inaccessible location for percutaneous biopsy, surgical excision was planned.
(A) An X-ray shows a lytic lesion and fracture in the right first rib; (B) a CT scan shows osteolytic destruction in the mid-segment of the right first rib, with soft tissue swelling; (C) the 3D printed model based on the CT scan; (D) T2-weighted MRI images show high-intensity signals in the middle part of right first rib.
PET-CT demonstrates a single lesion in the middle part of the first right rib with an SUVmax of 11.1.
Surgical technique
The patient was placed in a left lateral decubitus position under general anesthesia with double-lumen endotracheal intubation. The right cervicothoracic region was prepared and draped. A 12-cm supraclavicular incision was made extending from the sternoclavicular joint to the acromioclavicular joint (Figure 3A). Subcutaneous tissues and the platysma were divided. The clavicular insertion of the sternocleidomastoid muscle was detached. The clavicle was exposed, and a V-shaped osteotomy was performed at its midshaft using a piezosurgical device. This allowed elevation of the medial clavicular segment along with the underlying musculature.
(A) The patient is positioned in the left decubitus position, and a right supraclavicular surgical incision is created. (B) The brachial plexus is carefully dissected and protected (green arrow). (C) The resected first rib is extracted through the infraclavicular space. (D) Anatomical reduction of the clavicle is achieved using an anatomically contoured locking plate. (E) Gross specimen of the resected first rib and the cross-section shows the tumor within the rib and clear surgical margins. (F) A postoperative X-ray confirms stable clavicular fixation. (G) A photo of the surgical wound after surgery.
The phrenic nerve was identified coursing on the anterior surface of the anterior scalene muscle and was gently mobilized and protected throughout the procedure. The anterior scalene muscle was then divided close to its insertion into the first rib, taking care to avoid injury to the underlying subclavian artery. The subclavian vein and artery were meticulously dissected free from the rib and encircled with vessel loops. A moist gauze was passed beneath the vascular bundle to facilitate its gentle retraction (Figure 3B).
The brachial plexus trunks were identified posterior to the anterior scalene muscle. The plexus was carefully dissected from the tumor and surrounding tissues. Particular attention was paid to avoiding excessive traction. The middle scalene muscle was detached from the first rib, further exposing the rib posteriorly. A moist gauze was passed under the brachial plexus and used to gently lift the brachial plexus to create a space between the first rib and the brachial plexus (Figure 3B).
With the neurovascular structures protected and retracted, the first rib was fully visualized. The intercostal muscles were then divided. The rib was disarticulated posteriorly at the costotransverse joint and anteriorly at the sternocostal junction using rib cutters. The entire first rib, along with the tumor, was then removed en bloc through the infraclavicular space (Figure 3C). A small pleural tear was noted and repaired. A 24-Fr chest tube was inserted through a separate incision in the seventh intercostal space at the midaxillary line for postoperative drainage. The clavicular fragments were anatomically reduced and fixed with a pre-contoured titanium locking plate (Figure 3D). The wound was closed in layers. Finally, the specimen showed a satisfactory macroscopic margin (Figure 3E).
Postoperative course and follow-up
The patient's postoperative recovery was smooth. The chest tube was removed on postoperative day 3. His preoperative neck and back pain resolved completely. Upon a neurological examination, the right upper limb remained intact, with no evidence of brachial plexus injury, Horner's syndrome, or phrenic nerve palsy. A postoperative X-ray confirmed stable clavicular fixation (Figure 3F). The clavicular wound healed well without infection (Figure 3G). The patient was discharged on postoperative day 10. At the 3-month follow-up, he reported no pain, had full shoulder girdle function, and was satisfied with the cosmetic outcome. A histopathological examination diagnosed diffuse large B-cell lymphoma. The patient was referred to the hematology department for adjuvant therapy.
Discussion
First rib tumors present a formidable surgical challenge due to the overlying clavicle and the intimate relationship with the subclavian vessels, brachial plexus, and phrenic nerve (1, 11). This anatomical complexity also makes preoperative needle biopsy hazardous and often non-diagnostic (12). Therefore, careful preoperative planning with advanced imaging (CT, MRI, PET-CT, and 3D reconstruction) is of paramount importance to define the tumor's extent and its relationship with adjacent structures (13).
Our case illustrates the utility of the transclavicular approach for achieving the wide exposure necessary for safe, en bloc resection of a malignant first rib tumor. The key surgical principles in this region, shared with procedures for Pancoast tumors, cervicothoracic junction tumors, and thoracic outlet syndrome, include the following: (1) systematic identification and protection of the phrenic nerve on the anterior scalene muscle; (2) meticulous dissection and control of the subclavian vessels prior to rib manipulation; and (3) gentle handling and minimal retraction of the brachial plexus cords to prevent neuropraxia (5, 14, 15).
The literature describes several approaches to the first rib, including the transaxillary, transmanubrial, supraclavicular, and combined methods (2–5, 8–10). The transclavicular approach, involving clavicular osteotomy, provides direct anterior access to the thoracic inlet. While not “minimally invasive” in the conventional sense, it offers a wide and safe surgical field that is crucial for vascular control and complete tumor excision, especially for malignancies where en bloc resection is the goal. The main drawback is the need for clavicular osteotomy and reconstruction. However, as demonstrated, anatomical fixation with a modern locking plate provides stable union and preserves shoulder girdle function without cosmetic deformity, in contrast to older techniques involving clavicular resection. This approach appears particularly suitable for the following: (1) malignant or locally aggressive benign tumors requiring wide margins; (2) tumors located in the mid-portion of the rib where vascular control is critical; and (3) cases where other approaches (e.g., transaxillary) may offer insufficient exposure for safe dissection.
A literature review of first rib resection was performed after searching the PubMed database. Though not based on a systematic meta-analysis, it summarized reported cases and highlighted that complete first rib resection is rarely performed. Only 12 cases have been reported between 2000 and 2025. Table 1 presents a summary of these previous studies.
The previously reported transclavicular approach (2, 6, 11) requires the removal of the clavicle, which may offer a good surgical view, but postoperative deformity and functional impairment of the shoulder girdle were also reported. Compared to a previously reported method involving complete clavicular resection for surgical exposure and subsequent reconstruction (5), our approach is relatively minimally invasive.
It is worth mentioning that three-dimensional reconstruction of computed tomography can determine the size, location, and internal structure of the tumor, as well as its relationship with neighboring organs, playing a guiding role in surgical resection planning. These examinations enabled us to delineate the extent of the tissues surrounded by the tumor, thereby informing our decision on the most appropriate surgical approach.
In general, chest wall reconstruction is recommended when at least three ribs are resected or the size of the chest wall defect is ≥10 cm (12, 13). Therefore, chest wall reconstruction was not performed in this patient. A brachial plexus injury did not occur after surgery. The patient recovered gradually after 2 weeks with no residual symptoms. It is important to note that gentle manipulation during exposure of the subclavian tissue, avoidance of excessive stretching, and limited use of electrocoagulation are recommended.
The limitations of this report include its nature as a single case and the inherent selection bias. Larger, multicenter studies are needed to better define the indications and outcomes of different surgical approaches for first rib tumors.
In conclusion, the transclavicular approach with clavicular osteotomy and reconstruction is a valuable and safe technique for resecting challenging tumors of the first rib. It provides excellent exposure, protects critical neurovascular structures, and leads to complete oncological resection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Payne-James JJ Walesby RK. Symptomatic fibrous dysplasia of the right first rib excised via a posterolateral thoracotomy. Thorax. (1986) 41(7):575–6. 10.1136/thx.41.7.5753787540 PMC 460397 · doi ↗ · pubmed ↗
- 2Dartevelle PG Chapelier AR Macchiarini P Lenot B Cerrina J Ladurie FL Anterior transcervical-thoracic approach for radical resection of lung tumors invading the thoracic inlet. J Thorac Cardiovasc Surg. (1993) 105(6):1025–34. 10.1016/S 0022-5223(19)33774-28080467 · doi ↗ · pubmed ↗
- 3Grunenwald D Spaggiari L. Transmanubrial osteomuscular sparing approach for apical chest tumors. Ann Thorac Surg. (1997) 63(2):563–6. 10.1016/S 0003-4975(96)01023-59033349 · doi ↗ · pubmed ↗
- 4Lee SY Lee SJ Lee CS Lee KR. Aneurysmal bone cyst originating from the first rib. Am J Surg. (2008) 195(1):104–5. 10.1016/j.amjsurg.2007.01.03918082549 · doi ↗ · pubmed ↗
- 5Medina M Paul S. Aneurysmal bone cyst arising from the first rib: a rare cause of thoracic outlet syndrome. Thorac Cardiovasc Surg Rep. (2016) 5(1):74–6. 10.1055/s-0035-156999428018833 PMC 5177442 · doi ↗ · pubmed ↗
- 6Spaggiari L Calabrese L Chiesa F Pastorino U. Overcoming the transclavicular approach: the transmanubrial approach to the thoracic inlet. Head Neck. (2000) 22(6):629–30. 10.1002/1097-0347(200009)22:6<629::AID-HED 14>3.0.CO;2-310941167 · doi ↗ · pubmed ↗
- 7Furukawa M Soh J Toyooka S Ozaki T Miyoshi S. Resection of the entire first rib for fibrous dysplasia using a combined posterior-transmanubrial approach. Gen Thorac Cardiovasc Surg. (2012) 60(9):584–6. 10.1007/s 11748-012-0044-022614525 · doi ↗ · pubmed ↗
- 8Matsunobu T Maekawa A Nabeshima A Sakamoto A Tamura K Odate S Giant cell tumor of bone of the first rib successfully treated with combined preoperative denosumab therapy and surgery via a transmanubrial approach. Am J Case Rep. (2021) 22:e 931796. 10.12659/AJCR.93179634059614 PMC 8183306 · doi ↗ · pubmed ↗