Case Report: long complete metabolic response assessed by LAFOV FDG-PET/CT to FOLFIRINOX in first-line treatment of metastatic low-differentiated pancreatic carcinoma
Ronan Abgral, Jacques Dzuko Kamga, Jean-philippe Metges, Pierre-Yves Salaun

TL;DR
A 56-year-old patient with advanced pancreatic cancer showed a long-lasting complete metabolic response to FOLFIRINOX chemotherapy, as detected by FDG-PET/CT.
Contribution
This case report presents a rare long-term complete metabolic response to FOLFIRINOX in metastatic pancreatic cancer using FDG-PET/CT.
Findings
The patient showed a sustained metabolic complete response over 23 months.
FDG-PET/CT was used to assess the treatment response in metastatic pancreatic cancer.
This case suggests the potential of FDG-PET/CT in evaluating systemic cancer therapies.
Abstract
FOLFIRINOX chemotherapy is recommended as first-line treatment for metastatic pancreatic ductal adenocarcinoma (mPDAC). While its efficacy has been well documented in clinical trials, the responses observed have been predominantly partial. To date, only rare cases of complete response (CR) assessed by CT scan have been reported in the literature. We present a case of sustained metabolic CR over 23 months assessed by LAFOV FDG-PET/CT in a 56-year-old male patient with poorly differentiated mPDAC treated with FOLFIRINOX. This case highlights the emerging role of latest generation of digital FDG-PET/CT in assessing the therapeutic efficacy of systemic treatments for solid cancers.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
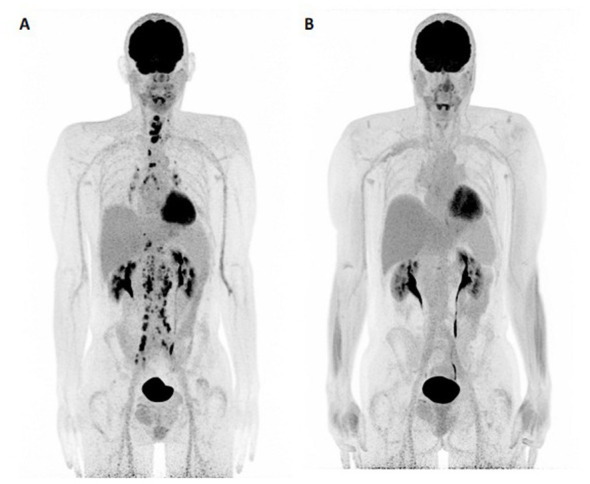 Figure 1
Figure 1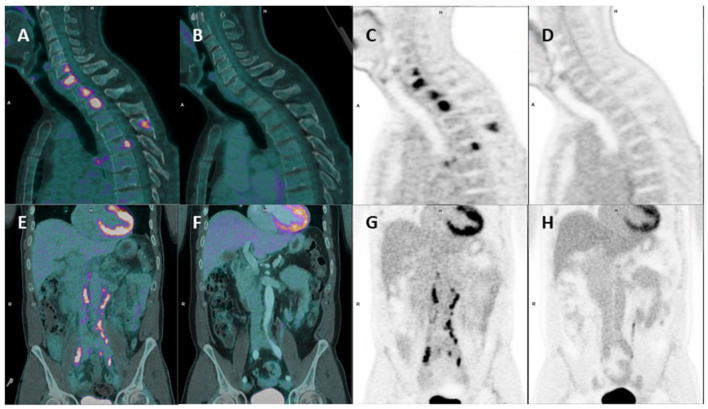 Figure 2
Figure 2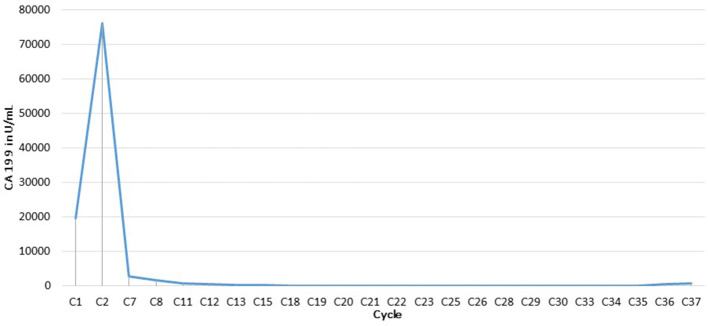 Figure 3
Figure 3|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Our case | 56/M | Lymph nodes, bone | Poorly differentiated | MMR positivity and HER2 negativity; MSS and KRAS mutation; no BRAF or BRCA mutations | FOLFIRINOX → FOLFIRI | Radiological CR | General condition alteration, PS 0–1 | Neuropathy → oxaliplatin discontinued; Esophagitis → irinotecan dose reduction | 7,5000 U/mL | Normalized | PET-CT | 23 months |
| Shelemey 2020 (PMID: 34031062) | 59/F | Liver | Moderately differentiated | MSI-stable; CCND1 amplification; KRAS (G12D) and TP53 (G245S) mutations; BRCA1/2–, PALB2– | FOLFIRINOX → FOLFIRI | Radiological CR | Pain, nausea, sweating; PS 1 | Neuropathy → oxaliplatin discontinued | ↑ 14514 U/mL; peak at 35,170 U/mL | Normalized | CT/MRI | >4 years |
| Tsujie 2020 (PMID: 32698268) | 46/F | Distant lymph nodes | ND | BRCA1/2 negative | FOLFIRINOX → FOLFIRI | Histological and radiological CR | Obstructive jaundice | Neuropathy → oxaliplatin discontinued | ↑ 71795.1 U/mL | Normalized | CT/PET-CT | ≥4 years |
| Nikolaou 2015 (PMID: 26090249) | 51/M | Post-surgery: lymph nodes, liver, lungs | ND | ND | FOLFIRINOX → FOLFIRI | Radiological CR | Abdominal pain; jaundice; weight loss; PS 0 | Neuropathy → oxaliplatin discontinued; Hematologic toxicity; Digestive toxicity with steatohepatitis | ↑ 12000 U/mL | Normalized | CT | ≥3 years |
| Yildirim 2023 (PMID: 36729128) | 42/F | Liver | ND | BRCA2 mutated | FOLFIRINOX | Radiological CR | ND | ND | ND | ND | CT | >5 years |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Medical Imaging Techniques and Applications · Radiomics and Machine Learning in Medical Imaging
Introduction
Pancreatic ductal adenocarcinoma (PDAC) accounts for approximately 500,000 new cases worldwide and is the 7th leading cause of cancer-related death in both men and women. The prognosis for PDAC remains extremely poor, with only 50% of patients surviving beyond 4 months and a 5-year survival rate of less than 10 % for metastatic disease (1).
FOLFIRINOX (oxaliplatin, irinotecan, fluorouracil, and leucovorin) chemotherapy is recommended as a first-line treatment for metastatic pancreatic ductal adenocarcinoma (mPDAC) (2). The randomized phase III PRODIGE trial showed that FOLFIRINOX significantly improved both median progression-free survival (6.4 vs. 3.3 months; p < 0.001) and overall survival (11.1 vs. 6.8 months; p < 0.001) compared to gemcitabine in patients with mPDAC. However, of the 54 responding patients in the FOLFIRINOX arm (n = 171), only one (0.6%) achieved a complete response (CR) (3).
18F-Fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) is an accurate tool for the initial staging of PDAC, particularly for the detection of distant metastases. In addition, FDG-PET/CT is emerging as a useful approach and valuable method for the therapeutic assessment of systemic treatments in metastatic gastrointestinal cancers (4).
Case Description
We report the case of a 56-year-old man with no prior medical history who was diagnosed with poorly differentiated metastatic pancreatic ductal adenocarcinoma (mPDAC). At diagnosis, the patient was in good general condition (ECOG performance status = 0), with no reported symptoms or abnormal clinical findings. Immunohistochemistry showed positivity for MMR proteins and HER2 negativity, while molecular analysis revealed microsatellite stable (MSS) status and a KRAS mutation, with no BRAF or BRCA mutations. Initial staging with FDG-PET/CT revealed lymph node and bone metastases (Figures 1A, 2A–C, E–G).
Initial evaluation and follow-up by FDG-PET/CT. (A, B) PET MIP showing all lesions at baseline and their disappearance on follow-up.
Initial evaluation and follow-up by FDG-PET/CT. (A, B) Sagittal PET/CT fusion and PET-only images. (C, D) showing the disappearance of cervical and thoracic spinal lesions. (E, F) coronal PET/CT fusion and PET-only images. (G, H) illustrating the resolution of the para-aortic and common iliac lymph nodes.
According to current guidelines, first-line treatment with FOLFIRINOX was initiated administered at dose of: oxaliplatin 85 mg/m^2^; irinotecan 180 mg/m^2^; leucovorin 400 mg/m^2^; and fluorouracil 400 mg/m^2^ as a bolus, followed by 2,400 mg/m^2^ as a 46-h continuous infusion every 2 weeks. Oxaliplatin was discontinued from the 5th cycle onward due to grade 2 hepatic cytolysis associated with grade 1 peripheral neuropathy. Following improvement in liver function tests and stabilization of neuropathy, oxaliplatin was reintroduced at the 8th cycle with a 20% dose reduction. However, it was permanently discontinued at the 10th cycle due to recurrence of hepatic cytolysis and peripheral neuropathy. Neuropathy subsequently remained stable at grade 1, and hepatic cytolysis completely resolved. Irinotecan was omitted at the 26th cycle due to esophagitis, and its dose was subsequently reduced by 17% for treatment continuation. Other adverse events were mainly gastrointestinal, consisting of nausea and vomiting, particularly at treatment initiation.
Follow-up FDG-PET/CT demonstrated a complete metabolic response (CMR) of the target lesions according to PERCIST criteria (Figures 1B, 2B–D, F–H). This response was correlated with a marked decrease in CA 19-9 levels, from more than 75,000 U/mL to within the normal range (Figure 3). Remission has been maintained for more than 23 months. The patient has remained in excellent general condition with an ECOG performance status of 0, continuing all usual daily activities. The baseline examination was performed using a conventional digital PET/CT without iodinated contrast enhancement, whereas response assessment was conducted using a long axial field-of-view (LAFOV) PET/CT with contrast-enhanced CT acquired during the portal venous phase.
CA 19-9 (U/ml) changes over the course of chemotherapy.
Discussion
Platinum-based chemotherapy has been associated with improved overall survival in patients with pancreatic adenocarcinoma harboring germline BRCA1 or BRCA2 mutations (5–7). This was not the case for our patient, in whom no BRCA mutation was identified. Moreover, the detected KRAS mutation is not known to confer specific sensitivity to FOLFIRINOX or FOLFIRI according to available data (8). Historically, gemcitabine monotherapy was the standard treatment for unresectable or recurrent disease (9). Subsequently, phase III trials demonstrated the superiority of FOLFIRINOX and gemcitabine plus nab-paclitaxel over gemcitabine alone (3, 10).
To our knowledge, this represents one of the rare cases of CMR observed on FDG-PET/CT in a patient with mPDAC treated with FOLFIRINOX. To date, only four cases of complete response assessed by CT have been reported; among them, one patient had a FDG-PET/CT demonstrating a CMR (11–14).
Therapeutic assessment was performed using a latest-generation LAFOV PET system, approximately ten-fold more sensitive compared with the digital PET system used at baseline, thereby strengthening the validity of this complete response. Although two different imaging systems were used, the sequence of their use limits the potential impact of this methodological heterogeneity. The conventional digital PET performed at diagnosis, being less sensitive, may theoretically have failed to detect very small additional lesions; however, this would not have altered the already metastatic stage of the disease. Conversely, the LAFOV PET/CT used for therapeutic evaluation provides an excellent negative predictive value. Therefore, the demonstration of a CMR with this system strongly suggests that it would also have been observed with a conventional PET system. Furthermore, iodinated contrast enhancement does not influence metabolic response assessment. The literature indicates that CMR assessed by functional imaging often precedes morphological response in metastatic gastrointestinal cancers (15, 16). A literature review of previously published cases of complete response in mPDAC treated with FOLFIRINOX is summarized in Table 1 (11–14).
Conclusion
We report a case of complete response of a metastatic PDAC on FDG-PET/CT using a more sensitive LAFOV system, highlighting the potential of FDG-PET/CT for therapeutic assessment of solid cancers in future clinical trials, particularly with these highly sensitive innovative systems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Tempero MA Malafa MP Al-Hawary M Behrman SW Benson AB Cardin DB . Pancreatic adenocarcinoma, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. (2021) 19:439–57. doi: 10.6004/jnccn.2021.001733845462 · doi ↗ · pubmed ↗
- 3Conroy T Desseigne F Ychou M BouchéO Guimbaud R Bécouarn Y . FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. (2011) 364:1817–25. doi: 10.1056/NEJ Moa 101192321561347 · doi ↗ · pubmed ↗
- 4Salaün P-Y Abgral R Malard O Querellou-Lefranc S Quere G Wartski M . Good clinical practice recommendations for the use of PET/CT in oncology. Eur J Nucl Med Mol I. (2020) 47:28–50. doi: 10.1007/s 00259-019-04553-831637482 · doi ↗ · pubmed ↗
- 5Kondo T Kanai M Kou T Sakuma T Mochizuki H Kamada M . Association between homologous recombination repair gene mutations and response to oxaliplatin in pancreatic cancer. Oncotarget. (2018) 9:19817–25. doi: 10.18632/oncotarget.2486529731985 PMC 5929428 · doi ↗ · pubmed ↗
- 6Blair AB Groot VP Gemenetzis G Wei J Cameron JL Weiss MJ . BRCA 1/BRCA 2 germline mutation carriers and sporadic pancreatic ductal adenocarcinoma. J Am Coll Surg (2018) 226:630-637.e 1. doi: 10.1016/j.jamcollsurg.2017.12.02129309945 PMC 6178809 · doi ↗ · pubmed ↗
- 7Golan T Kanji ZS Epelbaum R Devaud N Dagan E Holter S . Overall survival and clinical characteristics of pancreatic cancer in BRCA mutation carriers. Br J Cancer. (2014) 111:1132–8. doi: 10.1038/bjc.2014.41825072261 PMC 4453851 · doi ↗ · pubmed ↗
- 8Buscail L Bournet B Cordelier P. Role of oncogenic KRAS in the diagnosis, prognosis and treatment of pancreatic cancer. Nat Rev Gastroenterol Hepatol. (2020) 17:153–68. doi: 10.1038/s 41575-019-0245-432005945 · doi ↗ · pubmed ↗