Primary esophageal marginal zone lymphoma with respiratory symptoms: a case report and review of the literature
Xiaoyun Cheng, Wensi Zhang, Minggang Zhang, Shiyu Du

TL;DR
A rare case of primary esophageal lymphoma presented with respiratory symptoms instead of typical swallowing issues, highlighting the need for accurate diagnosis using specialized techniques.
Contribution
This is the first reported case of primary esophageal marginal zone lymphoma presenting with respiratory symptoms and no dysphagia.
Findings
The patient's long-standing atypical symptoms led to a delayed diagnosis of primary esophageal marginal zone lymphoma.
Endoscopic ultrasound-guided fine-needle aspiration was crucial for confirming the diagnosis and avoiding misdiagnosis.
The patient showed suboptimal response to initial treatment but improved with a combination of Obinutuzumab, Orelabrutinib, and Lenalidomide.
Abstract
Primary esophageal lymphoma is a rare disease whose pathogenesis may be related to immune abnormalities. We report a case of primary esophageal marginal zone lymphoma (MZL) in the esophagus for 2 years, which initially presented with respiratory symptoms and was subsequently diagnosed by endoscopic ultrasound-guided fine-needle aspiration. A 68-year-old male presented with a 10-day history of cough, excessive sputum production, and wheezing after physical activity. Two years prior to this admission, the patient had sought medical attention at our hospital for fever and cough. After completing the relevant examinations, the preliminary diagnosis was considered to be a pulmonary infection, with the possibility of an esophageal neoplastic lesion. Upon readmission, a follow-up chest CT revealed thickening of the esophageal wall in multiple segments, which was more pronounced than it had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
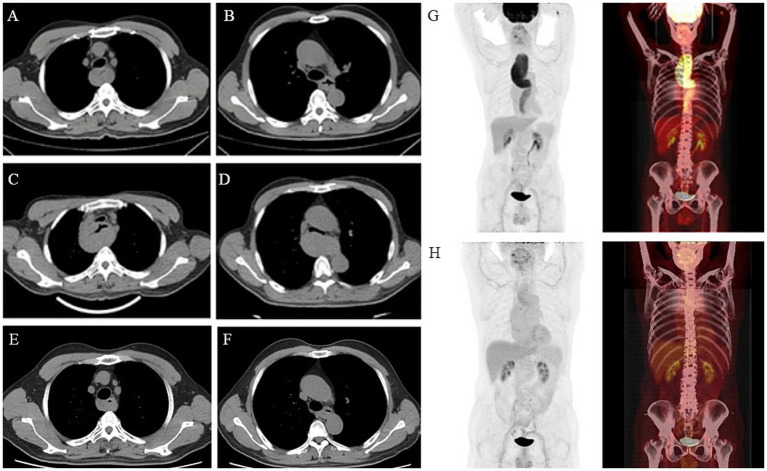 Figure 1
Figure 1 Figure 2
Figure 2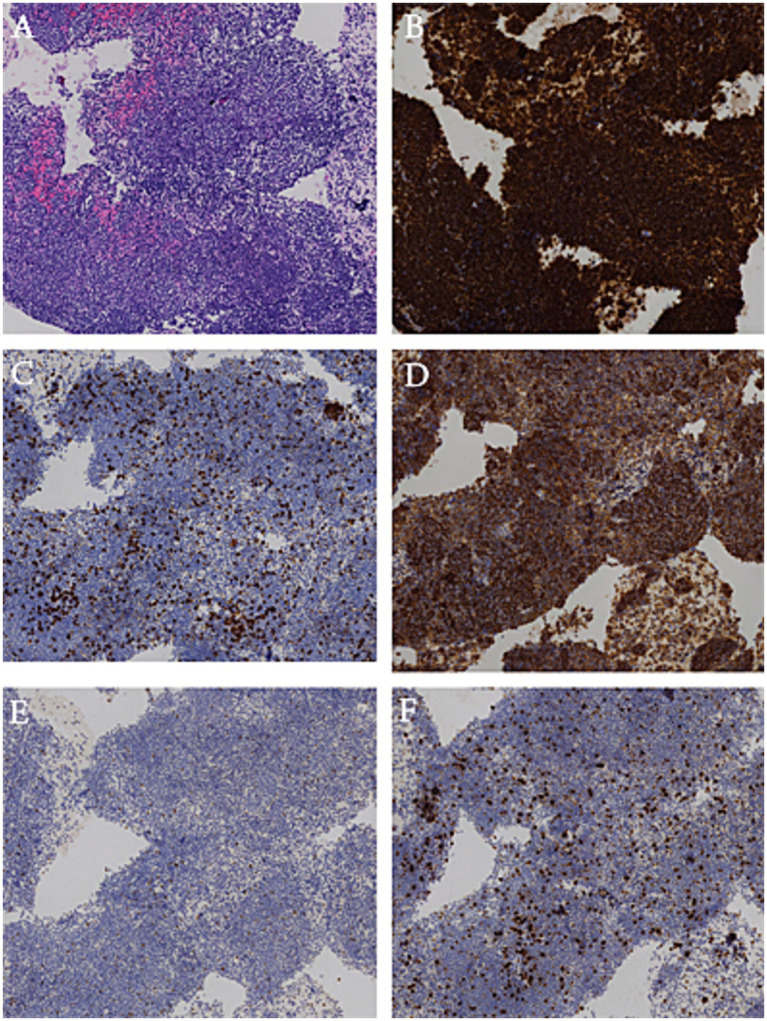 Figure 3
Figure 3| Ref | Age | Sex | Symptoms | Tumor | Treatment | Follow-up period (mo) | Outcome | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Location | Size, cm | Diagnostic method | Primary | Adjuvant | ||||||
| 2 | 62 | F | Dysphagia and weight loss | U-L | 2.7 | Biopsy | Chemotherapy and immunotherapy | NA | CR | |
| 6 | 68 | F | Dysphagia and weight loss | U-L | 7 | Biopsy | Chemotherapy and immunotherapy | NA | CR | |
| 7 | 66 | F | Dysphagia | M and L | 2.7 × 2.1 × 4.8 and 2.2 × 2.2 × 3.0 | Surgery | Surgery | Chemotherapy | NA | CR |
| 8 | 50 | M | NA | M-L | 10 | Surgery | Surgery | 12 | CR | |
| 9 | 49 | M | None | M | NA | Surgery | Surgery | 12 | CR | |
| 10 | 75 | M | NA | U-L | 14 × 3.5 × 2.5 | Surgery | Surgery | 8 | CR | |
| 11 | 53 | M | Dysphagia | M | 3.5 × 2.5 × 0.7 | Surgery | Surgery | Radiotherapy | 8 | CR |
| 12 | 61 | M | Dysphagia | U-L | 2 × 8 | Surgery | Surgery | 1 | CR | |
| 13 | 55 | M | None | M | 5 | Surgery | Surgery | 21 | Relapse (stomach) | |
| 14 | 62 | F | Dysphagia | U-L | 15.0 × 6.0 | ESD | Esd | 12 | CR | |
| 15 | 83 | F | Heartburn | U | 1 | EMR | Emr | 22 | CR | |
| 16 | 77 | F | Dysphagia | L | 4.3 × 2.8 × 1.5 | ESD | Esd | 5 | CR | |
| 17 | 70 | F | None | M | 0.6 × 0.4 and 2.0 × 0.8 | Biopsy | Emr | Radiotherapy | 36 | CR |
| 18 | 76 | M | Muscular weakness | M | NA | Biopsy | Radiotherapy | 12 | CR | |
| 19 | 59 | M | Tarry stool | U-L | 15 × 6.5 × 6 | Biopsy | Radiotherapy | 36 | CR | |
| 20 | 70 | F | None | L | 2 | Biopsy | Radiotherapy | 13 | CR | |
| 21 | 65 | M | Dysphagia | U | 10 × 3 × 3 | Biopsy | Chemotherapy | 24 | CR | |
| 22 | 49 | M | Hematochezia | M | 0.8 | Biopsy | Chemotherapy | 6 | CR | |
| 23 | 61 | M | Upper gastrointestinal bleeding | U | 1.2 | Biopsy | Chemotherapy | NA | NA | |
| 24 | 70 | M | Dysphagia | M | 5 | Biopsy | Immunotherapy | 6 | PR | |
| 25 | 60 | F | Dysphagia | U-L | NA | Biopsy | Chemotherapy and immunotherapy | NA | CR | |
| 26 | 85 | M | Dysphagia | U-L | NA | Biopsy | Chemotherapy and immunotherapy | NA | CR | |
| 27 | 60 | F | NA | L | 5 × 2 × 0.5 | Biopsy | Chemotherapy and immunotherapy | 24 | CR (granulomatous nodules) | |
| 28 | 72 | F | Anemia | M | 2 | Biopsy | Chemotherapy and immunotherapy | 12 | PR | |
| 29 | 63 | F | NA | U | 10 | Biopsy | Na | NA | NA | |
| 30 | 37 | M | NA | NA | NA | Biopsy | Na | NA | NA | |
| 31 | 72 | M | NA | NA | >10 | Biopsy | Na | NA | NA | |
| Present case | 68 | M | Cough, excessive sputum production and wheezing | U-L | >10 | Biopsy | Chemotherapy and immunotherapy | 12 | PR | |
- —China-Japan Friendship Hospital10.13039/501100012173
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Esophageal Cancer Research and Treatment · Eosinophilic Esophagitis
Introduction
Primary esophageal lymphoma is extremely rare, accounting for less than 1% of all gastrointestinal lymphomas (1). To date, fewer than 30 cases of primary esophageal lymphoma have been reported worldwide (2). The exact etiology remains unclear, but immunosuppression is considered an important risk factor, with a higher incidence observed in immunocompromised individuals (such as HIV-infected patients) (3–5). According to the current literature, clinical manifestations of primary esophageal lymphoma typically include progressive dysphagia and weight loss (6). Diagnosis is primarily based on endoscopic examination, biopsy, and immunohistochemical analysis. Treatment generally includes chemotherapy, often in combination with immunotherapy, radiation therapy, or surgery, depending on the pathological subtype and individual patient factors.
Case presentation
A 68-year-old male presented with a 10-day history of cough, excessive sputum production, and wheezing after physical activity, which developed without an obvious trigger. He reported no dysphagia or significant weight change. Physical examination was unremarkable, with no palpable lymphadenopathy or hepatosplenomegaly. Two years prior to this admission, the patient had sought medical attention at our hospital for fever and cough. A chest CT at that time revealed viral pneumonia and an irregular thickening of the esophagus, raising suspicion of a tumor. As the patient reported no other discomfort and did not pay close attention to these residual abnormalities, no further investigations were pursued at that time. In this context, the differential diagnosis mainly includes esophageal malignancies such as esophageal squamous cell carcinoma and esophageal adenocarcinoma, as well as benign esophageal conditions such as esophagitis and esophageal tuberculosis.
Upon admission, laboratory tests revealed the following results: white blood cell count of 6.95 × 10^9^/L, red blood cell count of 2.76 × 10^12^/L, hemoglobin level of 101 g/L, platelet count of 409 × 10^9^/L, total lymphocyte count of 0.96 × 10^9^/L, and reticulocyte percentage of 3.55%. The immunoglobulin M level was elevated at 713 mg/dL, complement C4 level was 15.4 mg/dL, the C1q circulating complex level was 392 mg/L, and the serum cystatin C level was 1.14 mg/L. HIV testing was negative. Lactate dehydrogenase at 183 U/L and C-reactive protein at 2.86 mg/L were both within normal limits. However, the CD4^+^ T-cell count was 265 cells/μL, which is below the normal reference range, indicating an underlying immunosuppressive state in the patient.
Two years prior, the patient’s chest CT revealed multisegmental thickening of the esophageal wall with mild local compression of the trachea (Figures 1A,B). Upon readmission, a follow-up chest CT demonstrated significantly increased thickening of the esophageal mucosa compared with that 2 years prior, with severe local tracheal compression. No obvious enlargement of the mediastinal lymph nodes was observed (Figures 1C,D). To further assess the benign or malignant nature of the lesion, identify the primary site, and evaluate the extent of disease involvement, a PET-CT scan was performed. PET-CT revealed irregular thickening of the entire esophageal wall, particularly in the upper chest segment, with uneven increased radioactive uptake (SUVmax: 8.9) and tracheal compression (Figure 1G). Esophagogastroduodenoscopy (EGD) revealed extensive uplifting lesions in the upper esophagus and longitudinal uplifting lesions in the lower esophagus, with the mucosal surface mostly smooth and intact, without ulcerative lesions. No abnormalities were found in the stomach or duodenum (Figures 2A,B). Endoscopic ultrasound (EUS) revealed the disappearance of the normal layered structure of the esophageal wall at the site of the lesion, with blood flow signals detected within the lesion (Figure 2C). The histopathological findings revealed that the lesion was indolent B-cell lymphoma, with the following immunohistochemical results: CD20(+), CD79a(+), CD3 (few +), CD5 (few +), Bcl6(−), CD10(−), Ki67 (MIB-1) (approximately 20%+), and EBER(−). The combination of histopathology and immunohistochemistry suggested a diagnosis of marginal zone lymphoma (Figure 3).
Findings of chest CT and PET-CT in 2022, 2024, and 2025. (A,B) Chest CT in 2022: multisegmental thickening of the esophageal wall and slight local compression of the trachea. (C,D) Chest CT taken in 2024 revealed that the esophageal mucosa thickened significantly with severe local pressure in the trachea and that there was no significant lymph node enlargement in the mediastinum. (E,F) Chest CT in 2025: significant improvement in esophageal mucosal thickening compared to previous scans, with reduced compression on the trachea. (G) PET-CT in 2024: revealed irregular thickening of the entire esophageal wall and an uneven increase in radioactivity uptake. (H) PET-CT in 2025: reduced esophageal wall thickening compared to previous scans, suggesting partial remission.
Findings of white light endoscopy and endoscopic ultrasound in 2024. (A) Esophagogastroduodenoscopy (EGD) in a forward endoscopic view revealed extensive uplifting lesions in the upper esophagus. (B) EGD revealed longitudinal uplifting lesions in the lower esophagus. (C) Endoscopic ultrasound demonstrated thickening of the esophageal wall, with the arrow indicating a hyperechoic puncture needle.
Histopathological analysis and immunohistochemical examination of the resected specimen. Diffuse infiltration of atypical lymphocytes in the marginal zone of lymphoid follicles. (A) HE. (B) CD20 (+). (C) CD3 (−). (D) CD21 (+). (E) Bcl6 (−). (F) Ki-67 (20%). Original magnification 100×.
In the same year, the patient consulted the hematology department. Tests for tuberculosis, Epstein–Barr virus, cytomegalovirus, and hepatitis B virus were all negative. Bone marrow aspiration revealed hypoactive marrow proliferation with no significant evidence of tumor involvement. KRAS and NRAS gene mutation analyses were also negative, and no abnormalities were detected in the immunoglobulin gene rearrangement test. Immunohistochemical analysis revealed the following: CD10 (partial +), CD117 (−), CD138 (partial +), CD235a (erythroid +), CD3 (+), CD34 (vascular +), CD5 (+), CD61 (megakaryocytic +), CD79α (sporadic +), Cyclin D1 (−), MPO (myeloid +), TdT (−), and CD20 (L26) (scattered +). The findings were consistent with marginal zone lymphoma. The patient was diagnosed with primary esophageal marginal zone lymphoma (MZL) (Ann Arbor-Cotswold Stage IE).
On the basis of the PET–CT results, the lymphoma was considered to be primary and confined to the esophagus and was staged as stage 1E. Currently, after two courses of the G-CVP regimen (Obinutuzumab + Cyclophosphamide + Vincristine + Prednisone) demonstrated suboptimal efficacy, the treatment was switched to a triple combination of Obinutuzumab, Orelabrutinib, and Lenalidomide, which has now completed six courses. The patient’s cough and wheezing after exercise improved. After completion of treatment, follow-up chest CT showed that the esophageal mucosal thickening had significantly improved compared to previous scans, and the tracheal compression was alleviated (Figures 1E,F). Follow-up PET-CT revealed that the esophageal wall thickening was reduced compared to previous scans, and no suspicious new lesions were found, suggesting partial remission (Figure 1H). The patient is still being closely monitored.
Discussion
Primary esophageal lymphoma is an extremely rare and unique clinical entity, accounting for less than 1% of all gastrointestinal lymphomas1. Most cases of primary esophageal MZL are linked to immunosuppressive conditions, such as HIV/AIDS, suggesting that immune dysfunction plays a significant role in its pathogenesis (3–5). Although this patient did not present with obvious immunodeficiency, immunological tests revealed elevated levels of immunoglobulin M, complement C4, and C1q. The exact underlying mechanism remains unclear, and further research is needed to better understand the genetic and molecular factors contributing to its development.
Clinically, primary esophageal MZL presents with nonspecific symptoms such as dysphagia and weight loss (6). The clinical manifestations are highly heterogeneous, and diagnosis relies heavily on pathological results from biopsy due to the absence of specific diagnostic tests and endoscopic or imaging findings. These nonspecific features often lead to misdiagnosis as other esophageal diseases, such as squamous cell carcinoma, adenocarcinoma, esophagitis, leiomyoma, or tuberculosis, which may present similarly on imaging as wall thickening or submucosal masses. This diagnostic challenge highlights the main focus of this case report: not the treatment itself, but the difficulty in detecting primary esophageal MZL due to its rarity and lack of distinctive features. Therefore, even in cases where imaging only shows esophageal wall thickening and the patient presents with mild symptoms, clinicians should include primary esophageal lymphoma in the differential diagnosis to raise awareness of this disease and avoid missed diagnosis and misdiagnosis. With advancements in endoscopic techniques, this patient underwent endoscopic biopsy through endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA), avoiding the trauma associated with traditional surgical procedures. The treatment of MZL typically includes surgery, chemotherapy, and radiotherapy. However, owing to the limited number of cases, the lack of large-scale studies, and insufficient long-term follow-up data, treatment strategies and prognostic outcomes have not been fully standardized. A literature review up to March 1, 2026, identified 27 reported cases of primary esophageal MZL, 23 of which included treatment details (Table 1). Among these, 11 patients underwent surgical treatment (7–17), including 3 patients who underwent endoscopic resection (14–17). Three patients received adjuvant radiotherapy or chemotherapy following surgery (7, 11, 17). There were 3 patients treated with radiotherapy alone (18–20), 3 patients treated with chemotherapy alone (21–23), 1 patient treated with immunotherapy alone (24), and 6 patients treated with a combination of chemotherapy and immunotherapy (2, 6, 25–28). In the remaining 3 reports, only the diagnosis was mentioned without treatment details (29–31). Most patients achieved remission after treatment. However, 1 patient experienced relapse after radiotherapy (13), and 1 patient developed mediastinal lymph node granulomatous nodules after combined chemoimmunotherapy (27). Notably, with the advancement of endoscopic techniques, diagnosis increasingly relies on endoscopic procedures rather than surgical interventions. In the past 8 years, 4 newly reported cases were primarily diagnosed through endoscopy. Among them, 1 patient with mucosa-confined disease was completely resected by endoscopic submucosal dissection (ESD) (14), while the other 3 patients were diagnosed through endoscopic biopsy and subsequently treated with combined chemoimmunotherapy, all of which produced favorable responses (2, 6, 26). In accordance with the latest guidelines (32), this patient was treated with the G-CVP regimen (cyclophosphamide, vincristine, prednisone, and obinutuzumab) and has completed two cycles of therapy, but the treatment efficacy has been suboptimal. Currently, the triple combination regimen of Obinutuzumab + Orelabrutinib + Lenalidomide has not been listed as a standard recommended therapy in international mainstream guidelines. However, clinical trials are exploring its potential, and it is primarily used for aggressive or refractory B-cell non-Hodgkin lymphomas (NHL), especially as salvage therapy after failure of standard treatments.
Conclusion
In conclusion, primary esophageal MZL is a rare but treatable type of lymphoma, and timely and thorough endoscopic biopsy is crucial, especially in immunocompromised patients. With appropriate treatment, the prognosis is generally favorable. However, further research is needed to better understand its pathogenesis and to optimize treatment strategies, aiming to improve patient outcomes and guide clinical decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Herrmann R Panahon AM Barcos MP Walsh D Stutzman L. Gastrointestinal involvement in non-Hodgkin's lymphoma. Cancer. (1980) 46:215–22. doi: 10.1002/1097-0142(19800701)46:1<215::AID-CNCR 2820460136>3.0.CO;2-6, 7388763 · doi ↗ · pubmed ↗
- 2Han C Lin R Xu M Liu J Ding Z. Primary mucosa-associated lymphoid tissue lymphoma of the entire esophagus diagnosed by endoscopic ultrasound-guided fine needle aspiration. Endoscopy. (2022) 54:E 694–e 5. doi: 10.1055/a-1722-2386, 35226934 · doi ↗ · pubmed ↗
- 3Gaskin CM Low VH Ho LM. Isolated primary non-hodgkin's lymphoma of the esophagus. AJR Am J Roentgenol. (2001) 176:551–2. doi: 10.2214/ajr.176.2.1760551, 11159120 · doi ↗ · pubmed ↗
- 4Golioto M Mc Grath K. Primary lymphoma of the esophagus in a chronically immunosuppressed patient with hepatitis C infection: case report and review of the literature. Am J Med Sci. (2001) 321:203–5. doi: 10.1097/00000441-200103000-00010, 11269799 · doi ↗ · pubmed ↗
- 5Moses AE Rahav G Bloom AI Okon E Polliack A Maayan S . Primary lymphoma of the esophagus in a patient with AIDS. J Clin Gastroenterol. (1995) 21:327–8. doi: 10.1097/00004836-199512000-00018, 8583112 · doi ↗ · pubmed ↗
- 6Oría IC Pizzala JE Villaverde AM Urgiles DC Wright FG Jauk F . Primary lymphoma of the entire esophagus diagnosed by endoscopic ultrasound-guided fine needle aspiration (EUS-FNA). Radiol Case Rep. (2021) 16:1242–4. doi: 10.1016/j.radcr.2021.02.051, 33868528 PMC 8041659 · doi ↗ · pubmed ↗
- 7Karamustafaoglu YA Can N Yanık F Yoruk Y. Prımary esophageal Extranodal margınal zone lymphoma: a rare tumor: primary esophageal lymphoma in a patient presenting as dysphagia. Dig Dis Sci. (2025) 70:4000–2. doi: 10.1007/s 10620-025-09273-8, 40711741 · doi ↗ · pubmed ↗
- 8Bardisi ES Alghanmi N Merdad AA. Primary mucosa-associated lymphoid tissue lymphoma of the esophagus masquerading as a benign tumor. Ann Med Surg (Lond). (2014) 3:39–42. doi: 10.1016/j.amsu.2014.05.001, 25568784 PMC 4268481 · doi ↗ · pubmed ↗