Mortality and Causes of Death After Metabolic Bariatric Surgery in Older Patients
Peter Gerber, Giola Santoni, My von Euler-Chelpin, Joonas H. Kauppila, Dag Holmberg

TL;DR
Metabolic bariatric surgery may reduce mortality in older patients with severe obesity, particularly for deaths related to cardiovascular disease.
Contribution
This study provides evidence that metabolic bariatric surgery reduces mortality in older patients with severe obesity.
Findings
Patients who underwent metabolic bariatric surgery had a 32% lower mortality risk compared to non-operated patients.
Operated patients were less likely to die from cardiovascular disease.
No mortality benefit was observed for patients over 70 years old at the time of surgery.
Abstract
Metabolic bariatric surgery leads to improved life expectancy in younger individuals, but whether older (> 60 years) individuals benefit from metabolic bariatric surgery is uncertain. This study examined mortality and causes of death in patients with metabolic bariatric surgery at age 60 years or older. This was a population-based matched cohort study based on all healthcare in Denmark, Finland, and Sweden between 1996 and 2024. All patients who had primary metabolic bariatric surgery at age > 60 years were included and exactly matched 1:5 to comparison individuals of the same age, sex, country, and calendar year with non-operative treatment for obesity. Cox regression provided hazard ratios with 95% confidence intervals for mortality adjusted for multiple obesity-related diseases and frailty. In total, 3879 (16.7%) patients with metabolic bariatric surgery and 19395 (83.3%) patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
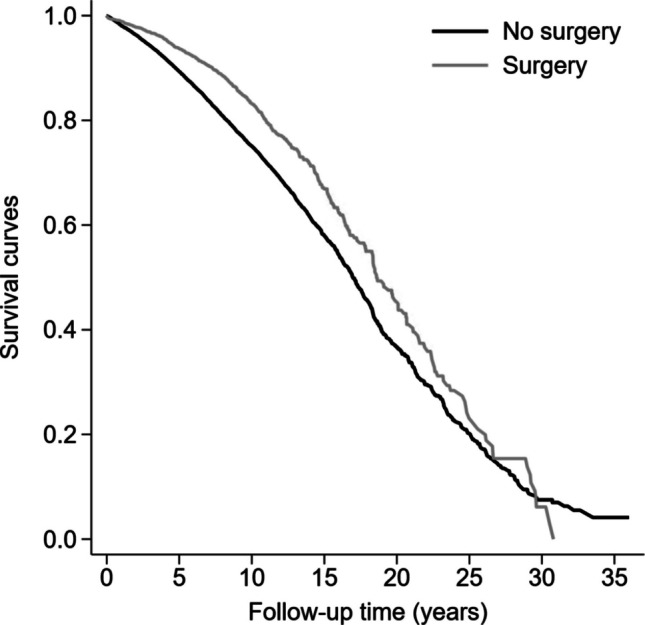 Figure 1
Figure 1- —Karolinska Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Cardiovascular Function and Risk Factors · Cardiovascular Disease and Adiposity
Introduction
Obesity is a global health problem that currently affects 30–40% of adults in high-income countries [1]. Obesity is associated with several diseases, mainly diabetes, hypertension, cardiovascular diseases, cancer, and psychiatric disorders, as well as reduced overall survival [2, 3]. Individuals with severe obesity (body mass index ≥ 35 kg/m^2^) are eligible for metabolic bariatric surgery, which induces rapid, pronounced and long-lasting weight loss, and in many cases resolution of obesity-related diseases [4–11]. Multiple studies have demonstrated the association between metabolic bariatric surgery and prolonged life expectancy, but have generally been conducted in younger patients [4, 7, 8, 12].
There is controversy whether metabolic bariatric surgery should be recommended to older individuals (> 60 years) with severe obesity, as the complication rate may be increased and the weight loss decreased compared to bariatric surgery performed in the young [13, 14]. Few studies have examined the potential long-term benefits of metabolic bariatric surgery in individuals age > 60 years. Using nationwide data from three Nordic countries, we set out to assess mortality and causes of death in patients who had bariatric surgery at age 60 years or older in comparison to patients with non-operative care for obesity.
Materials and Methods
Design
This was a population-based matched cohort study including data from three entire Nordic countries. The study period varied between the participating countries: Denmark, July 1, 1996-December 31, 2018; Finland, January 1, 1989-December 31, 2018; Sweden, January 1, 1989-December 31, 2024. Start of follow-up occurred with the introduction of ICD-9 in Finland and Sweden and with the introduction of operation codes for metabolic bariatric surgery in Denmark. All data used in the study were retrieved from nationwide healthcare databases, i.e., the patient registries, cancer registries, and cause of death registries of the three countries. Approvals were obtained from the relevant authorities in each country.
Exposure
The study population was retrieved from the patient registries, which prospectively collect data on all in-hospital and specialized out-patient healthcare (not primary care), including individual level data on diagnoses and procedures. All patients that had undergone primary metabolic bariatric surgery, i.e., gastric bypass, sleeve gastrectomy, gastric banding, vertical banded gastroplasty, duodenal switch with biliopancreatic diversion, or other metabolic bariatric procedures (Supplementary Table 1), at age > 60 years in any of the three countries were considered exposed. These patients were compared to patients diagnosed with obesity (Supplementary Table 2) by a physician and not treated with metabolic bariatric surgery, i.e., non-operative treatment. After exact matching by country, age, sex, and calendar year, up to 5 patients with non-operative treatment for obesity were randomly selected for each operated patient. If 10 or less matching patients with non-operative treatment for obesity were available for a specific operated patient, matching age was extended up to a maximum of ± 2 years of age. Patients with a history of neoplasia were excluded.
The patient registries of the Nordic countries have been extensively validated overall with positive predictive values of diagnoses ranging from 73%−88% in Denmark [15], 75%−99% in Finland [16], and 85%−95% in Sweden [17]. Metabolic bariatric surgery has been specifically validated in Sweden, where a study of 938 patients showed 97% concordance between reviewed operation charts and data from the patient registry [18].
Endpoints
The outcome was death due to any cause, which was identified in the cause of death registries. Additionally, we described the main cause of death for operated and non-operated patients. The cause of death registries contain virtually complete and continuously updated information on date of death and cause(s) of death in all three countries based on an assessment by the physician confirming the death [19, 20].
Confounders
We identified several relevant confounders potentially associated with both a propensity of undergoing/not undergoing metabolic bariatric surgery and mortality: diabetes (yes or no), hypertension (yes or no), peripheral vascular disease (yes or no), chronic obstructive pulmonary disease (yes or no), renal disease (yes or no), and cardiovascular disease (yes or no). Additionally, we included frailty-related diagnoses: deep vein thrombosis or pulmonary embolism (yes or no), pneumonia (yes or no), and number of previous hospital admissions (continuous). All confounders were identified through a two-year historical search in the patient registries (Supplementary Table 3).
Statistical Analysis
Operated patients entered the study on the date of primary metabolic bariatric surgery, with their corresponding matched comparison patients entering on the same date. Patients were followed until date of death or the end of the study period in each participating country, whichever occurred first. Multivariable Cox regression analysis was used to calculate hazard ratios (HR) with 95% confidence intervals (CI) for all-cause mortality. Standard errors were estimated using the clustered sandwich estimator. Two statistical models were used: one crude and one adjusted for all potential confounders with categorizations as described above (“Confounders” paragraph). The proportionality of the hazard was assessed by calculating the Schoenfeld residuals; the assumption of proportionality was not met, why the main analysis was presented stratified by follow-up period. Analyses were also stratified according to age (categorizations), sex (male or female), calendar year (divided by the median year), and diabetes (yes or no). Using Laplace regression, we calculated the difference in the 5th and 10th percentile of time to death with 95% CI in operated and non-operated patients adjusted by the confounders listed above [21]. In a post-hoc sub analysis, we excluded patients with a history of cardiovascular disease at baseline. Data management and analyses were conducted by a senior biostatistician (GS) in accordance with a detailed and pre-planned study protocol. The study followed the STROBE reporting guideline for cohort studies.
Results
Patients
We included 3879 patients with metabolic bariatric surgery at age > 60 years and 19,395 matched patients with non-operative treatment for obesity. Median age was 63 years (interquartile range, 62–65 years) and 64.1% were female in both groups (Table 1). Most operated patients underwent either gastric bypass (74.0%, n = 2871) or sleeve gastrectomy (15.4%, n = 599). Operated patients were more frequently diagnosed with diabetes and hypertension, but to a less degree cardiovascular disease. Variables associated with frailty were similarly distributed in both groups. 90-day mortality was 0.6% (n = 24) in operated patients and 0.4% (n = 74) in patients with non-operative treatment for obesity (p = 0.03). Causes of death within 90-days are reported in Supplementary Table 4.Table 1. Characteristics among older patients with metabolic bariatric surgery and matched controls with nonoperative treatment for obesityPatients, No. (%)CharacteristicNonoperative treatmentMetabolic bariatric surgeryTotal19395 (83.3)3879 (16.7)Sex Female12430 (64.1)2486 (64.1) Male6965 (35.9)1393 (35.9)Age, median (IQR), y63 (62–65)63 (62–65) 60–6515,338 (79.1)3072 (79.2) 66–703216 (16.6)642 (16.6) > 70841 (4.3)165 (4.3)Year of entry, median (IQR)2013 (2010–2017)2013 (2010–2017)Country Denmark2190 (11.3)438 (11.3) Finland4060 (20.9)812 (20.9) Sweden13145 (67.8)2629 (67.8)Diabetes4496 (23.2)1454 (37.5)Hypertension6116 (31.0)2147 (55.3)Peripheral vascular disease464 (2.4)64 (1.6)Chronic obstructive pulmonary disease972 (5.0)157 (4.0)Renal disease596 (3.1)86 (2.2)Cardiovascular disease2719 (14.0)381 (9.8)Frailty Deep vein thrombosis or pulmonary embolism224 (1.2)32 (0.8) Pneumonia573 (3.0)84 (2.2) Previous hospital admissions*, median (IQR), no3 (1–7)4 (2–9)90-day mortality74 (0.4)24 (0.6)All-cause mortality4536 (23.4)677 (17.5)Follow-up time, median (IQR), y7.1 (3.3–10.9)7.8 (4.0–11.3)*Within two years of cohort entry
Mortality
Patients were followed for median 7.7 years of follow-up, during which 5 213 (22.4%) died. The cumulative mortality was 17.5% (n = 677) in the operated patients compared to 23.4% (n = 4536) in the non-operated (Fig. 1). After adjustments, patients with metabolic bariatric surgery had a 32% decreased risk of mortality compared to matched patients (HR 0.68, 95% CI 0.63–0.73) (Table 2). Stratification by follow-up period revealed that the decreased risk associated with metabolic bariatric surgery was due to decreased mortality in the first 15 years after surgery (Table 2). With longer follow-up time, the adjusted hazard of death was similar in operated and non-operated patients. The association between surgery and mortality was apparent in patients operated at age > 60–64 (HR 0.64, 95% CI 0.58–0.71) and 65–70 years (HR 0.66, 95% CI 0.55–0.78), but there was no apparent benefit of surgery at age > 70 years (HR 1.23, 95% CI 0.90–1.67). Further stratified analyses by sex, country, calendar year, and diabetes largely verified a protective association between metabolic bariatric surgery and mortality (Table 2). The protective association was more pronounced in patients with diabetes (HR 0.56, 95% CI 0.48–0.66) compared to those without diabetes (HR 0.81, 95% CI 0.72–0.91) (Table 2). In the adjusted analysis of time to death, metabolic bariatric surgery was associated with 1.3 (95% CI 0.6–1.9) and 1.9 (95% CI 1.4–2.4) years longer life among the first 5% and 10% of people who died, respectively. A sub analysis restricted to patients with gastric bypass (n = 2871) with matched controls (n = 14355) showed 36% decreased mortality in operated patients (HR 0.64, 95% CI 0.58–0.71) (Supplementary Table 5). Similarly, the sub analysis in patients without cardiovascular disease at baseline (n = 17488), metabolic bariatric surgery remained associated with a decreased risk of all-cause mortality (HR 0.72, 95% CI 0.64–0.79).Fig. 1. Cumulative survival as a function of time among older patients with metabolic bariatric surgery compared to nonoperative treatment for obesityTable 2Mortality in older patients with metabolic bariatric surgery and non-operative treatment for obesityNon-operative treatmentMetabolic bariatric surgeryHazard ratio (95% CI)CharacteristicPerson-yearsDeaths, NoPerson-yearsDeaths, NoUnadjustedAdjusted*Total1457454536308876770.69 (0.64–0.74)0.68 (0.63–0.73)Follow-up (years) < 1186333543746420.59 (0.43–0.81)0.62 (0.45–0.84) 1–5723401757150782060.56 (0.49–0.65)0.57 (0.49–0.66) 6–1038916141885662300.74 (0.64–0.84)0.71 (0.62–0.82) 11–151289668129001230.80 (0.66–0.97)0.75 (0.62–0.91) > 152960326710760.96 (0.75–1.23)0.95 (0.74–1.20)Sex Female961822539204383670.66 (0.60–0.74)0.65 (0.59–0.72) Male495631997105603100.72 (0.64–0.80)0.72 (0.64–0.81)Age ≤ 651187363221253264670.67 (0.61–0.73)0.64 (0.58–0.71) 65–702208691447911340.66 (0.55–0.78)0.66 (0.55–0.78) > 704923401881761.08 (0.86–1.36)1.14 (0.89–1.47)Country Denmark138793612862500.67 (0.51–0.88)0.68 (0.51–0.90) Finland204646434219830.64 (0.52–0.77)0.63 (0.51–0.77) Sweden1114023532239185440.70 (0.64–0.76)0.69 (0.63–0.75)Calendar year ≤ 20131024273553219255760.74 (0.68–0.81)0.72 (0.66–0.78) > 20134331898390731010.49 (0.40–0.59)0.50 (0.41–0.62)Diabetes No1142682941194143990.77 (0.70–0.85)0.78 (0.71–0.86) Yes314771595115842780.46 (0.41–0.52)0.56 (0.49–0.63)*Adjusted for diabetes, hypertension, peripheral vascular disease, chronic obstructive pulmonary disease, renal disease, cardiovascular diseases, deep vein thrombosis or pulmonary embolism, pneumonia, number of previous hospital admissions
Causes of Death
Cardiovascular disease (64.7%, n = 3375) was the most commonly occurring cause of death in both operated and non-operated, followed by cancer (26.0%, n = 1 354) and abdominal diseases (11.2%, n = 586) (Table 3). Operated patients were less likely to die from cardiovascular disease than the non-operated (57.6% versus 65.8%, p < 0.001)), but otherwise the causes of death were overall similarly distributed.Table 3. Causes of death in older patients with metabolic bariatric surgery and non-operative treatment for obesityDeaths, No. (%)Cause of deathNon-operative treatmentMetabolic bariatric surgeryTotal4536677 Cardiovascular2985 (65.8)390 (57.6) Cancer1161 (25.6)193 (28.5) Infections447 (9.9)61 (9.0) Intoxication†166 (4.0)43 (6.9) Complications†44 (1.1)12 (1.9) Abdominal495 (10.9)91 (13.4) Other568 (12.5)94 (13.9)†Not available in Denmark
Discussion
The main result of this study was that metabolic bariatric surgery at age > 60 years was associated with a decreased mortality compared to non-operative treatment for obesity.
Main strengths of the study include the population-based design and the large sample size of patients with metabolic bariatric surgery at older age, which was achieved through nationwide inclusion from three countries. We used data from national registries which have been largely validated for the purposes of the study, reducing the risk of misclassification and selection. Due to the large sample size of older operated patients, we could use both matching and extensive adjustments for obesity-related diseases and frailty variables to reduce confounding. We could also analyse mortality in women and men separately and patients in different age strata with retained precision. We were aware of the potential risk of confounding through selection of healthier individuals to have metabolic bariatric surgery at older age and therefore took meticulous care to reduce its impact. Following matching, we did not find any clear signs that patients that underwent surgery were healthier at baseline apart from a slightly lower prevalence of cardiovascular disease. As we observed this, we performed a post-hoc analysis which demonstrated that metabolic bariatric surgery was associated with decreased mortality after exclusion of patients with cardiovascular disease at baseline, suggesting robustness of the main results.
While known confounding was likely well controlled after adjustments, we lacked data on preoperative body mass index, smoking, and socioeconomic status, which was not available from the data sources. While these variables may be associated with both exposure and outcomes, they were indirectly adjusted for by the inclusion of closely associated diseases (e.g., diabetes and chronic obstructive pulmonary disease) in the statistical model. The direction of bias from any residual confounding by body mass index or smoking is not immediately clear. Presumably, patients who underwent operation might have more severe obesity compared to non-operated, while active smoking may be a reason to not operate. We attempted to account for any selection of healthier individuals by adjusting for three separate variables associated with frailty, i.e., previous pneumonia, hospitalizations, and thrombosis. These variables were similarly distributed among operated and non-operated patients at baseline, suggesting no major differences in frailty. Nevertheless, it cannot be ruled out that frailty was not completely captured by these three variables and that there remained residual confounding. Finally, we did not have data on the precise treatment for obesity in the non-operative group. With these limitations in mind, the study should be internally valid and the nationwide inclusion from three countries suggests excellent generalizability to other countries with similar demographics and healthcare structure.
Few studies have examined long-term mortality rates specifically in older patients undergoing metabolic bariatric surgery. A US cohort study performed in a high-volume metabolic bariatric surgery centre examined mortality outcomes by different age strata in patients with gastric bypass. Of these, 1210 patients were operated at age 55 or older and followed for mean 5.9 years, where mortality was 50% decreased (HR 0.50, 95% CI 0.31–0.79) compared to age-matched controls with obesity [22]. The association found in that study was slightly more pronounced than in the current study, which may have been due to overall younger age in the American cohort or by the inclusion of gastric bypass procedures only. Metabolic bariatric surgery performed in high-volume centres is also associated with improved long-term survival, which would also explain more moderate associations observed in the current study, which included all metabolic bariatric surgeries in the participating countries (including from low volume centres) [23]. From this study, it appeared as if the protective association between metabolic bariatric surgery and mortality becomes weaker with older age as the benefit of surgery disappeared at age > 70 years. It should be noted that the study could not entirely rule out a small benefit for surgery in patients > 70 years because of limited precision. Also, patients with metabolic bariatric surgery had a considerably better prognosis with lower mortality in the first 15 years of follow-up. After this period, the adjusted mortality rates were similar among operated and non-operated patients, meaning that the effect size of the protective association between metabolic bariatric surgery and mortality waned with longer follow-up time.
There are reports of reduced benefits of metabolic bariatric surgery in older patients, including less weight loss and lower rates of resolution of obesity-related diseases such as diabetes and hypertension [24]. The consequences of the reduced impact of metabolic bariatric surgery on weight and obesity-related diseases were also largely verified in a recent population-based cohort study where the incidence of cancer (HR 0.81, 95% CI 0.64–1.03) and cardiovascular disease (HR 0.86, 95% CI 0.74–1.01) were similar in patients with metabolic bariatric surgery at age 60 years or older compared to matched controls [25]. While the results of that study were non-significant, point estimates indicated a slightly decreased risk of both outcomes, which are major causes of death for older patients with obesity. This was also verified in this study, were both operated and non-operated patients largely died due to diseases related to old age, e.g., cardiovascular disease and cancer, and to a less degree related to intoxication, which is a more common cause of death in younger individuals with metabolic bariatric surgery [26]. Protective associations were particularly pronounced in patients with diabetes and in those operated in more recent calendar periods, which may be explained by a higher proportion of patients with gastric bypass in these strata. This notion was also verified in the subgroup analysis limited to patients with gastric bypass, where the association with decreased mortality was profound. It should be noted that perioperative mortality in this study was clearly higher than what has been reported in younger individuals (typically < 0.1%), which highlights the need for preoperative risk assessment and careful selection of older individuals for surgery [27].
In conclusion, this population-based cohort study of older patients with severe obesity found metabolic bariatric surgery to be associated with improved mortality and prolonged life expectancy. These benefits did not appear to extent to patients of age 70 years or older but were more profound in patients with diabetes. The findings from this study suggests a role for metabolic bariatric surgery as a procedure to prolong life expectancy in older patients with severe obesity.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 29 KB)