Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) Syndrome Following Carbamazepine Use in a Young Male With Psychiatric Comorbidities
Nilar Win, Bianca Afroz Liya, Sadia Arefin

TL;DR
A young man developed a severe drug reaction called DRESS after taking carbamazepine for psychiatric issues, which improved after stopping the drug.
Contribution
This case highlights DRESS syndrome as a rare but serious side effect of carbamazepine in psychiatric patients.
Findings
The patient showed typical DRESS symptoms like fever, rash, and eosinophilia after carbamazepine use.
Stopping the drug and providing supportive care led to clinical improvement.
Lymph node biopsy and imaging confirmed reactive lymphadenopathy consistent with DRESS.
Abstract
Drug reaction with eosinophilia and systemic symptoms (DRESS) is a rare but potentially life-threatening drug-induced hypersensitivity reaction. It is characterized by fever, widespread rash, hematologic abnormalities including eosinophilia, lymphadenopathy, and visceral organ involvement. We report a case of a 25-year-old male who developed DRESS syndrome following initiation of carbamazepine for psychiatric indications. The patient presented with systemic symptoms and a characteristic dermatologic and hematologic profile. Diagnostic workup included lymph node biopsy and imaging, with findings consistent with reactive lymphadenopathy. Prompt recognition and cessation of the offending drug, alongside supportive treatment, led to clinical improvement.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
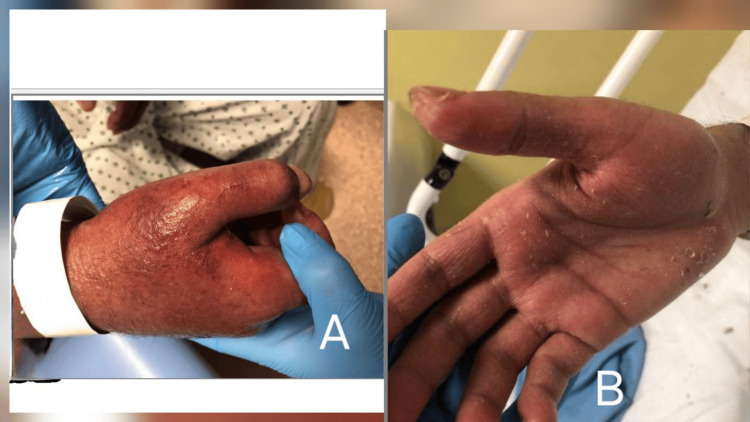 Figure 1
Figure 1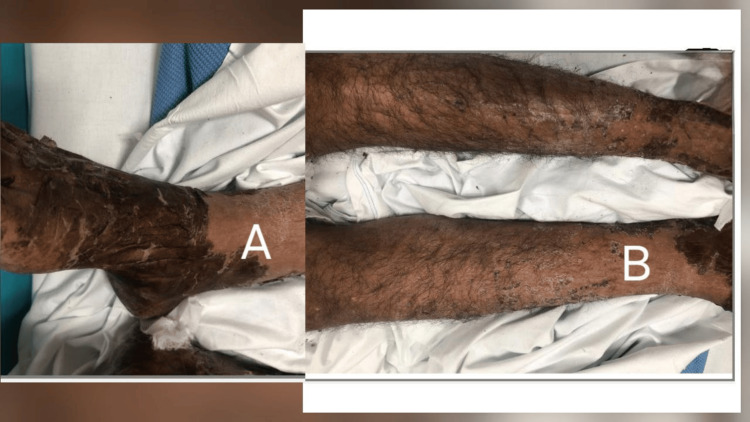 Figure 2
Figure 2| Test | Result | Normal Range |
| White Cell Count | 63 x 109/L | 4-11 x 109/L |
| Hemoglobin | 89 g/L | 130-165 g/L |
| Platelet | 477 x 109/L | 152-450 x 109/L |
| Eosinophils | 8.29 x 109/L | 0-0.4 x 109/L |
| Lymphocytes | 10.8 x 109/L | 1-3 x 109/L |
| C-reactive Protein | 113 mg/L | 0-4.9 mg/L |
| Serum Creatinine | 77 µmol/L | 40-80 µmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Forensic Toxicology and Drug Analysis · Eosinophilic Disorders and Syndromes
Introduction
Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a severe adverse drug reaction with delayed onset, typically occurring two to eight weeks after exposure to the offending medication [1]. It is most frequently associated with aromatic anticonvulsants such as carbamazepine and phenytoin, as well as allopurinol and sulfonamides [2]. The exact pathogenesis remains unclear, but proposed mechanisms include drug-specific immune responses, genetic susceptibility, and viral reactivation [3]. Mortality can reach up to 10%, most commonly due to hepatic failure [4]. Early diagnosis and immediate withdrawal of the causative drug are essential to improve outcomes [5].
Case presentation
A 25-year-old male presented with a one-day history of fever, shortness of breath, pleuritic chest pain, productive cough, and a generalized erythematous, intensely pruritic rash involving the trunk and extremities. He also developed excoriated blistering lesions around the lips, without mucosal ulceration. Past medical history included schizophrenia (recent inpatient admission), asthma, irritable bowel syndrome, attention-deficit/hyperactivity disorder (ADHD), and a history of polysubstance misuse (cannabis, 3,4-methylenedioxymethamphetamine (MDMA), heroin, lysergic acid diethylamide (LSD), and cocaine). Carbamazepine had been recently initiated for behavioural management during his psychiatric admission.
On examination, the patient was febrile (38.1°C), normotensive (BP 134/75 mmHg), and bradycardic (HR 67 bpm). Dermatological examination revealed diffuse erythematous, blistering rash with excoriation affecting the trunk, limbs, and face, with prominent perioral involvement but no mucosal ulceration (Figures 1, 2). Generalized lymphadenopathy was noted, including a palpable right axillary lymph node. Cardiovascular and respiratory examinations were otherwise unremarkable.
Generalized erythematous pruritic rash on the hand (A). Area of dryness and desquamation on the palmar aspect (B).
Desquamation of the lower limbs (A). Erythematous scaly patch with a papule on the anterior aspect of the lower limbs (B).
Early dermatology review suggested a differential diagnosis including Stevens-Johnson syndrome and severe drug reaction. Features of eczema and seborrhoeic dermatitis were also observed. Serial review, exclusion of alternative diagnoses, and histopathology ultimately indicated DRESS syndrome.
Laboratory blood tests demonstrated leukocytosis (WBC 13.4 × 10^9^/L) on admission, peaking at 63 × 10^9^/L before declining with treatment. Marked eosinophilia was noted (peak 8.24 ×10^9^/L, 22% of total WBC). Atypical lymphocytes were present (peak 10.8 ×10^9^/L). CRP was elevated (peak 113 mg/L) and normalized with therapy. Renal function was preserved (creatinine 77 µmol/L), while liver function tests were initially deranged and improved following treatment (Table 1). Thyroid function was within normal limits. Serology for Epstein-Barr virus was negative.
Further investigations, including a core biopsy of a right axillary lymph node, revealed preserved architecture with paracortical expansion, pallor, melanophages, scattered eosinophils, and clusters of Langerhans cells. Immunohistochemistry demonstrated a mixed population of CD4+ and CD8+ T cells, preserved B- and T-cell zones, and reactive germinal centers. These findings were consistent with dermatopathic lymphadenitis and reactive lymphoid hyperplasia.
Based on the patient's presentation of a widespread rash, eosinophilia, systemic involvement, and a recent history of starting carbamazepine, the primary differential diagnosis included DRESS syndrome, which was favored over viral exanthema, Stevens-Johnson syndrome (due to the lack of significant mucosal involvement), and lymphoproliferative disorders (ruled out by lymph node biopsy). Utilizing the European Registry of Severe Cutaneous Adverse Reactions (RegiSCAR) scoring system, the diagnosis was confirmed as DRESS syndrome secondary to carbamazepine.
Carbamazepine was immediately discontinued. The patient was commenced on intravenous hydrocortisone, followed by a tapering course of systemic corticosteroids. Supportive management included antipyretics, antihistamines for pruritus, emollients, and close monitoring of liver and renal function. Dermatology and psychiatry teams were involved throughout.
Following drug withdrawal and corticosteroid therapy, the patient’s fever resolved, and the cutaneous eruption improved. Lymphadenopathy remained stable. The patient continues follow-up with dermatology and psychiatry.
Discussion
DRESS syndrome is a potentially fatal hypersensitivity reaction with a heterogeneous clinical presentation. Carbamazepine is among the most frequently implicated agents [6]. Delayed onset after drug exposure can complicate diagnosis. Hallmark features include fever, rash, eosinophilia, lymphadenopathy, and internal organ involvement, particularly of the liver and kidneys [7].
Diagnosis is primarily clinical, supported by laboratory and histopathological findings. Dermatopathic lymphadenitis, as in this case, is a benign reactive process commonly associated with extensive skin disease and supports the diagnosis of DRESS [4,8]. Prompt discontinuation of the offending agent is essential, and systemic corticosteroids are recommended for significant systemic involvement [1,9]. Multidisciplinary care is critical in patients with complex psychiatric comorbidities to ensure safe management and medication rationalization.
Conclusions
High clinical suspicion for DRESS syndrome should be maintained in patients presenting with rash and systemic symptoms after starting high-risk medications such as carbamazepine. Early recognition, prompt drug cessation, and coordinated multidisciplinary care are crucial to reducing morbidity and improving outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The DRESS syndrome: a literature review Am J Med Cacoub P Musette P Descamps V Meyer O Speirs C Finzi L Roujeau JC 58859712420112159245310.1016/j.amjmed.2011.01.017 · doi ↗ · pubmed ↗
- 2Drug-induced pseudolymphoma and drug hypersensitivity syndrome (drug rash with eosinophilia and systemic symptoms: DRESS)Semin Cutan Med Surg Bocquet H Bagot M Roujeau JC 250257151996906959310.1016/s 1085-5629(96)80038-1 · doi ↗ · pubmed ↗
- 3Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: does a DRESS syndrome really exist?Br J Dermatol Kardaun SH Sidoroff A Valeyrie-Allanore L Halevy S Davidovici BB Mockenhaupt M Roujeau JC 60961115620071730027210.1111/j.1365-2133.2006.07704.x · doi ↗ · pubmed ↗
- 4Drug reaction with eosinophilia and systemic symptoms: a retrospective study of 60 cases Arch Dermatol Chen YC Chiu HC Chu CY 1373137914620102071377310.1001/archdermatol.2010.198 · doi ↗ · pubmed ↗
- 5DRESS syndrome: part I. Clinical perspectives J Am Acad Dermatol Husain Z Reddy BY Schwartz RA 69361468201310.1016/j.jaad.2013.01.03323602182 · doi ↗ · pubmed ↗
- 6Drug reaction with eosinophilia and systemic symptom (DRESS) induced by carbamazepine: a case report and literature review Pan Afr Med J E L omairi N Abourazzak S Chaouki S Atmani S Hida M 918201410.11604/pamj.2014.18.9.3799 PMC 421352325360193 · doi ↗ · pubmed ↗
- 7DRESS syndrome: a literature review and treatment algorithm World Allergy Organ J Calle AM Aguirre N Ardila JC Cardona Villa R 1006731620233708274510.1016/j.waojou.2022.100673 PMC 10112187 · doi ↗ · pubmed ↗
- 8Carbamazepine-induced drug rash with eosinophilia and systemic symptoms (DRESS) syndrome Cureus Mantri N Qasim A Zacharia GS Hoazhe S Patel H 017202510.7759/cureus.91226 PMC 1247668941024927 · doi ↗ · pubmed ↗