Association Between Computed Tomography–Based AI-Derived Body Composition and Survival in Patients With Pancreatic Ductal Adenocarcinoma
Koen J.H. Wijsman, Derk C.F. Klatte, Hani M. Babiker, Aleksander M. Bogdanski, Brandon R. Grossardt, Jeanin E. van Hooft, Monique E. van Leerdam, J. Sven D. Mieog, Alexander D. Weston, Michael B. Wallace, Yan Bi

TL;DR
This study shows that body composition measured via CT scans at PDAC diagnosis is linked to patient survival, suggesting it could help guide treatment decisions.
Contribution
The study identifies specific AI-derived body composition parameters independently associated with survival in pancreatic cancer patients.
Findings
Myosteatosis, sarcopenic obesity, and low subcutaneous adipose tissue are linked to higher mortality in surgically resected PDAC patients.
Lower skeletal muscle density is associated with higher mortality in patients receiving palliative therapy.
Less visceral adipose tissue correlates with higher mortality in untreated PDAC patients.
Abstract
A deeper understanding of the factors influencing survival in patients with pancreatic ductal adenocarcinoma (PDAC) is essential for optimizing treatment strategies. This study investigates the independent association of body composition parameters with overall survival in patients with PDAC. This retrospective multisite cohort study included patients diagnosed with PDAC. Diagnostic computed tomography scans were retrieved, and body composition was evaluated using a validated deep learning-based segmentation algorithm that measured tissue volume and density in a 20 cm vertical abdominal section. A total of 1,666 patients with PDAC were included, 938 male (56.3%) and median age 69 years (interquartile range 61–76). In the subgroup of patients who underwent surgical resection (n = 509), myosteatosis (intramuscular infiltration of adipose tissue; hazard ratio [HR] 1.56, 95% confidence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
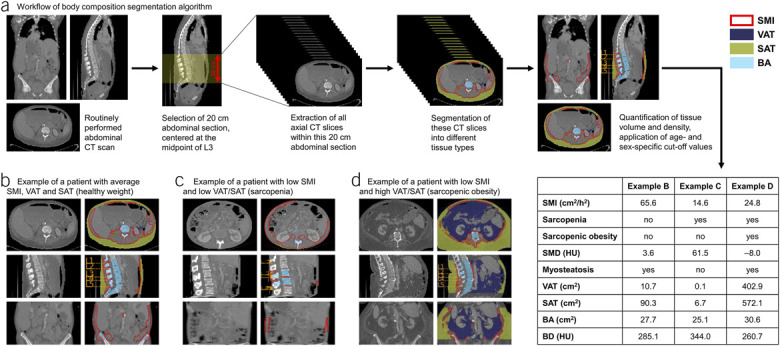 Figure 1
Figure 1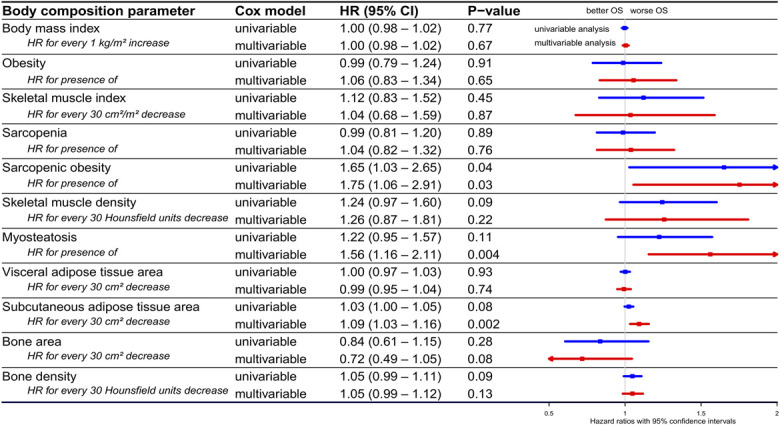 Figure 2
Figure 2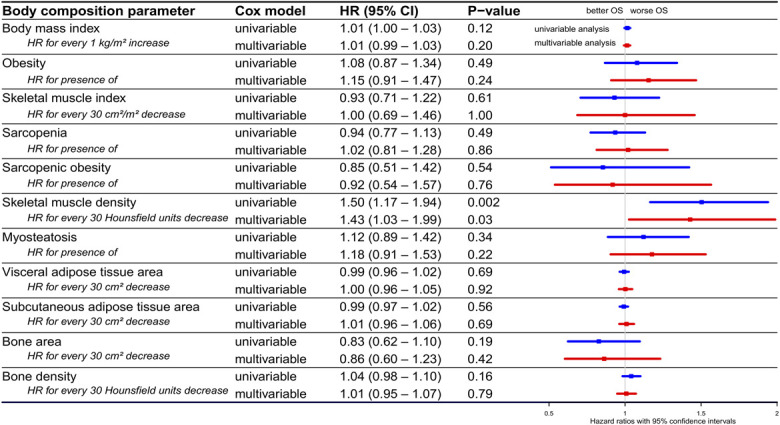 Figure 3
Figure 3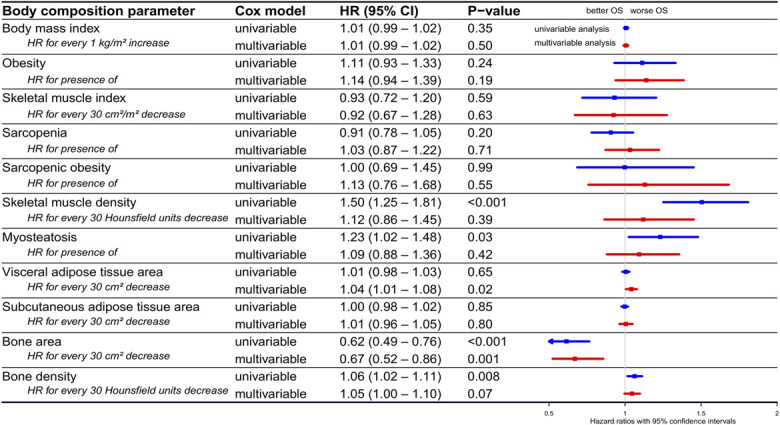 Figure 4
Figure 4- —René Vogels Stichting
- —Prof. dr. A.E. Meinders Fund
- —LUF International Study Fund
- —Professor Chris Gips Foundation
- —Minerva Scholarship Fund
- —CAPER Travel Grant
- —Quintus Fund
- —LUSTRA+ Scholarship
- —Leiden University Trustee Funds
- —ESC Travel Grant
- —KNMG Dick Held
- —Hanarth Fonds
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutrition and Health in Aging · Pancreatic and Hepatic Oncology Research · Inflammatory Biomarkers in Disease Prognosis
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) is among the deadliest cancers, currently the third leading cause of cancer-related deaths in the United States (1), with projections to become the second by 2030 (2). Surgical resection offers the only potential cure, but comes with significant morbidity, a 1.7% mortality rate (3) and a 76.7% recurrence rate, with a median recurrence-free survival of 12 months (4). However, surgery is not an option for most patients because 30%–35% present with locally advanced unresectable disease and 50%–55% with metastatic disease (5). For these patients, palliative chemotherapy is the primary treatment, but their low performance status combined with the substantial burden of treatment leads to 68% of these patients not receiving tumor-targeted treatment (6).
Although surgery can be life-saving and palliative therapy can be life-prolonging, these treatments are often burdensome and do not always yield substantial survival benefits. This underscores the importance of carefully selecting patients who are most likely to benefit from these treatments. Conversely, among patients who do not undergo tumor-targeted treatment and receive best supportive care, identifying those who could still benefit from palliative therapy may offer survival benefits. A better understanding of the factors influencing prognosis in PDAC could aid in personalizing treatment strategies.
Prognosis in PDAC is influenced by both tumor-specific factors and patient-specific factors, such as comorbidities, performance status, and body composition (7). While body composition has traditionally been assessed using body mass index (BMI), this measure is insufficient because it does not differentiate between tissue types. An increasing body of literature recognizes a more comprehensive assessment of abdominal body composition (defined as the quantity and density of skeletal muscle, visceral adipose tissue, subcutaneous adipose tissue, and bone within the abdomen) as an important factor influencing overall survival (OS) in patients with PDAC (8). For instance, sarcopenia (decreased muscle mass) (9–14), sarcopenic obesity (combined presence of sarcopenia and obesity) (7,15–20), myosteatosis (reduced muscle quality because of intramuscular infiltration of ectopic adipose tissue) (19,21–31), high visceral adipose tissue (29,30,32,33), and high subcutaneous adipose tissue (33) have been associated with worse OS. However, studies often yield contradictory results, potentially because of ethnic variability, differences in assessment techniques and cut-off values, and small sample sizes, which limit the generalizability of their findings.
Currently, abdominal body composition is often estimated by segmenting a single computed tomography (CT) slice at the level of the third lumbar vertebra (L3) into different tissue types. However, recent advancements in artificial intelligence now enable a more accurate assessment of body composition across a larger abdominal section (34). This study is among the first to utilize a deep learning-based algorithm to extract 3D abdominal body composition parameters from routinely performed diagnostic CT scans of patients with PDAC. Our objective was to investigate the independent association of body composition parameters with OS, aiming to better understand how these parameters influence the prognosis of patients with PDAC.
METHODS
Study design and population
This retrospective cohort study identified patients (18 years or older) diagnosed with PDAC from 2000 to 2020 at Mayo Clinic sites in Minnesota, Florida, and Arizona. Exclusion criteria were the absence of an abdominal CT scan at the day of or within 1 month before initial clinical PDAC diagnosis, lack of histopathological confirmation of PDAC, and the presence of other synchronous neoplasms. This study was conducted in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines (35). The study was approved by the Mayo Clinic Institutional Review Board (IRB protocol #21-011051).
Data collection
Demographic (age, sex, race/ethnicity), lifestyle (alcohol consumption, smoking status), clinical (Eastern Cooperative Oncology Group [ECOG] performance status, comorbidities), tumor (localization, stage), laboratory (carbohydrate antigen 19-9 [CA19-9]), treatment, and survival data were collected from the Mayo Clinic Cancer Registry and patient medical records. Pre-existing comorbidities were aggregated into a modified version of the Charlson Comorbidity Index (CCI), excluding age, diabetes, and tumor stage because these factors were separately adjusted for in the regression analyses.
Measurement of body composition parameters
Body composition parameters were extracted from diagnostic CT scans using a previously validated deep learning-based segmentation algorithm, which uses a 3-dimensional U-Net Convolutional Neural Network model (Figure 1) that achieved a Dice similarity coefficient of 0.92–0.98 (36). Detailed information on the training, validation, and functionality of the algorithm is outlined in the Supplementary Digital Content (see Supplementary Methods, http://links.lww.com/AJG/D845) and a previous publication (36). The algorithm automatically selects a 20 cm vertical section of the abdomen, centered at the midpoint of the L3 vertebra, and reports the average skeletal muscle area (SMA, cm^2^), visceral adipose tissue area (VAT, cm^2^), subcutaneous adipose tissue area (SAT, cm^2^), and bone area (BA, cm^2^) within this section. To account for differences in stature, SMA was indexed to the patient's height in meters squared, resulting in the skeletal muscle index (SMI, cm^2^/m^2^). Skeletal muscle density (SMD) and bone density (BD) were defined as the average Hounsfield unit (HU) attenuation of all voxels within their respective compartments, with lower HU values indicating lower tissue radiodensity. All abdominal segmentations generated by the body composition algorithm were manually reviewed by an expert (A.D.W.) to ensure accurate segmentation.
Overview of the body composition segmentation algorithm and representative examples of patients. (a) Body composition was derived from CT scans using a segmentation algorithm that automatically selects a 20 cm section of the abdomen, centered at the midpoint of the third lumbar vertebra (L3). Within this section, all axial CT slices are segmented into different tissue types, after which the quantity and density of these tissue types are measured. Skeletal muscle tissue is outlined in red, visceral adipose tissue is colored purple, subcutaneous adipose tissue is colored green, and bone tissue is colored blue. (b) Example of a patient with average SMI, VAT, and SAT (healthy weight). (c) Example of a patient with low SMI and low VAT and SAT (sarcopenia). (d) Example of a patient with low SMI and high VAT and SAT (sarcopenic obesity). BA, bone area; BD, bone density; CT, computed tomography; SAT, subcutaneous adipose tissue area; SMD, skeletal muscle density; SMI, skeletal muscle index; VAT, visceral adipose tissue area.
Definitions of obesity, sarcopenia, sarcopenic obesity, and myosteatosis
Height data (missing for 13 patients, 0.8%) and weight data (missing for 174 patients, 10.4%) were imputed using Multivariate Imputation by Chained Equations. BMI was calculated, and obesity was defined as BMI ≥30 kg/m^2^. Age- and sex-specific cut-off values for sarcopenia (based on SMI) and myosteatosis (based on SMD) were derived from a previous study that used the same abdominal segmentation algorithm to establish reference ranges for CT-based body composition parameters in a population-representative American cohort (see Supplementary Methods and Supplementary Table 1, http://links.lww.com/AJG/D845) (37). SMD below the age-specific and sex-specific threshold serves as a proxy for myosteatosis (decreased muscle quality due to intramuscular infiltration of ectopic adipose tissue), as adipose tissue has a lower radiodensity than muscle tissue (38). Notably, sarcopenia is not limited to individuals of normal or low weight; it also affects overweight individuals. This phenomenon, termed sarcopenic obesity, was defined as the combined presence of sarcopenia and obesity (39).
Statistical analysis
The primary objective of this study was to investigate the association of various CT-based body composition parameters with OS, defined as the time from PDAC diagnosis to death from any cause. Patients who were still alive at the time of analysis were censored at the date of their last recorded contact. Hazard ratios (HRs) for mortality and 95% confidence intervals (CIs) were calculated using univariable and multivariable Cox proportional hazards regression models. To examine the independent association between body composition parameters and OS, separate multivariable analyses were conducted, adjusting each body composition parameter individually for potential confounders (age, sex, race/ethnicity, alcohol consumption, smoking status, ECOG Performance Status, BMI, comorbidities, diabetes, tumor localization, tumor stage, and CA19-9 level). Analyses were performed using both continuous muscle variables (SMI and SMD) and their corresponding dichotomous variables (sarcopenia and myosteatosis). While we recognize that continuous variables provide more detailed information, dichotomous classifications are more intuitive for clinical interpretation. Kaplan-Meier plots were used to estimate cumulative OS, and the log-rank test was performed to compare OS between groups. Statistical analyses were conducted using R (version 4.3.2). All P values were 2-sided, and P < 0.05 was considered statistically significant.
RESULTS
Patient characteristics and body composition parameters
A total of 1,825 patients diagnosed with PDAC were identified from the Mayo Clinic Cancer Registry. Of these, 127 patients were excluded due to the absence of a CT scan within 1 month before diagnosis, and 32 were excluded due to a lack of histopathological confirmation of PDAC. Of the included 1,666 patients, 938 (56.3%) were male, and the median age was 69 years (interquartile range 61–76). Demographic characteristics, clinical characteristics, and body composition parameters of the study population are summarized in Table 1 and Supplementary Digital Content (see Supplementary Table 2, http://links.lww.com/AJG/D845). Sarcopenia was present in 772 patients (46.3%), sarcopenic obesity in 69 patients (4.1%), and myosteatosis in 328 patients (19.7%). A detailed breakdown of the CCI is provided in Supplementary Digital Content (see Supplementary Table 3, http://links.lww.com/AJG/D845). Supplementary Digital Content (see Supplementary Table 4, http://links.lww.com/AJG/D845) summarizes treatment characteristics, including surgery details and margins, chemotherapy, radiotherapy, and treatment sequencing. Supplementary Digital Content (see Supplementary Table 5, http://links.lww.com/AJG/D845) consists of detailed imaging acquisition and reconstruction parameters. The study population was stratified into 3 subgroups based on treatment type: 509 patients (30.6%) who underwent curative-intent surgery, 439 patients (26.4%) who received palliative therapy (i.e., systemic therapy or radiation therapy), and 718 patients (43.1%) who did not undergo tumor-targeted treatment (i.e., best supportive care). Survival outcomes for these subgroups are presented in Supplementary Digital Content (see Supplementary Figure 1, http://links.lww.com/AJG/D845). Further survival analysis was performed separately within these subgroups.
Table 1.: Baseline characteristics and body composition parameters of patients with PDAC by treatment subgroup
Body composition and OS in surgery subgroup
Figure 2 presents the association between body composition parameters and OS in patients with PDAC who underwent surgery. In multivariable analysis, myosteatosis (HR 1.56, 95% CI 1.16–2.11, P = 0.004), sarcopenic obesity (HR 1.75, 95% CI 1.06–2.91, P = 0.03), and lower SAT (HR 1.09 for every 30 cm^2^ decrease, 95% CI 1.03–1.16, P = 0.002) were significantly associated with increased mortality (i.e., worse OS). Kaplan-Meier curves comparing OS based on the presence of sarcopenia, obesity, sarcopenic obesity, and myosteatosis are shown in Supplementary Digital Content (see Supplementary Figure 2, http://links.lww.com/AJG/D845).
Hazard ratios for mortality in patients with PDAC who underwent surgery. Forest plot showing HRs for mortality and their 95% confidence intervals in patients with PDAC who underwent surgery, based on various body composition parameters, determined using univariable (blue lines) and multivariable (red lines) Cox regression analysis. To study the independent association between various body composition parameters and overall survival, separate multivariable analyses were performed with every body composition parameter individually adjusted for potential confounders (age, sex, race/ethnicity, alcohol consumption, smoking status, ECOG performance status, BMI, comorbidities, diabetes, tumor localization, tumor stage, and CA19-9 level). BMI, body mass index; CA19-9, carbohydrate antigen 19-9; CCI, Charlson Comorbidity index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PDAC, pancreatic ductal adenocarcinoma.
Body composition and OS in palliative therapy subgroup
In patients with PDAC who received palliative therapy, lower SMD was significantly associated with worse OS in both univariable analysis (HR 1.50 for every 30 HU decrease, 95% CI 1.17–1.94, P = 0.002) and multivariable analysis (HR 1.43 for every 30 HU decrease, 95% CI 1.03–1.99, P = 0.03; Figure 3). Kaplan-Meier curves based on the presence of sarcopenia, obesity, sarcopenic obesity, and myosteatosis are provided in Supplementary Digital Content (see Supplementary Figure 3, http://links.lww.com/AJG/D845).
Hazard ratios for mortality in patients with PDAC who received palliative therapy. Forest plot showing HRs for mortality and their 95% confidence intervals in patients with PDAC who received palliative therapy, based on various body composition parameters, determined using univariable (blue lines) and multivariable (red lines) Cox regression analysis. To study the independent association between various body composition parameters and overall survival, separate multivariable analyses were performed with every body composition parameter individually adjusted for potential confounders (age, sex, race/ethnicity, alcohol consumption, smoking status, ECOG performance status, BMI, comorbidities, diabetes, tumor localization, tumor stage, and CA19-9 level). BMI, body mass index; CA19-9, carbohydrate antigen 19-9; CCI, Charlson Comorbidity Index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PDAC, pancreatic ductal adenocarcinoma.
Body composition and OS in no tumor-targeted treatment subgroup
In patients with PDAC who did not undergo tumor-targeted treatment, lower VAT (HR 1.04 for every 30 cm^2^ decrease, 95% CI 1.01–1.08, P = 0.02; Figure 4) and greater BA (HR 0.67 for every 30 cm^2^ decrease, 95% CI 0.52–0.86, P = 0.001) were independently related to worse OS in multivariable analysis. Kaplan-Meier curves based on the presence of sarcopenia, obesity, sarcopenic obesity, and myosteatosis are shown in Supplementary Digital Content (see Supplementary Figure 4, http://links.lww.com/AJG/D845). An overview of all multivariable analysis results across all 3 subgroups is presented in Supplementary Digital Content (see Supplementary Figure 5, http://links.lww.com/AJG/D845).
HRs for mortality in patients with PDAC who did not undergo tumor-targeted treatment. Forest plot showing HRs for mortality and their 95% confidence intervals in patients with PDAC who did not undergo tumor-targeted treatment, based on various body composition parameters, determined using univariable (blue lines) and multivariable (red lines) Cox regression analysis. To study the independent association between various body composition parameters and overall survival, separate multivariable analyses were performed with every body composition parameter individually adjusted for potential confounders (age, sex, race/ethnicity, alcohol consumption, smoking status, ECOG performance status, BMI, comorbidities, diabetes, tumor localization, tumor stage, and CA19-9 level). BMI, body mass index; CA19-9, carbohydrate antigen 19-9; CCI, Charlson Comorbidity Index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PDAC, pancreatic ductal adenocarcinoma.
DISCUSSION
This multisite study is the largest to date examining the association between abdominal body composition parameters and OS in various subgroups of patients with PDAC and among the first to apply a deep learning-based 3D approach to routinely performed CT scans. We found that several body composition parameters, such as low SMD, adipose tissue, and sarcopenic obesity, were significantly associated with OS, even after adjusting for potential confounders such as age, ECOG performance status, and tumor stage.
Myosteatosis
Our most notable finding was that either lower SMD, a continuous variable, or myosteatosis, a dichotomous variable derived from SMD, was independently associated with worse OS in patients who underwent surgery or palliative therapy, which is in line with previous literature (19,21–31). In contrast to these findings, other studies did not find this association (17,18,40–42), highlighting the contradictory nature of current research on body composition in patients with PDAC. This lack of generalizability may be due to several factors, including differences in demographic characteristics and patient cohorts. For instance, most of these studies have been conducted within the Asian population (27,28,42) that has a significantly different body composition compared with the Western population (43). In addition, most studies have either focused solely on patients who underwent surgery (18,28,31) or patients with locally advanced or metastatic disease (7,19,20). Importantly, only a few studies adjusted for comorbidities using the Charlson Comorbidity Index (CCI) (16,23,44), World Health Organization (WHO) Performance Status (30), Eastern Cooperative Oncology Group (ECOG) Performance Status Scale (27), American Society of Anesthesiologists (ASA) Classification (45), or specifically for diabetes mellitus (21,31), despite these being important confounders in the relationship between body composition and OS (46).
Myosteatosis is characterized by excessive fat accumulation within skeletal muscle (47), while skeletal muscle normally contains only minimal amounts of adipose tissue (48). Both skeletal muscle and adipose tissue are considered secretory organs, with myocytes producing myokines and adipocytes producing (proinflammatory) adipokines, which are supposed to maintain a balance (49,50). The increase in adipocytes (producing proinflammatory adipokines) seen in myosteatosis is believed to disrupt this balance, leading to systemic inflammation (51), which may contribute to several negative outcomes such as cachexia, tumor progression, and tumor proliferation (52). Clinical studies in patients with PDAC corroborate this theory, showing that patients with low SMD have lower levels of albumin (19,31) and higher levels of inflammatory blood markers (19), both indicators of systemic inflammation. There are 2 possible explanations for the observed association between myosteatosis and OS. First, myosteatosis may be a manifestation of the systemic effects of PDAC itself, serving as an indicator of disease progression. In this case, myosteatosis reflects the systemic impact of PDAC rather than being an independent driver of worse outcomes. Second, patients who already have myosteatosis—because of factors such as lifestyle, comorbidities, or metabolic dysfunction—may have a predisposition to worse outcomes, independent of PDAC.
Subcutaneous and visceral adipose tissue
Our study also found that lower SAT (in the surgery subgroup) and lower VAT (in the no tumor-targeted treatment subgroup) were associated with worse OS. Although several smaller studies have investigated the association between SAT and OS in patients with PDAC (18,22,30–33,42,44,53–55), this association has only been observed in a Chinese cohort of patients with irresectable pancreatic cancer (HR 1.31 for high SAT, 95% CI 1.01–1.69, P = 0.05 in univariable analysis) (33). Similarly, of all studies examining the association between VAT and OS in patients with PDAC (15,18,20,22,29–33,42,44,45,53–58), only 4 have found a significant association (29,30,32,33). The lack of consistency in these findings may be attributed to the same factors mentioned earlier. A recent study from our group found that both SAT and VAT significantly decreased over time in CT scans up to 36 months before PDAC diagnosis (59). This finding suggests that patients with low SAT and VAT at the moment of diagnosis may have experienced more adipose tissue loss before diagnosis, possibly reflecting a more advanced disease stage that leads to worse OS.
Sarcopenia and sarcopenic obesity
Interestingly, we did not observe an association between low SMI (i.e., sarcopenia) and OS in our cohort, despite several meta-analyses linking sarcopenia to worse OS in patients with PDAC, and similar sarcopenia rates in our study (9–14). However, the combined presence of sarcopenia and obesity (i.e., sarcopenic obesity) was associated with worse OS in the subgroup of patients with PDAC who underwent surgery. This finding is consistent with previous research (7,10,15–20,29), although other studies did not observe this association (23,30,54,57). Chronic systemic inflammation caused by obesity might contribute to worse OS (60), similar to the inflammation caused by myosteatosis. Furthermore, obesity has been linked with major complications after pancreatic surgery (61,62), which could explain why sarcopenic obesity was associated with worse OS specifically in the surgery subgroup.
Bone area
In addition, we found that greater BA was strongly associated with worse OS in the subgroup of patients who did not undergo tumor-targeted treatment, which is an unexpected finding that remains unexplained. This observation seems to contradict our previous research, which used the same body composition segmentation algorithm on the same cohort of patients to study prediagnostic changes and found a 10% decrease in BA in the 6 months before PDAC diagnosis (59). According to this trend, one would expect that patients with lower BA at the time of diagnosis have more advanced disease and therefore worse OS, rather than patients with greater BA. While bone metastases might explain this finding, they occur in only about 10% of patients with PDAC and typically lead to altered bone density rather than increased BA (63). Although this finding could be due to chance, the observed association was relatively strong (P < 0.001 in univariable and P = 0.001 in multivariable analysis), with a notably higher HR compared with other treatment groups, suggesting that this finding may not be entirely random. BA showed only a weak Pearson correlation (r < 0.1) with other body composition parameters that were significantly associated with OS, indicating that the observed association is unlikely to be driven by correlations with another body composition parameter. To better understand this phenomenon, it would be valuable to explore not only the temporal changes in BA before diagnosis but also how BA evolves after diagnosis as the disease progresses.
Strengths
Our study has several strengths, including its large sample size, extensive adjustment for potential confounders (such as ECOG performance status, comorbidities, clinical factors, and CA19-9), and comprehensive body composition assessment. Only a recent study by Keyl et al. used a similar deep learning-based algorithm with a 3-dimensional approach in patients with PDAC, but focused solely on muscle tissue in patients with advanced disease (25). While our method of measuring body composition across a 20 cm vertical section of the abdomen is more comprehensive than estimating body composition from a single CT slice at the L3 level, most previous literature on body composition is based on single-slice assessment, limiting comparability with novel methods like ours. Furthermore, the established cut-off values for myosteatosis and sarcopenia are based on SMD and SMI at L3 (64,65). Because SMD and SMI vary across the abdomen, these cut-off values are less applicable to our body composition measurement approach (66). To overcome this challenge, we used the reference ranges reported by Weston et al (37) who applied the same abdominal segmentation algorithm to characterize CT-based body composition in a population-representative American cohort. For future studies using a similar measurement approach as ours, we advocate for using the same reference ranges to ensure consistency and comparability.
Limitations
Next to the limited comparability with older research, our study has several other limitations. First, owing to its retrospective design, selection bias cannot be entirely ruled out. Our cohort primarily consisted of non-Hispanic White patients, which may limit the generalizability of our findings to other populations. Furthermore, although we stratified our cohort by treatment type, we did not account for detailed treatment information such as type of surgery or chemotherapy regimens. Despite being the largest study to date, further subdividing our cohort could lead to smaller subgroups with insufficient statistical power. In addition, while we assessed morphological muscle parameters (SMI and SMD) using CT scans, we could not evaluate actual muscle quality or strength through clinical tests because of the study's retrospective nature. Although imaging-based muscle quality relates to actual strength (67), clinical tests could provide more precise insights.
Future directions and clinical implications
A promising next step after this study would be to develop and validate a prediction model for PDAC prognosis at the time of diagnosis. Such a model could integrate demographic and clinical information, tumor characteristics, laboratory results, and CT-based body composition parameters. This could aid in risk stratification, personalized treatment planning, and early identification of patients who may benefit from more or less aggressive treatment. In addition, further investigation into how body composition parameters evolve after PDAC diagnosis, and their relationship to outcomes such as chemotherapy response and toxicity, could deepen our understanding of the role of body composition in PDAC. Prospective studies combining nutritional, exercise, and metabolic interventions are warranted to determine whether improving muscle quality or mitigating myosteatosis translates into better tolerance to therapy and survival (68,69). Although small-scale studies suggest that such programs may improve SMI and SMD, their impact on survival outcomes remains to be established (70,71).
Conclusion
In conclusion, our study found that body composition parameters, such as low SMD, adipose tissue, and sarcopenic obesity, are independently associated with worse OS across various subgroups of patients with PDAC. Given that CT imaging is routinely performed for diagnostic and staging purposes, these parameters can be readily extracted using a deep learning-based algorithm. Future research should explore the clinical implications of these body composition parameters for treatment planning.
CONFLICTS OF INTEREST
Guarantors of the article: Koen J.H. Wijsman, MD, MSc; Yan Bi, MD, PhD.
Specific author contributions: K.J.H.W., D.C.F.K., M.B.W., Y.B., J.E.v.H., M.E.v.L., A.D.W.: conceptualization. K.J.H.W., D.C.F.K., A.D.W.: data curation. K.J.H.W., A.D.W.: formal analysis. K.J.H.W., M.B.W., Y.B., J.E.v.H., M.E.v.L.: funding acquisition. K.J.H.W.: investigation. K.J.H.W., D.C.F.K., M.B.W., Y.B., J.E.v.H., M.E.v.L., A.D.W., B.R.G.: methodology. K.J.H.W.: project administration. M.B.W., Y.B.: resources. K.J.H.W., A.D.W.: software. D.C.F.K., M.B.W., Y.B., J.E.v.H., M.E.v.L.: supervision. K.J.H.W., B.R.G.: validation. K.J.H.W.: visualization. K.J.H.W.: writing—original draft. D.C.F.K., M.B.W., Y.B., J.E.v.H., M.E.v.L., A.D.W., B.R.G., A.M.B., H.M.B., J.S.D.M.: writing—review and editing.
Financial support: K.J.H.W.: received grants from the René Vogels Foundation, Nijbakker-Morra Foundation, Prof. dr. A.E. Meinders Fund, LUF International Study Fund, Professor Chris Gips Foundation, Minerva Scholarship Fund, CAPER Travel Grant, Quintus Fund, LUSTRA+ Scholarship, Leiden University Trustee Funds, ESC Travel Grant, KNMG Dick Held, and Hanarth Foundation. The funding sources had no involvement in the study design; collection, analysis, and interpretation of data; writing of the report; or decision to submit the article for publication. The research was conducted independently by the authors.
Potential competing interests: J.E.v.H. reported receiving lecture fees from Cook Medical, Boston Scientific, Fujifilm, and Falk, as well as a consultancy fee from Olympus Medical, all outside the submitted work. M.B.W. reported consulting for Boston Scientific, CDX Diagnostics, ClearNote Health, Cosmo Pharmaceuticals, Digma Medical, Endostart, Endiatix, Fujifilm, Medtronic, Surgical Automations, Ohelio Ltd, Venn Bioscience; research grants from Fujifilm, Boston Scientific, Olympus, Medtronic, Cosmo Intelligent Medical Devices; stock/stock options in Virgo Inc., Surgical Automation; consulting on behalf of Mayo Clinic for Boston Scientific, Microtek; all outside the submitted work. All other authors report no potential conflicts of interest.Study HighlightsWHAT IS KNOWN
- ✓ Pancreatic ductal adenocarcinoma (PDAC) has a poor prognosis, with a 5-year survival rate of only 5%.
- ✓ A better understanding of the factors influencing prognosis in PDAC could support more personalized treatment approaches.
- ✓ Cancer prognosis is influenced by both tumor-related and patient-related factors, including body composition.
- ✓ Computed tomography-derived body composition parameters have been associated with survival outcomes in various cancers.
- ✓ Previous studies on computed tomography-based body composition and survival in patients with PDAC have reported inconsistent results. WHAT IS NEW HERE
- ✓ This multisite study is the largest to date investigating the association between body composition parameters and overall survival in patients with PDAC.
- ✓ It is among the first to apply a deep learning-based 3D approach to quantify body composition in this patient population.
- ✓ Several body composition parameters, such as low skeletal muscle density, adipose tissue, and sarcopenic obesity, were significantly associated with overall survival, even after adjustment for potential confounders.
- ✓ Evaluating body composition at the time of diagnosis could enhance clinical decision-making and enable more personalized treatment strategies.
Supplementary Material
**
**
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL Giaquinto AN Jemal A. Cancer statistics, 2024. CA Cancer J Clin 2024;74(1):12–49.38230766 10.3322/caac.21820 · doi ↗ · pubmed ↗
- 2Rahib L Wehner MR Matrisian LM . Estimated projection of US cancer incidence and death to 2040. JAMA Netw Open 2021;4(4):e 214708.33825840 10.1001/jamanetworkopen.2021.4708 PMC 8027914 · doi ↗ · pubmed ↗
- 3Kokkinakis S Kritsotakis EI Maliotis N . Complications of modern pancreaticoduodenectomy: A systematic review and meta-analysis. Hepatobiliary Pancreat Dis Int 2022;21(6):527–37.35513962 10.1016/j.hbpd.2022.04.006 · doi ↗ · pubmed ↗
- 4Groot VP Rezaee N Wu W . Patterns, timing, and predictors of recurrence following pancreatectomy for pancreatic ductal adenocarcinoma. Ann Surg 2018;267(5):936–45.28338509 10.1097/SLA.0000000000002234 · doi ↗ · pubmed ↗
- 5Park W Chawla A O’Reilly EM. Pancreatic cancer: A review. JAMA. 2021;326(9):851–62.34547082 10.1001/jama.2021.13027 PMC 9363152 · doi ↗ · pubmed ↗
- 6Mackay TM Latenstein AE Augustinus S . Implementation of best practices in pancreatic cancer care in the Netherlands: A stepped-wedge randomized clinical trial. JAMA Surg 2024;159(4):429–37.38353966 10.1001/jamasurg.2023.7872 PMC 10867778 · doi ↗ · pubmed ↗
- 7Dalal S Hui D Bidaut L . Relationships among body mass index, longitudinal body composition alterations, and survival in patients with locally advanced pancreatic cancer receiving chemoradiation: A pilot study. J Pain Symptom Manage 2012;44(2):181–91.22695045 10.1016/j.jpainsymman.2011.09.010PMC 3990439 · doi ↗ · pubmed ↗
- 8Borga M West J Bell JD . Advanced body composition assessment: From body mass index to body composition profiling. J Invest Med 2018;66(5):1–9.