Surgical Management of Adult-Onset Artery From the Pulmonary Artery (ALCAPA): A Narrative Review of Surgical Techniques
Chandler Pugh, Kristina Snoddy, Erin Reid, Adam Witcher

TL;DR
This paper reviews surgical techniques for treating a rare heart condition called ALCAPA in adults, focusing on how to best restore normal blood flow to the heart.
Contribution
The paper provides a comprehensive review of surgical strategies for adult-onset ALCAPA, highlighting new techniques and their potential.
Findings
Direct reimplantation of the left coronary artery into the aorta is preferred when feasible.
The Takeuchi procedure is an alternative when reimplantation is not possible but has associated risks.
New techniques like modified Cabrol and modified Takeuchi show promise but need further research.
Abstract
Anomalous left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital coronary anomaly in which the left coronary artery originates from the pulmonary artery, resulting in myocardial ischemia due to coronary steal after postnatal reduction in pulmonary artery pressure. Most patients present in infancy with heart failure, but a subset survives into later childhood or adulthood through extensive collateralization from the right coronary artery. Late presenters typically demonstrate a dilated, tortuous right coronary artery with retrograde flow into the pulmonary artery. Surgical correction is recommended at all ages; however, optimal management in older patients remains debated. This review summarizes the existing literature and discusses surgical strategies for adult-onset ALCAPA. Surgical repair of adult-onset ALCAPA aims to eliminate coronary steal and restore a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
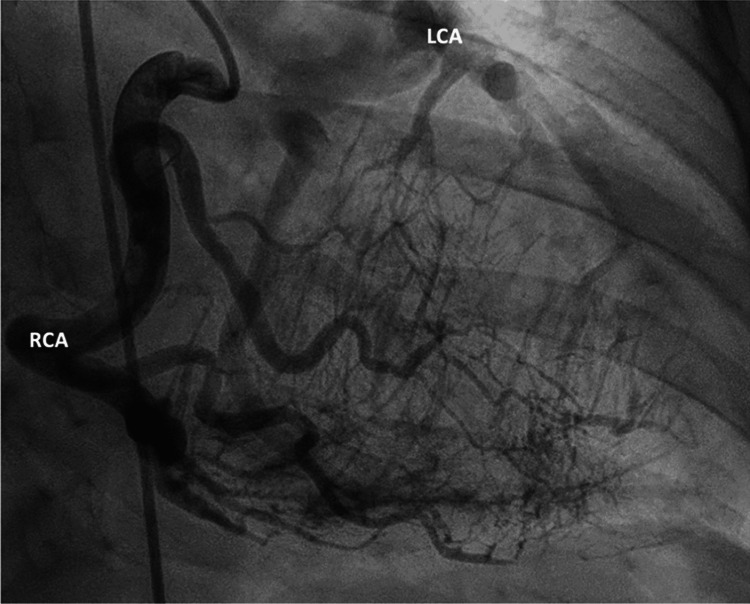 Figure 1
Figure 1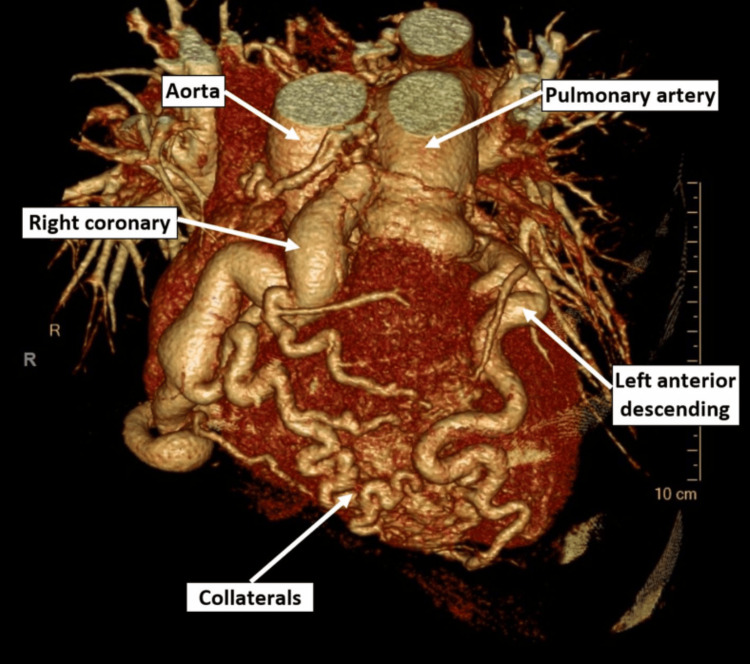 Figure 2
Figure 2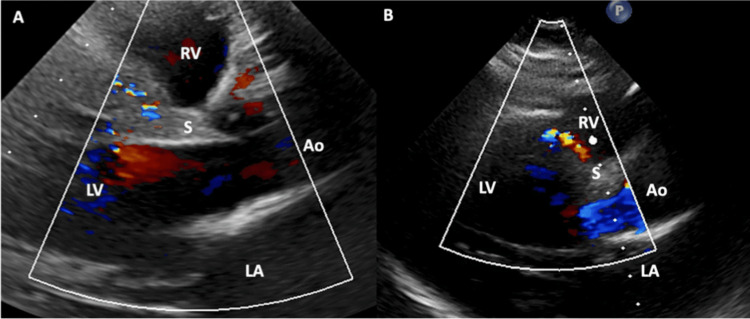 Figure 3
Figure 3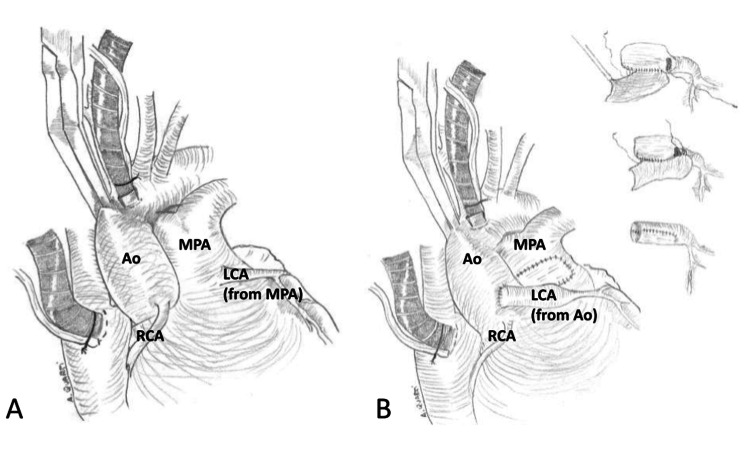 Figure 4
Figure 4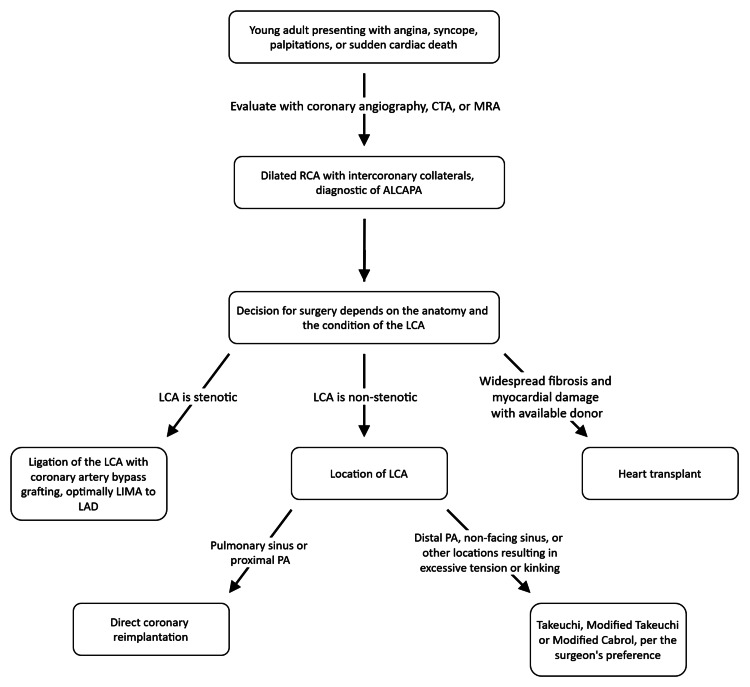 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Tracheal and airway disorders · Congenital Heart Disease Studies
Introduction and background
Anomalous left coronary artery from the pulmonary artery (ALCAPA), also known as Bland-White-Garland syndrome, is a rare congenital anomaly presenting in approximately 1 in 300,000 live births and accounts for 0.25-0.5% of congenital heart defects [1,2]. The abnormal origin of a coronary artery from the pulmonary artery was first reported by Brooks in 1882; however, a comprehensive clinical description of the condition was not published until 1933 by Bland, White, and Garland, who described the syndrome in association with cardiac hypertrophy [3,4]. ALCAPA is most commonly an isolated cardiac defect. Still, it can occur in combination with atrial septal defect, ventricular septal defect, patent ductus arteriosus, tetralogy of Fallot, aorto-pulmonary window, and coarctation of the aorta [5]. The pathophysiology of ALCAPA likely begins embryonically, with abnormal separation of the conotruncus into the aorta and pulmonary artery (PA) or from persistence of the pulmonary buds and involution of the aortic buds, which eventually form the coronary arteries [6].
While ALCAPA most commonly presents in infants, approximately 10-15% of patients survive into adulthood due to well-developed collateral circulation from the right coronary artery (RCA) to the left coronary artery (LCA) [7]. This robust collateralization prevents the typical infantile presentation, though these patients remain at risk for myocardial ischemia, left ventricular dysfunction, mitral regurgitation, and ventricular arrhythmias [6]. Both infant-type and adult-type presentations are characterized by ischemic cardiomyopathy due to inadequate left ventricular perfusion; however, the clinical presentation varies widely across age groups [6,8].
In infants, ischemia is typically acute, with symptoms including crying during feeding, failure to thrive, tachypnea, cyanosis, fatigue, and colic [8,9]. In the neonatal period, when pulmonary artery pressure remains elevated near systemic levels, the anomalous left coronary artery receives relatively well-oxygenated blood at adequate pressure from the pulmonary artery, transiently protecting against severe ischemia. As pulmonary vascular resistance falls during the first weeks of life, pulmonary artery pressure decreases to approximately one-half of systemic pressure within 24 hours and continues to decline to one-third or less by 2 weeks of age. The LCA now receives only deoxygenated blood at low pressure from the pulmonary artery, which is insufficient for adequate myocardial perfusion [10]. Collateral vessels develop from the right coronary artery to supply the left ventricular territory, but because pulmonary artery pressure is lower than left ventricular pressure, blood flows retrograde from the left ventricular myocardium through these collaterals and drains into the low-pressure pulmonary artery, resulting in coronary steal [8,9,11]. This creates a left-to-right shunt at the coronary level, diverting blood away from myocardial perfusion and causing severe left ventricular ischemia, myocardial infarction, and heart failure, precipitating acute decompensation in infancy [12].
In adults, survival is established by robust collateralization from the RCA, but coronary steal persists, and cardiomyopathy is thus chronic. Patients often present with dyspnea, angina, palpitations, arrhythmias, syncope, and rarely sudden cardiac death, rather than acute systolic heart failure in infants [13]. Cardiomegaly, mitral regurgitation, and vastly dilated collateral arteries are often present [14]. Among adults, the average age of presentation is 41, but it is highly variable. Patients who are more physically active may present earlier, but ALCAPA can present as late as 75 years of age [15,16].
This paper will focus on the adult presentation of ALCAPA and will serve to examine surgical techniques for adult ALCAPA patients. Direct reimplantation, the Takeuchi procedure, coronary artery bypass grafting (CABG) with left internal mammary artery (LIMA) ligation, and the modified Cabrol technique will be reviewed. Among these, direct reimplantation is the most frequently performed and generally preferred approach, followed by the Takeuchi and CABG approaches.
Review
Pathophysiology and diagnosis
In normal anatomy, the LCA arises from the aortic trunk superiorly to the left cusp of the aortic valve [17]. However, in ALCAPA, the LCA arises from the PA rather than the aortic arch and can have several possible origins [18]. Most commonly, the LCA arises from the left-facing sinus of the main pulmonary artery (MPA), or more rarely from the right-facing or non-facing sinus [19-21]. While origin from the pulmonary sinus is the most common pathology in around half of cases, the LCA can also arise from the MPA (41.66% of cases) and the right pulmonary artery (8.3% of cases) [22]. The origin of the LCA does not usually alter symptomatology; rather, it plays an important role in determining the surgical approach, which will be discussed later.
Adult ALCAPA is almost universally characterized by a dilated and tortuous RCA with well-developed intercoronary collaterals, features that are not present in the infantile form [16,20]. A dilated and tortuous RCA is shown in Figure 1. Despite the development of robust collateral vessels, RCA-derived flow cannot provide adequate long-term perfusion due to progressive coronary steal into the low-pressure PA. Once demand exceeds the capacity of the collaterals, symptoms will emerge [23]. Many patients thus present with an acute myocardial infarction due to progressive coronary steal and undergo an invasive coronary evaluation, which reveals the diagnosis of ALCAPA [16]. However, ALCAPA can also be diagnosed incidentally in patients who undergo a transthoracic echocardiogram (TTE) or electrocardiogram (ECG) for unrelated reasons [6].
Angiogram of an adult patient with ALCAPA.Angiogram demonstrating the typical findings of angiography in adult patients with ALCAPA, a dilated and tortuous right coronary artery with intercoronary collaterals. There is retrograde filling of the left coronary artery via collateral branches from the right coronary artery, and the left coronary artery originates from the main pulmonary artery [24].Reproduced from Stolz et al., Clinical Research in Cardiology (2025), distributed under the Creative Commons Attribution 4.0 International (CC BY 4.0) license.
Per the 2025 American Heart Association Guidelines, coronary angiography, computed tomography angiography (CTA), and cardiac magnetic resonance imaging (CMRI) are the recommended methods for evaluating an anomalous coronary artery in adults to demonstrate a dilated and tortuous RCA. CTA is generally preferred for superior resolution (Figure 2), although CMR may provide adequate imaging of the PA and pulmonary sinus. Coronary angiography by catheterization can be helpful when there is concern about coronary artery stenosis [25]. TTE and ECG, while not recommended by official guidelines, can be diagnostic and are non-invasive. Diagnostic findings on TTE (Figure 3) include retrograde blood flow from the LCA to the PA and a dilated, tortuous RCA. Intracoronary collaterals may be demonstrated on color Doppler [26]. Other findings may include mitral regurgitation, dilated collateral coronary arteries, ventricular dysfunction, and increased echogenicity of the papillary muscles [27]. ECG findings include Q waves, ST depressions, and T-wave changes in the anterolateral leads I, AVL, V5, and V6 [28].
Cardiac CTA of a patient with ALCAPA.Cardiac CTA demonstrates collaterals from the right coronary artery to the left ventricle [29].Reproduced from Liu et al., CJC Open (2023), distributed under the Creative Commons Attribution (CC BY) license.
Echocardiography with Color Doppler in a patient with ALCAPA.A: Abnormal septal TTE color Doppler signal due to an excessive septal collateral system seen in ALCAPA [24].B: Abnormal septal TTE color Doppler signal due to an excessive septal collateral system seen in ALCAPA [24].Ao: Aorta; LA: Left Atrium; LV: Left Ventricle; RV: Right Ventricle; S: Interventricular SeptumReproduced from Stolz et al., Clinical Research in Cardiology (2025), distributed under the Creative Commons Attribution 4.0 International (CC BY 4.0) license.
The treatment approach for patients with ALCAPA, whether discovered acutely or incidentally, is surgery [25]. However, in older adults, particularly those who are asymptomatic or those with low-risk anatomy, such as in the absence of stenosis, a conservative approach may be considered due to the increased risks associated with surgery [16,25].
Methods
A narrative literature review was performed using PubMed, MEDLINE, and Google Scholar databases. Search terms included combinations of “ALCAPA,” “anomalous left coronary artery,” “adult ALCAPA,” “late-presenting ALCAPA,” “Takeuchi repair,” “coronary reimplantation,” “coronary artery bypass grafting,” and “Cabrol technique.” Only English-language publications were included.
Eligible studies consisted of adult and adolescent case reports, case series, retrospective cohort studies, and systematic reviews describing surgical management strategies, perioperative outcomes, and long-term follow-up. Pediatric-only cohorts were excluded unless they provided comparative insight relevant to adult surgical decision-making.
Extracted variables included patient age at diagnosis, presenting symptoms, coronary anatomy and site of anomalous origin, imaging modalities utilized, operative technique employed, postoperative complications, and survival or functional outcomes. Given the rarity of late-presenting ALCAPA and the heterogeneity of available data, formal meta-analysis was not feasible. Findings were therefore synthesized qualitatively, with emphasis on reproducible surgical principles and outcome trends.
Surgical techniques
Direct Reimplantation
Direct reimplantation of the anomalous LCA from the PA into the aorta reestablishes the normal two-coronary system, as demonstrated in Figure 4. The ascending aorta and MPA are dissected free from surrounding tissues to ensure full mobilization and avoid injury to the LCA. The MPA is transected, and the LCA is carefully detached from the pulmonary root with a generous cuff of surrounding arterial wall tissue to preserve the integrity of the ostium. The proximal LCA is mobilized toward its bifurcation to ensure adequate length for tension-free reimplantation. A neo-ostium is then created in the left coronary sinus of the aorta. The LCA is reimplanted end-to-end into the neo-ostium using a running 6-0 polypropylene suture, beginning at the deepest point and proceeding bilaterally to complete the anastomosis. The defect in the PA root is reconstructed with a non-treated autologous pericardial patch using a continuous 6-0 polypropylene suture, ensuring restoration of pulmonary root structure. The repair is completed with continuous closure of the pulmonary patch margins, ensuring hemostasis and restoration of normal great vessel alignment [30].
Diagram of direct coronary reimplantation in a patient with ALCAPA.A: Anatomy present in a patient with ALCAPA [31].B: The creation and relocation of the conduit (see right) as part of direct coronary reimplantation [31].Ao: Aorta; LCA: Left Coronary Artery; MPA: Main Pulmonary Artery; RCA: Right Coronary ArteryAdapted from Quarti et al., Case Reports in Medicine (2009), distributed under the Creative Commons Attribution (CC BY) license.
Limitations of the direct reimplantation technique include feasibility based on anatomy. Direct reimplantation is limited in stenotic or fibrosed LCAs, which are often unmanipulable [20]. In other scenarios, the LCA may originate from a site difficult to access during the procedure, such as a distal location on the PA, from the lateral wall of the PA, or the non-facing pulmonary sinus. Performing direct reimplantation when the LCA arises from these locations can result in excessive tension or distortion due to the larger distance between the anomalous LCA and the aorta [32-34]. In such cases, coronary artery elongation techniques can be utilized with direct reimplantation, or other methods can be considered [35,36].
Takeuchi Method
Dr. Takeuchi et al. in 1979 established an innovative approach to establishing a dual-coronary system without direct coronary translocation by creating an intrapulmonary tunnel that redirects oxygenated blood from the aorta to the anomalous LCA, thereby restoring myocardial perfusion. This technique is a suitable alternative when direct reimplantation of the LCA onto the aorta is not feasible due to anatomical constraints [37]. A transverse incision is made just below the bifurcation of the PA to determine the origin of the LCA accurately. Following aortic cross-clamping, antegrade cardioplegia is administered while manually compressing the LCA ostium to ensure optimal myocardial protection. A box-shaped incision is then fashioned in the anterior wall of the MPA. Simultaneously, an inverse “L”-shaped aortotomy is performed. The PA flap and the adjacent aortic wall are then excised in a face-to-face manner to facilitate the creation of an aortopulmonary window. This connection establishes a direct pathway for oxygenated blood from the aorta to reach the intrapulmonary tunnel. The PA flap is then positioned to fully enclose the LCA orifice, with special care to extend coverage beyond the posterior commissure. The anterior wall of the PA is subsequently reconstructed using an autologous pericardial patch. This refined version of the procedure reflects technical advances and long-term refinements since Takeuchi's original description, while preserving the core principle of rerouting aortic blood into the anomalous LCA [32].
The Takeuchi technique avoids direct manipulation of the LCA to avoid kinking or excess stress on the LCA and restores normal coronary circulation via an intrapulmonary baffle [38,39]. The technique avoids direct manipulation, allowing its use in older patients with less vessel mobility and in those with a narrowed (but not occluded) LCA [39,40]. Limitations of the Takeuchi technique include PA stenosis around the baffle, baffle leaks or obstructions, and a high reoperation rate due to baffle leaks and PA stenosis [39,41-43].
However, modifications to the Takeuchi technique have been pioneered to reduce the risk of baffle leaks, chiefly by altering the shape or material of the baffle or reinforcing the tunnel. Such procedures are known as the modified Takeuchi method [44]. The baffle can be adapted with synthetic materials such as Gore-Tex or autologous pericardial patches to reduce leaks and improve outcomes [41,45].
Coronary Artery Bypass Grafting (CABG)
Coronary artery bypass grafting should be considered in patients without a patent LCA, as in those with coronary artery disease, or when the anatomy is not suitable for either direct reimplantation or the Takeuchi procedure [46,47]. CABG is performed via ligation of the abnormal LCA from the pulmonary artery with coronary revascularization using a LIMA graft to the LAD.
Early attempts at surgical correction of ALCAPA included the use of saphenous vein grafts to restore coronary perfusion. In 1977, eight patients received saphenous vein grafts, which remained patent for the 8-year monitoring period [48]. Similar positive findings have been replicated with other studies demonstrating resolution of angina for 2-8 years [48-50]. The benefits include feasibility when anatomy is not suitable for direct repair, a good early safety profile, restoration of dual coronary circulation, and improved long-term graft patency when arterial conduits are used compared to venous conduits [27,46,49]. The risks include perioperative mortality due to massive infarcts, long-term graft failure, which is increased with venous grafts, and an overall limited scope of evidence. There is also concern for the maturation of an arterial graft to the distally bilateral vessel with major collaterals from the RCA and the long-term patency of vein grafts in a young population [19]. Additionally, redo surgeries and complex reoperations carry an increased risk [51]. While CABG can be effective in select ALCAPA cases, its use should be tailored to patient-specific factors, with careful weighing of risks and benefits to ensure the best possible outcomes.
Modified Cabrol Technique
The modified Cabrol technique has been reported in a case study where anatomical constraints prevented direct reimplantation. Therefore, a polytetrafluoroethylene (PTFE) graft was chosen to reduce anatomical stress caused by distance and vessel orientation. PTFE is a more rigid material than traditional Dacron, which can decrease the likelihood of graft kinking when the vessel length is inadequate. Modified Cabrol was successful on a one-year follow-up and was thus deemed successful [19]. More research will likely be needed to determine its place in the future of ALCAPA repairs; however, it has considerable potential.
Heart Transplant
An orthotopic heart transplant has not been extensively performed in ALCAPA. In a case study, a 46-year-old woman with symptomatic New York Heart Association (NYHA) functional classification Class IV heart failure underwent orthotopic heart transplant. She returned to full functional status [52]. Thus, a heart transplant can be useful in ALCAPA when irreversible myocardial damage has occurred, assuming there are donors available. Further research would be needed to validate this case study, but it does hold promise for a rare diagnosis and presentation.
Surgical decision making in the patient with ALCAPA
When approaching the patient with ALCAPA, the decision on which surgical technique to use should primarily be based on the anatomy, as shown in our suggested algorithm in Figure 5.
Our suggested algorithm for the surgical approach to a patient with ALCAPA (anomalous left coronary artery from the pulmonary artery).CTA: Computed Tomography Angiography; MRA: Magnetic Resonance Angiography; RCA: Right Coronary Artery; ALCAPA: Anomalous Left Coronary Artery from the Pulmonary Artery; LCA: Left Coronary Artery; LIMA: Left Internal Mammary Artery; LAD: Left Anterior Descending (Artery); PA: (Pulmonary Artery)
If the LCA originates from the pulmonary sinus or from the proximal PA, direct coronary reimplantation is recommended, as this technique restores normal coronary anatomy and physiology [31,53]. However, origins from the non-facing pulmonary sinus or the lateral wall of the PA are likely to be more technically challenging due to the larger distance between the anomalous LCA and the aorta in adult patients. In such cases, direct reimplantation remains preferred, with coronary artery elongation techniques used as needed [35,36].
If the LCA is more distal on the PA, direct reimplantation can result in excessive tension or distortion of the LCA; thus, in such cases, the Takeuchi technique should be considered [32-34]. If the LCA is fibrosed or stenotic, CABG is preferred, as the LCA is unlikely to be amenable to manipulation, and bypassing around the abnormal vessel is preferred [20]. If the patient has widespread fibrosis with NYHA Class IV heart failure and a donor is available, transplantation can be considered, though evidence is extremely limited [52]. Conservative therapy can be considered in an elderly, asymptomatic patient with favorable anatomy [16,25].
Conclusions
Despite the rarity of adults presenting with ALCAPA, its surgical management requires excessive surgical planning and consideration. Various vessel patterning and general myocardial viability should be considered when planning the intervention strategy. Additionally, early intervention is essential, especially in young patients, as untreated ALCAPA may result in sudden cardiac death. The surgical management of adult-onset ALCAPA remains a complex case-by-case challenge, but clinical guidelines have become clearer with time.
Direct reimplantation remains the gold standard when anatomically suitable. However, when anatomical limitations exist, various alternative procedures should be considered, including the Takeuchi method, the modified Takeuchi method, the modified Cabrol technique, CABG, and heart transplant. Regarding both the modified Takeuchi method and the modified Cabrol technique, further research will be necessary to assess their validity and value in adult ALCAPA repair. Tailored surgical strategies at specialized centers offer the best outcomes with close follow-up. As collective experience grows, procedural selection and clinical guidelines will continue to improve. However, further research is needed to evaluate options beyond direct reimplantation, especially in patients with anatomical limitations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The anomalous origin of the left coronary artery from the pulmonary artery Br Heart J KEJD 1491612119591365150010.1136/hrt.21.2.149PMC 1017563 · doi ↗ · pubmed ↗
- 2Anomalous origin of left coronary artery from pulmonary artery: A rare cause of myocardial infarction in children J Family Community Med Lardhi AA 1131161720102135902010.4103/1319-1683.74319 PMC 3045108 · doi ↗ · pubmed ↗
- 3Two cases of an abnormal coronary artery of the heart arising from the pulmonary artery: with some remarks upon the effect of this anomaly in producing cirsoid dilatation of the vessels J Anat Physiol Brooks HS 2629201885 https://pubmed.ncbi.nlm.nih.gov/17231608/PMC 128853417231608 · pubmed ↗
- 4Congenital anomalies of the coronary arteries: Report of an unusual case associated with cardiac hypertrophy Am Heart J Bland EF White PD Garland J 78780181933
- 5Management of anomalous left coronary artery from the pulmonary artery Circulation Arciniegas E Farooki ZQ Hakimi M Green EW 09621980 https://pubmed.ncbi.nlm.nih.gov/6967375/6967375 · pubmed ↗
- 6Anomalous left coronary artery from the pulmonary artery (ALCAPA) diagnosed in adulthood: Varied clinical presentation, therapeutic approach and outcome Int J Cardiol Boutsikou M Shore D Li W 495326120182954853710.1016/j.ijcard.2018.02.082 · doi ↗ · pubmed ↗
- 7Anomalous origin of the left coronary artery from the pulmonary artery (Bland-White-Garland syndrome) in adult patients: Long-term follow-up after surgery Am Heart J Moodie DS Fyfe D Gill CC 3813881061983686922110.1016/0002-8703(83)90207-7 · doi ↗ · pubmed ↗
- 8Early presentation of patients with abnormal origin of left coronary artery from the pulmonary artery is a predictor of poor mid-term outcomes Pediatr Cardiol El-Louali F Lenoir M Gran C 7197254320223479739510.1007/s 00246-021-02777-w PMC 8602883 · doi ↗ · pubmed ↗