Rate and Characteristics of Frequent Attenders at Primary Healthcare Centres in Muscat Governorate, Oman: A cross-sectional study
Manar Al Sanaa Ali AlZeedi, Najlaa Jaafar Mohammed, Fatma Al Hadhrami, Hadya Al Lawati, Muna Aal Talib, Rahma Al Riyami, Rahma Al Shuhaimi, Wiam Al Tuqi

TL;DR
The study finds that a small percentage of patients in Oman's primary healthcare centers visit very frequently, often due to mental illness and chronic conditions, suggesting a need for targeted interventions.
Contribution
This study identifies sociodemographic and clinical factors associated with frequent attendance in primary healthcare in Muscat, Oman.
Findings
Frequent attenders constituted 1.1% of patients but accounted for 6.9% of all visits.
Mental illness was the strongest predictor of frequent attendance.
26.2% of frequent attenders persisted in high utilization across two consecutive years.
Abstract
Frequent attenders (FAs) are patients who use primary healthcare centre (PHC) services at disproportionately high rates which puts a strain on health systems and affects the quality of care. This study aimed to determine the prevalence of FAs in PHCs in Muscat Governorate, Oman, and to identify their demographic, socioeconomic and clinical characteristics. This cross-sectional study was conducted across 10 randomly selected PHCs in Muscat from January to December 2024. Data were collected retrospectively from electronic medical records for 2023. FAs were defined as individuals with 10 or more visits per year. Descriptive statistics and multivariate Poisson regression were used to identify factors associated with frequent attendance. A total of 83,749 visits by 41,017 adult patients were analysed. FAs constituted 1.1% of patients (95% confidence interval: 0.95–1.15%) and accounted for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
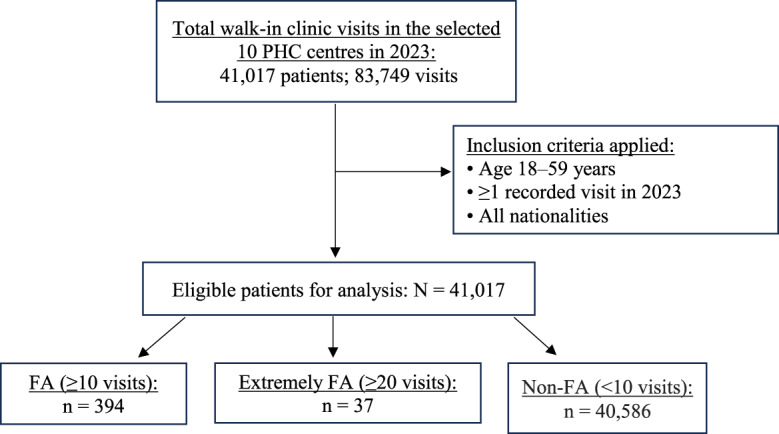 Fig. 1
Fig. 1| Characteristic | n (%) |
|---|---|
|
| |
| Male | 215 (49.9) |
| Female | 216 (50.1) |
|
| |
| Mean ± SD | 35.58 ± 10.58 |
| Median (range) | 35.0 (18–59) |
|
| |
| Wataya | 22 (5.1) |
| Wadi Kabir | 36 (8.4) |
| South Mabela | 140 (32.5) |
| AL Khudh | 56 (13.0) |
| North Khuwair | 12 (2.8) |
| Amerat | 21 (4.9) |
| Hai Aljami | 40 (9.3) |
| Ansab | 39 (9.0) |
| Muscat | 27 (6.3) |
| Hajer | 38 (8.8) |
|
| |
| Single | 64 (36.6) |
| Married | 107 (61.1) |
| Divorced | 3 (1.7) |
| Widow | 1 (0.6) |
|
| |
| Not educated | 34 (57.6) |
| Secondary | 8 (13.6) |
| High education | 17 (28.8) |
|
| |
| No | 88 (38.8) |
| Yes | 139 (61.2) |
|
| |
| No | 243 (59.4) |
| Yes | 166 (40.6) |
|
| |
| No | 306 (84.3) |
| Yes | 57 (15.7) |
|
| |
| No | 357 (89.7) |
| Yes | 41 (10.3) |
|
| |
| No | 82 (19.0) |
| Yes | 349 (81.0) |
|
| |
| No | 329 (76.3) |
| Yes | 102 (23.7) |
|
| |
| No | 325 (75.4) |
| Yes | 106 (24.6) |
|
| |
| No | 426 (98.8) |
| Yes | 5 (1.2) |
|
| |
| No | 312 (72.4) |
| Yes | 119 (27.6) |
|
| |
| No | 245 (56.8) |
| Yes | 186 (43.2) |
|
| |
| No | 325 (75.4) |
| Yes | 106 (24.6) |
|
| |
| No | 398 (92.3) |
| Yes | 33 (7.7) |
|
| |
| No | 234 (54.3) |
| Yes | 197 (45.7) |
|
| |
| No | 242 (56.1) |
| Yes | 189 (43.9) |
|
| |
| No | 318 (73.8) |
| Yes | 113 (26.2) |
|
| |
| No | 245 (56.8) |
| Yes | 186 (43.2) |
| Variable | Number of visits, median (IQR) or correlation coefficient | |
|---|---|---|
|
| ||
| Male | 12.0 (10.0–14.0) | 0.144 |
| Female | 12.0 (10.0–14.0) | |
|
| r = –0.014 | 0.774 |
|
| ||
| Single/separated | 14.0 (12.0–19.75) | <0.001 |
| Married | 12.0 (11.0–15.0) | |
|
| ||
| Uneducated | 21.0 (13.0–27.25) | <0.001 |
| Educated (secondary or above) | 12.0 (10.0–13.5) | |
|
| ||
| Not employed | 14.0 (10.25–18.75) | <0.001 |
| Employed | 12.0 (10.0–14.0) | |
|
| ||
| No | 11.0 (10.0–13.0) | <0.001 |
| Yes | 13.0 (11.0–16.0) | |
|
| ||
| No | 12.0 (10.0–14.0) | <0.001 |
| Yes | 14.0 (12.0–21.5) | |
|
| ||
| No | 12.0 (10.0–14.0) | 0.503 |
| Yes | 12.0 (11.0–14.0) | |
|
| ||
| No | 12.0 (10.0–14.0) | 0.323 |
| Yes | 12.0 (10.0–14.0) | |
|
| ||
| No | 12.0 (10.0–14.0) | 0.390 |
| Yes | 12.0 (10.0–13.0) | |
|
| ||
| No | 12.0 (10.0–14.0) | 0.278 |
| Yes | 12.0 (10.0–15.0) |
| Parameter (n = 203) | Beta coefficient (95% CI) | OR (95% CI) | |
|---|---|---|---|
| Gender – male (reference: female) | –0.082 (–0.160 to –0.005) | 0.921 (0.853 to 0.995) | 0.037 |
| Employment – yes (reference: no) | –0.060 (–0.151 to 0.030) | 0.941 (0.860 to 1.030) | 0.190 |
| Chronic disease – yes (reference: no) | 0.148 (0.056 to 0.240) | 1.160 (1.057 to 1.271) | 0.002 |
| Mental illness – yes (Reference: no) | 0.400 (0.298 to 0.502) | 1.491 (1.347 to 1.652) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Systems and Reforms · Primary Care and Health Outcomes · Chronic Disease Management Strategies
1. Introduction
Frequent attenders (FAs) are patients who make a high number of healthcare visits. They account for approximately 2–15% of all attendees at primary healthcare centres (PHCs), yet they represent 25–50% of total clinic visits. This significantly impacts the efficiency, accessibility and quality of health services for other patients.^12^ Various definitions of FAs exist, with numerous systematic studies conducted to characterise this population and determine interventions that effectively reduce their overutilisation of healthcare resources.^345^ The most commonly accepted definition in primary care is either being in the top 10^th^ percentile of clinic visits or making ≥10 visits within a 12-month period.^36^ The concept of frequent attendance was first introduced in 1954 by Backett et al. who observed that a small group of patients accounted for the majority of a physician's workload in general practice settings.^7^
A longitudinal study in Australia found that FAs accounted for 33.4% of primary healthcare consultations at baseline, with persistent FAs accounting for 15.5% of consultations over three data collection waves, assessed every four years.^8^ Persistent frequent attendance was associated with gender, depression, physical conditions, disability and medication use.^8^ Similarly, a study conducted at a family practice centre in Kuwait found that 5.8% of patients accounted for 19.2% of all visits, with a median of 16 visits per FA.^9^ Interestingly, only 45.5% of FAs presented with symptoms. High attendance was strongly linked to chronic illnesses and sociodemographic factors such as nationality, gender, age and employment type.^9^ A recent mixed-methods study conducted in the UK in 2022 found that FAs often visited clinics for personal, emotional and mental health reasons.^1^ From the FAs' perspectives, clinics were viewed as sources of information and medical support, with primary care physicians perceived as authoritative and knowledgeable figures and nurses as treatment managers and intermediaries. In contrast, healthcare staff reported more negative than positive perceptions when describing their interactions with FAs.^1^
In Oman, there are limited data regarding the characteristics and underlying factors driving frequent attendance, hindering the development of effective management strategies. A retrospective longitudinal study conducted in Ad Dakhiliyah Governorate in 2018 found that FAs constituted only a small proportion of PHC visits.^10^ The overall mean number of visits per patient per year was 3.2 ± 3.3, with a median of 2 visits, indicating that the governorate has a low-utilisation rate.^10^ However, these results cannot be generalised as the study only covered the Ad Dakhiliyah Governorate. This study aimed to determine the rate of FAs at PHCs in Muscat Governorate, which would provide a more comprehensive picture. Such findings will hopefully aid in the development of a clear and practical definition of FAs within the context of the primary healthcare system in Oman. Additionally, this study sought to identify the demographic, socioeconomic and health-related characteristics of FAs in order to better understand factors contributing to frequent attendance. These results would support the development of recommendations to more effectively manage FAs, thereby enhancing the efficiency and quality of primary healthcare services in Muscat.
2. Methods
This cross-sectional study was conducted from January to December 2024 across primary healthcare centres (PHCs) under the Ministry of Health in Muscat Governorate, Oman. The sampling frame included all 32 PHCs in the governorate, which are distributed across 6 administrative wilayats (districts).
A total of 10 PHCs were selected using stratified random sampling to ensure proportional representation across different wilayats. The stratification was based on both wilayat and patient volume, defined as the total number of patient visits recorded in 2022. It also considered the population size and catchment area for each centre. Within each stratum, PHCs were randomly chosen. The selected health centres included: Al Amerat Health Center, Al Hajer Health Center, Al Khudh Health Center, Ansab Health Center, Hai Aljami Health Center, North Al Khuwair Health Center, South Mabela Health Center, Muscat Health Center, Wattayah Health Center and Wadi Kabeer Health Center. Stratified random sampling was employed to ensure proportional representation of PHCs across wilayats.
Data were retrospectively extracted from the Al-Shifa electronic health record system for the full calendar year of 2023. Only adult patients aged 18–60 years were included in the study and only visits to walk-in clinics were analysed. Visits to clinics designated as specialised appointment clinics were excluded from the analysis along with visits from paediatric and elderly age groups.
For this study, FAs were defined as having 10 or more visits within 12 months.^36^ This definition is based on widely accepted international thresholds. Using this absolute cut-off allows for practical comparability across different studies and prevents the misclassification of patients with only 3 to 4 visits as FAs, which would have occurred if a relative definition (such as the 90^th^ percentile) was used in a population such as that of Oman.^10^
A structured data collection sheet was used to gather information from Al-Shifa electronic medical records. These included demographic characteristics (gender and age), socioeconomic characteristics (marital status, educational level and employment status) and health-related variables (known to have chronic diseases, mental illness or disability condition). Data were also collected on healthcare utilisation, including the total number of visits over the 2-years, reasons for visits, clinical diagnoses recorded during visits and whether a sick leave certificate was issued. Visit reasons were categorised as follows: acute conditions (short-term medical issues such as infections, injuries or sudden onset symptoms); continuous care (visits related to follow-up or ongoing management of known chronic diseases) and systemic issues (encounters related to administrative matters that are not directly linked to a new or ongoing clinical complaint, such as laboratory or referral follow-up, medication refill and medical reports). The analysis of visit reasons was based on a patient-level classification. That is, if a FA had any visits during the year that fell under a particular category above, they were counted only once in that category. This approach was chosen to summarise the variety of reasons for visits among FAs, rather than to quantify the proportions of different visit types across all encounters. All data collectors were physicians tasked with extracting data from the health record system, ensuring consistency and accuracy in the data collection process.
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) software, Version 30.0 (IBM Corp., Armonk, New York, USA). Categorical variables were presented as frequencies and percentages, while continuous variables were described as mean ± standard deviations or medians and ranges. Due to the non-normal distribution of the studied outcome data, crude associations between frequent attendance and various factors were assessed using a Mann-Whitney U test and Spearman's correlation coefficient. For the multivariate analysis, Poisson regression was performed, including all factors with P values of <0.25 in the crude analysis. Variables with substantial missing data were not entered into the multivariate regression analysis. A P value of <0.05 was considered statistically significant.
3. Results
A total of 83,749 visits to the selected PHCs by 41,017 individual patients in 2023 were analysed [Fig. 1]. The average number of visits per day was 229.45. The mean number of visits per person per year was 2.04 ± 1.94, with a median of 1 visit (range: 1–58 visits/person/year). More than half of the patients (53.3%, n = 21,862) made only a single visit in 2023, while 46.7% (n = 19,155) made more than one visit. Overall, 431 patients were classified as FAs, accounting for 1.1% of the study population (95% confidence interval: 0.95–1.15%), with a total of 5,785 visits, representing 6.9% of all visits. Among FAs, the mean number of visits per year was 13.42 ± 5.54, with a median of 12.0 (range: 10–58 visits/person/year). A total of 37 FAs (8.6%) were categorised as extremely frequent attenders, defined as those with ≥20 visits per year.
Flowchart showing this study's selection process. PHC = primary healthcare centre; FA = frequent attender.
There was a relatively even distribution of male and female FAs (49.9% versus 50.1%). The PHC with the largest proportion of FAs was South Mabela (32.5%, n = 140), followed by Al Khudh (13.0%, n = 56) and Hai Aljami (9.3%, n = 40). The mean age was 35.58 ± 10.58 years old (range: 18–59 years). Most FAs were married (61.1%, n = 107), uneducated (57.6%, n = 34) and unemployed (61.2%, n = 88). Chronic diseases, mental illnesses and disabilities were reported in 40.6%, 15.7% and 10.3% of FAs, respectively. Regarding the reason for clinic visits (81.0%, n = 349) were related to acute conditions (23.4%, n = 189) to continuous care and (43.9%, n = 325) to systemic issues. In addition, (43.2%, n = 186) of FAs sought sick leave. The most common diagnoses included respiratory diseases (43.2%, n = 186), musculoskeletal (MSK) disorders (27.6%, n = 119) and gastrointestinal diseases (24.6%, n = 106). Overall (26.2%, n = 113) of FAs in 2023 remained FAs in 2024, indicating persistent attendance behaviour over time [Table 1].
The crude analysis indicated that the median number of PHC visits per person per year was significantly higher among FAs compared to non-FAs (14 versus 12 visits; P <0.001). Marital status, education level, employment status, chronic diseases and mental illnesses were all significantly associated with frequent attendance (P <0.001 each). Specifically, uneducated individuals had a higher median number of visits than educated individuals (21 versus 12 visits; P <0.001), while unemployed individuals had a higher median number of visits than employed individuals (14 versus 12 visits; P <0.001). Similarly, individuals with chronic diseases (13 versus 11 visits; P <0.001) and mental illnesses (12 versus 14 visits; P <0.001) exhibited higher median numbers of visits than their respective counterparts. No significant associations were observed between PHC visit frequency and other FA characteristics, such as gender, age, diagnosis or sick leave-seeking behaviour [Table 2].
In the multivariate regression analysis, gender, along with chronic diseases and mental illnesses, emerged as significant independent predictors of frequent attendance. Specifically, male patients had 0.082 fewer visits than females (P = 0.037). Unemployment also resulted in an increase of 0.060 visits, although this was not statistically significant (P = 0.190). The presence of chronic diseases (P = 0.002) and mental illnesses (P <0.001) increased the number of visits by 0.148 and 0.400, respectively [Table 3].
4. Discussion
The frequency of PHC visits varies considerably, with most individuals making 1–2 visits per year.^1112^ The number of visits tends to be higher among certain patient populations, including older adults, women and those with chronic diseases.^1213^ Research consistently shows that FAs in primary care make up 2–15% of patients but account for 25–50% of all visits. This highlights the significant impact that these patients have on the workload and resource allocation in primary care.^113^
The current study focused on identifying FAs among patients attending walk-in clinics for adults aged 18 to 60 years, excluding paediatric and elderly patients, as well as those with appointments for specialised clinics to treat chronic medical conditions. FAs accounted for 1.1% of all patients attending walk-in clinics at PHCs in Muscat in 2023, accounting for 6.9% of all visits. This rate is notably lower than the 2.5% reported in a previous study conducted in Ad Dakhiliyah Governorate in 2018, where FAs contributed to 10.7% of total visits. Nonetheless, this concentration of utilisation among a minority of patients reflects a consistent pattern across settings and underscores the importance of identifying and addressing the needs of this FAs group to optimise healthcare delivery.
In general, comparing average rates of FAs between different studies is challenging due to differences in how an FA is defined and in the research inclusion criteria used. In the current study, extremely frequent attenders accounted for 8.6% of all FAs. Although this percentage may seem low, it is relatively high compared to other studies. For instance, in a UK general practice, patients with 20 or more visits per year represented less than 1% of the total patient population;^14^ a finding echoed in the Danish observational study.^15^
The current study also revealed considerable variation in attendance rates among different PHCs in Muscat. These differences are likely due to factors such as population density, accessibility, service quality and patient preferences. For instance, the South Mabela Health Center had the highest proportion of FAs at 32.5%, followed by Al Khudh (13.0%) and Hai Aljami (9.3%), all of which are located in Seeb wilayat, an area characterised by high population density, rapid urban development and a younger, mobile population. In contrast, Al Hajer and Al Amerat PHCs—despite serving large catchment areas—had relatively lower FA proportions (8.8% and 4.9%, respectively), which may reflect factors such as limited accessibility, longer waiting times, perceived quality differences or the availability of alternative facilities in nearby wilayat such as Mutrah.
Gender plays a significant role in the frequency of healthcare visits, with females tending to seek medical care more often than males.^16^ Several factors contribute to this trend; female patients are more likely to report symptoms, experience a higher burden of illness and assume caregiving roles for children, which can affect their own health.^917^ This finding aligns with results from other studies conducted in the Ad Dakhiliyah region of Oman, Kuwait and Norway.^91018^ Notably, the current study showed that the effect of gender only became statistically significant in the multivariate regression model, suggesting that gender differences in attendance patterns become more apparent when controlling for other variables such as chronic diseases and mental health conditions. Moreover, the findings indicate that the majority of FAs were married (61.1%), uneducated (57.6%) and unemployed (61.2%). These sociodemographic patterns are consistent with previous studies suggesting that low educational attainment and unemployment are associated with higher primary care utilisation.^1920^ Additionally, married individuals may seek care more often due to family responsibilities, increased reproductive consultations, perceived social norms or greater health awareness prompted by spouses.^21^
The current study also showed that 40.6% of FAs had chronic diseases, 15.7% had mental illnesses and 10.3% had disabilities. Other studies have similarly shown that depressive and somatoform disorders are among the strongest predictors of FA.^22^ Previous research has found that FAs in primary healthcare settings have significantly higher rates of mental illness compared to routine attenders, reaching up to 54%.^23^ The lower rate noted in the current study could be due to under-reporting, stigma or differences in healthcare-seeking behaviour within the patient population. More research is needed to further explore these factors. Conversely, the rate of physical disability observed in the current study is comparable to findings from other settings. One study found that 14.9% of persistent FAs had a disability, compared to only 1.6% of non-FAs.^24^ Disabilities may indirectly lead to frequent health facility visits by fostering a sense of control over one's environment and contributing to lower socioeconomic status.^2526^ Importantly, chronic conditions, disabilities and mental illnesses are major needs-based factors that influence how often patients visit healthcare facilities.^25^ In the current study, patients with chronic conditions or mental illnesses made significantly more frequent visits compared to other FAs. These findings support the need for a person-centred approach in primary care that considers social determinants of health and emphasises building patient capacity and self-efficacy.
Reports show that 68–85% of FAs have at least one chronic physical illness, with many experiencing multiple conditions.^2728^ Respiratory conditions were the most frequently recorded diagnoses in the current study (43.2%) which aligns with prior Gulf region research.^929^ This pattern may reflect limited use of community pharmacies or self-care measures, highlighting the need for improved health education and public reassurance strategies. Similarly, MSK diagnoses were also common (27.6%). Often, these visits are not due to the severity of the condition, but rather to functional limitations, chronic pain syndromes or psychosomatic factors, particularly in the context of concurrent mental health issues. Incorporating physiotherapy into PHC services and educating patients about chronic pain could help reduce repeat visits for these complaints.
Visit patterns among FAs in this study were influenced by a mix of medical, behavioural and systemic factors, with most visits for acute issues, followed by systemic concerns and continuity of care. Similar patterns have been observed in prior studies from Oman, Kuwait, Singapore, and the UK.^1910^ Although acute conditions are often self-limiting, they contribute to high utilisation of PHCs, indicating possible gaps in self-management and a distrust of alternative care models. To reduce the burden on PHCs and improve preventive care, initiatives like home-based guidance and teleconsultation can triage non-urgent cases. The traditional model of primary care as the main provider for acute illnesses is changing, with a reported one-third reduction in acute care visits to primary care practices from 2002 to 2015.^30^
One of the most critical findings in this study is the high proportion of FAs who sought care for non-clinical reasons, with 75.4% of visits related to systemic issues. Previous research shows that many FA visits are due to bureaucratic demands rather than clinical necessity.^1^ These figures highlight that administrative processes, rather than medical needs alone, are a primary driver of frequent utilisation which emphasises the need for administrative reforms, such as simplifying digital access to reports, decentralising sick leave approvals and expanding non-physician roles in documentation and coordination.
In the current study, over 1 in 4 FAs showed sustained high service utilisation for 2 consecutive years. This aligns with research from Australia, where 20–30% of FAs maintained patterns over years, with a small group accounting for significant healthcare usage.^8^ Similarly, UK studies show that while many FAs are temporary, a core group with complex health and social needs remains consistent.^3^ Monitoring FAs and predictive modelling could help identify at-risk individuals early. A strategic focus on prevention and personalisation could shift care from a reactive model to anticipatory, coordinated healthcare delivery.
This study was subject to several limitations. A significant concern is the high proportion of missing data for key sociodemographic variables, such as marital status, education level and employment status, due to these fields not being mandatory in electronic medical records. This substantial rate of missing data may introduce selection bias, particularly if patients with incomplete records differ systematically from those with complete data. Consequently, the associations between FA and sociodemographic factors may be underestimated or biased. To mitigate this, multivariate regression analysis was conducted. Additionally, incomplete records may have affected visit counts and diagnoses accuracy which could lead to misclassification or underreporting of conditions. To minimise this risk, data collection was carried out by trained physicians. The research was limited to a random selection of PHCs in Muscat Governorate, making the findings less applicable to other regions of Oman.
5. Conclusion
This study identified key clinical and sociodemographic factors driving frequent attendance at PHCs in Muscat, including female gender, chronic illness, mental health conditions and social vulnerability. A significant number of visits were for administrative reasons, not just clinical care. Targeted interventions, such as streamlined administration, patient education and remote care, are needed to reduce unnecessary visits and improve care delivery. Simultaneously, access to mental health services should be expanded through integrated care models, telepsychiatry and enhanced mental health training for primary care staff. These reforms will not only lead to improved resource allocation and service delivery but also align with the goals of Oman Vision 2040. Future research should focus on incorporating patient perspectives to create healthcare solutions that are more responsive, equitable and sustainable.
Authors' Contribution
Manar Al Sanaa Ali AlZeedi: Supervision, Conceptualization, Methodology, Investigation, Writing-Original Draft, Writing - Review & Editing. Najlaa Jaafar Mohammed: Conceptualization, Investigation, Writing - Original Draft. Fatma Al Hadhrami: Investigation, Writing - Original Draft. Hadya Al Lawati: Methodology, Investigation, Writing - Original Draft. Muna Aal Talib: Investigation, Writing - Original Draft. Rahma Al Riyami: Conceptualization, Investigation, Writing - Original Draft. Rahma Al Shuhaimi: Investigation, Writing - Original Draft. Wiam Al Tuqi: Investigation, Writing - Original Draft.
Acknowledgement
The authors would like to acknowledge Mr. Mohammed Al Shidhani, IT Technician, for his support in the initial phase of data collection.
Ethics Statement
Ethical approval for this study was obtained from the Regional Research and Ethical Committee of the Directorate General of Health Services, Ministry of Health, Muscat Governorate, Oman (MH/DGHS/DPT/179/2024)
Generative AI Declaration
This manuscript was revised using Grammarly's AI tool and OpenAI's ChatGPT (GPT-4) for improved grammar and clarity. These tools assisted solely with language editing, while all scientific content, data analysis, interpretations and conclusions were developed by the authors.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sharabani R Kagan I Cojocaru S. Frequent attenders in primary health care: a mixed-methods study of patient and staff perspectives. J Clin Nurs 2023; 32:7135–46. https://doi.org/10.1111/jocn.1677210.1111/jocn.1677237264682 · doi ↗ · pubmed ↗
- 2Kontopantelis E Panagioti M Farragher T Munford LA Parisi R Planner C Consultation patterns and frequent attenders in UK primary care from 2000 to 2019: a retrospective cohort analysis of consultation events across 845 general practices. BMJ Open 2021; 11:e 054666. https://doi.org/10.1136/bmjopen-2021-05466610.1136/bmjopen-2021-05466634930742 PMC 8718478 · doi ↗ · pubmed ↗
- 3Shukla DM Faber EB Sick B. Defining and characterizing frequent attenders: systematic literature review and recommendations. J Patient Cent Res Rev 2020;7:255–64.https://doi.org/10.17294/2330-0698.174710.17294/2330-0698.174732760757 PMC 7398628 · doi ↗ · pubmed ↗
- 4Smits FT Wittkampf KA Schene AH Bindels PJ Van Weert HC. Interventions on frequent attenders in primary care. A systematic literature review. Scand J Prim Health Care 2008; 26:111–116. https://doi.org/10.1080/0281343080211299710.1080/0281343080211299718570010 PMC 3406646 · doi ↗ · pubmed ↗
- 5Vedsted P Christensen MB. Frequent attenders in general practice care: a literature review with special reference to methodological considerations. Public Health 2005; 119:118–37. https://doi.org/10.1016/j.puhe.2004.03.00710.1016/j.puhe.2004.03.00715694959 · doi ↗ · pubmed ↗
- 6Smits FT Mohrs JJ Beem EE Bindels P Jvan Weert HC. Defining frequent attendance in general practice. BMC Fam Pract 2008; 9:21. https://doi.org/10.1186/1471-2296-9-2110.1186/1471-2296-9-2118412954 PMC 2373296 · doi ↗ · pubmed ↗
- 7Backett EM Heady JA Evans JC. Studies of a general practice. II. The doctor's job in an urban area. Br Med J 1954; 1:109–115. 10.1136/bmj.1.4854.109PMC 208440713106492 · doi ↗ · pubmed ↗
- 8Pymont C Butterworth P. Longitudinal cohort study describing persistent frequent attenders in Australian primary healthcare. BMJ Open 2015; 5:e 008975. https://doi.org/10.1136/bmjopen-2015-00897510.1136/bmjopen-2015-00897526443661 PMC 4606421 · doi ↗ · pubmed ↗