Primary Vaginal Epithelioid Haemangioendothelioma with Pulmonary Metastasis: A case report and review of the literature
Anwar Al Shuaili, Huda Kashoob, Zahida Niaz, Nausheen Yaqoob, Khadhra Ahmed J. Galaal, Reem Ahmed Al Mazrouai

TL;DR
A rare case of vaginal cancer called epithelioid haemangioendothelioma is reported, with metastasis to the lungs and challenges in diagnosis.
Contribution
This is the first reported case of primary vaginal epithelioid haemangioendothelioma.
Findings
The patient had primary vaginal EHE that metastasized to the lungs.
The case highlights diagnostic challenges in distinguishing EHE from epithelioid angiosarcoma.
Molecular confirmation is emphasized for accurate diagnosis of this rare malignancy.
Abstract
Epithelioid haemangioendothelioma (EHE) is a rare vascular sarcoma of intermediate malignancy. In 2023, a 31-year-old female presented to a tertiary care hospital in Muscat, Oman, with symptoms later diagnosed as primary vaginal EHE. The patient had primary, locally invasive vaginal EHE that subsequently metastasised to the lungs. The patient experienced progression of systemic disease despite chemotherapy and was therefore transitioned to palliative chemotherapy. The clinical, radiological and histopathological findings as well as the diagnostic features that distinguish EHE from its aggressive mimic, epithelioid angiosarcoma, are described in this report. This case highlights the diagnostic challenges, the importance of molecular confirmation and the unpredictable clinical course of this ultra-rare malignancy. To the best of the authors' knowledge, this is the first reported case of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
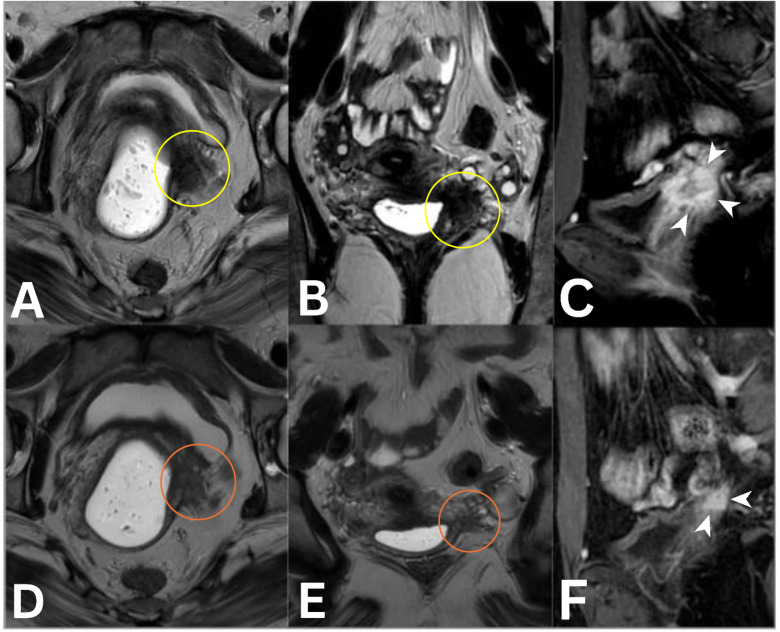 Fig. 1
Fig. 1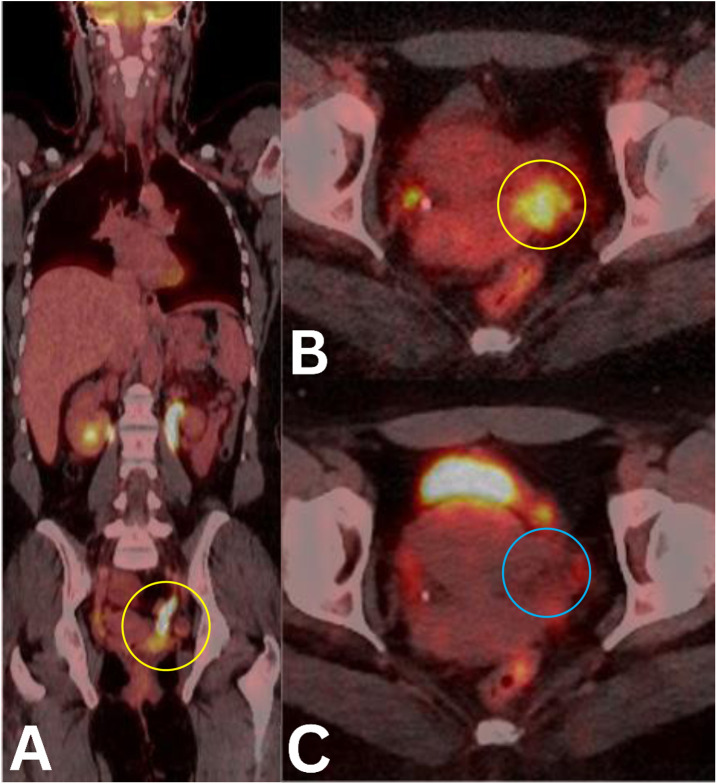 Fig. 2
Fig. 2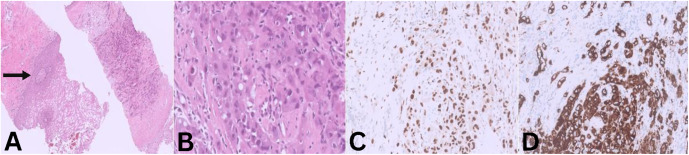 Fig. 3
Fig. 3| Author and year of publication | Clinical presentation | Age at diagnosis in years | Location | Treatment and management course |
|---|---|---|---|---|
| da Silva | Extensive granulomatous lesion | 19 | Vulva | Surgical resection |
| Lee | Fullness and lump at left vulva | 45 | Vulva | Local excision |
| Illueca | Unilateral right ovarian tumour in imaging | 20 | Ovary | Right salpingo-oophorectomy |
| Noreña-Rengifo | Fever and bloody stools | 8 months | Ovary | Left salpingo-oophorectomy |
| Koutsopoulos | Asymptomatic (found during labour) | 29 | Uterus | Surgical resection with no further treatment |
| Matsika | Routine Pap smear | 40 | Cervix | Cone excision followed by total hysterectomy |
| Strayer | Clitoral nodule | 30 | Clitoris | Modified radical vulvectomy with bilateral lymph node dissection; received photon radiotherapy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cancer, Hypoxia, and Metabolism · Occupational and environmental lung diseases
1. Introduction
Epithelioid haemangioendothelioma (EHE) is a rare and enigmatic vascular sarcoma of intermediate malignancy, positioned clinically and histologically between a benign haemangioma and a high-grade angiosarcoma. First described by Weiss and Enzinger in 1982, this tumour originates from endothelial or pre-endothelial cells and is characterised by its unpredictable clinical behaviour, which ranges from indolent and localised disease to aggressive, metastatic cancer.^1^ EHE accounts for less than 1% of all vascular tumours, with an estimated incidence of approximately 0.038 per 100,000 person-years and a prevalence of less than 1 in a million.^23^ While it can arise in any anatomical location, the most common primary sites include the liver, lungs, soft tissues and bone.^3^ The molecular pathogenesis of EHE is defined by specific chromosomal translocations, most commonly the WWTR1-CAMTA1 gene fusion, present in approximately 90% of cases and the YAP1-TFE3 fusion, found in approximately 10% of cases.^4^ These genetic alterations are crucial for diagnosis but do not currently predict clinical behaviour or response to therapy. The clinical presentation of EHE is often nonspecific, with a significant proportion of patients (50–76%) being asymptomatic, particularly when the tumour involves internal organs. This frequently leads to incidental diagnosis and can contribute to delays in management.^5^
EHE of the female genital tract is exceedingly rare, with only a handful of cases reported in the literature involving the ovaries, uterus and vulva.^678^ A comprehensive literature review conducted for this report found no previously documented cases of primary vaginal EHE, making the present case, to the best of the authors' knowledge, the first of its kind to be reported in the medical literature. Furthermore, while metastasis is a known feature of EHE, this is the first report of a primary vaginal EHE with confirmed pulmonary metastasis. This case, therefore, provides a unique and valuable opportunity to expand our understanding of the clinical spectrum and behaviour of this ultra-rare disease.
This report presents the case of a young woman with a primary, locally invasive vaginal EHE that subsequently metastasised to the lungs. This report describes the clinical, radiological and histopathological findings, highlighting the critical role of advanced imaging modalities such as magnetic resonance imaging (MRI) and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) in the diagnosis, staging and monitoring of this aggressive neoplasm. This case underscores the diagnostic challenges and therapeutic dilemmas posed by EHE in such an unusual location and contributes to the limited body of knowledge on this ultra-rare malignancy.
2. Case report
A 31-year-old female presented in 2023 to a tertiary cancer care centre in Muscat, Oman, with a 2-month history of postcoital vaginal bleeding, dyspareunia, left iliac fossa pain and yellowish, offensive mucoid vaginal discharge. A pelvic examination revealed a polypoidal, exophytic soft tissue mass originating from the left vaginal fornix. The lesion was firm, adherent to the pelvic sidewall and the cervix appeared hyperaemic. There was no evidence of rectal involvement on digital rectal examination.
Pelvic MRI showed a 2.6 × 3.3 cm mass in the left vaginal fornix. The lesion demonstrated hypointense signal on T2-weighted images with irregular margins. On diffusion-weighted imaging, it exhibited mild diffusion restriction. Following the administration of gadolinium-based contrast, the mass showed intense and homogeneous arterial enhancement. The tumour was seen abutting the posterior wall of the urinary bladder and encasing the left vesicoureteric junction, resulting in mild left-sided hydronephrosis. No invasion into the rectum was detected [Fig. 1].
Baseline and follow-up multimodality imaging of a patient with vaginal epithelioid haemangioendothelioma. The vagina is distended with vaginal gel for better delineation. A–C: Serial magnetic resonance imaging of the pelvis at baseline in the (A) axial T2, (B) coronal T2 and (C) sagittal post-contrast view showing a soft-tissue mass in the left vaginal fornix (yellow circles) appearing T2-hypointense with irregular margins (A and B) and with (C) intense arterial enhancement (white arrowheads). The lesion abuts the posterior bladder wall and encases the left vesicoureteric junction (white arrow), resulting in mild left hydronephrosis (not shown). D–F: Post-treatment serial magnetic resonance imaging of the pelvis in the (D) axial T2, (E) coronal T2 and (F) sagittal post-contrast view showing that the mass is smaller with reduced enhancement and a less scirrhous appearance (orange circles). The ureteric compression and hydronephrosis have improved (not shown).
Staging CT of the chest, abdomen and pelvis revealed multiple, bilateral ground-glass nodules, measuring 2–5 mm in size, suspicious for early pulmonary metastases. A whole-body 18F-FDG PET/CT demonstrated intense metabolic uptake in the primary vaginal mass (maximum standardized uptake value [SUVmax] = 10) and faint FDG activity in the bilateral pulmonary nodules (SUVmax = 2.2), supporting the suspicion of metastatic disease [Fig. 2].
Axial and coronal 18F-FDG PET/CT images demonstrating intense FDG uptake (SUVmax = 10) in the primary vaginal mass at baseline (yellow circles in A and B), with marked reduction in metabolic activity on follow-up (C; blue circle), consistent with treatment response. The left ureteral dilatation visible in panel A. Please note that the pulmonary nodules are not included in this figure.
The initial vaginal biopsy, performed at an outside facility, was reported as a p16-positive vaginal adenocarcinoma. However, upon review at the current institution, the diagnosis was questioned and a sarcoma was suspected. A repeat biopsy of the vaginal tumour was performed. Histopathological examination showed a neoplasm exhibiting cords, strands and small nests and clusters of large cells with abundant eosinophilic cytoplasm in a background of myxohyaline stroma [Fig. 3A]. Tumour cells had vesicular, round to oval nuclei with minimal pleomorphism [Fig. 3B]. Scattered tumour cells had intracytoplasmic, round, clear vacuoles with indented nuclei (‘bubble cells’). Mitoses were not readily identified (<1/10 hpf). No significant areas of necrosis were seen and areas of conventional angiosarcoma were absent.
Histopathological and immunohistochemical features of the vaginal biopsy. A: Haematoxylin and eosin stain at ×20 magnification showing sheets of tumour cells with adjacent stratified squamous epithelium (arrow). B: Haematoxylin and eosin stain at ×20 magnification showing nests, clusters and cords of tumour cells with abundant glassy cytoplasm as well as scattered cells with intracytoplasmic vacuole aka ‘bubble cells’. C: Tumour cells showing positive nuclear staining for ERG. D: Tumour cells showing strong membrane staining for CD34.
Immunohistochemical studies showed positive staining for ERG and CD34 in the tumour cells [Fig. 3C and Fig. 3D]. Ki67 labelling index was 20%. INI-1 showed intact nuclear expression. MOC31, BerEP4, CAM 5.2, D2-40, CK 5/6, Calretinin, WT-1, TTF-1, EMA, SALL-4, STAT-6, LCA, CD30, CKHMW, TFE-3, Napsin A, CK7, Desmin, CD30, chromogranin and CK19 were negative. The findings were consistent with EHE.
The histopathological features were crucial in differentiating this tumour from its more aggressive mimic, epithelioid angiosarcoma. The bland cytology, low mitotic rate and lack of significant necrosis are features that strongly favour EHE over angiosarcoma.
The patient was started on neoadjuvant chemotherapy with doxorubicin (60 mg/m^2^) and dacarbazine (750 mg/m^2^). After 3 cycles, a follow-up pelvic MRI demonstrated a partial response of the primary tumour [Fig. 1A]. A follow-up PET/CT showed a complete metabolic response in the vaginal lesion but a concerning increase in FDG activity in a right lower lobe pulmonary nodule [Fig. 2C]. A high-resolution CT of the chest confirmed an interval increase in the size and number of bilateral pulmonary nodules, highly suspicious for progressive metastatic disease.
A pulmonary wedge resection was performed and the histopathological analysis of the resected nodule confirmed metastatic EHE.
Given the progression of systemic disease despite chemotherapy, the patient was transitioned to palliative chemotherapy. Molecular profiling of the tumour for the characteristic WWTR1-CAMTA1 or YAP1-TFE3 fusion could not be performed due to lack of next-generation sequencing (NGS) at the current institute. At the most recent follow-up in December 2025, approximately 18 months after diagnosis, repeat imaging demonstrated stable disease while the patient remained on palliative systemic therapy. While the current follow-up duration is still relatively short, ongoing surveillance is planned given the known potential for delayed progression in EHE.
3. Discussion
A comprehensive review of the literature was conducted to identify all reported cases of EHE involving the female genital tract; these published cases highlight both the rarity and the diverse clinical presentation of this tumour [Table 1].^578910111213^
To the best of the authors' knowledge, this is the first documented instance of primary vaginal EHE; the diagnosis was complicated by an unusual primary site and early metastatic spread. The initial misdiagnosis as adenocarcinoma underscores the diagnostic challenge posed by EHE, which can mimic more common epithelial neoplasms, particularly in unusual locations. The definitive diagnosis was ultimately established based on a combination of classic histopathological features, a comprehensive immunohistochemical panel and distinct radiological findings.
The imaging findings in the current case were pivotal for both initial staging and treatment monitoring. On MRI, the primary tumour's T2-hypointense signal is an atypical, but recognised, feature of EHE, likely reflecting a prominent fibrous or sclerotic component rather than high cellularity.^13^ The intense arterial enhancement is, however, consistent with the vascular nature of the tumour. The early detection of subtle pulmonary metastases on staging CT and their faint FDG avidity on PET/CT emphasise the value of these modalities in systemic assessment. While EHE lesions typically demonstrate variable FDG uptake, with an average SUVmax of approximately 5.3, some lesions, particularly small pulmonary nodules, may not be strongly FDG-avid.^14^
Histopathologically, the tumour displayed the classic features of EHE: cords and nests of large, cytologically bland epithelioid cells with abundant, glassy eosinophilic cytoplasm set within a myxohyaline stroma. The presence of intracytoplasmic clear vacuoles, or ‘bubble cells’, representing primitive vascular lumina, is a hallmark feature. The differential diagnosis of EHE is broad and includes metastatic carcinoma, epithelioid angiosarcoma, epithelioid sarcoma and melanoma. The negative staining for epithelial markers (AE1/AE3, EMA, CK7, etc.) was crucial in excluding a carcinoma.^114^ The distinction from epithelioid angiosarcoma, the most important differential, was based on the bland cytology, minimal pleomorphism and low mitotic rate (<1/10 hpf). Angiosarcoma would be expected to show marked nuclear atypia, a high mitotic rate and often, extensive necrosis, all of which were absent in the current case. The intact nuclear expression of INI-1 helped to rule out epithelioid sarcoma, which frequently shows loss of this marker.^14^
The immunohistochemical profile, with strong positivity for vascular markers (ERG and CD34) and negativity for cytokeratins, further solidified the diagnosis. Molecular confirmation of the characteristic WWTR1-CAMTA1 or YAP1-TFE3 gene fusion would be the gold standard for diagnosis according to the latest World Health Organization classification.^411^ The constellation of morphological and immunohistochemical findings in this case provides very strong evidence for EHE. Despite the strong morphological and immunohistochemical evidence, the absence of molecular confirmation of the WWTR1-CAMTA1 or YAP1-TFE3 gene fusion remains a limitation of this case. Unfortunately, NGS was not available at the current institution at the time of diagnosis, and logistical barriers prevented external referral for molecular testing. This limitation highlights a common challenge in resource-constrained settings and underscores the importance of integrating molecular profiling into the diagnostic algorithm for EHE in future cases.
This case is also unique in its documentation of pulmonary metastasis from a primary vaginal EHE. EHE is known to have metastatic potential, with 5-year survival rates varying widely depending on the primary site.^313^ The management of this patient was guided by the principles of sarcoma treatment, with neoadjuvant chemotherapy. The discordant response to chemotherapy, with partial regression of the primary tumour but progression of the pulmonary metastases, illustrates the heterogeneous and unpredictable behaviour of EHE. This heterogeneity in therapeutic response has been reported in other EHE case series and retrospective studies, with patients showing mixed responses between primary and metastatic sites.^1516^ These findings suggest that biological differences within the tumour microenvironment or molecular heterogeneity may contribute to variable treatment outcomes, even within the same patient. This phenomenon highlights the urgent need for more effective systemic therapies, as response rates to conventional chemotherapy are often modest.^1516^ Recent international efforts to improve management strategies for advanced EHE have included consensus guidelines and multi-centre case series. The World Sarcoma Network position paper and the European Society for Medical Oncology Open 2021 consensus both recommend individualised treatment approaches, with close multidisciplinary collaboration.^215^
In addition to anthracycline-based chemotherapy, agents such as interferon-alpha, sirolimus and pazopanib have demonstrated modest benefit in select cases, although no standard regimen currently exists.^16^ These findings underscore the need for further clinical trials to optimise systemic therapy in EHE.
4. Conclusion
Primary vaginal EHE is an extremely rare and aggressive vascular sarcoma with a high potential for metastatic spread. This case highlights the importance of a multidisciplinary approach, including advanced imaging with MRI and PET/CT, for accurate diagnosis, staging and treatment monitoring. The diagnostic journey can be challenging and a high index of suspicion is required to differentiate EHE from more common vaginal malignancies. The unpredictable and often aggressive clinical course of EHE underscores the critical need for novel systemic therapies and the importance of molecular profiling to guide personalised treatment strategies. Further research and the reporting of similar cases are essential to improve our understanding and management of this ultra-rare disease.
Authors' Contribution
Anwar Al Shuaili: Writing – Original draft preparation, Data curation. Huda Kashoob: Investigation, Clinical management. Zahida Niaz: Pathology investigation, Validation. Nausheen Yaqoob: Pathology investigation, Validation. Khadra Ahmed J. Galaal: Supervision, Writing – Review & Editing. Reem Ahmed Al Mazrouai: Conceptualization, Radiological investigation, Supervision, Writing – Review & Editing.
Acknowledgement
The authors would like to acknowledge Dr. Babikir Mustafa Ahmed (Senior Consultant Histopathologist at Sultan Qaboos Comprehensive Cancer Care and Research Center, University Medical City, Muscat, Oman) for his valuable contribution and expert opinion in reaching the final diagnosis in this case.
Ethics Statement
This case report complies with the principles of the Declaration of Helsinki. Written informed consent was obtained from the patient for inclusion in this report and for the publication of clinical details and imaging findings.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weiss SW Enzinger FM. Epithelioid hemangioendothelioma: a vascular tumor often mistaken for a carcinoma. Cancer 1982; 50:970–81. https://doi.org/10.1002/1097-0142(19820901)50:5<970::AID-CNCR 2820500527>3.0.CO;2-Z.10.1002/1097-0142(19820901)50:5<970::AID-CNCR 2820500527>3.0.CO;2-Z 7093931 · doi ↗ · pubmed ↗
- 2Stacchiotti S Miah AB Frezza AM Messiou C Morosi C Caraceni A Epithelioid hemangioendothelioma, an ultra-rare cancer: A consensus paper from the community of experts. ESMO Open 2021; 6:100170. https://doi.org/10.1016/j.esmoop.2021.100170.10.1016/j.esmoop.2021.10017034090171 PMC 8182432 · doi ↗ · pubmed ↗
- 3Liu Z He S. Epithelioid haemangioendothelioma: Incidence, mortality, prognostic factors and survival analysis using the surveillance, epidemiology and end results database. J Oncol 2022; 2022:2349991. 10.1155/2022/2349991.36157226 PMC 9507694 · doi ↗ · pubmed ↗
- 4Sbaraglia M Bellan E Dei Tos AP. The 2020 WHO classification of soft tissue tumours: News and perspectives. Pathologica 2020; 113:70–84. https://doi.org/10.32074/1591-951X-213.10.32074/1591-951X-21333179614 PMC 8167394 · doi ↗ · pubmed ↗
- 5Sardaro A Bardoscia L Petruzelli MF Portaluri M. Epithelioid hemangioendothelioma: An overview and update on a rare vascular tumor. Oncol Rev 2014; 8:259. 10.4081/oncol.2014.259.25992243 PMC 4419652 · doi ↗ · pubmed ↗
- 6Illueca C Machado I Garcia A Covisa A Morales J Cruz J Uncommon vascular tumor of the ovary: Primary ovarian epithelioid hemangioendothelioma or vascular sarcomatous transformation in ovarian germ cell tumor? Arch Gynecol Obstet 2011; 284:1589–91. https://doi.org/10.1007/s 00404-011-1863-7.10.1007/s 00404-011-2036-121822906 · doi ↗ · pubmed ↗
- 7Koutsopoulos AV Sivridis E Tsikouras P Liberis V Karpathiou G Giatromanolaki A Low-grade uterine epithelioid hemangioendothelioma presented as a submucosal leiomyoma during labor. Case Rep Pathol 2013; 2013:423584. 10.1155/2013/423584.23401828 PMC 3563176 · doi ↗ · pubmed ↗
- 8da Silva BB Lopes-Costa PV Furtado-Veloso AM Borges RS. Vulvar epithelioid hemangioendothelioma. Gynecol Oncol 2007; 105:539–41. https://doi.org/10.1016/j.ygyno.2007.01.022.10.1016/j.ygyno.2007.01.02217306346 · doi ↗ · pubmed ↗