Relationship Between Parents' Mental Health and Infant Admission to the Neonatal Intensive Care Unit at Sultan Qaboos University Hospital, Oman
Jahad Al Omairi, Abrar Al Balushi, Hana Al Sumri

TL;DR
This study explores how parents' mental health is linked to their infants being admitted to a neonatal intensive care unit in Oman.
Contribution
The study identifies specific parental and infant factors associated with depression, anxiety, and stress in NICU parents in Oman.
Findings
Anxiety was the most common mental health issue among parents of NICU infants.
Prematurity and male infant sex were significantly associated with parental depression and stress.
Parents with a history of stillbirth or infants requiring resuscitation reported higher stress levels.
Abstract
This study aimed to assess levels of depression, anxiety and stress among parents of neonatal intensive care unit (NICU)-admitted infants at Sultan Qaboos University Hospital (SQUH) in Muscat, Oman, and to examine their association with parental sociodemographic characteristics and infants' clinical factors. This cross-sectional study was conducted at SQUH between December 2024 and March 2025 and included parents of NICU-admitted infants. Mental health status was assessed using the validated Arabic version of the Depression, Anxiety and Stress Scale (DASS-42), while sociodemographic and clinical data were collected using structured questionnaires. Descriptive and inferential statistical analyses were performed, with significance set at P ≤0.05. A total of 86 participating parents were included; 44.2% were fathers, 54.7% mothers and 1.2% other caregivers with a mean age of 33.85 ± 5.81…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
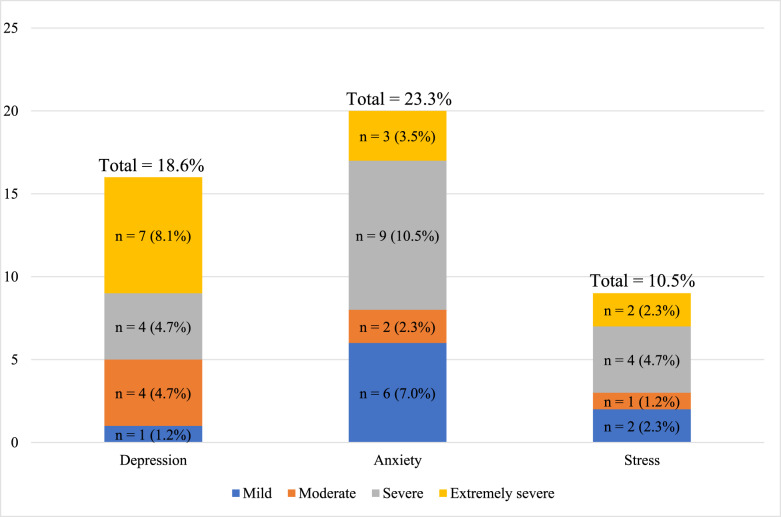 Fig. 1
Fig. 1| Characteristic | n (%) |
|---|---|
|
| |
| Father | 38 (44.2) |
| Mother | 47 (54.7) |
| Other | 1 (1.2) |
|
| |
| 20–29 | 21 (24.4) |
| 30–39 | 49 (57.0) |
| ≥40 | 14 (16.3) |
| Missing | 2 (2.3) |
|
| |
| Married | 86 (100) |
| Single/widowed | 0 (0.0) |
|
| |
| Primary | 2 (2.3) |
| Secondary | 29 (33.7) |
| College or university | 44 (51.2) |
| Postgraduate (Master's or PhD) | 11 (12.8) |
|
| |
| <500 | 25 (29.1) |
| 500–1,000 | 37 (43.0) |
| 1,001–2,000 | 17 (19.8) |
| >2,000 | 7 (8.1) |
|
| |
| Employee | 52 (60.5) |
| Not employed | 29 (33.7) |
| Retired | 2 (2.3) |
| Self-employed | 3 (3.5) |
|
| |
| Al Buraimi | 1 (1.2) |
| Al-Batinah | 27 (31.4) |
| Al Sharqiyah | 10 (11.6) |
| Al Dakhiliyah | 10 (11.6) |
| Muscat | 36 (41.9) |
| Al Wusta | 0 (0.0) |
| Al Dahira | 1 (1.2) |
| Musandam | 0 (0.0) |
| Dhofar | 1 (1.2) |
| Characteristic | n (%) |
|---|---|
|
| |
| Female | 37 (43.0) |
| Male | 44 (51.2) |
|
| |
| Singleton | 81 (94.2) |
| Multiple births | 5 (5.8) |
|
| |
| 20–24 | 2 (2.3) |
| 25–29 | 13 (15.1) |
| 30–34 | 21 (24.4) |
| ≥35 | 45 (52.3) |
| Missing data | 5 (5.8) |
|
| |
| 1st | 25 (29.1) |
| 2nd | 23 (26.7) |
| ≥3rd | 38 (44.2) |
|
| |
| <2 | 7 (8.1) |
| 2–4 | 32 (37.2) |
| 5–10 | 24 (27.9) |
| 1st child | 21 (24.4) |
| Missing data | 2 (2.3) |
|
| |
| Caesarean section | 43 (50.0) |
| Vaginal | 37 (43.0) |
| Assisted | 6 (7.0) |
|
| |
| Using drugs/medications | 3 (3.5) |
| Using embryo transfer | 1 (1.2) |
| Natural | 82 (95.3) |
|
| |
| Respiratory | 18 (20.9) |
| Prematurity | 36 (41.9) |
| Severe jaundice | 9 (10.5) |
| Others | 23 (26.7) |
|
| |
| 2–7 | 43 (50.0) |
| 7–14 | 20 (23.3) |
| 14–30 | 13 (15.1) |
| >30 | 10 (11.6) |
|
| |
| Yes | 14 (16.3) |
| No | 72 (83.7) |
|
| |
| Yes | 4 (4.7) |
| No | 82 (95.3) |
|
| |
| Yes | 5 (5.8) |
| No | 81 (94.2) |
|
| |
| Yes | 9 (10.5) |
| No | 77 (89.5) |
|
| |
| Yes | 12 (14.0) |
| No | 74 (86.0) |
|
| |
| Yes | 10 (11.6) |
| No | 76 (88.4) |
| n (%) | |||
|---|---|---|---|
|
| |||
| Variable | No depression | Depression | |
|
| 0.048 | ||
| 20–29 | 14 (66.7) | 7 (33.3) | |
| ≥30 | 55 (87.3) | 8 (12.7) | |
|
| 0.033 | ||
| Female | 33 (89.2) | 4 (10.8) | |
| Male | 35 (79.5) | 9 (20.5) | |
|
| 0.049 | ||
| 20–35 | 29 (72.5) | 11 (27.5) | |
| ≥36 | 42 (90.2) | 4 (9.8) | |
| n (%) | |||
|---|---|---|---|
|
| |||
| Variable | No anxiety | Anxiety | |
|
| |||
| Female | 33 (89.2) | 4 (10.8) | 0.019 |
| Male | 31 (66.0) | 16 (34.0) | 0.034 |
|
| 0.034 | ||
| Singleton | 43(50.0) | 38(44.2) | |
| Multiple | 1 (20.0) | 4(80.0) | |
| Variable | n (%) | ||
|---|---|---|---|
|
| |||
| No stress | Stress | ||
|
| 0.029 | ||
| 20–35 | 33 (82.5) | 7 (17.5) | |
| ≥36 | 40 (97.6) | 1 (2.4) | |
|
| 0.049 | ||
| No | 71 (92.2) | 6 (7.8) | |
| Yes | 6 (66.7) | 3 (33.3) | |
|
| 0.019 | ||
| No | 69 (93.2) | 5 (6.8) | |
| Yes | 8 (66.7) | 4 (33.3) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Development and Preterm Care · Neonatal Respiratory Health Research · Family and Patient Care in Intensive Care Units
1. Introduction
Neonatal intensive care units (NICUs) are specialised hospital units that provide advanced care for critically ill or preterm newborns through the use of sophisticated medical technology and multidisciplinary teams comprising neonatologists, nurses and respiratory therapists. Admission to NICU is often necessitated by complex medical conditions arising before, during or shortly after birth, such as prematurity (gestational age <37 weeks), low birth weight (<2,500 g), respiratory distress syndromes including neonatal respiratory distress syndrome, congenital anomalies requiring surgical intervention, and life-threatening infections such as neonatal sepsis.^1^
Globally, more than 300,000 infants receive critical, often life-saving care in NICUs each year.^2^ The availability of specialised technology and expertise within NICUs has markedly improved the survival rate for preterm and medically fragile infants, contributing to substantial reductions in infant mortality over the past 5 decades. However, the complex and resource-intensive nature of NICU care can also impose considerable emotional and financial strain on families.^2^
NICU-admitted infants often face an elevated risk of long-term developmental delays, chronic health problems and neurodevelopmental disabilities. Concurrently, their parents frequently experience heightened stress, anxiety and feelings of helplessness, which may impair parent-infant bonding and adversely affect parental mental well-being, while compounding financial pressures. This cumulative burden underscores the need for comprehensive and sustained psychosocial support for both infants and their families during and after NICU admission.^2^
In one study, a racially diverse cohort of 73 mothers of preterm infants completed a questionnaire at NICU discharge assessing postpartum depression, anxiety and related factors.^3^ Approximately 20% of mothers with NICU-admitted infants experience postpartum depression, often at higher severity than mothers of healthy term infants. Anxiety and post-traumatic stress are also common; approximately 35% of mothers and 24% of fathers develop acute stress disorder during the early NICU period and 15% of mothers and 8% of fathers continue to experience post-traumatic stress symptoms even after discharge.^3^
A study by Bua et al. conducted in a tertiary-level NICU in Northern Italy, compared levels of stress, depression, anxiety and participation in care between mothers and fathers of hospitalised newborns.^4^ Using validated tools, the researchers assessed psychological well-being and parental involvement among 191 participants (112 mothers and 79 fathers). The findings revealed that mothers experienced significantly higher stress, trait anxiety and depression than fathers, with 45.5% of mothers versus 24.1% of fathers reporting high stress and 43.8% versus 19.0% showing depressive symptoms, highlighting notable gender disparities in emotional responses to the NICU experience.^4^ Similarly, a study at the Royal Women's Hospital in Melbourne, Australia, followed 184 families of very preterm children (born at <30 weeks' gestation or <1,250 g) born between 2001 and 2003, comparing them to families of full-term children (born at ≥36 weeks from English-speaking households). This study assessed parenting stress, family functioning and the impact of parental mental health. Families of very preterm children reported higher stress levels, poorer family functioning, and a greater sense of burden. Higher stress was associated with parental mental health problems and the presence of neurodevelopmental disabilities in the children.
A recent systematic review and meta-analysis aimed to understand parental psychological phenomena. The emotional response of parents of newborns during NICU admission were assessed. The review comprised 6,822 parents (5,083 mothers, 1,788 fathers; age range: 18–37 years) of NICU patients. Admission of an infant to the NICU tends to be more distressing for mothers than for fathers, often impacting their mental health and overall quality of life. Studies show that mothers experience higher rates of stress, anxiety and depression, likely linked to the emotional burden and guilt associated with giving birth to a critically ill newborn.^5^
Despite these advances, a substantial knowledge gap persists globally and particularly in Oman regarding the short- and long-term mental health outcomes for parents of NICU-admitted infants. This lack of understanding limits the provision of effective psychosocial support, potentially leading to undiagnosed and untreated conditions such as post-traumatic stress disorder, anxiety and depression. These disorders can disrupt parenting, impair child development, strain family relationships and increase healthcare costs. Furthermore, the absence of local data hinders accurate planning and allocation of resources for mental health support services. Therefore, this study aimed to address this gap through focused research to inform the development of targeted interventions aimed at mitigating the lasting psychological impact of NICU admission on parents and families.
2. Methods
This prospective observational cross-sectional study included all eligible Omani parents (mothers or fathers) of infants admitted to the NICU at Sultan Qaboos University Hospital (SQUH) in Muscat, Oman, between December 2024 and March 2025. Those who were of Omani nationality, a parent (mother or father but not both) of an infant admitted to the SQUH NICU during the study period and had an infant admitted for any reason or duration at the time of data collection were included. Parents who declined, were unable to consent, were unavailable during data collection or were non-Omani or of NICU-discharged newborns were excluded.
An online sample size calculator (OpenEpi) was used to estimate the required sample size. According to unpublished hospital data, an average of 100 newborns are expected to be admitted to the NICU at SQUH over 4 months. Therefore, considering a 5% error rate and 95% confidence interval, the required sample size considering at least one parent per admitted child was calculated to be a minimum of 80 parents.
Data were collected using a self-administered electronic questionnaire developed based on the study objectives. The questionnaire collected sociodemographic data from parents including age, nationality, marital status, relationship to the infant, educational level, occupation, monthly household income and place of residence. It also gathered clinical information about the infants such as sex, gestational age, birth order, age of the youngest child, mode of delivery, mode of conception, reason for NICU admission, duration of NICU stay at the time of questionnaire completion, number of previous NICU admissions among siblings, number of children with physical or mental disabilities, presence of a diagnosed disability in the current infant, history of stillbirth and whether the mother had been admitted to the ICU following the current delivery. In addition, parents were asked to complete the validated Arabic version of the Depression, Anxiety, and Stress Scale (DASS-42) to assess their psychological status.^67^
The DASS-42 is a widely used self-report instrument designed to measure negative emotional states, comprising 42 items equally distributed across 3 subscales: depression, anxiety and stress.^8^ This scale has been extensively used to assess psychological distress among parents of newborns in neonatal units in the Arab region.^91011^ The depression subscale assesses symptoms such as dysphoria, hopelessness, devaluation of life, self-criticism, anhedonia, reduced interest in activities and inertia. The anxiety subscale measured symptoms of autonomic arousal, musculoskeletal tension, situational anxiety and subjective feelings of fear, while the stress subscale evaluates tension, irritability and difficulty relaxing, reflecting how individuals respond to daily stressors and their impact on their overall well-being. Participants rated each item on a 4-point Likert scale (0–3), indicating the extent to which they had experienced each symptom during the past week. The DASS-42 has demonstrated robust reliability and validity across diverse populations, with Cronbach's alpha reported as 0.96 for the total scale and 0.93, 0.89 and 0.92 for the depression, anxiety and stress subscales, respectively.^12^ Established cut-off scores were used to categorise symptom severity: depression scores were classified as normal (0–9), mild (10–13), moderate (14–20), severe (21–27) and extremely severe (≥28); anxiety scores as normal (0–7), mild (8–9), moderate (10–14), severe (15–19) and extremely severe (≥20); and stress scores as normal (0–14), mild (15–18), moderate (19–25), severe (26–33) and extremely severe (≥34). These thresholds were applied to categorise participants' psychological outcomes for subsequent statistical analysis.
Although initial plans included in-person interviews, restricted visiting hours and infection-control protocols necessitated the shift to self-administered electronic questionnaires. Therefore, the research team contacted eligible participants via the hospital telephone to provide a brief explanation of the study and obtain verbal consent. Parents who agreed to participate were sent the questionnaire link through WhatsApp (Menlo Park, California, USA). This approach proved more efficient than in-person distribution, facilitating the recruitment of a larger number of participants within the available timeframe. All questionnaires to parents were administered during the newborns' NICU admission period, regardless of admission duration.
Categorical variables were summarised as frequencies and percentages, while continuous variables were presented as means and standard deviations. The prevalence of depression, anxiety and stress was reported according to severity categories based on the established cut-off scores of the DASS-42. Associations between parental sociodemographic characteristics, infant clinical characteristics and the severity of psychological outcomes were examined using the Chi-squared test for categorical variables. When more than 20% of cells had expected frequencies below 5, the two-tailed Fisher's exact test was applied as an alternative. The level of statistical significance was set at P ≤0.05.
In cases of multiple gestations (e.g., twins or triplets), neonatal outcomes such as reason for NICU admission, birth order, presence of disability and clinical course were recorded once per family unit rather than per infant. This approach was adopted to avoid duplication of parental psychological data and ensure that the unit of analysis reflected the parental experience rather than the number of infants. Moreover, only one parent per infant was included in this study to maintain the independence of observations and ensure that each newborn was represented once in the analysis.
3. Results
A total of 86 parents of infants admitted to the NICU at SQUH participated in this study. The majority were mothers (54.7%), followed by fathers (44.2%) and one respondent who was another caregiver (1.2%). The mean age of parents was 33.85 ± 5.81 years, with fathers averaging 35.42 years and mothers 32.43 years. Most participants were aged 30–39 years (57.0%), followed by those aged 20–29 years (24.4%) and those aged 40 years or older (16.3%). All respondents were married. In terms of education, 51.2% had completed college or university, 33.7% had secondary education and 12.8% held postgraduate degrees. Regarding employment, 60.5% were employed, 33.7% were unemployed, 3.5% were self-employed and 2.3% were retired. Monthly family income was reported as <500 Omani riyal (OMR) in 29.1%, 500–1,000 OMR in 43.0%, 1,001–2,000 OMR in 19.8% and >2000 OMR in 8.1% of participants. Most resided in Muscat (41.9%), followed by Al-Batinah (31.4%) with smaller proportions from other regions [Table 1].
Among the 86 infants, 51.2% were male and 43.0% female. Most were singletons (94.2%), with only 5 multiple births (5.8%). Regarding gestational age, 52.3% of the deliveries occurred at 35 weeks or later, 24.4% at 30–34 weeks, 15.1% at 25–29 weeks and 2.3% at 20–24 weeks. The majority were first (29.1%) or third-or-higher order children (44.2%). The youngest sibling's age varied, with 37.2% aged 2–5 years and 24.4% being firstborn. Caesarean section was the most common mode of delivery (50.0%), followed by vaginal delivery (43.0%) and assisted delivery (7.0%). Nearly all infants (95.3%) were conceived naturally. The most frequent reason for NICU admission was prematurity (41.9%), followed by respiratory problems (20.9%), severe jaundice (10.5%) and other causes (26.7%). NICU stays ranged from 2–7 days (50.0%) to more than 30 days (11.6%). A minority of families had a history of NICU admission for another child (16.3%) or a child with physical or mental disability (4.7%); 5 of the current admitted infants (5.8%) were diagnosed with a disability. A total of 9 participants (10.5%) reported a history of stillbirth. Additionally, 14.0% of newborns required resuscitation and 11.6% of mothers were admitted to the ICU following delivery [Table 2].
Based on the DASS-42, 18.6% (n = 16) of parents were classified as having depression. Specifically, 8.1% (n = 7) had mild depression, 4.7% (n = 4) moderate, 4.7% (n = 4) severe and 1.2% (n = 1) extremely severe depression. Anxiety was reported by 23.3% (n = 20) of participants, with 3.5% (n = 3) classified as mild, 10.5% (n = 9) moderate, 2.3% (n = 2) severe and 7.0% (n = 6) extremely severe anxiety. Stress was the least prevalent condition, affecting 10.5% (n = 9) of participants, including 2.3% (n = 2) with mild, 4.7% (n = 4) moderate, 1.2% (n = 1) severe and 2.3% (n = 2) extremely severe stress [Fig. 1].
Prevalence and severity of mental health disorders among parents of newborns admitted to the neonatal intensive care unit at Sultan Qaboos University Hospital (N = 86).
Depression showed a statistically significant association with the youngest parental age group (20–29 years) at 33.3% (n = 7) compared to 12.7% (n = 8) in those aged ≥30 years (P = 0.048). No significant associations were observed between depression and other sociodemographic characteristics including relationship to the infant, educational or employment status, income level or place of residence (P >0.05). Similarly, levels of stress and anxiety did not differ significantly according to any parental sociodemographic characteristics (P >0.05). Depression was significantly more prevalent among parents of male infants (20.5%, n = 9) than female infants (10.8%, n = 4; P = 0.033) and among parents of preterm infants (<36 weeks; 27.5%, n = 11) compared to nearly term and term infants (9.8%, n = 4; P = 0.049) [Table 3]. Parents of infants admitted for prematurity had a higher prevalence of depression (30.6%, n = 11) than those admitted for other reasons (26.7%, n = 23), though this did not reach statistical significance (P = 0.052). Depression was also more common among parents whose infants stayed in the NICU for longer than 1 week (27.9%, n = 12) than among those whose infants stayed 1 week or less (9.3%, n = 4; P = 0.05). Although depression was more frequent among parents of firstborn infants (24.0%, n = 5), those who delivered vaginally (18.9%, n = 7) or by assisted/caesarean delivery (18.4%, n = 9), these differences were not statistically significant (P >0.05).
Anxiety was significantly more common among parents of male infants (34.0%, n = 16) than female infants (10.8%, n = 4; P = 0.019) and for parents of multiples compared to those with a singleton (80.0% versus 44.2%; P = 0.034) [Table 4]. Anxiety was slightly more prevalent among parents of preterm infants (25.0%, n = 10) compared to term infants (22.0%, n = 9; P = 0.798). Higher anxiety was also observed among parents whose infants were admitted for prematurity (27.8%, n = 10; P = 0.833) and among those whose infants stayed longer than 1 week (32.6%, n = 14) compared to 1 week or less (18.6%, n = 6; P = 0.072). First-time parents reported more anxiety (28.0%, n = 7) compared to parents of second or later-born children (21.3%) though this was not significant (P = 0.577). Anxiety prevalence was similar between vaginal (21.6%) and caesarean/assisted deliveries (24.5%; P = 0.802) and between parents with natural conception (24.4%, n = 20) and those who used assisted methods (P = 0.569). Anxiety was more common among parents with a history of stillbirth (44.4%, n = 4), although this did not reach significance (P = 0.203).
Stress was significantly associated with gestational age, being reported by 17.5% (n = 7) of parents of preterm infants compared to 2.4% (n = 1) of parents of term infants (P = 0.029). Stress was also significantly higher among parents with a history of stillbirth (33.3%, n = 3; P = 0.049) and among those whose infants required resuscitation (33.3%, n = 4; P = 0.019) [Table 5]. Parents of male infants reported more stress (11.4%, n = 5) than parents of female infants (5.4%, n = 2), although this was not statistically significant (P = 0.083). Prematurity was the most common reason for NICU admission among parents who reported stress (22.2%, n = 6; P = 0.234). Stress did not differ significantly by mode of delivery (8.1% versus 12.2%; P = 0.726), length of NICU stays (16.3% for >1 week versus 4.7% for ≤1 week; P = 0.429) or birth order (16.0% among first-time parents versus lower rates among parents of later-born children; P = 0.438).
4. Discussion
This study examined the psychological well-being of parents of infants admitted to the NICU at SQUH, focusing on symptoms of depression, anxiety and stress and their associations with parental sociodemographic characteristics and infant clinical factors. The findings demonstrate that NICU admission imposes a considerable psychological burden on parents, though patterns of distress vary across domains and parental subgroups.
In this cohort, 18.6% of parents reported depressive symptoms, predominantly of mild to moderate severity. Depression was more common in mothers (19.1%) than fathers (15.8%), consistent with previous reports indicating that mothers are more vulnerable during the transition to the maternal role in the NICU environment.^1314^ Anxiety emerged as the most prevalent domain (23.3%) and was likewise higher among mothers (25.5%) than fathers (18.4%), reflecting disruptions to maternal role attainment, separation from the infant and concerns regarding the infant's health.^101516^ While these rates are lower than those reported in larger systematic reviews, the direction of the gender differences aligns with international evidence.^12^ Stress was the least frequently reported domain (10.5%), contrasting with higher levels documented in other studies.^1117^ This discrepancy likely reflects the use of the DASS-42, which captures general stress, whereas NICU-specific instruments such as the Parental Stressor Scale: NICU often yield higher estimates, as well as the supportive family-centred care model implemented at SQUH.
Sociodemographic factors appeared to influence parental outcomes. Younger parents (20–29 years) had significantly higher depression rates (33.3%; P = 0.048), which may reflect reduced emotional preparedness for the NICU experience. Anxiety was slightly higher among parents with higher income, unemployment or residence in Muscat, although these associations were not statistically significant. Prior evidence suggests that maternal anxiety often stems from role restriction and uncertainty about post-discharge care, while paternal anxiety tends to arise from financial pressures and role-related expectations.^161819^
Clinical factors were more strongly associated with distress. Preterm birth (<36 weeks) was linked to significantly higher levels of depression and stress, consistent with evidence that lower gestational age and prolonged hospitalisation exacerbate parental psychological symptoms.^2021^ In the current study, even moderate preterm birth (32–36 weeks) was associated with elevated risk, expanding on previous studies that have primarily focused on very preterm infants. Extended NICU stays were also associated with increased depression and stress, corroborating reports that longer hospitalisation amplifies cumulative psychological strain.^22^
Infant gender was another relevant factor, with parents of male infants reporting significantly higher rates of depression and anxiety compared to those with female infants, a finding that diverges from some studies showing no gender effect.^23^ This pattern may reflect sociocultural expectations in Oman, where male children are traditionally viewed as future providers, intensifying parental concerns during illness. Parents of multiples also showed particularly high levels of anxiety, which aligns with prior reports that families with twins or triplets face greater psychological burden due to extended hospitalisation, fertility treatment histories and heightened caregiving demands.^24^
In a recent qualitative study by Bry and Wigert, 16 open-ended interviews were conducted with 27 parents after their infant's discharge from the NICU, inductive content analysis was performed and findings highlight.^25^ The diverse and often complex psychosocial needs of parents with extremely preterm infants create significant challenges for NICU teams. Enhancing staff numbers and strengthening nurses' skills in addressing the emotional and psychological aspects of neonatal care would benefit both caregivers and families. Clearly defining the roles of various professionals and fostering stronger interdisciplinary collaboration could help ease nurses' workload. Moreover, engaging parents in open communication about their needs and providing early information on available support services during their infant's NICU stay are crucial steps in helping them cope with the hospitalisation experience.^25^
In recent years, many NICUs have embraced a family-centred care model. The main objective of this approach is to foster a collaborative partnership between families and healthcare providers, one that promotes parental involvement in the newborn's care and decision-making, encourages open communication and respects each family's unique strengths, concerns and circumstances. A key element of this model is enabling parents to remain with their infants in the hospital.^26^ For example, in Sweden, parents of preterm infants receive compensation for lost income, allowing both to take leave from work to participate in their baby's care. Active family involvement not only helps parents gain confidence in caring for their infant after discharge but also strengthens the parent–infant bond. However, this process can be disrupted by various factors, such as the infant's medical condition and the structure or environment of the NICU itself.^27^
Family-centred care emphasises timely, two-way communication between parents and multidisciplinary staff to coordinate emotional, educational and medical assistance throughout the hospital stay and after discharge. Successful implementation requires open information sharing to identify psychosocial challenges, offer tailored emotional and educational support as well as create individualised, flexible pre- and post-discharge plans that promote a smooth and healthy transition from hospital to home.^28^
Overall, these findings indicate that while both mothers and fathers experience NICU-related psychological strain, mothers appear more vulnerable to anxiety and depression, whereas paternal distress often stems from financial and role-related pressures. Clinical factors such as prematurity, male infant gender and prolonged NICU admission intensify this burden. These results underscore the need to integrate routine psychological screening and culturally sensitive psychosocial support into NICU care to mitigate the long-term psychological impact on families.
This study is limited by its cross-sectional design, single-centre setting and modest sample size, which may restrict the ability to make causal inferences and generalise findings. Reliance on self-reported measures introduces potential reporting bias. Larger, multicentre and longitudinal studies are needed to confirm these findings. Future research could use more context-specific tools to measure parental distress in the NICU setting, including the Parental Stressor Scale: Neonatal Intensive Care Unit as the DASS-42 may underestimate NICU-specific psychological distress.
5. Conclusion
This study demonstrated that parents of infants admitted to the NICU at SQUH experience notable levels of depression, anxiety and stress, with psychological distress most strongly associated with clinical factors such as preterm birth, prolonged hospitalisation and male infant gender, while sociodemographic associations were less pronounced. Although limited by its single-centre design and modest sample size, these findings underscore the urgent need to integrate routine psychological screening and culturally sensitive psychosocial support into NICU care to safeguard parental mental health, strengthen parent-infant relationships and inform the development of evidence-based policies and staff training that enhance family-centred neonatal care.
Authors' contribution
Jahad Al Omairi: Methodology, Validation, Formal analysis, Investigation, Data curation, Visualization, Project administration, Review and Editing. Abrar Al Bulushi: Investigation, Resources, Data curation, Validation, Project administration, Review, and Editing. Hana Al Sumri: Conceptualization, Methodology, Formal analysis, Visualization, Supervision, Project administration, Writing Original Draft, Review and Editing.
Acknowledgement
The authors would like to thank the Department of Child Health, specifically Ms. Samha, for facilitating data collection, and the parents of newborns admitted to the NICU at SQUH for their contribution in this reserach.
Ethics statement
All participants provided consent to take part in this study; this was done via a consent statement, which was attached to the questionnaire link and had to be ticked by the participants who agreed to take part in the study. Ethical approval for this study was obtained from the Medical Research and Ethics Committee of the College of Medicine and Health Sciences, Sultan Qaboos University, Muscat, Oman (SQU-SQU-EC/120/2024).
Conflict of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Standford Medicine Children's Health. The Neonatal Intensive Care Unit (NICU). From: https://www.stanfordchildrens.org/en/topic/default?id=the-neonatal-intensive-care-unit-nicu-90-P 02389 Accessed: Dec 2025.
- 2Valencia Z Sen A Martin K. NICU admissions and spending increased slightly from 2017-2021. Health Care Cost Institute. From: https://healthcostinstitute.org/hcci-originals-dropdown/all-hcci-reports/nicu-use-and-spending-1 Accessed: Dec 2025.
- 3Lean RE Rogers CE Paul RA Gerstein ED. NICU Hospitalization: Long-Term Implications on Parenting and Child Behaviors. Curr Treat Options Pediatr 2018; 4:49–69. https://doi.org/10.1007/s 40746-018-0112-5.10.1007/s 40746-018-0112-529881666 PMC 5986282 · doi ↗ · pubmed ↗
- 4Bua J Dalena P Mariani I Girardelli M Ermacora M Manzon U Parental stress, depression, anxiety and participation in care in neonatal intensive care unit: a cross-sectional study in Italy comparing mothers versus fathers. BMJ Paediatr Open 2024; 8:e 002429. https://doi.org/10.1136/bmjpo-2023-002429.10.1136/bmjpo-2023-00242938589039 PMC 11002394 · doi ↗ · pubmed ↗
- 5Shetty AP Halemani K Issac A Thimmappa L Dhiraaj SK R Prevalence of anxiety, depression, and stress among parents of neonates admitted to neonatal intensive care unit: a systematic review and meta-analysis. Clin Exp Pediatr 2024; 67:104–15. https://doi.org/10.3345/cep.2023.00486.10.3345/cep.2023.0048637986569 PMC 10839189 · doi ↗ · pubmed ↗
- 6Abdellatif M Ahmed M Bataclan MF Khan AA Al Battashi A Al Maniri A. The patterns and causes of neonatal mortality at a tertiary hospital in oman. Oman Med J 2013; 28:422–6. https://doi.org/10.5001/omj.2013.119.10.5001/omj.2013.11924223246 PMC 3815857 · doi ↗ · pubmed ↗
- 7Healthfocus Clinical Psychology Services. Depression Anxiety and Stress Scale DASS (-42). From: https://www.healthfocuspsychology.com.au/tools/dass-42/Accessed: Dec 2025.
- 8Treyvaud K Doyle LW Lee KJ Roberts G Cheong JLY Inder TE Family functioning, burden and parenting stress 2 years after very preterm birth. Early Hum Dev 2011; 87:427–31. https://doi.org/10.1016/j.earlhumdev.2011.03.008.10.1016/j.earlhumdev.2011.03.00821497029 · doi ↗ · pubmed ↗