Complications and Outcomes of Orbital Fracture Repair in Oman
Saleh Al Ghailani, Abdulaziz Bakathir, Ahmed Al Ajmi, Shuhra Al Washahi, Tiamour Al Baloshi, Ahmed Al Hashmi

TL;DR
This study examines the complications and outcomes of orbital fracture repair in Oman, finding that motor vehicle collisions are the main cause and that complication rates are low.
Contribution
The study provides new insights into the outcomes of orbital fracture repair in the Omani population.
Findings
Motor vehicle collisions were the leading cause of orbital fractures in Oman.
The complication rate of orbital reconstruction was low and comparable to global reports.
Titanium mesh was the most commonly used implant material for reconstruction.
Abstract
This study aimed to investigate and analyse the complications and outcomes of orbital fracture repair in Oman. This multicentre retrospective study included all patients with orbital floor and/or medial wall fractures who underwent orbital reconstruction at four tertiary hospitals in Oman between January 2014 and December 2021. The data collected included demographics, fracture aetiology, surgical approach, reconstruction material, complications and repair outcomes. A total of 41 patients were included in this study. Motor vehicle collisions (MVCs) were the most common cause of orbital fractures, accounting for (53.7%) of the patients. Isolated orbital fractures were encountered in 25 patients, 12 patients had orbital fractures associated with the zygomaticomaxillary complex and 4 had fractures associated with naso-orbital ethmoidal fractures. The transconjunctival approach was the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
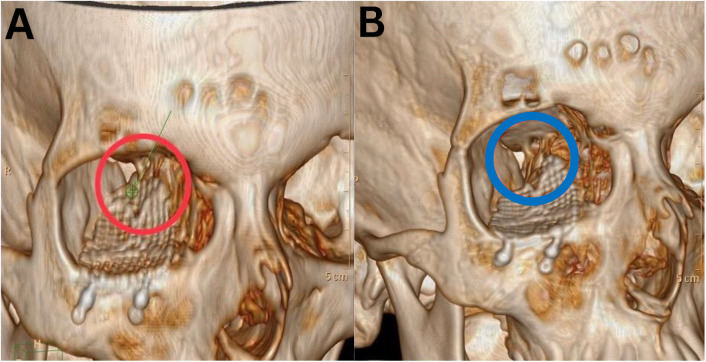 Fig. 1
Fig. 1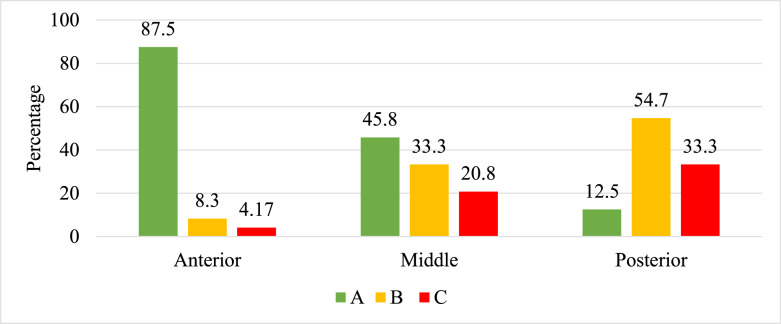 Fig. 2
Fig. 2| Characteristic | n (%) |
|---|---|
| Mean age in years ± SD (range) | 24.7 ± 10.5 (8–60) |
| Mean durations of injury to surgery in days ± SD (range) | 18.2 ± 35.5 (0–220) |
| Mean follow-up in months (range) | 15.5 (3–48) |
| Gender | |
| Male | 34 (82.9) |
| Female | 7 (17.1) |
| Type of fracture | |
| Unilateral isolated orbital fractures | 25 (61.0) |
| Unilateral orbital fractures associated with ZMC | 12 (29.3) |
| Unilateral orbital fracture associated with NOE | 4 (9.8) |
| Classification of fracture | |
| Type 1 | 19 (46.3) |
| Type 2 | 15 (36.6) |
| Type 3 | 4 (9.8) |
| Type 4 | 3 (7.3) |
| Mode of injury | |
| MVC | 22 (53.7) |
| Sport | 4 (9.8) |
| Assault | 7 (17.1) |
| Fall | 4 (9.8) |
| Others | 4 (9.85) |
| Reconstruction material | |
| Bone | 10 (24.4) |
| PDS | 5 (12.2) |
| Titanium | 26 (63.4) |
| Surgical approaches | |
| Pre-existing laceration | 2 (4.9) |
| Subtarsal | 9 (22.0) |
| Infraorbital | 10 (24.4) |
| Transconjunctival | 15 (36.6) |
| Others | 5 (12.2) |
| Indications for surgery | n (%) |
|---|---|
| Ocular restriction | 27 (65.9) |
| Diplopia | 27 (65.9) |
| Enophthalmos | 31 (75.6) |
| Exophthalmos | 1 (2.4) |
| Hypoglobus | 9 (22.5) |
| Retrobulbar haemorrhage | 1 (2.4) |
| Time postoperative, n (%) | |||
|---|---|---|---|
|
| |||
| Complications | 0–2 weeks | 2 weeks–3 months | >3 months |
| Ocular restriction | 10 (24.4) | 8 (19.5) | 4 (9.8) |
| Diplopia | 14 (34.1) | 7 (17.1) | 6 (14.6) |
| Exophthalmos | 4 (9.8) | 3 (7.3) | 4 (9.8) |
| Enophthalmos | 13 (31.7) | 11 (26.8) | 7 (17.1) |
| Hypoglobus | 4 (9.8) | 3 (7.3) | 2 (4.9) |
| Abnormal vision acuity | 5 (12.2) | 5 (12.2) | 5 (12.2) |
| Infection | 1 (2.4) | 2 (4.9) | 0 |
| Epiphora | 1 (2.4) | 2 (4.9) | 2 (4.9) |
| Ectropion | 0 | 1 (2.4) | 0 |
| Entropion | 2 (4.9) | 1 (2.4) | 0 |
| Infra orbital hypoesthesia | 15 (36.6) | 4 (9.8) | 2 (4.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Trauma and Fracture Management · Ocular Disorders and Treatments · Traumatic Ocular and Foreign Body Injuries
1. Introduction
The anatomy of the orbit is complex, with bony structures consisting of multiple cranial facial bones forming the orbital walls within a limited volumetric space. Orbital fractures are relatively common injuries, primarily resulting from motor vehicle collisions (MVCs), falls, sports injuries and interpersonal violence.^1^ Orbital fractures may be managed using either conservative or surgical approaches.^2^ Surgical reconstruction aims to restore the function and structure of the orbit however, it can be associated with several complications, including infection, haemorrhage, ocular restriction, persistent diplopia, enophthalmos, implant-related issues, infraorbital dysesthesia, lacrimal system damage, globe injury, eyelid complications and blindness.^3^
This study aimed to evaluate the postoperative complications and outcomes associated with orbital fracture repair in Oman, offering the first reported insight in the region. This study provides valuable data for future research aimed at enhancing treatment protocols and patient outcomes in cases of orbital trauma.
2. Methods
This retrospective observational cohort study included patients who underwent orbital fracture repair and reconstruction at four tertiary hospitals in Oman (Al-Nahdha Hospital, Sultan Qaboos University Hospital [SQUH], Khoula Hospital and Sohar Hospital). All patients with orbital floor and/or medial wall fractures who underwent orbital reconstruction between January 2014 and December 2021 were included. The inclusion criteria included both adult and paediatric patients (>7 years old) with orbital trauma requiring repair and reconstruction of isolated or associated orbital floor and/or medial wall fractures with zygomaticomaxillary complex (ZMC) or naso-orbital ethmoidal (NOE) fractures. Patients were required to have a minimum follow-up period of 3 months, along with preoperative computed tomography (CT) scans. The exclusion criteria were as follows: patients who underwent conservative treatment, orbital reconstruction due to pathological or pan-facial fractures (including the orbital roof), patients without preoperative CT scans, incomplete documentation and with follow-up periods of less than 3 months. Patient records were accessed and data were extracted from two electronic healthcare systems: Alshifa 3 Plus (Ministry of Health, Oman) for Al-Nahdha, Khoula and Sohar Hospitals and TrakCare^®^2018 (Unified Healthcare System, InterSystems Corporation, Cambridge, Massachusetts, USA) for SQUH.
The study data and variables included gender, age, mechanism of injury, type of orbital fracture (floor, medial wall or both), fracture association (isolated, ZMC-associated or NOE-associated), surgical approach and timing of repair, reconstruction materials, pre- and postoperative CT assessments, reported complications, need for reoperation and follow-up duration. The surgical approaches were categorised as follows: pre-existing laceration, subtarsal, infraorbital incision and transconjunctival. Complications were grouped into three time-frames: within 2 weeks post-surgery, 2 weeks to 3 months post-surgery and beyond 3 months.
The anteroposterior and mediolateral extents of the fracture defect were classified using Jaquiéry et al.'s 5-graded classification of orbital defects.^4^ Post-surgical CT scans were analysed by the principal investigator for implant positioning (anterior, middle and posterior locations of the orbital floor) and graded as ideal, adequate or poor positioning according to the criteria established by Ellis and Tan.^5^ Particular attention was given to sagittal views to confirm the restoration of the normal orbital floor contour and posterior support.^5^ On sagittal CT, an ideal implant position was defined as a reconstruction that follows the expected S-shaped sagittal curvature of the orbital floor without step deformity, provides continuous support to the orbital contents and is seated on stable bony support most importantly the posterior ledge without posterior “drop-off” or sagging into the maxillary sinus. A satisfactory position is indicated by minor under-coverage or small contour discrepancy without clear loss of posterior support, whereas a poor position is indicated obvious malposition (e.g., posterior displacement/drop-off, inadequate posterior ledge support or significant sagging or under-coverage likely to compromise support).
Data on extraocular motility and diplopia were recorded based on ophthalmologist documentation, the anterior and posterior positions of the globe were measured pre- and postoperatively using Hertel exophthalmometry. The forced duction test was documented before and after the surgery.
Collected data were entered into Epidata, Version 2.0 (EpiData Association, Denmark, Europe) and summarised using descriptive statistics. Continuous variables were presented as mean, median and standard deviation, while categorical variables are presented as frequency and percentage. All analyses were performed using Statistical Package for Social Sciences (SPSS) software, Version 28 (IBM Corp., Armonk, New York, USA).
3. Results
A total of 71 patients underwent orbital reconstruction, of whom 41 met the inclusion criteria and were included in the analysis. The sample was comprised of 34 males (82.9%) and 7 females (17.1%), with a mean age of 24.7 ± 10.5 years (range: 8–60 years). The mean postoperative follow-up period was 15 months (range: 3–48 months). The most common cause of orbital fractures was MVCs (53.7%) followed by assault (17.1%). The mean time interval between trauma and orbital repair was 18.2 ± 35.5 days (range: 0–220 days). Pure blow-out fractures were the most common type (n = 25, 61%), followed by impure blow-out fractures (n = 16, 39%), orbital fractures were associated with ZMC (n = 12, 29.3%) and NOE fractures (n = 4, 9.8%). Using Jaquiéry et al. orbital fracture classification system, type I (isolated floor or medial wall defect of 1–2 cm in the orbital anterior 2/3) and type II (floor or medial wall defect of >2 cm in the orbital anterior 2/3) were the most prevalent type, accounting for 46.3% and 36.6% of patients, respectively. The least common forms were types III and IV, representing only 17.1%. The transconjunctival approach was the most frequently used surgical approach (n = 15, 36.6%), followed by the infraorbital approach (n = 10, 24.4%) and subtarsal approach (n = 9, 22.5%). Direct repair via existing wounds was performed in 2 patients (4.9%). Orbital reconstruction primarily utilised titanium mesh (n = 26, 63.4%), followed by bone grafts (n = 10, 24.4%) and polydioxanone (PDS) sheets (n = 5, 12.2%) [Table 1].
The 3 most common indications for repair were enophthalmos, ocular restriction, and diplopia, with frequencies of 75.6%, 65.9% and 65.9%, respectively [Table 2].
Immediate postoperative complications were common during the first 2 weeks following surgery. The most frequent complication was infraorbital nerve hypoesthesia, which occurred in 15 patients (36.6%). Diplopia was observed in 14 patients (34.1%), while enophthalmos was documented in 13 patients (31.7%). Ocular restriction occurred in 10 patients (24.4%). Other less common complications included abnormal visual acuity in 5 patients (12.2%), exophthalmos in 4 patients (9.8%), hypoglobus in 4 patients (9.8%) and infection in 1 patient (2.4%) during the first 2 weeks postoperatively. During the period between 2 weeks and 3 months postoperatively, several complications showed improvement. Infraorbital nerve hypoesthesia decreased to 4 patients (9.8%), diplopia to 7 patients (17.1%) and ocular restriction to 8 patients (19.5%). Enophthalmos persisted in 11 patients (26.8%). Other complications observed during this period included abnormal visual acuity in 5 patients (12.2%), exophthalmos in 3 patients (7.3%), hypoglobus in 3 patients (7.3%), infection in 2 patients (4.9%), epiphora in 2 patients (4.9%) and ectropion in 1 patient (2.4%). Beyond 3 months postoperatively, most complications had resolved or improved. Persistent complications included diplopia in 6 patients (14.6%), enophthalmos in 7 patients (17.1%), ocular restriction in 4 patients (9.8%), abnormal visual acuity in 5 patients (12.2%), infraorbital nerve hypoesthesia in 2 patients (4.9%), hypoglobus in 2 patients (4.9%), epiphora in 2 patients (4.9%) and exophthalmos in 4 patients (9.8%) [Table 3]. Overall, a total of 10 patients experienced more than one complication beyond 3 months, giving an overall complication rate of 24.4%, while 75.6% of patients were free of complications.
Infection occurred in 2 patients (4.9%), during the period of 0–3 months postoperatively; 1 patient was managed with antibiotics, while the other required removal of the reconstruction material and replacement with autogenous bone graft due to a persistent infection that did not respond to antibiotic therapy; both cases initially involved the use of titanium mesh. Revision surgery was required for 4 patients (9.8%), 2 revisions were necessitated by persistent ocular motility restriction. In the first case, no immediate postoperative CT scan was conducted following the initial procedure however, due to incomplete recovery of ocular motility during the follow-up period, CT imaging was subsequently performed. This imaging revealed titanium screw impingement that affected extraocular muscle function. Consequently, revision surgery was undertaken to remove the hardware related to the mechanical limitation, resulting in full recovery of ocular motility. In the second case, revision was performed approximately 2 months postoperatively, the initial procedure had not fully addressed the fracture, and no postoperative CT was conducted at that time. At the 2-month follow-up, CT imaging was requested for further evaluation, revealing persistent posterior muscle entrapment with incomplete release of the muscle from the fracture site. Revision was subsequently performed using a PDS sheet. In this instance, force-duction testing was positive pre-revision and negative post-revision however, the patient developed retrobulbar haemorrhage within hours, necessitating urgent surgical decompression with removal of the implant and haemostatic packing, despite decompression surgery, the patient still had permanent partial loss of visual acuity. A third patient underwent revision 40 days postoperatively due to postoperative infection following titanium mesh reconstruction; notably, the initial injury was contaminated with soil, potentially contributing to the infectious complication and revision was performed using bone graft reconstruction. The fourth revision was conducted within 24 hours due to involvement of the superior orbital fissure and was managed by repositioning the titanium mesh to an optimal position [Fig. 1].
Computed tomography scan 3D reconstruction showing (A) implant malposition (red circle) compressing the superior orbital fissure content leading to superior orbital fissure syndrome and (B) postoperative revision surgery showing the implant in favourable position (blue circle).
Among the 41 patients who underwent orbital reconstruction, 24 had postoperative CT imaging of sufficient quality to assess implant positioning. An ideal implant position in the anterior zone was achieved in 21 cases (87.5%), while in the middle zone, the implant was ideally positioned in 11 (45.8%) and satisfactory in 8 cases (33.3%). In the posterior zone, implant position was satisfactory in 13 (54.2%) and poor in 8 cases (33.3%) [Fig. 2].
Implant position of 24 patients according to criteria of Ellis and Tan et al.5A = ideal position; B = satisfactory position but not following orbital contour; C = poor position/into sinus/not following orbital contour.
4. Discussion
Orbital fractures are common, and when surgical repair is indicated, it should aim to reconstruct the orbital volume and structures with minimal complications and good aesthetic and functional outcomes for the patients. Orbital floor fractures can cause mild to severe dysfunction, obvious aesthetic asymmetry and vision is rarely compromised. The main reported complications associated with orbital fractures are diplopia, enophthalmos, extraocular movement limitation and visual abnormalities.^6^
There are no published data on orbital injuries and their surgical repair in Oman or the region. To the best of the authors' knowledge, the current study is the first in the region to highlight the complications and outcomes associated with orbital fracture reconstruction. In addition, this analysis provided basic data for future orbital trauma and can be used to improve treatment and outcomes of orbital trauma. The results of this study showed a high percentage of orbital fractures in the age group of 20–30 years. This finding differs from previously reported findings by Bronstein et al. and Gander et al.^78^ This suggests potential variations in the observed outcomes that warrant further investigation.
In general, most orbital fractures do not require urgent interventions. Surgery is typically delayed to allow time for the orbital swelling to subside thereby fully facilitating a more thorough assessment of the extent of the injury and ensuring optimal surgical planning. However, there are urgent indications for surgery in cases such as trap-door orbital floor fractures associated with an oculo-cardiac reflex as well as instances of retrobulbar haemorrhage (RBH) that pose an immediate risk to vision and require immediate intervention.^9^ A systematic review by Jazayeri et al. analysed data from 20 studies and concluded that repairing orbital floor fractures within 2 weeks of injury was associated with higher success rates, a greater likelihood of complete recovery and early intervention demonstrated a lower risk of postoperative complications including diplopia and enophthalmos compared to delayed treatment initiated at 3–4 weeks post-injury.^10^ In contrast, Dal Canto and Linberg found no statistically significant difference in outcomes when orbital repair was performed within 2 weeks versus up to 4 weeks post-injury.^11^ Notably, delayed repair may introduce technical challenges associated with fibrosis formation. Consequently, patients with clear indications for surgery should undergo timely interventions to optimise outcomes. For patients at low risk of enophthalmos who demonstrate improvements in function and aesthetics, observation for up to 4 weeks may be a safe alternative.^11^ In the present study, a young adolescent who presented with diplopia following blunt orbital trauma sustained 6 months earlier was treated, the delay in presentation was primarily due to logistical factors. Clinical and radiographic evaluations revealed muscle entrapment and ophthalmoplegia. Due to the long and delayed corrective orbital repair at 220 days post-injury, the patient achieved only partial recovery of ocular muscle motility with residual diplopia. In this case, an earlier surgical repair might have yielded a better outcome by minimising muscle trauma, scarring and fibrotic changes.
The choice of surgical approach may not significantly affect the overall success of orbital fracture reconstruction. However, cosmetic outcomes and potential complications must be considered, emphasising the importance of proper surgical techniques and careful planning. In the present study, commonly used approaches, such as transconjunctival and infraorbital incisions, yielded favourable cosmetic results with a low risk of ectropion and entropion. However, 2 patients developed postoperative entropion following the transconjunctival approach, one of whom resolved spontaneously, while the other required oculoplastic surgical correction. These findings align with those of Bronstein et al. who reported a 3.9% risk of entropion. In addition, other published literature has highlighted an increased number of reports of entropion in association with the transconjunctival approach, though not statistically significant.^712^
Serious postoperative complications following orbital reconstruction are relatively rare. However, this study reported a case of RBH that developed within 12-hours postoperatively. The patient presented with proptosis, pain and reduced visual acuity with CT scan showing proper implant positioning but revealing a haemorrhagic collection in the retrobulbar space. Despite the administration of intravenous steroids and decompression of the RBH, the patient ultimately had permanent partial vision loss.^13^
Orbital fractures are usually associated with neurosensory disturbances of the infraorbital nerve (ION). Based on the present study's results, the prevalence of preoperative ION disturbance was 36.5%, which is slightly higher than the reported range of 11–35%.^141516^ During the follow-up period, improvement was noted in all patients except for 2 (4.8%). These findings are in line with published studies that have reported a 9.3–55% risk of residual ION neurosensory disturbance in patients who underwent orbital reconstruction.^141516^
The ideal material for orbital fracture repair has been a subject of controversy, as each material offers distinct advantages and disadvantages depending on the fracture type. Autologous bone grafts, which are free from immunological reactions, were once considered a good choice for orbital fracture repair and are typically harvested from sites such as the iliac crest or calvarium. However, their use has become less favoured in recent years due to the prolonged operating time, donor site morbidity, difficulty in adapting to orbital anatomy and the unpredictable degrees of bone resorption.^1718^
Titanium implants are widely used because of their physical strength, malleability for adaptation to orbital anatomy and visibility on imaging. However, the risks of using titanium include the development of adhesions and foreign body reactions.^19^ In the present study, there was 1 case of postoperative exophthalmos following the use of an autogenous iliac bone graft. The development of exophthalmos may be attributed to the challenges in reshaping the flat bone graft to conform to the orbital curvature, as well as anticipated graft resorption, which can lead to overcorrection. However, it is important to note that graft resorption remains unpredictable.^20^ Although there was considerable individual variability, both materials were successfully used in this study. However, titanium mesh was used in most cases (63.4%) and demonstrated favourable outcomes in terms of ocular movement correction and reduction of diplopia. Additionally, titanium mesh was associated with a lower incidence of complications, such as infection, wound dehiscence and implant exposure. The present study's results align with the published literature, which supports the superior outcomes associated with the use of titanium as a core material.^521^
Published data on revision surgery following orbital reconstruction indicate that it is relatively uncommon. According to the literature, revision rate ranges from 6.5–17%.^22232425^ The most commonly reported indications for orbital revision surgery include implant malposition and suboptimal orbital reconstruction, that are often associated with clinical symptoms such as globe malposition, visual acuity disturbances and restricted ocular motility.^2227^ In the present study, the revision surgery rate was (9.7%), which is consistent with internationally reported rates.^23242526^ Among the 4 patients who underwent revision, 1 developed a foreign body reaction and infection, requiring removal of the orbital plate and replacement with a bone graft. In another case, the patient had a malpositioned implant compressing the superior orbital fissure contents and revision surgery was done within 6 hours to reposition the titanium implant, with full recovery observed in the immediate postoperative period. Additionally, 1 patient had suboptimal reconstruction, leading to enophthalmos and minimal ocular restriction that did not improve over 2 months. Radiographic imaging revealed rectus muscle entrapment in the posterior orbit, and revision surgery was performed to release the entrapped muscle and correct the enophthalmos, achieving a satisfactory outcome.
Displacement or malpositioning of orbital reconstructive materials can result in serious complications, including diplopia, ophthalmoplegia, enophthalmos, visual acuity disturbances and, in severe cases, blindness.^18^ Malpositioned orbital implants can alter the orbital volume, leading to clinically evident enophthalmos. In the present study, residual enophthalmos at 3 months postoperatively was observed in (17.1%) of cases, which is within the reported range of (3.75–27%) noted in the literature.^2227282930^ Large fractures involving the combined medial and orbital walls or the medial wall alone are technically challenging to reconstruct with a prefabricated plate. Using an autogenous bone graft is even more difficult, as it is often impossible to contour the bone graft to the orbital shape, potentially leading to enophthalmos.^23^ To overcome such challenges, it is now recommended to use intraoperative imaging to assist the surgeon in controlling and optimising the position of the implant during orbital reconstruction. This approach can improve surgical outcomes and reduce the need for revision surgery.^303132^ Borad et al. and Schlittler et al.'s studies reported that 44% of orbital implants were repositioned intraoperatively with the assistance of imaging. This highlights the importance of real-time imaging in optimising implant placement and ensuring better alignment with orbital anatomy, ultimately improving surgical outcomes and minimising the need for revision procedures.^3334^
The primary goal of orbital reconstruction is to accurately restore the orbital defect using an appropriate material that conforms to the orbital anatomy and preserves ocular function. However, the reconstruction of large or multi-walled fractures remains a significant surgical challenge. Recent studies have demonstrated a better surgical outcome with patient-specific implants (PSI) than with traditional titanium meshes. PSIs offer advantages in terms of anatomical fit, reducing the need for intraoperative adjustments and minimising the risk of complications such as implant malposition or postoperative enophthalmos.^16^ By being tailored to the patient's unique orbital anatomy, PSIs contribute to improved cosmetic and functional results, highlighting their growing role in orbital reconstruction.^816^ However, the main drawbacks of PSIs are their relatively high cost and the potential for delays in their supply, which can limit their widespread use. Timoshchuk et al. suggested that the routine use of orbital PSIs may not always be warranted, as their study found no statistically significant difference in postoperative complications compared to preformed orbital implants. Despite this, they highlighted the superior accuracy of PSI positioning, which plays a crucial role in achieving optimal anatomical alignment and improving cosmetic and functional outcomes.^35^ While PSIs may not be necessary for all cases, they may still offer significant advantages in complex orbital reconstructions where a precise anatomical fit is essential.
Diplopia is a well-known complication following orbital fractures, with its aetiology linked to various factors such as orbital fractures, neuromuscular trauma. The presence of diplopia can significantly impact a patient's quality of life, affecting their daily activities such as reading and driving.^36^ In the present study (34.1%) of patients experienced postoperative diplopia and by 3 months the residual rate was (9.8%) which is lower than the reported rates of up to (20%) in treated cases.^283637^ The potential causes of persistent residual diplopia after primary surgery have been discussed in the literature including the timing of surgical repair, orbital adherence syndrome that frequently occur after surgical reconstruction of orbital fractures with titanium implants could potentially contribute to the residual postoperative diplopia.^19^ Jung et al. investigated the relationship between clinical and radiographic findings and residual diplopia in a large patient cohort and found that older patients, those presenting with muscle entrapment and ocular muscle swelling, were more likely to experience persistent diplopia after surgical repair.^39^ These findings suggest that, although the resolution of diplopia is common, residual cases are influenced by various factors including the timing of surgery and the presence of muscle involvement. Early intervention, muscle entrapment management and careful surgical techniques can help in reducing the risk of persistent symptoms.
In the present study, postoperative CT assessments of orbital reconstruction revealed poor implant positioning in (33.3%) of cases, specifically in the posterior part of the orbit. This rate is higher than the reported range of 5.6–14.3% observed by Nikunen et al. and Schlittler et al, which may be attributed to the inclusion of patients who underwent orbital reconstruction using PSIs in their studies.^2534^ In contrast, the present study, based on Jaquiéry et al.'s classification, showed that more than 50% of the patients had orbital fractures classified as class 2 or higher.^4^ Schlittler et al. found a correlation between Jaquiéry et al.'s classification and the incidence of implant malposition. They recommended that PSI should be considered for class 4 and, to a lesser extent, class 3 fractures to improve outcomes and reduce the risk of implant malposition.^325^ Given that the present study showed a slightly higher rate of implant malposition, the authors predict that the higher class of orbital defects in this study may have contributed to this increased rate of malposition, underscoring the potential value of PSI in complex cases.
This study had several limitations, including its retrospective nature, small sample size due to missing clinical and radiographic data, and variable follow-up periods for some patients. In addition, fixation for associated ZMC/NOE fractures was not consistently recorded, which may have influenced postoperative outcomes.
5. Conclusion
This study demonstrated a low complication rate for orbital fracture repair, comparable to that in the existing literature, with most immediate postoperative complications resolving within 3 months. Ensuring intraoperative or immediate postoperative CT scan to assess implant positioning, particularly in the posterior orbital zone, is crucial for minimising postoperative complications.
Generative AI Declaration
Paperpal Version 2.0.3, was utilised exclusively for the improvement of sentence structure and language flow. No content generation, analysis or intellectual contribution were made by the AI system beyond linguistic enhancement.
Authors' Contribution
Saleh Al Ghailani: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing – original draft preparation, Writing – review & editing. Ahmed Al Hashmi: Conceptualization, Data curation, Investigation, Writing – review & editing. Ahmed Al Ajmi: Data curation, Investigation. Shuhra Al Washahi: Data curation, Investigation. Tiamour Al Baloshi: Data curation, Investigation. Abdulaziz Bakathir: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Supervision, Writing – review & editing.
Acknowledgement
The authors would like to thank Mr. Sachin Jose, Statistics Specialist, Research and Studies Department, Oman Medical Specialty Board (OMSB), Muscat, Oman, for his assistance with the statistical analysis.
Ethics Statement
Ethical approval for the study was obtained from the Research and Ethics Committee of the Ministry of Health, Muscat, Oman (MoH/CSR/22/25630) and the Medical Research Ethics Committee at Sultan Qaboos University, Muscat, Oman (MREC #2717).
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiang E Saadat LV Spitz JA Bryar PJ Chambers CB. Etiology of orbital fractures at a level I trauma center in a large metropolitan city. Taiwan J Ophthalmol 2016; 6:26–31. https://doi.org/10.1016/j.tjo.2015.12.002.10.1016/j.tjo.2015.12.00229018706 PMC 5602121 · doi ↗ · pubmed ↗
- 2Zhang J Zhou P Qi Y Zhou P. The better surgical timing and approach for orbital fracture: a systematic review and meta-analysis. Ann Transl Med 2022; 10:564. https://doi.org/10.21037/atm-22-1465.10.21037/atm-22-146535722414 PMC 9201124 · doi ↗ · pubmed ↗
- 3Gonzalez MO Durairaj VD. Indirect orbital floor fractures: a meta-analysis. Middle East Afr J Ophthalmol 2010; 17:138–41. https://doi.org/10.4103/0974-9233.63076.10.4103/0974-9233.6307620616920 PMC 2892129 · doi ↗ · pubmed ↗
- 4Jaquiéry C Aeppli C Cornelius P Palmowsky A Kunz C Hammer B. Reconstruction of orbital wall defects: critical review of 72 patients. Int J Oral Maxillofac Surg 2007; 36:193–9. 10.1016/j.ijom.2006.11.002.17241771 · doi ↗ · pubmed ↗
- 5Ellis E 3rd Tan Y. Assessment of internal orbital reconstructions for pure blowout fractures: cranial bone grafts versus titanium mesh. J Oral Maxillofac Surg 2003; 61:442–53. https://doi.org/10.1053/joms.2003.50085.10.1053/joms.2003.5008512684961 · doi ↗ · pubmed ↗
- 6Kotecha S Ferro A Harrison P Fan K. Orbital reconstruction: a systematic review and meta-analysis evaluating the role of patient-specific implants. Oral Maxillofac Surg 2023; 27:213–26. https://doi.org/10.1007/s 10006-022-01074-x.10.1007/s 10006-022-01074-x 35589881 PMC 10234907 · doi ↗ · pubmed ↗
- 7Bronstein JA Bruce WJ Bakhos F Ishaq D Joyce CJ Cimino V. Surgical approach to orbital floor fractures: comparing complication rates between subciliary and subconjunctival approaches. Craniomaxillofac Trauma Reconstr 2020; 13:45–8. https://doi.org/10.1177/1943387520904893.10.1177/194338752090489332642031 PMC 7311850 · doi ↗ · pubmed ↗
- 8Gander T Essig H Metzler P Lindhorst D Dubois LRúcker M Patient specific implants (PSI) in reconstruction of orbital floor and wall fractures. J Craniomaxillofac Surg 2015; 43:126–30. https://doi.org/10.1016/j.jcms.2014.10.024.10.1016/j.jcms.2014.10.02425465486 · doi ↗ · pubmed ↗