Computed Tomography-Guided Percutaneous Core Needle Biopsy of Lung Lesions: Factors influencing diagnostic yield and complications
Raza Sayani, Jayakrishnan B, Rashid Al Sukaiti, Zahida Niaz, Muhammad Sharjeel Usmani, Mustafa Talib Yousif Al Ani, Hasan Al-Sayegh, Subhash Chand Kheruka

TL;DR
This study evaluates the effectiveness and safety of CT-guided lung biopsies, finding that larger and more superficial lesions yield better results with fewer complications.
Contribution
The study identifies lesion size and depth as key factors influencing diagnostic yield and complication rates in CT-guided lung biopsies.
Findings
Diagnostic yield was 81.9%, with malignancy confirmed in 72.4% of cases.
Lesion size >2.1 cm showed significantly higher diagnostic accuracy (93.9%) compared to <1 cm (55%).
Complications occurred in 28.8% of patients, primarily pneumothorax (21.2%).
Abstract
This study aimed to evaluate the diagnostic yield and complications associated with computed tomography (CT)-guided transthoracic core-needle biopsy (CNB) of lung lesions and to identify factors influencing biopsy outcomes. This retrospective study included patients who underwent CT-guided CNB of lung lesions at Sultan Qaboos Comprehensive Cancer Care & Research Centre, University Medical City, Muscat, Oman, from November 2021 to December 2024. Patients were categorised as either having undiagnosed lung masses/nodules or suspected pulmonary metastases from known malignancies. Biopsies were performed using an 18-gauge coaxial needle, following standard protocols. Diagnostic yield, sample adequacy for molecular analysis and complications were analysed using descriptive statistics and Chi-squared or Fisher's exact tests. A total of 105 patients were included. Diagnostic yield of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
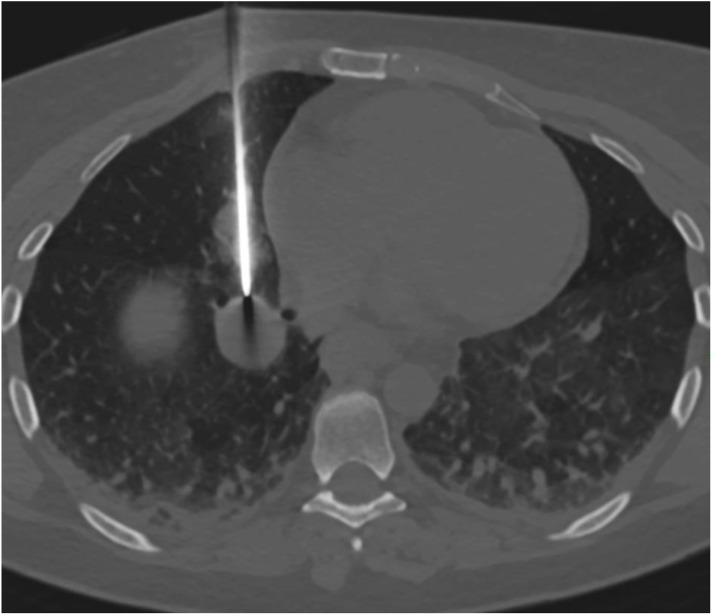 Fig. 1
Fig. 1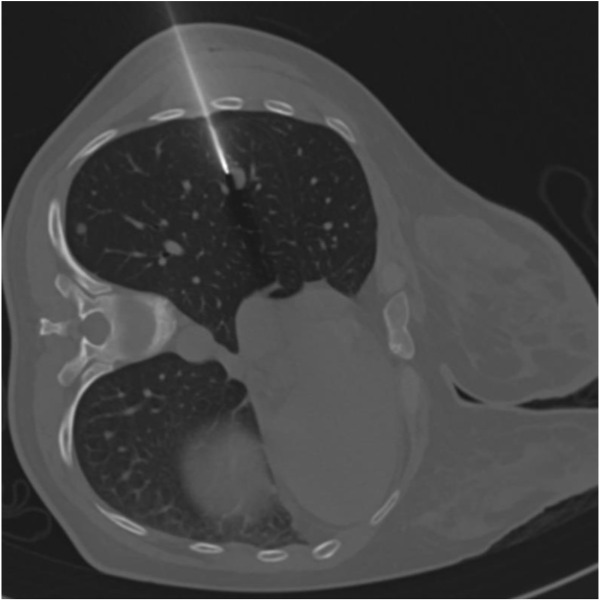 Fig. 2
Fig. 2| Characteristic | n (%) |
|---|---|
|
| |
| ≤40 | 11 (10.5) |
| 41–60 | 36 (34.3) |
| 61–80 | 53 (50.5) |
| >80 | 5 (4.8) |
|
| |
| Male | 48 (45.7) |
| Female | 57 (54.3) |
|
| |
| Lung mass | 31 (29.5) |
| Breast cancer | 27 (25.7) |
| Gastrointestinal cancer | 14 (13.3) |
| Lung cancer | 8 (7.6) |
| Sarcoma | 7 (6.7) |
| Oro/nasopharyngeal cancer | 6 (5.7) |
| Genitourinary cancer | 4 (3.8) |
| Gynaecological cancer | 4 (3.8) |
| Other cancers | 4 (3.8) |
|
| |
| Solitary | 61 (58.1) |
| Multiple | 44 (41.9) |
|
| |
| Solid | 93 (88.6) |
| Solid cystic/necrotic | 3 (2.9) |
| Cavity | 4 (3.8) |
| Consolidation | 5 (4.8) |
|
| |
| Right upper lobe | 19 (18.1) |
| Right middle lobe | 10 (9.5) |
| Right lower lobe | 27 (25.7) |
| Left upper lobe | 19 (18.1) |
| Left lingula | 1 (1.0) |
| Left lower lobe | 27 (25.7) |
| Mediastinum | 1 (1.0) |
| Pleura | 1 (1.0) |
|
| |
| 0.4–1 | 20 (19.0) |
| 1.1–2 | 29 (27.6) |
| 2.1–5 | 33 (31.4) |
| >5 | 23 (21.9) |
|
| |
| Lung nodules | 74 (70.5) |
| Lung mass | 31 (29.5) |
|
| |
| PET positive | 69 (65.7) |
| PET negative/not done | 36 (34.3) |
|
| |
| ≤5 | 45 (42.9) |
| >5.1 | 60 (57.1) |
|
| |
| Low intensity (<5) | 26 (35.6) |
| Moderate intensity (5–10) | 20 (27.4) |
| Intense (10.1–15) | 14 (19.2) |
| Very intense (>15.1) | 13 (17.8) |
|
| |
| 1 | 6 (5.9) |
| 2–3 | 73 (72.3) |
| ≥4 | 22 (21.8) |
|
| |
| Negative | 19 (18.1) |
| Positive (non-malignant) | 10 (9.5) |
| Positive (malignant) | 76 (72.4) |
| Characteristic | Diagnostic yield, n (%) | |
|---|---|---|
|
| 0.800 | |
| ≤60 | 39 (83.0) | |
| >60 | 47 (81.0) | |
|
| 0.870 | |
| Male | 39 (81.2) | |
| Female | 47 (82.5) | |
|
| 0.280 | |
| Breast cancer | 19 (70.4) | |
| Gastrointestinal cancer | 10 (71.4) | |
| Genitourinary cancer | 4 (100) | |
| Gynaecological cancer | 3 (75.0) | |
| Lung cancer | 8 (100) | |
| Lung mass | 28 (90.3) | |
| Oro/nasopharyngeal cancer | 4 (66.7) | |
| Other cancers | 4 (100) | |
| Sarcoma | 6 (85.7) | |
|
| 0.980 | |
| Solitary | 50 (82.0) | |
| Multiple | 36 (81.8) | |
|
| 0.220 | |
| Solid | 78 (83.9) | |
| Solid cystic/necrotic | 2 (66.7) | |
| Cavity | 3 (75.0) | |
| Consolidation | 3 (60.0) | |
|
| 0.180 | |
| Lingula | 0 (0) | |
| Lower lobes | 46 (85.2) | |
| Left upper lobe | 15 (78.9) | |
| Mediastinum | 1 (100) | |
| Pleura | 1 (100) | |
| Right middle lobe | 6 (60.0) | |
| Right upper lobe | 17 (89.5) | |
|
| 0.003 | |
| 0.4–1 | 11 (55.0) | |
| 1.1–2 | 23 (79.3) | |
| 2.1–5 | 31 (93.9) | |
| >5 | 21 (91.3) | |
|
| 0.150 | |
| Lung nodules | 58 (78.4) | |
| Lung mass | 28 (90.3) | |
|
| 0.270 | |
| ≤5 | 39 (86.7) | |
| >5.1 | 47 (78.3) | |
|
| 0.003 | |
| Low intensity (<5) | 16 (61.5) | |
| Moderate intensity (5–10) | 17 (85.0) | |
| Intense (10.1–15) | 14 (100) | |
| Very intense (>15.1) | 13 (100) | |
|
| 0.120 | |
| 1 | 3 (50.0) | |
| 2–3 | 62 (84.9) | |
| ≥4 | 19 (86.4) | |
|
| 0.800 | |
| PET positive | 57 (82.6) | |
| PET negative/not done | 29 (80.6) | |
|
| 0.002 | |
| Yes | 19 (63.3) | |
| No | 66 (89.2) |
| Characteristic | Complications, n (%) | |
|---|---|---|
|
| 0.750 | |
| ≤60 | 14 (30.4) | |
| >60 | 16 (27.6) | |
|
| 0.500 | |
| Male | 12 (25.5) | |
| Female | 18 (31.6) | |
|
| 0.015 | |
| Breast cancer | 12 (44.4) | |
| Gastrointestinal cancer | 8 (57.1) | |
| Genitourinary cancer | 2 (50.0) | |
| Gynaecological cancer | 1 (25.0) | |
| Lung cancer | 2 (25.0) | |
| Lung mass | 4 (12.9) | |
| Oro/nasopharyngeal cancer | 1 (16.7) | |
|
| 0.760 | |
| Solitary | 18 (30.0) | |
| Multiple | 12 (27.3) | |
|
| 0.200 | |
| Solid | 24 (26.1) | |
| Solid cystic/necrotic | 2 (66.7) | |
| Cavity | 2 (50.0) | |
| Consolidation | 2 (40.0) | |
|
| 0.300 | |
| Lingula | 1 (100) | |
| Lower lobes | 16 (29.6) | |
| Left upper lobe | 4 (21.1) | |
| Right middle lobe | 5 (50.0) | |
| Right upper lobe | 4 (21.1) | |
|
| 0.001 | |
| 0.4–1 | 12 (60.0) | |
| 1.1–2 | 11 (37.9) | |
| 2.1–5 | 4 (12.1) | |
| >5 | 3 (13.6) | |
|
| 0.019 | |
| Lung nodules | 26 (35.6) | |
| Lung mass | 4 (12.9) | |
|
| 0.080 | |
| ≤5 | 9 (20.0) | |
| >5.1 | 21 (35.6) | |
|
| 0.027 | |
| Low intensity (<5) | 13 (50.0) | |
| Moderate intensity (5–10) | 2 (10.0) | |
| Intense (10.1–15) | 5 (35.7) | |
| Very intense (>15.1) | 3 (23.1) | |
|
| 0.250 | |
| 1 | 3 (50.0) | |
| 2–3 | 23 (31.5) | |
| ≥4 | 4 (18.2) | |
|
| 0.340 | |
| PET positive | 22 (31.9) | |
| PET negative/not done | 8 (22.9) | |
|
| 0.002 | |
| Any positive result | 19 (22.4) | |
| Negative | 11 (57.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Lung Cancer Treatments and Mutations · Pleural and Pulmonary Diseases
1. Introduction
Computed tomography (CT)-guided transthoracic core-needle biopsy (CNB) is a conventional and dependable approach for diagnosing uncertain lung lesions, particularly when surgical intervention is not feasible. With increased screening for lung cancer in at-risk individuals, there is a need to sample suspicious lung nodules in a safe manner. Furthermore, in patients with a known malignancy, it is essential to be able to distinguish between malignant and non-malignant lung opacity for further treatment decisions.^1^ CT is considered to be the most effective test to detect lung metastasis. Currently, there are no guidelines on the preferred invasive diagnostic tests of pulmonary nodules. Therefore, depending on the availability, different institutions either use “inside-out” or “outside-in” approaches such as electromagnetic navigational bronchoscopy, radial endobronchial ultrasound, optical coherence tomography, ultrathin bronchoscopy, robotic-assisted bronchoscopy or CT-guidance to localise and sample.^2^
Numerous studies have consistently demonstrated the high accuracy of CNB and its minimal complications in the evaluation of lung masses and sub-centimetre pulmonary opacities.^13^ The diagnostic accuracy tends to vary based on the size and characteristics of the lesions. For example, a diagnostic yield of 83.9% for lesions measuring >16 mm, and 75.6% for solid-dominant lesions was reported.^4^ Nonetheless, CNB may fail to detect some cancers, particularly in the case of large, intricate lesions or those featuring cysts and necrotic areas. Positron emission tomography (PET) with 2-deoxy-2-[fluorine-18] fluoro- D-glucose integrated with CT (18F-FDG PET/CT)) scans can identify areas with heightened metabolic activity, assisting with the choice of diagnostic test.^5^ Intepe et al. showed that using 18F FDG-PET/CT, to guide transthoracic biopsy, increases the rate of accurate diagnosis.^6^ A study from USA showed that CNB could yield accurate molecular testing data in approximately 90% of lung nodules <1.5cm with a low rate of easily manageable complications.^7^
Complications from a lung CNB include pneumothorax, pulmonary haemorrhage, haemoptysis, air embolism and tumour seeding. Decubitus position, multiple needle passes and longer lesion-pleura distance are the usual risk factors for CNB-related complications.^8^ Fortunately, most of the complications are minor and do not normally require admission or definitive management.
The objectives of the present study were to evaluate the overall diagnostic yield of CT-guided lung biopsies, explore the complications rate and identify the factors that may influence the diagnostic yield and risk for complications.
2. Methods
This retrospective study was conducted at Sultan Qaboos Comprehensive Cancer Care & Research Centre (SQCCCRC), University Medical City, Muscat, Oman, from November 2021 to December 2024. Electronic patient records of all individuals who underwent CT-guided percutaneous transthoracic CNB of the lung were reviewed. Patients who underwent CNB with clear history of primary malignancy before the procedure and lung lesion(s) suspicious for being metastasis by chest CT scan as well as new cases of undiagnosed lung masses/nodules were included. Patients with probable metastatic disease were referred to Interventional Radiology unit, after discussion in the tumour boards. These lesions were either found to be enlarging in serial CTs or demonstrated metabolic activity on 18F FDG-PET/CT studies.
All patients underwent the CT-guided biopsy as per the standard protocols. All biopsies were performed using an 18-gauge coaxial core cutting needle device (Medcut, MEDAX S.R.L. Unipersonale, San Possidonio, Italy). Before the biopsy, bleeding profile including platelet count, activated partial thromboplastin time and international normalised ratio were checked along with other routine investigations. Patients were positioned appropriately in a multi-slice CT scanner (SOMATOM Force 128 Dual Source; Siemens Healthcare GmbH, Erlangen, Germany), based on the location of the lesion to enhance accessibility. Following this, a standard CT scan was carried out to locate, determine and mark the biopsy points on the body surface. The operator planned the puncture path with the intention of avoiding any damage to critical structures such as the ribs, blood vessels, interlobar fissures and intercostal nerves. When PET images were available, an accessible site with maximum avidity was chosen. The biopsies were performed independently by two senior consultants, with 22 and 15 years of experience in interventional radiology, respectively.
Details on the basic demographic data, primary cancer diagnosis, lesion specific attributes (location, size and nature), biopsy result, results of molecular studies and complications, if any, were collected. Specific procedure details such as the location of the lesion, depth from the skin, distance from the inner chest wall, patient placement during the procedure and the total number of needle passes were also documented. Furthermore, the pathological results after CNB were classified into three categories: malignant, benign and non-diagnostic result. In cases where a molecular analysis was requested, the samples were evaluated to determine if they were sufficient and suitable.
Descriptive analyses were performed to examine the demographic and clinical characteristics of the study population, and the frequencies and proportions were reported. Differences in the outcomes were examined using the Chi-squared test or Fisher's exact test, as applicable. A two-tailed P value ≤0.05 was considered statistically significant. R software (R Foundation, Vienna, Austria) was used for all analyses.
3. Results
A total of 105 patients were included in this study; 31 (29.5%) had undiagnosed lung nodules/masses. Primary malignancies were breast cancer in 27 (25.7%), gastrointestinal cancers in 14 (13.3%), lung cancer in 8 (7.6%) patients as well as other malignancies. The mean age was 60.05 ± 14.78 years, with a slight predominance of females (54.3%). Lesions were solitary in 61 (58.1%) and multiple in 44 (41.9%) patients [Table 1]. The biopsies were done in 44 patients (41.9%) positioned in supine [Fig. 1], 33 (31.4%) in prone and 18 (26.7%) in lateral positions [Fig. 2]. The biopsy results were negative for any diagnosis in 19 (18.1%) patients giving an overall diagnostic yield of 81.9%. Malignancy was confirmed in 76 (72.4%) patients while 10 (9.5%) patients were given other non-malignant diagnoses.
Axial non-contrast computed tomography image of the chest showing the biopsy needle in place in a patient with primary breast carcinoma, with the patient positioned supine. Histopathology confirmed a benign solitary fibrous tumour of the lung, consistent with a non-metastatic lesion.
Axial computed tomography image of the chest showing the biopsy needle in situ in a patient with primary breast carcinoma, with the patient placed in the left lateral decubitus position. Histopathology confirmed pulmonary metastasis.
The principal diagnosis did not show any significant association with the biopsy diagnostic yield (P = 0.280). The lowest diagnostic yield was observed for lesions suspected to be metastatic from nasopharyngeal carcinoma (66.7%). Mass/nodule size substantially affected the biopsy diagnostic yield (P = 0.003). Larger lesions exhibited better diagnostic yield; lesions measuring 2.1 to 5 cm and those above 5 cm had positive diagnostic yields of 93.9% (n = 31/33) and 91.3% (n = 21/23), respectively. Nodules with sizes between 1.1 and 2 cm had 79.3% (n = 23/29) positive diagnostic yield, while smaller lesions measuring 0.4 to 1 cm demonstrated the lowest yield with only 55.0% (n = 11/20) positive results. Additional parameters, including patient's age, gender, lesion morphology, location, skin-to-lesion distance, number of needle-passes and PET status did not demonstrate a significant correlation with the diagnostic yield. However, the diagnostic yield was highest in solid lesions (83.9%) compared to cavitary (75.0%), cystic (66.7%) and consolidative (60.0%) lesions (P = 0.220). Upper lobe and lower lobe lesions give a similar diagnostic yield of 84.2% and 85.1%, respectively. The diagnostic yield was marginally higher in lesions located less than 5 cm from the skin. Additionally, the diagnostic yield improved when multiple attempts were made to sample the lesion. PET guidance did not significantly affect yield (82% with PET versus 80.6% without PET; P = 0.800), though lesions with intense or very intense avidity had a 100% yield [Table 2].
Of the 31 cases of undiagnosed lung masses suspected to be primary lung malignancy, 21 requests were made for molecular analysis. Molecular analysis is not routinely requested for the metastatic lesions in the lung. All 21 samples (100%) were deemed adequate for molecular analysis, as the assays successfully generated repeatable and reliable data, with each sample yielding positive results.
Of 104 patients with available data on post-procedure complications, 30 (28.8%) encountered complications due to the procedure. Pneumothorax was the predominant complication affecting 22 individuals (21.2%). Haemoptysis occurred in 9 (8.7%) and haemothorax in 2 (1.9%) patients. Patients with undiagnosed lung masses were less likely to have complications compared to patients with other primary diagnoses (12.9% versus 35.6%; P = 0.019). Mass/nodule size was also significantly associated with complications (P = 0.001) with the smallest size group (0.4 to 1 cm) having the highest complication rate (60.0%). Deeper lesions of >5.1 cm were associated with a higher incidence of complications; however, this difference did not reach statistical significance (35.6%; P = 0.080). Interestingly, the number of passes did not correlate with complication rates, as those subjected to even a single puncture experienced a high 50.0% complication rate. Patients with positive biopsy results had lower complication rates compared to patients with negative results (22.4% versus 57.9%; P = 0.002) [Table 3]. Older age, gender, number of lesions, nature of the lesions, lower lobe localisation or pass number did not influence the incidence of pneumothorax. However, pneumothorax occurred more in lesions less than 1 cm in size (50.0%; P = 0.007) and the incidence was less in undiagnosed lung masses compared to secondary lesions (9.7% versus 26.0%; P = 0.060).
4. Discussion
This study found a good diagnostic yield from CT-guided lung CNBs with an acceptable complication rate. The diagnostic yield was comparable, when analysed both as an entire cohort and specifically in patients, with established malignancies presenting with new lung lesions. Small lesion size and deep location of the lesions were independent risk factors for non-diagnostic results of lung biopsy.
A network meta-analysis comparing sophisticated approaches on sampling of 79,519 nodules in 363 studies ranked CNB as the most effective method for diagnosing peripheral pulmonary lesions with a yield of 88.9%.^9^ A study from Brazil reported a higher diagnostic accuracy of 92.3% for CT-guided percutaneous 20-gauge CNB of pulmonary nodules smaller than 2 cm.^10^ Another retrospective study from Italy reported a diagnostic yield of 82.0% with 87.3% positivity for malignancy.^11^ In the current study, the overall diagnostic yield was 81.9% with confirmation of malignancy in 72.4%.
Notably, the primary diagnosis did not markedly influence the diagnostic yield. However, suspected metastasis from nasopharyngeal carcinoma had the lowest diagnostic yield. The nodule size was significantly associated with the biopsy diagnostic yield with lesions >2.1 cm giving a high yield. The diagnostic yield was highest in solid lesions compared to cavitary, cystic or consolidative lesions. The diagnostic yield was marginally higher in lesions located less than 5 cm depth from the skin. Additionally, the diagnostic yield improved when multiple attempts were made to sample the lesion. However, no substantial link could be identified between the diagnostic yield and variables such as patient's age, gender, nature of the mass, location, distance from the skin, number of passes and PET status. The diagnostic yield for lung nodules ≤10 mm in diameter is often affected by lobar and segmental location with superior segments of the lower lobes having the highest diagnostic yield and least in basal segments of the lower lobes.^12^ But in the current study no such differences were seen with upper lobe and lower lobe lesions giving a similar diagnostic yield.
In a recent study on the evaluation of pulmonary lesions in patients with a known malignancy, the overall diagnostic accuracy of CNB was 83.3%.^13^ In their patients, smaller lesion size, pneumothorax, high-grade pulmonary haemorrhage and haemoptysis were associated with unsuccessful biopsies.^13^ Another study reported three intrinsic features, basal localisation, smaller lesions and a low 18F-FDG uptake leading to a biopsy failure.^14^ Basal localisation is a limiting factor due to the greater respiratory motion in the vicinity with the diaphragm. Low PET avidity may represent a low cellular density present in some malignant lesions or the benign nature of the tissue.
Core biopsy provides a greater proportion of representative samples and offers a higher likelihood of successful sample extraction than fine needle aspiration biopsy (FNAB), and is a preferred method regardless of the higher rate of complications.^15^ However, a meta-analysis showed that, though CNB could achieve better sample adequacy than FNAB, CNB did not have any superiorities in items of diagnostic accuracy and safety.^16^ CNB may fail to detect some cancers, particularly in the case of large, intricate lesions or those featuring cysts and necrotic areas. This limitation may be due to the fact that CNB only samples a limited part of the lesion, and a surrounding collapsed lung or pneumonia can make it difficult to obtain a representative sample. Functional and metabolic imaging modalities such as 18F-FDG PET/CT can be utilised to overcome these challenges.
The utility of PET-CT prior to biopsies has been debated in many platforms. In a study on 340 patients, the use of PET-CT before the CNB led to significantly increased biopsy success rates in patients with a mass (OR = 7.01; P = 0.004), compared to a nodule (P = 0.498) or multiple nodules (P = 0.163).^5^ A study from Brazil showed that PET-CT-guided biopsy of lung lesions led to fewer inconclusive biopsies than CT-guided biopsy, with similar complication rates.^17^ Among the lesions sampled in the first round of biopsies, malignant results were observed in 78.7% in the PET-CT group versus 61.6% in the CT group.^17^ As per The European Association of Nuclear Medicine guidelines, one of the indications for doing a PET-CT is to select the region of tumour for biopsy which is most likely to yield diagnostic information.^18^ However, PET guidance in the current study did not improve the diagnostic yield (82% with PET versus 80.6% without PET). A similar observation was also noted in a report on 111 consecutive procedures where the accuracy for patients who underwent a PET/CT scan pre-biopsy was 94.8%, while it was 94% for those who did not.^19^ The reasons for this in the present study may be attributed to the fact that a high diagnostic accuracy had already been achieved through a well-planned CNB protocol at the SQCCCRC and additional aids were unlikely to significantly enhance the yield. Furthermore, other limitations such as challenges in accessing certain deep-seated lesions, respiratory motion during the procedure and small lesion size can impede precise guidance of the biopsy needle to the intended target, regardless of PET avidity. Nevertheless, lesions with intense or very intense avidity in the present study had a 100% yield.
In addition to the routine immunohistochemistry staining by the pathologist, molecular analysis (fluorescence in situ hybridisation and genomic mutational analyses/next generation sequencing) of the biopsy sample are useful to detect specific genetic or protein biomarkers that are required for individual patient-based treatment plan. In the current study, the CNB samples were adequate in all cases where molecular analysis was requested, with each sample yielding reliable and positive results. Similar results were reported in a study where 96.8% of samples with two or more passes of a lesion were found to be sufficient for molecular testing.^20^ Another study showed that CNB specimens were more likely to have sufficient sample for molecular testing compared to FNAB specimens.^21^
Complications of CNB of the lung include pneumothorax, pulmonary haemorrhage, haemoptysis, air embolism and tumour seeding. Various techniques such as normal saline tract sealant, tract plug, blood patch and rapid rollover and deep expiration and breath-hold on needle extraction can significantly reduce the risk of pneumothorax.^22^ The incidence of pneumothorax in the current study was acceptable (21.2%). A meta-analysis on 23,104 patients from 36 articles reports an overall pneumothorax incidence of 25.9% (range: 4.3–52.4%), with only 6.9% needing a chest tube placement.^23^ Decubitus position, a high number of needle passes and greater lesion-pleura distance are the usual risk factors for CNB-related complications. Most of the time these complications are minor and only few of them will require admission and definitive management. Older age, gender, number of lesions, nature of the lesions, lower lobe localisation or pass number did not influence the incidence of pneumothorax in this study. However, the pneumothorax occurred more in lesions less than 1 cm in size. Though deeper lesions of >5 cm were associated with a higher incidence of complications the difference did not reach statistical significance. On the same note, pneumothorax was reported as the most common complication of CT-CNB, being associated with a pleura-to-lesion distance >3 cm.^10^ Kim et al. also showed no association between the number of core biopsy samples obtained and postprocedural complications.^24^ Obstructive airway disease like asthma or emphysema increases the risk of iatrogenic pneumothorax. However, for this study data on pre-existing pulmonary co-morbidity was not collected.
In the near future, artificial intelligence will enable real-time lesion recognition, segmentation, automated needle-trajectory prediction and integration with robotic guidance especially with considerations of spatial relationships and patient-specific anatomical variation. These advances are expected to improve accuracy, consistency, efficiency and procedural safety.^2526^ Within this context, the findings of this study should be interpreted in light of several limitations. First, as a single-centre retrospective analysis, the findings may have limited generalisability. Second, there was no control group to compare other techniques for tissue diagnosis of pulmonary opacities. Third, patient cooperation and limited accessibility of centrally located lesions may have introduced bias. Fourth, although the sample size was reasonable, a larger cohort would have strengthened the conclusions. Finally, the true-positive and true-negative verification was not performed; therefore, the diagnostic accuracy, sensitivity and specificity were not assessed.
5. Conclusion
CT-guided lung CNB is a reliable and safe diagnostic procedure for undiagnosed lung lesions with a high diagnostic yield and an acceptable complication rate. The samples obtained with CT-guided CNBs were acceptable for both histopathology and molecular studies. The diagnostic yield was comparable when analysed both as an entire cohort and separately for patients with established malignancies and new metastatic lung lesions. The highest diagnostic accuracy was achieved in solid, shallower nodules.
Authors' Contribution
Raza Sayani: Conceptualization, Resources, Methodology, Investigation, Writing– Review & Editing, Supervision. Jayakrishnan B: Data Curation, Formal analysis, Writing– Original draft preparation, Review & Editing, Visualization, Supervision. Rashid Al Sukaiti: Conceptualization, Resources, Methodology, Investigation, Writing– Review & Editing, Supervision. Zahida Niaz: Methodology, Investigation, Data Curation, Writing– Review & Editing. Muhammad Sharjeel Usmani: Conceptualization, Methodology, Investigation, Writing– Review & Editing. Mustafa Talib Yousif Al Ani: Methodology, Data Curation, Writing– Review & Editing. Hasan Al-Sayegh: Data Curation, Formal analysis, Writing– Review & Editing. Subhash Chand Kherukaa: Investigation, Writing– Review & Editing
Ethics Statement
The study was approved by the Institutional Review Board and Ethics Committee of SQCCCRC (IRB & EC Project ID: CCCRC-77-2024)
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Saggiante L Biondetti P Lanza C Carriero S Ascenti V Piacentino F Computed-tomography-guided lung biopsy: A practice-oriented document on techniques and principles and a review of the literature. Diagnostics (Basel) 2024; 14:1089. 10.3390/diagnostics 14111089.38893616 PMC 11171640 · doi ↗ · pubmed ↗
- 2Gould MK. Biopsy of peripheral lung nodules - inside out or outside In? N Engl J Med 2025; 392:2162–3. https://doi.org/10.1056/NEJ Me 2504035.10.1056/NEJ Me 250403540387026 · doi ↗ · pubmed ↗
- 3Feng JL Fu YF Li Y. Computed tomography-guided biopsy for sub-centimetre pulmonary nodules: A meta-analysis. Kardiochir Torakochirurgia Pol 2023; 20:139–45. 10.5114/kitp.2023.131947.37937168 PMC 10626403 · doi ↗ · pubmed ↗
- 4Shimizu K Ikeda N Tsuboi M Hirano T Kato H. Percutaneous CT-guided fine needle aspiration for lung cancer smaller than 2 cm and revealed by ground-glass opacity at CT. Lung Cancer 2006; 51:173–9. https://doi.org/10.1016/j.lungcan.2005.10.019.10.1016/j.lungcan.2005.10.01916378659 · doi ↗ · pubmed ↗
- 5Stefanidis K Bellos I Konstantelou E Yusuf G Hardavella G Jacob T 18F-FDG PET/CT anatomic and metabolic guidance in CT-guided lung biopsies. Eur J Radiol 2024; 171:111315. https://doi.org/10.1016/j.ejrad.2024.111315.10.1016/j.ejrad.2024.11131538237515 · doi ↗ · pubmed ↗
- 6Intepe YS Metin B Sahin S Kaya B Okur A. Our transthoracic biopsy practices accompanied by the imaging process: The contribution of positron emission tomography usage to accurate diagnosis. Acta Clin Belg 2016; 71:214–20. https://doi.org/10.1080/17843286.2016.1155810.10.1080/17843286.2016.115581027142092 · doi ↗ · pubmed ↗
- 7Tamrazi A Sundaresan S Parvizi A Eller A Fujii J Shaheen Z Clinical value of CT-guided biopsy of small (≤1.5 cm) suspicious lung nodules: Diagnostic accuracy, molecular characterization and long-term clinical outcomes. Cancer Treat Res Commun 2022; 33:100626. 10.1016/j.ctarc.2022.100626.36041372 · doi ↗ · pubmed ↗
- 8Hui H Yin HT Wang T Chen G. Computed tomography-guided core needle biopsy for sub-centimeter pulmonary nodules. Kardiochir Torakochirurgia Pol 2022; 19:65–9. 10.5114/kitp.2022.117492.35891992 PMC 9290407 · doi ↗ · pubmed ↗