Post-Traumatic Pituitary Stalk Transection Syndrome
Raya Albusaidi, Asma AlHatmi, Azza Al Shidhani, Eiman Al-Ajmi

Abstract
Click any figure to enlarge with its caption.
 Figure 1
Figure 1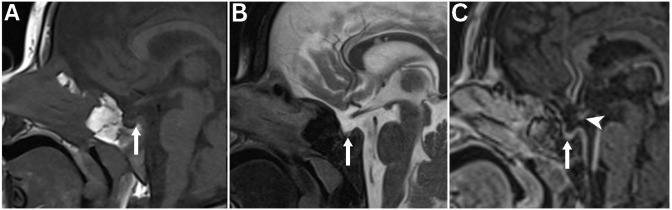 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGrowth Hormone and Insulin-like Growth Factors · Pituitary Gland Disorders and Treatments · Nerve injury and regeneration
A 15-month-old girl who had normal developmental milestones and no significant medical history was run-over by a car in 2023 in Oman; she sustained a head injury and was transferred to a community hospital for further management. Computed tomography (CT) was done immediately after the trauma and revealed fractures through the central skull base in the sphenoidal bone involving the tuberculum sella and extending to right greater wing of the sphenoid. In addition, there was a fracture of left temporal bone with opacification of left mastoid air cells and middle ear. Pneumocephalus in the suprasellar region and anterior and middle cranial fossa was present [Fig. 1]. The patient was managed conservatively and discharged after 1 week.
The patient developed polydipsia 2 weeks post-discharge which resolved spontaneously. She presented to a tertiary care centre in Muscat, Oman, 6 weeks after the trauma with suppurative otitis media. Due to the history of head trauma and the polydipsia, she was screened for post-traumatic hypopituitarism. She was found to have early morning hypoglycaemia (2.9 mmol/L). Her input and output fluid chart was normal with a urine output of 2.4 mL/kg/hour. Laboratory tests revealed central hypothyroidism (thyroid-stimulating hormone = 0.34 mIU/L, free thyroxine = 3.7 pmol/L). Low dose synacthen test revealed severe adrenocorticotropin hormone (ACTH) deficiency with a baseline serum cortisol of 10 mmol/L, a 60-minutes peak of 88 mmol/L and ACTH <1 ng/L. She was started on hydrocortisone replacement therapy for 5 days then followed by levothyroxine replacement. No polyurea or polydipsia was noticed after starting the hydrocortisone and her electrolytes remained stable (serum sodium = 138 mmol/L [normal range: 135–145 mmol/L], serum potassium = 4.5 mmol/L [normal range: 3.6–5.3 mmol/L]).
At 1-year follow-up, she was on cortisol and levothyroxine replacement with stable thyroid function. She was noticed to have plateauing of her height on the growth chart; subsequently, insulin-like growth factor (IGF)-1, IGF binding protein 3 (IGFBP3) and two growth hormone stimulation tests were done (clonidine and arginine). She was proven to have growth hormone deficiency with a very low growth hormone peak of 0.12 mIU/L, IGF-1 of 35 ng/mL (normal range: 45–305 ng/mL) and an IGFBP3 of 0.8 mg/L (normal range: 0.8–3.9 mg/L). Hence, growth hormone replacement therapy was started.
Considering the clinical and lab findings, magnetic resonance imaging (MRI) of the brain was done and showed a small anterior pituitary gland measuring 2 mm in height. T1 hyperintensity of the posterior pituitary was absent. In addition, the infundibulum was interrupted and only the upper third of the infundibulum was present at the level of the hypothalamus [Fig. 2].
1. Comment
Traumatic brain injury (TBI) is a significant public health concern, with potentially devastating consequences for affected individuals. Among the myriad complications arising from TBI, an often overlooked yet clinically significant sequela is pituitary dysfunction.
Clinical research has highlighted a substantial incidence of hypopituitarism among survivors of TBI. According to a systematic review, the prevalence of hypopituitarism following TBI has been reported to range from 27–31%.^1^ However, various studies have demonstrated a highly variable prevalence of pituitary dysfunction among TBI survivors. Rai et al.'s prospective study evaluated the incidence of hypopituitarism in 86 patients with moderate to severe TBI, both at admission and at a 6-month follow-up.^2^ They found that the thyroid and gonadotropin axis were the most commonly affected, with at least one hormonal axis deficient in 82.4% of patients during the acute phase and in 59.3% during the chronic phase.^2^
The exact pathophysiology of post-traumatic hypopituitarism remains unclear; however, the presence of brain oedema, diffuse axonal injury, intracranial haemorrhage and skull base fractures are important predicting factors. In addition to the primary mechanical injury, secondary factors such as hypotension, hypoxia, elevated intracranial pressure, alterations in cerebral perfusion and metabolism as well as ischaemic damage and necrosis may play a role in hypothalamic-pituitary impairment.^3^ If pituitary deficiency is confirmed, use of standard paediatric regimens for replacement is recommended (hydrocortisone for ACTH deficiency, before starting levothyroxine or growth hormone therapy).^3^
A rare form of post-traumatic pituitary dysfunction is post-traumatic pituitary stalk interruption syndrome (PSTS), as in the present case, which is caused by mechanical transection or damage of the pituitary stalk that is most likely related to the central skull base fracture, as documented in the CT at the time of trauma. PSTS is distinct from other forms of pituitary dysfunction after TBI due to the characteristic MRI findings.^4^
Pituitary stalk interruption syndrome (PSIS) is a genetic developmental disorder causing combined pituitary hormone deficiency (CPHD), marked on MRI by a triad: (1) absent or thin pituitary stalk, (2) underdeveloped anterior pituitary and (3) absent or ectopic posterior pituitary. It often coexists with midline brain defects.^5^
In contrast, post-traumatic PSTS is a rare acquired cause of CPHD due to head trauma.^45^ The current case demonstrates direct injury to the sellar area, resulting in imaging manifestations that are well-documented by MRI. MRI findings of PSTS can resemble the MRI features of PSIS which can lead to diagnostic challenges posed by these similarities. Correlation with clinical and past traumatic history and absence of midline brain malformations are the key in distinguishing the two. The MRI findings of PSTS typically include a transacted pituitary stalk, which may show a hyperintense signal from regenerating nerve fibres at the median eminence if the cut is proximal, or be invisible if the stalk is severed higher up, a small (hypotrophic) anterior pituitary lobe and an absent posterior pituitary due to ischaemic and neurotrophic atrophy.^5^
In summary, the present case emphasises the importance of closely monitoring patients with moderate to severe TBI for pituitary hormonal abnormalities, which allows early detection and treatment with hormone replacement, as well as planning long-term care. Furthermore, this case highlights the importance of MRI in identifying the characteristic imaging findings of PSTS as a unique post-TBI cause of pituitary dysfunction.
Authors' Contribution
Raya Albusaidi: Writing - Original Draft, Data Curation. Asma AlHatmi: Writing - Original Draft, Data Curation, Supervision. Azza Al Shidhani: Investigation, Data Curation, Writing - Review & Editing. Eiman Al-Ajmi: Conceptualization, Methodology, Data Curation, Writing - Review & Editing, Visualization, Supervision.
Ethics Statement
Informed consent was obtained from the patient's parent.
Data Availability
Data are available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Glynn N Agha A. The frequency and the diagnosis of pituitary dysfunction after traumatic brain injury. Pituitary 2019; 22:249–60. https://doi.org/10.1007/s 11102-019-00938-y.10.1007/s 11102-019-00938-y 30684166 · doi ↗ · pubmed ↗
- 2Rai A Rajasekar G Sahoo J Kumari MM Anbazhagan S. Anterior pituitary dysfunction after Traumatic Brain injury: a prospective study. World Neurosurg 2024; 190:e 588–94. https://doi.org/10.1016/j.wneu.2024.07.186.10.1016/j.wneu.2024.07.18639094934 · doi ↗ · pubmed ↗
- 3Sav A Rotondo F Syro LV Serna CA Kovacs K. Pituitary pathology in traumatic brain injury: a review. Pituitary 2019; 22:201–11. https://doi.org/10.1007/s 11102-019-00958-8.10.1007/s 11102-019-00958-830927184 · doi ↗ · pubmed ↗
- 4Ishiki Y Tamaki A Honma KI Yonaha K Yabiku T Teruya T Post-traumatic pituitary stalk transection syndrome (PSTS) expeditiously manifested after a fall from a height combined with acute traumatic spinal cord injury: a rare case report with review of literature. Endocr J 2024; 71:817–24. https://doi.org/10.1507/endocrj.ej 24-0091.10.1507/endocrj.EJ 24-009138811206 · doi ↗ · pubmed ↗
- 5Ruszala A Wojcik M Krystynowicz A Starzyk J. Distinguishing between post-trauma pituitary stalk disruption and genetic pituitary stalk interruption syndrome – case presentation and literature overview. Pediatr Endocrinol Diabetes and Metabo 2019; 25:155–62. 10.5114/pedm.2019.87708.31769274 · doi ↗ · pubmed ↗