Cutibacterium acnes as a cause of late prosthetic valve endocarditis: a case report
Amir Hakanovic, Filipe Patricio, Andres Spirig, Michel Zuber, Tobias A Fuchs

TL;DR
A rare case of late prosthetic valve endocarditis caused by Cutibacterium acnes is reported, highlighting the challenges in diagnosis and treatment.
Contribution
This case report presents a rare instance of late-onset endocarditis caused by Cutibacterium acnes following aortic valve replacement.
Findings
Cutibacterium acnes was identified as the causative agent in a late prosthetic valve endocarditis case.
The patient required re-operation due to a pseudoaneurysm caused by composite graft dehiscence.
Multimodal imaging and surgical intervention were crucial in managing the infection.
Abstract
Dehiscence of a composite graft following aortic valve (AV) and ascending aorta replacement represents a rare but potentially life-threatening complication. The need for re-operation after a Bentall procedure is usually related to the development of an endocarditis, formation of (pseudo)aneurysms, or recurrent dissection. We report a rare case of late pseudoaneurysm formation due to Cutibacterium acnes (C. acnes) endocarditis. A 52-year-old man was admitted to the emergency department due to dizziness, diplopia, right-sided hemiparesis, and dysarthria. Five and a half years ago, the patient underwent a replacement of the AV and entire ascending aorta due to a bicuspid AV with combined valvular disease and ascending aortic aneurysm. Transthoracic echocardiography revealed a large, perfused posterior pseudoaneurysm caused by the dehiscence of the composite graft, while the mechanical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
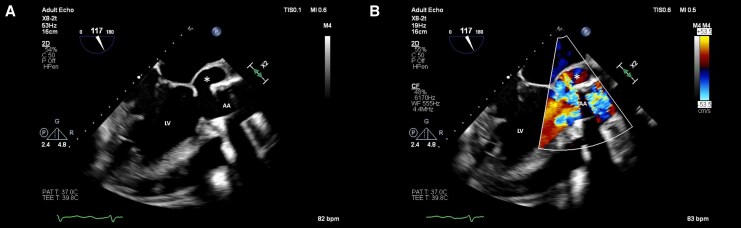 Figure 1
Figure 1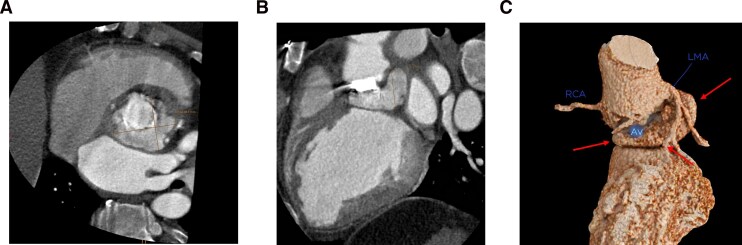 Figure 2
Figure 2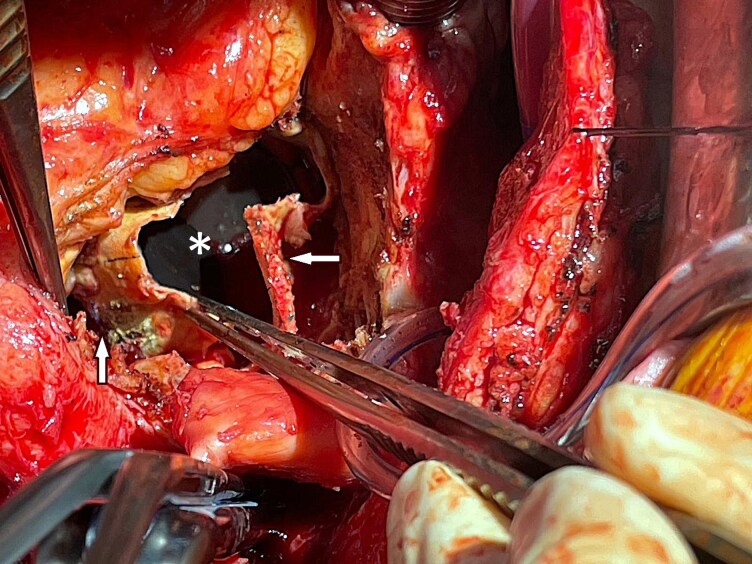 Figure 3
Figure 3| 5.5 years prior | Symptomatic severe aortic valve insufficiency with moderate stenosis due to a bicuspid valve. Severely dilated left ventricle (LV) with severely impaired left ventricle ejection fraction (20%). Ascending aortic aneurysm (60 mm) |
| Annual follow-up | First post-operative follow-up and subsequent annual evaluations showed good function of the mechanical aortic valve prosthesis, with an improved left ventricular ejection fraction of 36% |
| Day 0 | Presentation with transient ischaemic attack (dizziness, diplopia, right-sided hemiparesis, and dysarthria) |
| Day 1 | Fever (38°C), transthoracic and transoesophageal echocardiography revealed the dehiscence of the composite graft with a perfused subvalvular pseudoaneurysm. Blood cultures revealed |
| Day 19 | Re-operation with debridement and mechanical composite graft reconstruction in the modified Bentall technique with a 25 mm valve prosthesis (Medtronic AVG conduit) and reimplantation of the coronary arteries. In addition, hemiarch replacement was carried out, and a single coronary artery bypass graft (CABG) was performed using the left internal mammary artery (LIMA) to the left anterior descending artery (LAD) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Infective Endocarditis Diagnosis and Management · Orthopedic Infections and Treatments
Introduction
Dehiscence of a composite graft following aortic valve and ascending aorta replacement is a rare but potentially life-threatening complication.^1^ In this report, we describe a patient who developed a pseudoaneurysm due to Cutibacterium acnes (C. acnes) endocarditis, 5.5 years after the initial operation.
Cutibacterium acnes is a slow-growing, gram-positive anaerobe bacterium that belongs to the normal skin flora and has the ability to form biofilms. Over recent years, it has become increasingly recognized as a clinically relevant microorganism in delayed post-surgical infections, particularly in the context of cardiac surgery and prosthetic material.^2^
One of the challenges in diagnosing C. acnes endocarditis lies in the subtle or even absent clinical signs of systemic inflammation. Its low virulence, biofilm production, and slow growth can allow the infection to persist silently over extended periods—sometimes months or even years—before clinical symptoms emerge.^3^
Treatment generally requires prolonged antibiotic therapy. Cutibacterium acnes typically shows susceptibility to beta-lactam antibiotics such as penicillins and cephalosporins. However, in cases with complications like graft dehiscence or pseudoaneurysm formation, surgical intervention is frequently necessary.^4,5^
Summary figure
**: **
Case presentation
A 52-year-old man presented to the emergency department with acute-onset dizziness, diplopia, right-sided hemiparesis, and dysarthria. His past medical history revealed a replacement of the aortic valve (AV) (Medtronic STD MITRAL, Model 500D) and entire ascending aorta (intervascular, bulged graft, 34 mm, Intergard Woven 28 mm) replacement using the button technique due to combined AV disease in the setting of a bicuspid AV and ascending aortic aneurysm. Two months prior, routine cardiologic examination had shown normal prosthetic valve function with mildly reduced left ventricular systolic function. On admission, the patient was hypertensive (147/88 mmHg), in normal sinus rhythm (80 bpm), and febrile (38°C). His skin was unremarkable. Neurological examination revealed right-sided hemiparesis and dysarthria. Laboratory work-up demonstrated elevated inflammatory markers.
An urgent cranial computed tomography (CT) with extracranial computed tomography angiography (CTA) ruled out intracranial haemorrhage, perfusion deficit, and high-grade stenosis of the cerebral arteries. A followed transthoracic and transoesophageal echocardiography (TTE/TOE) revealed a large, perfused, posterior pseudoaneurysm with partial dehiscence of the composite graft. The left ventricle was severely dilated with moderately reduced systolic function (biplane ejection fraction 36%). No oscillating structures or thrombotic deposits were detected (Figure 1/see Supplementary material online, Video S1).
(A) Two-dimensional transoesophageal echocardiography demonstrating a dehiscence of the composite graft. (B) Colour Doppler imaging showing perfusion of the subvalvular pseudoaneurysm. LV, left ventricle; AA, ascending aorta; asterisk (), pseudoaneurysm.*
In summary, the patient met one major modified Duke criterion (dehiscence of the composite graft) and four minor criteria [fever, positive rheumatoid factor, transient ischaemic attack, and a predisposing cardiac condition (prosthetic graft)], fulfilling the definition of definitive prosthetic valve endocarditis. After obtaining blood cultures, empiric intravenous antibiotic therapy with amoxicillin/clavulanic acid (6 × 2.2 g/day) was initiated.
Following a multidisciplinary endocarditis team discussion, surgical intervention was recommended. Preoperative work-up included CT imaging of the coronary arteries and thoracic aorta, confirming dehiscence of the mechanical composite graft with formation of a paravalvular pseudoaneurysm and suspected periprosthetic abscess formation along the ascending aortic graft (Figure 2).
Multiplanar reconstructions (A, axial; B, coronal) and 3D rendering (C) of electrocardiogram -gated computed tomography angiography of the heart and the ascending aorta showing a subvalvular, perfused pseudoaneurysm (arrows) measuring 5.9 × 4.8 × 3.3 cm. AV, aortic valve; RCA, right coronary artery; LMA, left main artery.
Invasive coronary angiography revealed a significant stenosis in the mid-LAD.
In the further course, the patient developed acute cholecystitis, which was treated conservatively and led to a delay of the planned surgery. After 8 days, blood cultures showed growth of C. acnes, and the antibiotic therapy was adjusted according to the resistance profile to ceftriaxone 2 g/24 h.
Finally, a re-operation was performed, which included debridement and mechanical composite graft reconstruction using the modified Bentall technique with a 25 mm valve prosthesis and reimplantation of the coronary buttons (Medtronic AVG conduit). Hemiarch replacement was carried out under deep hypothermic circulatory arrest (DHCA) with a 28 mm sidearm graft (Gelweave). A single CABG was performed using the left internal mammary artery to the LAD (Figure 3). The patient was placed on long-term antibiotics, made an uneventful recovery, and was subsequently discharged to cardiac rehabilitation.
Intraoperative view showing the mechanical aortic valve prosthesis (), the ascending aortic graft (left arrow), and the pseudoaneurysm cavity after surgical debridement (right arrow).*
Discussion
Prosthetic valve endocarditis after a Bentall procedure is a severe complication that should be suspected in the presence of paravalvular abnormalities, as separation of the prosthetic valve from the conduit is often not feasible. Periannular involvement and paravalvular leakage are common findings in prosthetic valve endocarditis.^6^
Dehiscence of a composite graft is a rare but serious complication (occurring in 1%–3% of cases) following AV and aortic replacement, and it is associated with a high mortality rate.^1,6^
In this case, the infection with the slow-growing C. acnes (which has a median time-to-positivity of around 7 days, prompting some experts to recommend extended incubation for blood cultures) led to the formation of a pseudoaneurysm.^7^
Cutibacterium acnes is part of the skin’s normal flora, and it is a slow-growing bacterium capable of forming biofilms. Saha et al.^8^ reported that C. acnes is responsible for 3.1% of endocarditis cases, making it comparable in prevalence to the HACEK group. Recently C. acnes has been considered as a typical microorganism in infective endocarditis (IE) in the presence of intracardiac prosthetic material.^9^ Since patients often present without the typical signs of inflammation, diagnosing C. acnes endocarditis can be particularly challenging.^7^
The diagnosis of endocarditis is made according to the modified Duke criteria. The first-line imaging modality is TTE. If TTE results are negative or non-diagnostic and clinical suspicion remains high, or if there is a prosthetic valve or cardiac implantable electronic device (CIED), TOE is recommended. If TOE is inconclusive or there is suspicion of paravalvular or periprosthetic complications, a cardiac CT scan is recommended.^10^
Transoesophageal echocardiography is more effective than CT in detecting valvular lesions, especially small vegetations (<10 mm) and valve perforations. Another advantage of TOE is that it does not expose the patient to radiation or contrast agents. However, in the case of prosthetic valves, the accuracy of TOE can be reduced due to the acoustic shadowing caused by the prosthetic material.
Computed tomography, on the other hand, has a high sensitivity for detecting paravalvular lesions and is superior to TOE when it comes to identifying complications such as abscesses, pseudoaneurysms, and fistulas. Computed tomography is also less invasive for the patient and provides a comprehensive view of extracardiac structures and coronary arteries, which is critical for surgical planning.^11,12^
In addition to echocardiography and cardiac CT, positron emission tomography/computed tomography (PET/CT) plays an important role in the diagnostic work-up of prosthetic valve endocarditis, particularly when echocardiographic findings are inconclusive. PET/CT provides incremental diagnostic value by detecting inflammatory activity at the prosthetic valve and periprosthetic tissues and may help reclassify cases categorized as ‘possible’ IE by the modified Duke criteria.^10^
The management of C. acnes endocarditis typically involves a combination of antibiotic therapy and surgical intervention when indicated. First-line antibiotics for C. acnes infections include penicillin, ceftriaxone, and rifampicin.^4,5^
The role of C. acnes in this case emphasizes the importance of extended blood culture incubation and thorough imaging when prosthetic endocarditis is suspected. Although C. acnes is less virulent than other pathogens, untreated infections can lead to severe complications, including abscesses or pseudoaneurysms. In this case, a surgical revision, involving radical debridement and reimplantation of the composite graft, was necessary for successful management.
Conclusion
This case underscores several important aspects in prosthetic valve endocarditis. While late-onset C. acnes infection is uncommon, its potential for atypical presentations—including neurological symptoms—poses diagnostic challenges. The slow-growing, biofilm-forming nature of the pathogen highlights the need for prolonged blood culture incubation. A combination of multimodality imaging, microbiological diagnostics, and interdisciplinary therapy is crucial for successfully managing such complications. By sharing this case, we aim to reinforce clinical awareness, support early recognition, and provide practical insights for the management of similar patients with cardiovascular implants.
Supplementary Material
ytag214_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mohammadi S, Bonnet N, Leprince P, Kolsi M, Rama A, Pavie A, et al Reoperation for false aneurysm of the ascending aorta after its prosthetic replacement: surgical strategy. Ann Thorac Surg 2005;79:147–152; discussion 152.15620933 10.1016/j.athoracsur.2004.06.032 · doi ↗ · pubmed ↗
- 2Mayslich C, Grange PA, Dupin N. Cutibacterium acnes as an opportunistic pathogen: an update of its virulence-associated factors. Microorganisms 2021;9:303.33540667 10.3390/microorganisms 9020303 PMC 7913060 · doi ↗ · pubmed ↗
- 3Achermann Y, Goldstein EJ, Coenye T, Shirtliff ME. Propionibacterium acnes: from commensal to opportunistic biofilm-associated implant pathogen. Clin Microbiol Rev 2014;27:419–440.24982315 10.1128/CMR.00092-13PMC 4135900 · doi ↗ · pubmed ↗
- 4Lindell F, Söderquist B, Sundman K, Olaison L, Källman J. Prosthetic valve endocarditis caused by Propionibacterium species: a national registry-based study of 51 Swedish cases. Eur J Clin Microbiol Infect Dis 2018;37:765–771.29380224 10.1007/s 10096-017-3172-8PMC 5978902 · doi ↗ · pubmed ↗
- 5Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: an underestimated pathogen in implant-associated infections. Biomed Res Int 2013;2013:804391.24308006 10.1155/2013/804391 PMC 3838805 · doi ↗ · pubmed ↗
- 6Croon SI, Angkasuwan A, van Straten AH, Khamooshian A, Elenbaas TW, Soliman-Hamad MA. Surgical treatment and long-term outcome of aortic valve endocarditis with periannular abscess. Neth Heart J 2020;28:345–353.32198643 10.1007/s 12471-020-01409-x PMC 7270477 · doi ↗ · pubmed ↗
- 7Heinen FJ, Arregle F, van den Brink FS, Ajmone Marsan N, Bernts L, Houthuizen P, et al Clinical characteristics and outcomes of patients with Cutibacterium acnes endocarditis. JAMA Netw Open 2023;6:e 2323112.37436747 10.1001/jamanetworkopen.2023.23112 PMC 10339155 · doi ↗ · pubmed ↗
- 8Saha S, Joskowiak D, Marin-Cuartas M, De La Cuesta M, Weber C, Luehr M, et al Cutibacterium acnes infective endocarditis—an emerging pathogen. Eur J Cardiothorac Surg 2024;66:ezae 422.39585651 10.1093/ejcts/ezae 422 · doi ↗ · pubmed ↗