Association between systemic inflammation biomarkers and outcomes in patients with aneurysmal subarachnoid hemorrhage
Maria Della Giovampaola, Andrea Vieno, Adeline Higuet, Irene Cavalli, Claudia Stella, Giacomo Coppalini, Alberto Diosdado, Daniel Damasceno, Lucas Freitas, Fernando Oliveira Gomes, Ana Carolina Damasceno Lacerda Fernandes, Marcos Vinicius Tavares De Magalhães

TL;DR
This study shows that higher levels of systemic inflammation biomarkers CRP and NLr are linked to worse outcomes in patients with aneurysmal subarachnoid hemorrhage.
Contribution
The study demonstrates that CRP and NLr are independently associated with unfavorable neurological outcomes and delayed cerebral ischemia in aSAH patients.
Findings
Elevated CRP levels from days 2 to 7 after SAH were independently linked to unfavorable outcomes.
Higher NLr values were associated with both unfavorable outcomes and delayed cerebral ischemia.
CRP and NLr levels reinforce inflammation's role in secondary brain injury after aSAH.
Abstract
Aneurysmal subarachnoid hemorrhage (aSAH) is a devastating condition that is associated with cerebral and systemic inflammation. C-reactive protein (CRP) and neutrophil-to-lymphocyte ratio (NLr) are easily available biomarkers of systemic inflammation. Therefore, we aimed to assess the impact of elevated CRP and NLr on aSAH outcomes. This retrospective, single-center study included adult patients admitted with aSAH to the intensive care unit (ICU) from January 2007 to December 2023. We recorded serum CRP and NLr levels during the first 7 days of ICU stay. An unfavorable neurological outcome at 3 months was defined as a Glasgow Outcome Scale (GOS) score of 1–3. A total of 547 patients were included in the study; 250 (45.7%) experienced unfavorable outcomes (UOs), and 140 (25.6%) developed delayed cerebral ischemia (DCI). Patients with unfavorable outcomes had higher levels of CRP from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
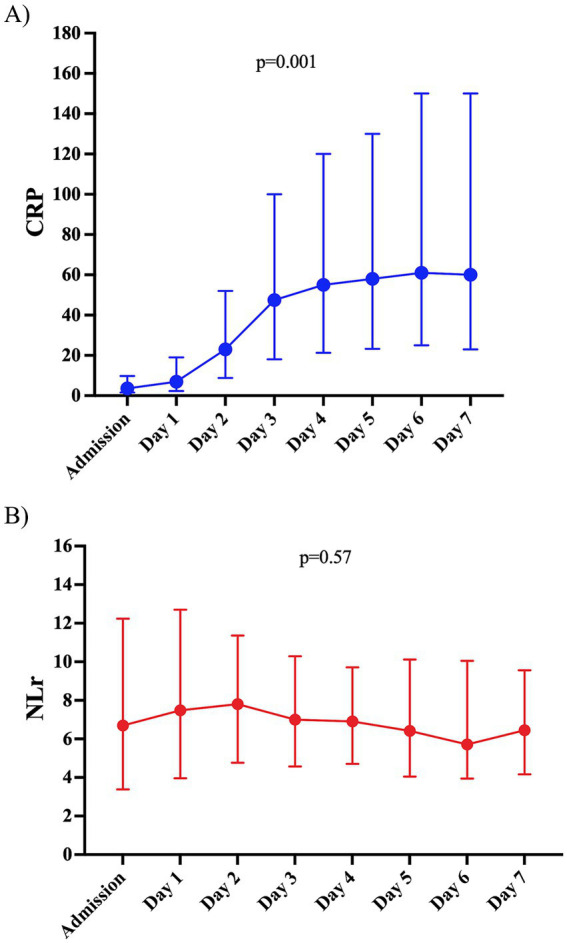 Figure 1
Figure 1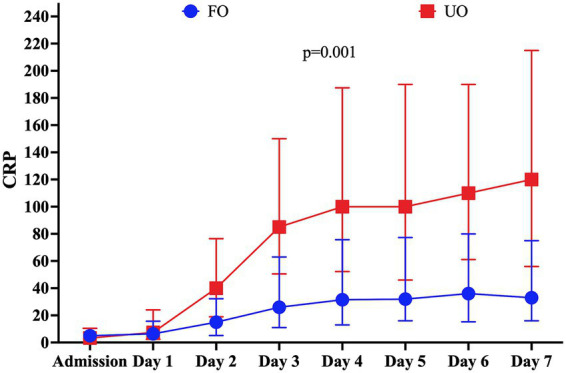 Figure 2
Figure 2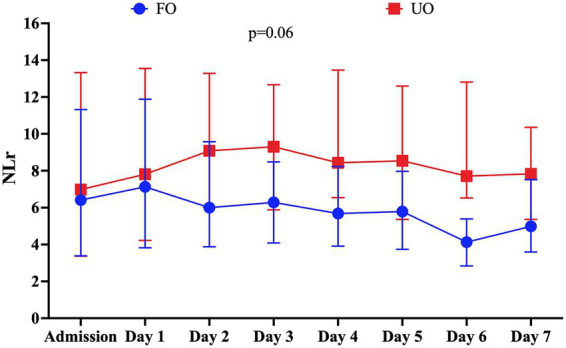 Figure 3
Figure 3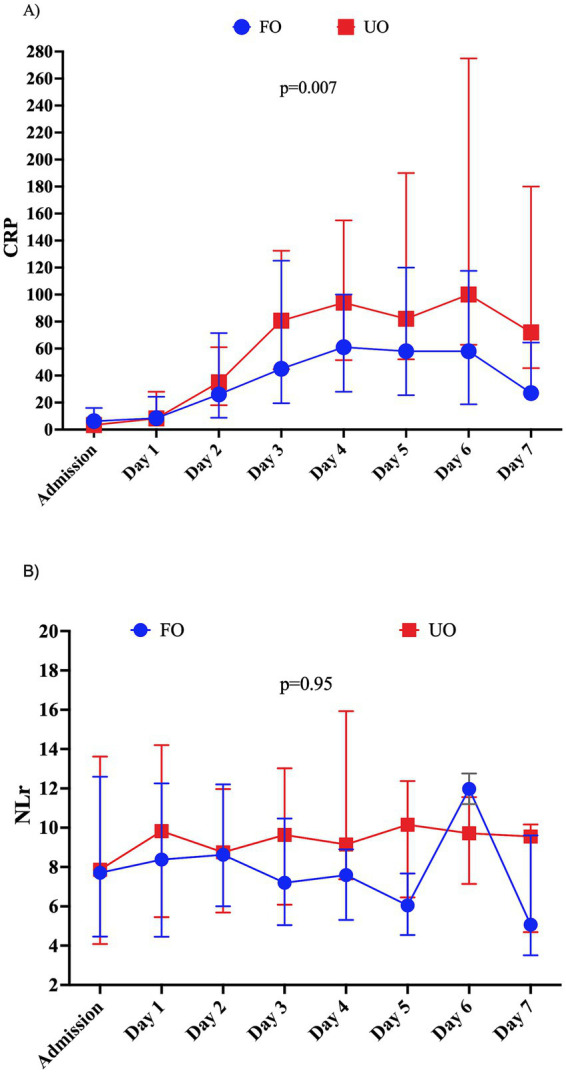 Figure 4
Figure 4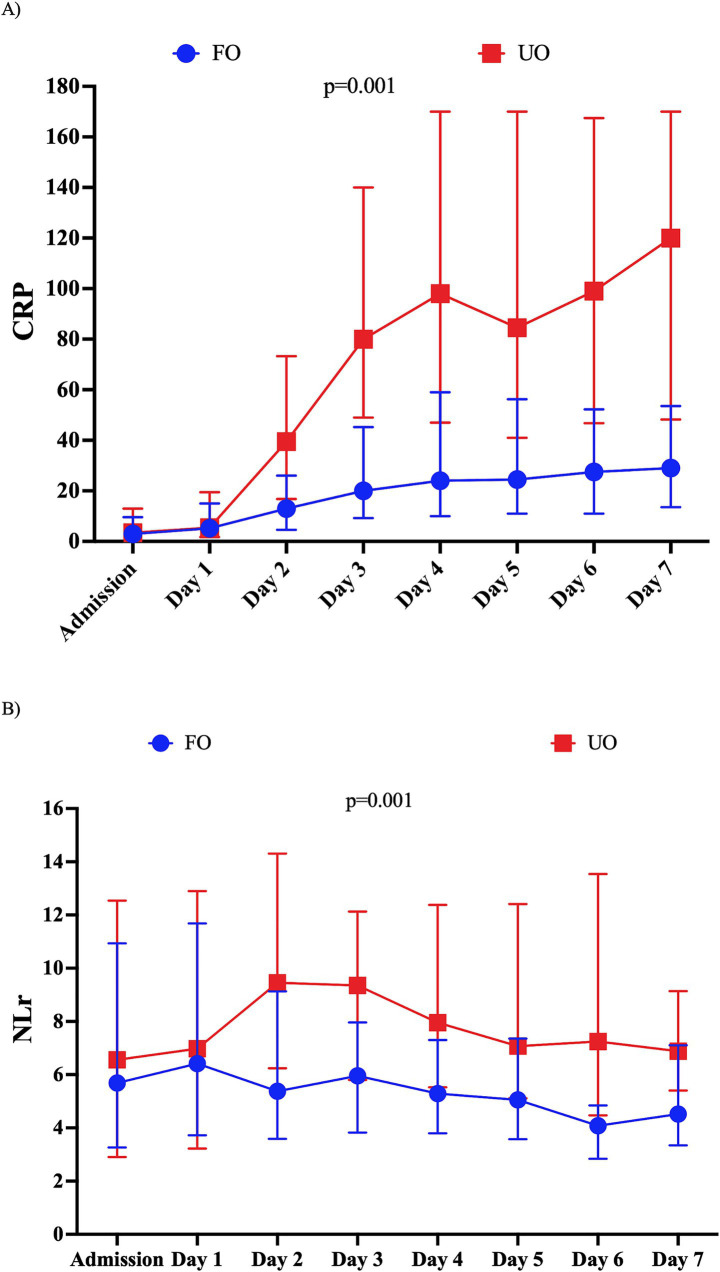 Figure 5
Figure 5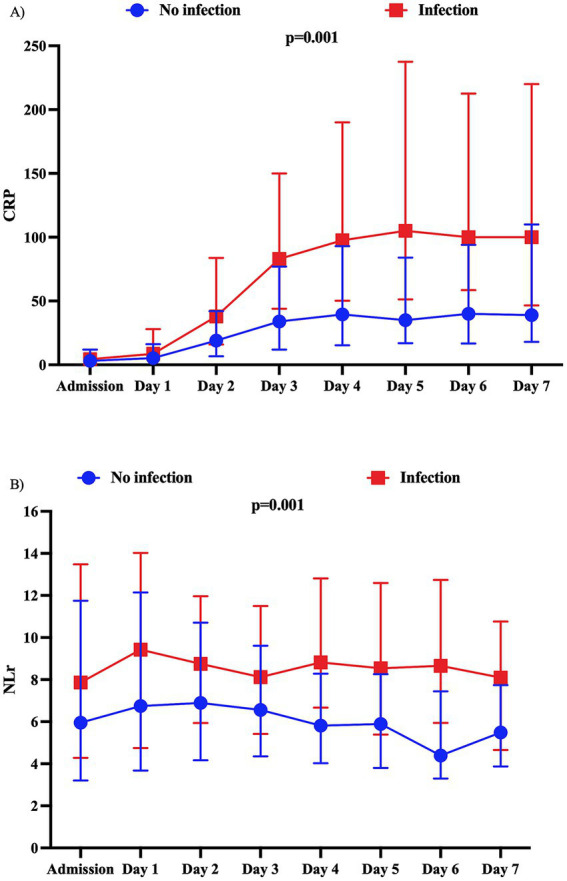 Figure 6
Figure 6| Variables | All patients ( | Favorable outcome ( | Unfavorable outcome ( | |
|---|---|---|---|---|
| Age (years), median (IQR: 25–75%) | 54 (45; 62.8) | 52 (43; 59) | 57 (49; 67) | 0.001 |
| Female, | 338 (61.8) | 120 (40.4) | 161 (64.4) | 0.253 |
| APACHE II, median (IQR: 25–75%) | 12 (7; 18.5) | 8 (5; 12) | 18 (13; 21) | 0.001 |
| SOFA score, median (IQR: 25–75%) | 4 (1; 8) | 2 (1; 4) | 8 (5; 9.8) | 0.001 |
| GCS, median (IQR) | 13 (4; 15) | 15 (13; 15) | 5 (3; 13) | 0.001 |
| mFisher score of 3–4, | 494 (90.3%) | 253 (85.2%) | 241 (96.4) | 0.001 |
| WFNS score of 4–5, | 249 (45.5%) | 65 (21.9%) | 184 (73.6) | 0.001 |
| Nimodipine | 475 (86.8) | 284 (95.6) | 191 (76.4) | 0.001 |
| Aneurysm treatment, | 0.009 | |||
| Endovascular treatment of aneurysm | 480 (87.8) | 271 (91.2) | 209 (83.6) | |
| Surgical treatment of aneurysm | 67 (12.2) | 26 (8.8) | 41 (16.4) | |
| Comorbidities, | ||||
| Arterial hypertension | 231 (42.2) | 130 (43.8) | 101 (40.4) | 0.434 |
| Diabetes | 45 (8.2) | 14 (4.7) | 31 (12.4) | 0.002 |
| Heart disease | 63 (11.5) | 27 (9.1) | 36 (14.4) | 0.060 |
| Previous ND | 38 (7) | 18 (6.1) | 20 (8) | 0.403 |
| Chronic renal failure | 9 (1.7) | 5 (1.7) | 4 (1.6) | 0.990 |
| COPD | 47 (8.6) | 24 (8.1) | 23 (9.2) | 0.650 |
| Cancer | 26 (4.8) | 13 (4.4) | 13 (5.2) | 0.691 |
| Liver cirrhosis | 7 (1.3) | 2 (0.7) | 5 (2) | 0.256 |
| ICU management, | ||||
| Vasopressors | 305 (55.8) | 91 (30.6) | 214 (85.6) | 0.001 |
| Inotropic agents | 89 (16.3) | 19 (6.4) | 70 (28) | 0.001 |
| Mechanical ventilation | 316 (57.8) | 87 (29.3) | 229 (91.6) | 0.001 |
| Renal replacement therapy | 2 (0.4) | 0 (0) | 2 (0.8) | 0.208 |
| Complications, | ||||
| Seizures | 128 (23.4) | 53 (17.9) | 75 (30) | 0.001 |
| Rebleeding | 37 (6.8) | 6 (2) | 31 (12.4) | 0.001 |
| Hydrocephalus | 185 (33.8) | 71 (23.9) | 114 (45.6) | 0.001 |
| Cerebral vasospasm | 218 (39.9) | 115 (38.7) | 103 (41.2) | 0.540 |
| Delayed cerebral ischemia | 140 (25.6) | 39 (13.1) | 101 (40.4) | 0.001 |
| Intracranial hypertension | 216 (39.5) | 45 (15.2) | 171 (68.4) | 0.001 |
| Anti-seizure prophylaxis | 377 (68.9) | 191 (64.3) | 186 (74.4) | 0.009 |
| Treatment for complications, | ||||
| Hypothermia | 50 (9.1) | 3 (1) | 47 (18.8) | 0.001 |
| Decompressive craniectomy | 29 (5.3) | 5 (1.7) | 24 (9.6) | 0.001 |
| Barbituric coma | 73 (13.4) | 3 (1) | 70 (28) | 0.001 |
| Hyperventilation | 166 (30.4) | 21 (7.1) | 145 (58) | 0.001 |
| Osmotic therapy | 157 (28.7) | 21 (7.1) | 136 (54.4) | 0.001 |
| IA spasmolytic for vasospasm | 96 (17.6) | 32 (10.8) | 64 (25.6) | 0.001 |
| Angioplasty for vasospasm | 47 (8.6) | 22 (7.4) | 25 (10) | 0.289 |
| Induced hypertension for DCI | 155 (28.3) | 50 (16.8) | 105 (42) | 0.001 |
| Infections, | ||||
| All | 149 (27.2) | 55 (18.5) | 94 (37.8) | 0.001 |
| Pneumonia | 80/149 (53.7) | 21/55 (38.2) | 59/94 (62.8) | 0.004 |
| Urinary tract infection | 42/149 (28.2) | 19/55 (34.5) | 23/94 (24.5) | 0.164 |
| BSI | 20/149 (13.4) | 14/55 (25.5) | 6/94 (6.4) | 0.01 |
| CNS infection | 5/149 (3.4) | 1 (1.8) | 4/94 (4.3) | 0.43 |
| Others | 2/149 (1.3) | 0 (0) | 2/94 (2.1) | 0.90 |
| Length of stay—days, median (IQR: 25–75%) | ||||
| ICU | 7 (2; 16) | 6 (3; 14) | 9 (2; 18) | 0.149 |
| Hospital | 18 (9; 28) | 19 (14; 27) | 11 (2; 35) | 0.001 |
| Variables | Univariate analysis OR (95% CI) | Multivariable analysis OR (95% CI) | Variables | Univariate analysis OR (95% CI) | Multivariable analysis OR (95% CI) |
|---|---|---|---|---|---|
| Highest CRP | 1.007 (1.005–1.009) | 1.005 (1.002–1.007) | Highest NLr | 1.05 (1.03–1.07) | 1.03 (1.001–1.05) |
| Age | 1.04 (1.03–1.06) | 1.07 (1.05–1.09) | Age | 1.04 (1.03–1.06) | 1.07 (1.04–1.09) |
| WFNS 4–5 | 9.95 (6.71–14.75) | 4.51 (2.64–7.71) | WFNS score of 4–5 | 9.95 (6.71–14.75) | 5.58 (3.33–9.38) |
| Rebleeding | 6.87 (2.82–16.74) | 10.18 (2.92–35.54) | Rebleeding | 6.87 (2.82–16.74) | 9.30 (2.57–33.67) |
| DCI | 4.52 (2.96–6.88) | 5.54 (3.10–9.89) | DCI | 4.52 (2.96–6.88) | 5.40 (3.05–9.57) |
| ICHT | 12.55 (8.27–19.04) | 6.69 (3.90–11.49) | ICHT | 12.55 (8.27–19.04) | 7.29 (4.27–12.43) |
| Nimodipine | 0.15 (0.08–0.28) | 0.10 (0.04–0.22) | Nimodipine | 0.15 (0.08–0.28) | 0.12 (0.05–0.28) |
| Variables | Multivariable analysis OR (CI 95%) |
|---|---|
| Highest CRP | 1.005 (1.002–1.007) |
| Highest NLr | 1.02 (0.99–1.04) |
| Age | 1.07 (1.05–1.09) |
| WFNS score of 4–5 | 4.50 (2.64–7.70) |
| Rebleeding | 10.24 (2.93–35.81) |
| DCI | 5.38 (3.01–9.63) |
| Intracranial hypertension | 6.73 (3.92–11.54) |
| Nimodipine | 0.09 (0.40–0.21) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Intracerebral and Subarachnoid Hemorrhage Research · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
1
Spontaneous subarachnoid hemorrhage (SAH) is a devastating condition that accounts for 5% of all strokes and affects 7.9 per 100,000 person-years (1, 2). Immediately after blood is released into the subarachnoid space, ventricles, and parenchyma, there is a significant rise in intracranial pressure (ICP), acute vasoconstriction, and microthrombosis, leading to a reduction in cerebral blood flow (CBF) and promoting cerebral edema (3). Ischemia combined with reactive oxygen species and toxic hemoglobin breakdown products activates the inflammatory cascade, causing neuroinflammation and blood–brain barrier dysfunction, which further aggravates cerebral edema (4, 5).
Neuroinflammatory cascades are primarily mediated by resident microglial cells and infiltrating leukocytes (6). Leukocytic infiltration from the peripheral blood is one of the first inflammatory events, as these cells stimulate the microglia and activate innate responses by secreting pro-inflammatory cytokines (7). Central cytokine expression by glial cells further promotes the recruitment of neutrophils, monocytes, macrophages, and other immune cells (8). Moreover, degraded blood products stimulate toll-like receptors (TLR-4) (9), enhancing inflammatory cytokine production and perpetuating intrinsic inflammatory pathways (7).
Interestingly, SAH is also associated with intense systemic inflammation, involving complex interactions between the coagulation cascade (10), sympathetic activation (11), and endothelial dysfunction (12). Patients often exhibit clinical signs of systemic inflammatory response syndrome (SIRS), such as fever, tachypnea, tachycardia, and leukocytosis (13), as well as organ dysfunction (14). The presence of SIRS in SAH patients has been associated with secondary brain injury, delayed cerebral ischemia (DCI), and worse outcomes (15, 16). Additionally, SAH patients also experience a decrease in lymphocytes (17), particularly T-cell regulators, contributing to a state of induced immunodepression (18).
In this context, serum biomarkers of inflammation may be useful for assessing the presence of a systemic inflammatory response, potentially identifying patients at high risk of DCI and unfavorable neurological outcomes after SAH. The neutrophil-to-lymphocyte ratio (NLr) is a readily available biomarker that reflects inflammatory disturbances by demonstrating a combination of significant neutrophilia with relative lymphopenia. Indeed, an elevated NLr appears to be associated with DCI and poor outcomes after SAH (19). Of note, the majority of studies have focused on one-time measurement of the NLr, usually on admission (20, 21). C-reactive protein (CRP) is a well-known acute-phase inflammatory protein involved in the classical complement pathway of innate immunity (22). In SAH, some studies have reported an association between elevated CRP and unfavorable neurological outcomes (23–30), whereas others have not (31–33). Conflicting results have also been reported regarding the association between elevated CRP and the development of DCI (31–35).
Therefore, we aimed to assess the association of CRP and NLr during the first 7 days after SAH with the occurrence of unfavorable neurological outcomes and the development of DCI.
Methods
2
Study design and population
2.1
This is a retrospective, single-center cohort study of consecutive aneurysmal SAH (aSAH) patients admitted to the Intensive Care Unit (ICU) of the “Hôpital Universitaire de Bruxelles” (HUB) in Brussels, Belgium, between January 2007 and August 2023. We included all consecutive adult (>18 years old) patients with a diagnosis of ruptured aneurysm as the primary cause of SAH, confirmed by neuroimaging [CT angiography (CTA) and/or digital subtraction angiography (DSA)]. We excluded patients who stayed less than 24 h in the ICU, patients without admission values for CRP and blood cell counts, and patients with pre-existing immunosuppression (e.g., human immunodeficiency virus (HIV), chronic steroid use, or chronic immunosuppressant use). This study was approved on 5 July 2024 by the Ethics Committee of Erasme Hospital (P2024/289), which waived the need for informed consent. All methods were carried out in accordance with the guidelines and regulations of the Declaration of Helsinki. This study was performed according to the STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) guidelines (36).
Data collection
2.2
Demographic and clinical data, including age, sex, and comorbidities, were recorded. Neurological status on admission was assessed using the World Federation of Neurological Surgeons score (WFNS) (37) and Glasgow Coma Scale (GCS) (38). The severity of bleeding was assessed using the modified Fisher scale (mFisher) (39). The Acute Physiology and Chronic Health Evaluation II (APACHE II) (40) score and the Sequential Organ Failure Assessment (SOFA) (41) score were calculated on admission. Aneurysm location and treatment (e.g., coiling and/or clipping) were also collected. We recorded neurological complications, such as rebleeding, intracranial hypertension, angiographic vasospasm, DCI, hydrocephalus, and seizures, as well as their management (i.e., osmotic therapy, decompressive craniectomy, and intra-arterial vasodilators), as previously reported (42). Vasospasm was defined by a neuroradiologist as moderate-to-severe arterial narrowing (>50%) on specific imaging (DSA or CTA) not attributable to atherosclerosis, catheter-induced spasm, or vessel hypoplasia (43). Cerebral vasospasm could also be defined using transcranial Doppler assessment as mean flow velocity in any vessel >200 cm/s or >120 cm/s with a Lindegaard ratio above 3 (44). DCI (45) was defined as the occurrence of focal neurological impairment or a decrease of at least 2 points on the GCS that lasted for at least 1 h, was not apparent immediately after aneurysm occlusion, and could not be attributed to other causes. Additionally, the presence of a new cerebral infarction on a CT or magnetic resonance (MR) scan of the brain within 6 weeks after SAH or proven at autopsy, not attributable to other causes, and not present on the admission CT scan or immediately after aneurysm occlusion was also considered DCI (45). Rebleeding was defined as sudden clinical deterioration with signs of a new or increased hemorrhage on a CT scan compared with prior CT imaging (46). Hydrocephalus was defined as a bicaudate index above the 95th percentile for age, assessed by an experienced neuroradiologist (47).
The use of oral nimodipine, sedation, vasopressors, inotropic agents, and continuous renal replacement therapy (CRRT) was also recorded. We also documented the development of infection within the first 7 days after admission, using definitions from the Centers for Disease Control and Prevention/National Healthcare Safety Network (CDC/NHSN) (48).
Serum CRP values and neutrophil and lymphocyte counts were collected at admission and then daily for the following 7 days. A CRP level of >10 mg/L was considered “elevated,” according to local laboratory thresholds. No specific cutoff has been established for NLr.
Neurological status was assessed using the Glasgow Outcome Scale (GOS) (49) at 3 months. In our institution, GOS is routinely recorded in the medical chart at 3 months by neurologists or neurosurgeons during the follow-up clinic. A GOS score of 1–3 (death, persistent vegetative state, and severe disability) was considered an unfavorable outcome (UO), while a GOS score of 4 (moderate disability) or 5 (good recovery) was considered a favorable outcome (FO).
Endpoints
2.3
The primary endpoint of the study was the association of CRP and NLr with the occurrence of UOs. The secondary endpoints included: (a) the association of CRP and NLr with infections occurring within the first 7 days post-ictus and (b) the association of CRP and NLr with the occurrence of DCI.
Statistical analysis
2.4
Continuous data were expressed as mean [standard deviation (SD)] or median [interquartile range (IQR)] according to data distribution. Differences between groups were assessed using Student’s t-test or the Mann–Whitney U-test for normally or non-normally distributed data for independent samples. For related samples, we used the Friedman test to compare continuous variables, including CRP and NLr. Categorical data were presented as numbers [percentage, (%)], and comparisons between groups were performed using the chi-squared test. We performed univariate and multivariable logistic regression analyses to assess the association between the highest NLr/CRP and UOs, adjusting for pre-specified covariates identified using the “historical method” (50), such as commonly described variables associated with UOs in the literature (e.g., age, DCI, a WFNS score of 4–5, intracranial hypertension, rebleeding, and nimodipine prophylaxis) (1). The independence of errors, the presence of multicollinearity, and the presence of influential outliers were assessed, and none were violated. The results of the multivariate logistic regression models were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). We also performed a competing risk analysis to assess the association between the highest NLr, the highest CRP, and DCI, adjusted for mFisher, the presence of angiographic cerebral vasospasm, a WFNS score of 4–5 (51), age, sex, and history of systemic hypertension. Death was considered a competing factor. The results of the competing risk analysis were presented as subhazard ratios (sHRs) with 95% CIs. We performed a multilevel mixed model with random intercepts at the patient and time level (measured in days) to evaluate the association between repeated measures of NLr/CRP and UOs, as well as the occurrence of any infection within the first 7 days post-bleeding. Only CRP/NLr values that preceded the onset of infection were included in their respective analyses. We performed a sensitivity analysis to account for the interaction between NLr/CRP and infection. A logistic regression analysis was used to assess the impact of CRP and NLr on UOs, adjusting for age, DCI, a WFNS score of 4–5, intracranial hypertension, rebleeding, and nimodipine prophylaxis in patients with and without infection. The independence of errors, the presence of multicollinearity, and the presence of influential outliers were checked, and none were violated. A multilevel mixed model with random intercepts at the patient and time levels (in days) was performed to assess the association of repeated measures of CRP and NLr over time and UOs in patients with and without infection. Statistical significance was considered at a p-value of <0.05. No imputation for missing values was performed, as the number of missing NLr and CRP values was less than 10%, and all patients had at least 3 values of NLr and CRP. All analyses were performed using IBM SPSS Statistics version 29 and GraphPad Prism 10.
Results
3
Study population
3.1
A total of 567 consecutive aSAH patients were admitted during the study period; 20 (3.5%) patients were excluded (n = 5, ICU stay less than 24 h; n = 15, lack of blood count and CRP levels on admission), resulting in 547 (96.5%) patients included in the final analysis. The characteristics of the study population are shown in Table 1. Patients were predominantly female (61.8%) with a median age of 54 years (IQR: 45–63). The median GCS score on admission was 13 (4–15); 249 (45.5%) patients presented with a WFNS grade of 4–5 (poor grade), and 90.3% of patients had an mFisher score of 3–4. The majority of patients underwent aneurysm endovascular coiling (n = 480, 87.8%). In the first 7 days following SAH, 149 (27.2%) patients experienced an infection (mostly pneumonia in 80/149, 53.7%). DCI occurred in 140 (25.6%) patients, and UOs were observed in 250 patients (54.3%).
C-reactive protein and neutrophil-to-lymphocyte ratio values
3.2
The median CRP and NLr on admission were 3.6 mg/L (IQR: 1.6–9.6) and 6.67 (IQR: 3.40–12.21), respectively (Supplementary Table S1). There was an increase over time in the daily median CRP levels (Figure 1A, p = 0.001), while NLr remained elevated but stable over time (Figure 1B, p = 0.57).
(A) C-reactive protein (CRP) levels from admission to the seventh day post-ictus in the study population. Data are presented as a median and interquartile range of 25–75%. The p-value was calculated using the Friedman test. (B) Neutrophil-to-lymphocyte ratio (N/L) levels from admission to the seventh day post-ictus in the study population. Data are presented as a median and interquartile range of 25–75. The p-value was calculated using the Friedman test.
Neurological outcome
3.3
Patients who had UOs were older and had a lower GCS on admission than patients with FOs. Patients with UOs also had a higher rate of neurological complications and infection than those with FOs (Table 1). The highest CRP value was significantly higher in the UO group [130.0 (56.3–220.0) mg/L vs. 45.0 (20.0–100.0) mg/L; p = 0.001]; although CRP progressively increased over time in both groups, CRP values were consistently higher from days 2 to 7 in patients with UOs than in patients with FOs (Supplementary Table S1 and Figure 2). In a multivariable logistic regression model, the highest CRP value (OR: 1.005; 95% CI: 1.0002–1.007) was independently associated with UOs when adjusted for confounders (Table 2).
C-reactive protein (CRP) levels from admission to the seventh day post-ictus in the study population according to the neurological outcome at 3 months. Unfavorable outcomes (UOs) were defined as a Glasgow Outcome Scale score of 1–3 (death, vegetative state, and severe disability). Data are presented as a median and interquartile range of 25–75%. The p-value corresponds to the statistical significance of the interaction time and group in a mixed model.
Similarly, the highest NLr value was significantly higher in the UO group [12.50 (8.28–17.65) vs. 9.01 (IQR: 5.38–13.69); p = 0.001]. Moreover, NLr values remained stable over time among patients with UOs, while they decreased in patients with FOs (Supplementary Table S1 and Figure 3). In a multivariable logistic regression model, the highest NLr value (OR: 1.025; 95% CI: 1.001–1.050) was independently associated with UOs when adjusted for confounders (Table 2).
Neutrophil-to-lymphocyte ratio (N/L) levels from admission to the seventh day post-ictus in the study population according to the neurological outcome at 3 months. Unfavorable outcomes (UOs) were defined as a Glasgow Outcome Scale score of 1–3 (death, vegetative state, and severe disability). Data are presented as a median and interquartile range of 25–75%. The p-value corresponds to the statistical significance of the interaction time and group in a mixed model.
When including both the highest CRP and the highest NLr in the same model, only CRP (OR: 1.005; 95% CI: 1.002–1.007) remained independently associated with unfavorable outcomes at 3 months (Table 3).
Infections
3.4
A total of 149 patients (27.2%) acquired infection during their ICU stay. The most common site of infection was pneumonia (80/149, 53.7%), followed by urinary tract infection (42/149, 28.2%) and bloodstream infection (20/149, 13.4%). Time from admission to infection was 5 days (IQR: 3–7). Patients with infections more frequently had a poor clinical grade on admission, had a higher prevalence of neurological complications, such as DCI, and had a higher frequency of UOs than patients without infection (Supplementary Table S2). Patients who developed infection had higher CRP (p = 0.001, Figure 4A) and NLr (p = 0.001, Figure 4B) values than those without infection.
Evolution of (A) C-reactive protein (CRP) levels and (B) neutrophil-to-lymphocyte ratio (NLR) over time according to the development of infection in the first 7 days post-ictus. The p-value represents the statistical significance of the interaction between infection and CRP levels and between infection and NLR. CRP values are expressed in mg/L.
Considering only patients with infection, CRP was consistently higher from days 3 to 7 in patients with UOs compared with those with FOs (Figure 5A). However, in these patients, the highest CRP (OR: 1.01, 95% CI: 1.00–1.01) was not independently associated with UOs (Supplementary Table S3) when adjusted for confounders. Additionally, NLr remained statistically similar over time in patients with UOs and those with FOs (Figure 5B); in an adjusted logistic regression model, NLr (OR: 1.02; 95% CI: 0.99–1.06) was not independently associated with UOs (Supplementary Table S3).
Evolution of (A) C-reactive protein (CRP) levels and (B) neutrophil-to-lymphocyte ratio (NLR) over time according to the neurological outcome at 3 months in patients who developed infection in the first 7 days post-ictus. CRP values are expressed in mg/L.
In patients without infection (Figures 6A,B), the highest CRP values (OR: 1.006; 95% CI: 1.001–1.010), but not the highest NLr values (OR: 1.02; 95% CI: 0.99–1.05), were significantly associated with UOs when adjusted for confounders (Supplementary Table S4).
Evolution of (A) C-reactive protein (CRP) levels and (B) neutrophil-to-lymphocyte ratio (NLR) over time according to the neurological outcome at 3 months in patients without infection in the first 7 days post-ictus. CRP values are expressed in mg/L.
Delayed cerebral ischemia
3.5
Patients who developed DCI had higher clinical and neurological severity on admission and a higher prevalence of hydrocephalus, intracranial hypertension, angiographic vasospasm, and infection than others (Supplementary Table S5). Supplementary Figure S1 shows that CRP (panel A, p = 0.001) and NLr (panel B, p = 0.001) daily values were higher in the first 7 days of ICU stay in patients with DCI than those without DCI.
The highest NLr (sHR: 1.02; 95% CI: 1.01–1.03) in the first 7 days, but not CRP (sHR: 1.00; 95% CI: 1.00–1.01), was independently associated with the development of DCI (Supplementary Table S6) in a competing risk analysis adjusted for age, sex, history of systemic hypertension, an mFisher score of 3–4, a WFNS score of 4–5, and angiographic vasospasm, with the competing event defined as ICU death. This association remained significant in a competing risk analysis considering only patients with an infection (highest NLr/sHR: 1.03; 95% CI: 1.01–1.05) but not in patients without infection (highest NLr/sHR: 1.01; 95% CI: 0.98–1.03), as shown in Supplementary Tables S7, S8.
Patients with infection who had developed DCI had higher CRP (p = 0.008) and NLr (p = 0.001) levels over time than those who had infection but did not have DCI (Supplementary Figure S2). Conversely, patients without infection who had developed DCI had comparable daily levels of CRP and NLr over time (Supplementary Figure S3) to patients without infection who did not develop DCI.
Discussion
4
In this retrospective single-center study on aSAH patients, elevated biomarkers of systemic inflammation, such as CRP and NLr, over the first week after bleeding were associated with a higher chance of unfavorable neurological outcomes at 3 months. Moreover, the highest NLr level was also associated with the development of DCI.
A systematic review and meta-analysis that analyzed 12 studies (20, 52–62), with a total of 4,840 SAH patients, revealed an independent association (OR: 1.31; 95% CI: 1.14–1.49) between admission NLr and poor neurological outcomes at 3 months (21). Of note, only 5 studies (52, 55, 57, 58, 62, and) of the 12 studies reported this association. In our study, we showed that the highest NLr in the first 7 days was associated with outcomes. Interestingly, this association was not significant in the univariate analysis, but only after considering the impact of clinical grade on admission assessed by the WFNS score, did we see this significant association between NLr and neurological outcomes. As previously described, patients with poor clinical grade can mount a more robust inflammatory response than patients with good grade after the initial hemorrhage (13).
Additionally, patients with favorable and unfavorable neurological outcomes had similar NLr in the first 24 h; however, from days 2 to 7, NLr remained elevated in patients with UOs, while in patients with FOs, NLr tended to decrease. This suggests that a “dose-effect” association with outcome, in which not only the peak of NLr is important, but also the time spent with elevated NLr.
Delayed cerebral ischemia has a complex pathophysiology, which includes neuroinflammation. In fact, leukocytosis and lymphopenia, represented by NLr, can promote microcirculatory dysfunction and contribute to microthrombi formation and cortical ischemia, all of which are processes involved in the development of DCI (63). Interestingly, the association between NLr and DCI may also reflect the role of neutrophil extracellular traps (NETs) in the pathology of DCI (64). NETs are a downstream neutrophil-mediated immune mechanism that can cause vascular endothelial injury and thrombosis (65). Previous studies have consistently identified NET biomarkers in the serum of aneurysmal subarachnoid hemorrhage patients (66, 67) and have shown an association between these biomarkers and delayed cerebral ischemia (68). In this setting, an association between NLr in the first 24 h after bleeding and the development of DCI has been consistently reported (20, 56, 58, 62, 69, 70) and was further confirmed in our study. This highlights the interplay between neuroinflammation and systemic inflammation.
Different from previous studies (15, 71–73), we did not observe an association between the highest CRP in the first 7 days after SAH and delayed cerebral ischemia. Conversely, we showed that elevated CRP was also associated with poor outcomes after SAH. Similarly, Lee et al. (74) also reported an association between the highest CRP in the first 7 days post-bleeding and poor neurological outcomes, while other studies showed an association between an early increase in CRP during early brain injury and poor outcomes, often independently of the development of DCI (16, 23, 28, 29, 31, 75–77).
Interestingly, when included in the same model, only CRP remained independently associated with poor outcomes, while NLr did not. Other studies (24, 78) have focused on the ratio between CRP and lymphocytes (CRL) and demonstrated an association between higher levels of CRL, DCI, and poor outcomes, possibly representing both increased inflammatory response (high CRP) and stroke-related immunodepression (low lymphocyte count) (79).
Importantly, NLr is easily obtained by performing a blood cell count, without any additional costs and with minimal risk of harm to patients. Similarly, CRP measurements are cheap, readily available, consistent, and reproducible in the majority of countries (74). Despite the low-quality level of evidence, as all studies are observational and conducted mostly in a single center, NLr and CRP may be useful as additional biomarkers for the identification of patients at risk of DCI and to help with neuro-prognostication in both low-and middle- and high-income countries (77).
Of note, infections, especially pneumonia, are a common medical complication (80) that significantly impacts the outcome of aSAH patients (81). In clinical practice, CRP and neutrophil count are biomarkers used to aid the diagnosis of infection and to monitor response to treatment (82). In our study, 27% of patients acquired an infection in the first week of hospitalization. In fact, infection is an important confounder when interpreting our results. In patients who acquired an infection, elevated levels of CRP and NLr are likely due to an inflammatory response to fight the infection rather than a systemic inflammatory response to the primary subarachnoid bleed. Additionally, the association between CRP/NLr and the outcome in infected patients may indirectly reflect the impact of infectious complications on the outcome, as previously described (83).
Our study has some limitations. As a retrospective study, data collection may be subject to biases related to clinical recording and is limited by missing data, and we cannot exclude the presence of unaccounted confounders that may have influenced our results. As a single-center study, our results may be applicable only to cohorts with characteristics similar to ours, and local practices may have impacted our results. Moreover, due to a lack of available data regarding long-term neurological assessment, we limited our investigation to short-term outcomes. Additionally, we chose to exclude patients with imminent death due to catastrophic injuries by excluding those who stayed less than 24 h in the ICU. However, by doing so, we failed to study the impact of inflammatory biomarkers on the mechanism of early death. We were also unable to assess the presence of inflammatory biomarkers in the central nervous system. In our center, no standardized guidelines on the collection of CRP exist, although blood cell counts are usually performed daily in the acute phase; the decision of whether, when, and how to monitor these biomarkers was made by the healthcare team, which may have impacted our results. An ideal biomarker would be monitored continuously and in real time. This, unfortunately, is not available for these biomarkers in a retrospective setting. Additionally, despite adjustments in the multivariable analysis for the most commonly described factors associated with the outcome of SAH patients, confounders not accounted for may have impacted our results. Propensity score matching may be a valid method to better address this bias, and future studies should consider it.
Conclusion
5
In this SAH cohort, commonly used biomarkers of systemic inflammation, such as C-reactive protein and neutrophil-to-lymphocyte ratio, were frequently elevated in the early phase after the initial bleed and were associated with the development of DCI and an increased risk of unfavorable outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Claassen J Park S. Spontaneous subarachnoid haemorrhage. Lancet. (2022) 400:846–62. doi: 10.1016/S 0140-6736(22)00938-2, 35985353 PMC 9987649 · doi ↗ · pubmed ↗
- 2Etminan N Chang HS Hackenberg K de Rooij NK Vergouwen MDI Rinkel GJE . Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: a systematic review and meta-analysis. JAMA Neurol. (2019) 76:588–97. doi: 10.1001/jamaneurol.2019.0006, 30659573 PMC 6515606 · doi ↗ · pubmed ↗
- 3Lauzier DC Jayaraman K Yuan JY Diwan D Vellimana AK Osbun JW . Early brain injury after subarachnoid hemorrhage: incidence and mechanisms. Stroke. (2023) 54:1426–40. doi: 10.1161/STROKEAHA.122.040072, 36866673 PMC 10243167 · doi ↗ · pubmed ↗
- 4Fujii M Yan J Rolland WB Soejima Y Caner B Zhang JH. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl Stroke Res. (2013) 4:432–46. doi: 10.1007/s 12975-013-0257-2, 23894255 PMC 3719879 · doi ↗ · pubmed ↗
- 5Pan P Xu L Zhang H Liu Y Lu X Chen G . A review of hematoma components clearance mechanism after subarachnoid hemorrhage. Front Neurosci. (2020) 14:685. doi: 10.3389/fnins.2020.00685, 32733194 PMC 7358443 · doi ↗ · pubmed ↗
- 6Rivest S. Regulation of innate immune responses in the brain. Nat Rev Immunol. (2009) 9:429–39. doi: 10.1038/nri 2565, 19461673 · doi ↗ · pubmed ↗
- 7de Oliveira Manoel AL Macdonald RL. Neuroinflammation as a target for intervention in subarachnoid hemorrhage. Front Neurol. (2018) 9:292. doi: 10.3389/fneur.2018.00292, 29770118 PMC 5941982 · doi ↗ · pubmed ↗
- 8Lucke-Wold BP Lucke-Wold B Logsdon A Manoranjan B Turner R Mc Connell E . Aneurysmal subarachnoid hemorrhage and neuroinflammation: a comprehensive review. Int J Mol Sci. (2016) 17:497. doi: 10.3390/ijms 17040497, 27049383 PMC 4848953 · doi ↗ · pubmed ↗