Humoral Hypercalcemia of Malignancy Caused by Parathyroid Hormone-Related Protein-Secreting Medullary Thyroid Carcinoma: A Case Report
Takuya Hirose, Hirotaka Nakayama, Osamu Matsubara, Satoru Uchida, Kazuyuki Tani, Nobuyasu Suganuma, Aya Saito

TL;DR
A rare case of medullary thyroid carcinoma caused severe hypercalcemia through the production of parathyroid hormone-related protein, highlighting the importance of PTHrP testing in similar cases.
Contribution
This paper presents a rare case of hypercalcemia in medullary thyroid carcinoma caused by PTHrP secretion.
Findings
The patient had severe hypercalcemia due to PTHrP production by medullary thyroid carcinoma.
Postoperative PTHrP levels normalized, and the patient showed no recurrence at 8 months.
PTHrP measurement is recommended for diagnosing hypercalcemia in thyroid cancer patients.
Abstract
Medullary thyroid carcinoma (MTC) is a rare neuroendocrine tumor arising from the parafollicular C cells, accounting for approximately 1.5% of all thyroid cancers. Although calcitonin secreted by the MTC typically lowers calcium levels, serum calcium concentrations usually remain within the normal range due to compensatory parathyroid hormone (PTH) secretion. Hypercalcemia of malignancy is broadly categorized as humoral hypercalcemia of malignancy (HHM), mediated by parathyroid hormone-related protein (PTHrP), or local osteolytic hypercalcemia. We report a rare case of HHM caused by a PTHrP-secreting MTC. A 60-year-old woman visited our hospital with weight loss, fatigue, and a large right-sided neck mass. Laboratory tests revealed marked hypercalcemia (16.5 mg/dL), hypophosphatemia, and renal dysfunction. The intact PTH level was within the normal range, whereas the PTHrP level was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
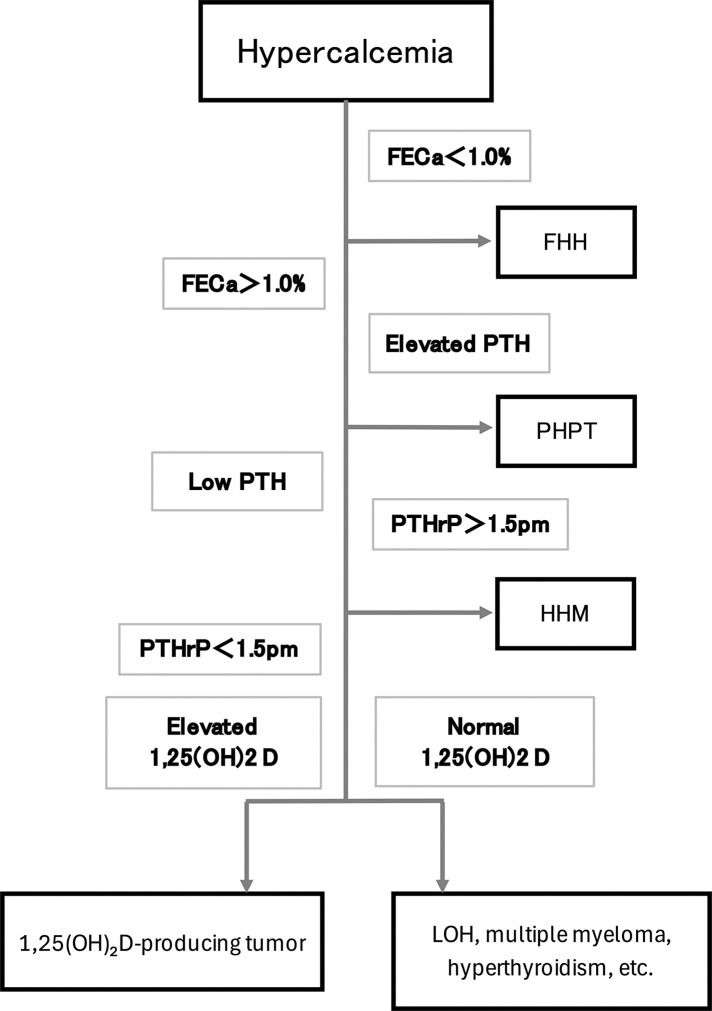 Fig. 1
Fig. 1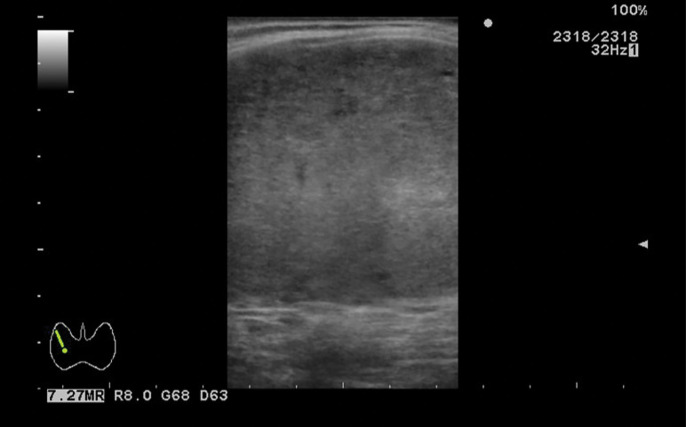 Fig. 2
Fig. 2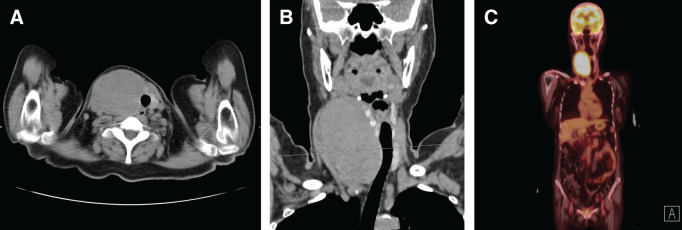 Fig. 3
Fig. 3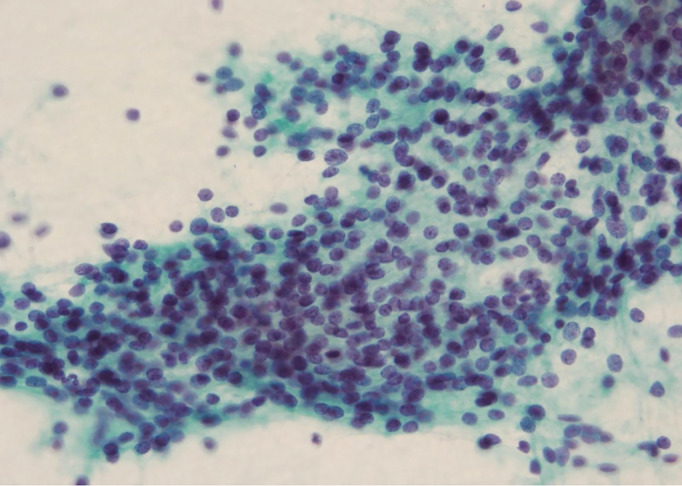 Fig. 4
Fig. 4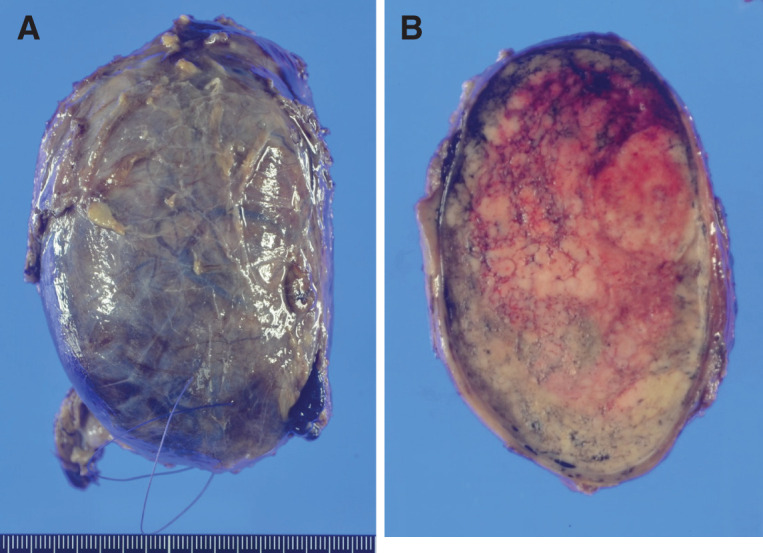 Fig. 5
Fig. 5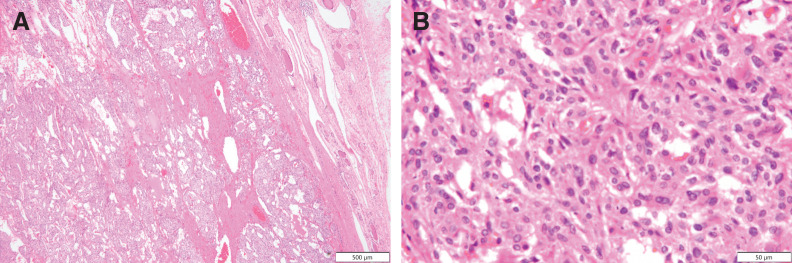 Fig. 6
Fig. 6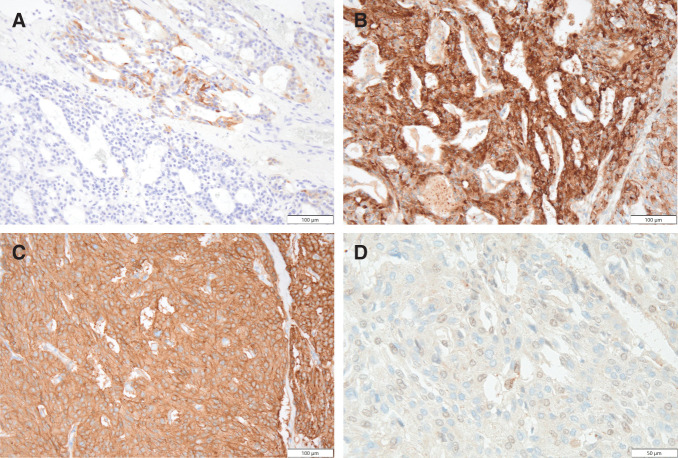 Fig. 7
Fig. 7| Hematology | Hormone | ||
|---|---|---|---|
| WBC | 10200/μL | TSH | 0.232 μIU/mL |
| Neut | 77.5% | fT3 | 2.58 pg/mL |
| Lymp | 15.5% | fT4 | 1.33 ng/dL |
| Mono | 6.5% | I-PTH | 12 pg/mL |
| RBC | 439 104/μL | PTHrP | 5.7 pmol/L |
| Hb | 12.8 g/dL | ACTH | 19.1 pg/mL |
| Plt | 33.4 104/μL | CORT | 17.1 μg/dL |
| Metanephrine | 62 pg/mL | ||
| Biochemistry | Normetanephrine | 132 pg/mL | |
| ALB | 4.7 g/dL | ||
| AST | 25 U/L | Tumor marker | |
| ALT | 24 U/L | CEA | 12243 ng/mL |
| ALP | 106 U/L | Calcitonin | 160 pg/mL |
| BUN | 25 mg/dL | CA19-9 | 19.4 U/mL |
| Cre | 2.19 mg/dL | CA125 | 14.7 U/mL |
| Na | 142 mEq/L | CA15-3 | 7.7 U/mL |
| K | 4 mEq/L | NSE | 4.2 ng/mL |
| Cl | 106 mEq/L | ||
| Ca | 16.5 mg/dL | Serology | |
| IP | 2.3 mg/dL | CRP | 0.59 mg/dL |
| 1,25(OH)2 D | 24.4 pg/mL | sIL-2R | 375 U/mL |
| FECa | 10.7% | ||
| Age | Sex | PTHrP | Intact-PTHrP | Ca(mg/dL) | Histology | |
|---|---|---|---|---|---|---|
| Kitamura | 48 | M | 11.1 pmol/L | 15.2 | ATC | |
| Yazawa | 67 | F | 4.02 pmol/L | 13.8 | ATC | |
| Kunisue | 63 | F | 39 pmol/L | 14 | ATC | |
| Iwai | 84 | F | 3.2 pmol/L | 10.9 | ATC | |
| Ito | 60 | F | 138 pg/mL | 11.2 | PTC | |
| Ito | 58 | F | 284 pg/mL | 11.4 | PTC | |
| Okutur | 50 | M | 8.5 pmol/L | 13.8 | MTC | |
| Ackah | 8 | F | 301 pmol/L | 18.8 | MTC | |
| Our Case | 60 | F | 5.7 pmol/L | 16.5 | MTC |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Bone health and treatments · Thyroid Cancer Diagnosis and Treatment
Abbreviations
ATC anaplastic thyroid carcinoma CA carbohydrate antigen CEA carcinoembryonic antigen FDG-PET/CT 18F-fluorodeoxyglucose PET/CT FECa fractional excretion of calcium FHH familial hypocalciuric hypercalcemia HHM humoral hypercalcemia of malignancy IL interleukin LOH local osteolytic hypercalcemia MEN2A multiple endocrine neoplasia 2A MTC medullary thyroid carcinoma PHPT primary hyperparathyroidism PTC papillary thyroid carcinoma PTH parathyroid hormone PTHrP parathyroid hormone-related protein RET rearranged during transfection
INTRODUCTION
MTC is a rare malignancy originating from parafollicular cells, accounting for approximately 1.5% of all thyroid cancers.^1)^ Although serum calcitonin levels are elevated in MTC and exert a hypocalcemic effect, serum calcium levels typically remain within the normal range due to the compensatory PTH secretion.^2,3)^
However, in rare cases, tumor-derived factors can cause hypercalcemia, broadly categorized as HHM and LOH. HHM results from the systemic effects of PTHrP secreted by tumor cells, while LOH is caused by bone resorption mediated by cytokines produced locally by tumor cells within bone lesions.^4,5)^
Here, we report a rare case of HHM caused by sporadic MTC associated with elevated PTHrP production.
CASE PRESENTATION
A 60-year-old woman was referred to our hospital for evaluation of progressive weight loss, fatigue, and a right cervical mass. The mass had been noted 10 years prior but remained uninvestigated. Her medical history included the presence of ovarian cysts and retinitis pigmentosa. She was not taking any medication and had no known allergies or relevant family history. She was a lifelong nonsmoker and abstained from alcohol consumption.
Upon initial examination, her height and weight were 164.1 cm and 49.9 kg, respectively. Her blood pressure was 200/100 mmHg, and her heart rate was 103 beats/min with a regular rhythm. Physical examination revealed a soft, mobile, and elastic mass, approximately 10 cm in diameter, in the right thyroid lobe.
Laboratory data revealed marked hypercalcemia (16.5 mg/dL; normal range 8.8–10.4 mg/dL), hypophosphatemia (2.3 mg/dL; normal, 2.5–4.5 mg/dL), and renal dysfunction (creatinine 2.19 mg/dL; normal, 0.47–0.79 mg/dL). Further evaluation following a diagnostic algorithm (Fig. 1) demonstrated elevated fractional excretion of calcium (FECa 10.7%; normal, 2%–4%), normal intact PTH (12 pg/mL; normal, 10–65 pg/mL), and elevated PTHrP (5.7 pmol/L; normal, ≤1.3 pmol/L), findings suggestive of HHM (Table 1). Tumor markers revealed elevated CEA (12243 ng/mL; normal, <5.0 ng/mL) and calcitonin (160 pg/mL; normal, ≤6.4 pg/mL), while thyroglobulin, CA19-9, CA125, CA15-3, and neuron-specific enolase levels were normal.
Diagnostic algorithm of hypercalcemia.FECa, fractional excretion of calcium; FHH, familial hypocalciuric hypercalcemia; HHM, humoral hypercalcemia of malignancy; LOH, local osteolytic hypercalcemia; PTH, parathyroid hormone; PTHrP, parathyroid hormone-related protein
Ultrasonography revealed a well-circumscribed, homogeneously hypoechoic mass measuring 100 mm in the right thyroid lobe (Fig. 2). FDG-PET/CT demonstrated increased uptake in a 93-mm mass within the right thyroid lobe, with no evidence of lymph node involvement or distant metastasis (Fig. 3). Upper and lower gastrointestinal endoscopies revealed no malignancy.
Ultrasonography. Ultrasonography revealed a hypoechoic mass measuring 100 mm in the right thyroid lobe.
FDG-PET/CT. (A) CT revealed a 93-mm mass within the right thyroid lobe. (B) The mass did not invade the trachea. FDG-PET/CT revealed increased uptake in the mass. (C) No evidence of lymph node involvement or distant metastasis was observed.FDG-PET/CT, 18F-fluorodeoxyglucose PET/CT
Fine-needle aspiration cytology of the thyroid mass revealed small round cells with scant stroma and no distinctive architectural pattern consistent with MTC (Fig. 4).
Fine-needle aspiration cytology. Fine-needle aspiration cytology of the thyroid mass revealed small round cells with scant stroma.
Plasma metanephrine and normetanephrine levels assessed for MEN2A were within normal limits (62 and 132 pg/mL, respectively). Genetic testing for RET mutations yielded negative results, confirming the diagnosis of sporadic MTC associated with HHM.
The patient initially underwent correction of the hypercalcemia with intravenous hydration (2 L/day for 10 days), elcatonin (80 units/day for 9 days), and a single dose of zoledronic acid (4 mg). After biochemical improvement, a right thyroid lobectomy with unilateral central neck lymph node dissection was performed.
The operative time was 163 min, and the intraoperative blood loss was minimal (3 mL). No gross invasion into adjacent structures or lymph node metastasis was observed. The final surgical stage was sT3aN0.
The resected specimen was a solitary nodule of the right lobe of the thyroid, 11 x 7 x 7 cm in size, with a smooth surface (Fig. 5A). On section was a brown to yellow tumor mass appearance with hemorrhages (Fig. 5B). Microscopically, the tumor tissue consists of sheets and solid nests of round and polygonal cells with pale eosinophilic cytoplasm (Fig. 6A and 6B). The tumor did not contain prominent nucleoli, multinucleated tumor cells, or nuclear grooves or inclusions. Amyloid deposition or calcification was not seen. Immunohistochemically the tumor cells were partially positive for calcitonin (Fig. 7A) and positive for chromogranin A (Fig. 7B), synaptophysin, CD56, CEA (Fig. 7C), and TTF1. Based on these findings, a diagnosis of MTC was confirmed. In addition, the tumor cells were positive for PTHrP in the nuclei and cytoplasm (Fig. 7D).
The resected specimen. (A) The resected specimen was a solitary nodule of the right lobe of the thyroid, 11 x 7 x 7 cm in size, with a smooth surface. (B) On section was a brown to yellow tumor mass appearance with hemorrhages.
Hematoxylin and Eosin staining. The tumor tissue consists of (A) sheets and solid nests of (B) round and polygonal cells with pale eosinophilic cytoplasm.
The tumor cells were (A) partially positive for calcitonin, and (B) positive for chromogranin A, (C) synaptophysin, CD56, CEA, and TTF1. The tumor cells were (D) positive for PTHrP in the nuclei and cytoplasm.CEA, carcinoembryonic antigen; PTHrP, parathyroid hormone-related protein
Immunohistochemical staining for PTHrP was performed using a mouse monoclonal PTHLH/PTHrP antibody (catalog no. MAB6734; Bio-Techne/R&D Systems, Minneapolis, MN, US) at a dilution of 1:25.
Additionally, extrathyroidal extension or lymph node involvement was absent. The pathological stage was T3aN0M0 stage II according to the Union for International Cancer Control (UICC) classification, 8th edition.
Serum PTHrP levels decreased to <1.1 pmol/L POD 2. The patient recovered uneventfully and was discharged on POD 4. Postoperatively, CEA and calcitonin levels exhibited a sustained decline, eventually normalizing. Eight months post-surgery, the patient remained disease-free with no clinical or biochemical recurrence.
DISCUSSION
Several conditions can cause hypercalcemia, including PHPT, HHM, LOH, and FHH. Among malignancy-related cases, HHM and LOH represent the two major subtypes, with HHM accounting for approximately 80%.^4)^
In HHM, PTHrP secreted by tumor cells exerts systemic effects, promoting osteoclastic bone resorption and increasing renal tubular calcium reabsorption, ultimately leading to hypercalcemia. Endogenous PTH levels are typically suppressed by negative feedback in this setting. The diagnostic hallmarks of HHM include hypercalcemia, hypophosphatemia, elevated PTHrP levels, and suppressed PTH levels.
Conversely, LOH is caused by the local production of osteoclast-activating cytokines such as IL-1, IL-6, and tumor necrosis factor within metastatic bone lesions, leading to increased osteoclastic bone resorption and subsequent hypercalcemia.^6)^
In the present case, following the diagnostic algorithm illustrated in Fig. 1, low-normal intact PTH, elevated FECa, and increased PTHrP levels confirmed the diagnosis of HHM.
Representative tumors known to cause HHM include adult T-cell leukemic lymphoma, squamous cell carcinomas (of the lungs, head and neck, and skin), renal cell carcinoma, and breast cancer.^7)^ However, HHM associated with thyroid carcinoma is rare.
Kitamura et al. reported that among 127 patients who died of thyroid cancer, 8 (6.3%) developed hypercalcemia, with 6 of these (75%) attributed to HHM.^5)^ Among the HHM cases, five were ATC and one was PTC.
A literature search for “thyroid cancer” and “PTHrP” in PubMed, Ichushi (Japanese medical database), and Google Scholar identified eight previously reported cases of thyroid carcinoma with measured PTHrP levels. These eight cases, along with the present case, are summarized in Table 2.^5,8–13)^
A correlation between PTHrP and serum calcium levels has been reported in oral squamous cell carcinoma.^14)^ However, HHM associated with thyroid cancer is rare, and no definitive correlation has been established to date. Given the rarity of HHM associated with thyroid cancer, further case studies are warranted.
CONCLUSIONS
Here, we report a rare case of MTC presenting with hypercalcemia due to PTHrP production. Although HHM is uncommon in thyroid cancer, it can cause severe hypercalcemia, highlighting the need for prompt diagnosis and treatment. In cases of thyroid cancer-associated hypercalcemia, HHM should be considered, and PTHrP measurements may aid diagnosis. Due to scarce reports, further accumulation of clinical data is required to improve our understanding of this rare condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miyauchi A. Pathological findings and treatment for medullary thyroid carcinoma of MEN 2 (in Japanese ). J Fam Tumors 2007; 7: 71–4.
- 2Welbourn RB. Current status of the apudomas. Ann Surg 1977; 185: 1–12.12724 10.1097/00000658-197701000-00001 PMC 1396259 · doi ↗ · pubmed ↗
- 3Deftos LJ, Parthemore JG. Secretion of parathyroid hormone in patients with medullary thyroid carcinoma. J Clin Invest 1974; 54: 416–20.4847251 10.1172/JCI 107777 PMC 301569 · doi ↗ · pubmed ↗
- 4Motilal Nehru V, Garcia G, Ding J, et al. Humoral hypercalcemia in uterine cancers: a case report and literature review. Am J Case Rep 2017; 18: 22–5.28057913 10.12659/AJCR.900088 PMC 5234677 · doi ↗ · pubmed ↗
- 5Kitamura Y, Ishikawa N, Kohno M, et al. Clinical study of thyroid cancer with hypercalcemia (in Japanese with English abstract). Jpn J Pract Surg Soc 1993; 54: 1701–1705.
- 6Mirrakhimov AE. Hypercalcemia of malignancy: an update on pathogenesis and management. N Am J Med Sci 2015; 7: 483–93.26713296 10.4103/1947-2714.170600 PMC 4683803 · doi ↗ · pubmed ↗
- 7Takeda K, Kimura R, Nishigaki N, et al. Humoral hypercalcemia of malignancy with a parathyroid hormone-related peptide-secreting intrahepatic cholangiocarcinoma accompanied by a gastric cancer. Case Rep Endocrinol 2017; 2017: 7012520.28573053 10.1155/2017/7012520 PMC 5442343 · doi ↗ · pubmed ↗
- 8Yazawa S, Toshimori H, Nakatsuru K, et al. Thyroid anaplastic carcinoma producing granulocyte-colony-stimulating factor and parathyroid hormone-related protein. Intern Med 1995; 34: 584–8.7549149 10.2169/internalmedicine.34.584 · doi ↗ · pubmed ↗