Surgical Management of a Rare Ascending Aortic Mural Thrombus Using a Modified Brain Isolation Strategy: A Case Report
Rei Sueoka, Shogo Takahashi, JeongA Lee, Akito Inoue, Kentaro Shirakura, Yuki Setogawa, Daisuke Takeyoshi, Hiroyuki Kamiya, Shingo Kunioka

TL;DR
A rare case of ascending aortic mural thrombus was successfully treated with a modified brain isolation strategy during surgery.
Contribution
A novel surgical approach combining bilateral axillary cannulation and modified brain isolation was used to safely treat ascending aortic mural thrombus.
Findings
ECG-gated contrast-enhanced CT is essential for accurate diagnosis of ascending aortic mural thrombus.
A modified brain isolation strategy using unilateral selective cerebral perfusion minimized neurological risks during surgery.
Surgical excision and partial arch replacement successfully treated the thrombus without complications.
Abstract
Ascending aortic mural thrombus (AMT) is an exceptionally rare condition. Diagnosis is often difficult because non-ECG-gated contrast-enhanced CT is susceptible to motion artifacts, and the distal ascending aorta can sometimes be challenging to evaluate using transesophageal echocardiography. A standardized surgical strategy for ascending AMT has not been established. A 61-year-old man presented with transient left hemiplegia caused by embolic stroke. A non-ECG-gated contrast-enhanced CT scan revealed a thrombus-like structure in the ascending aorta; however, ECG-gated contrast-enhanced CT clearly demonstrated a thin-stalked and mobile thrombus, prompting urgent surgery. Cardiopulmonary bypass (CPB) was established using bilateral axillary artery cannulation and bicaval venous drainage. To minimize the risk of cerebral embolization during CPB initiation, the left common carotid artery…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
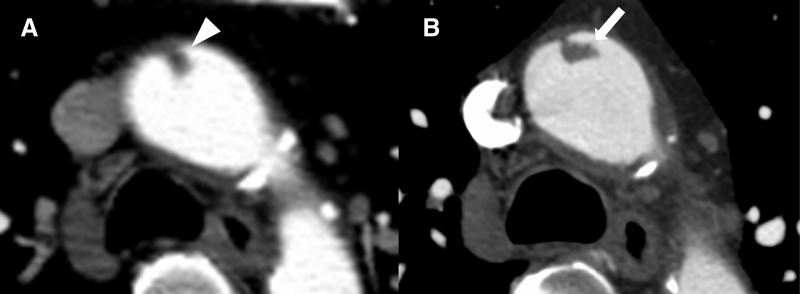 Fig. 1
Fig. 1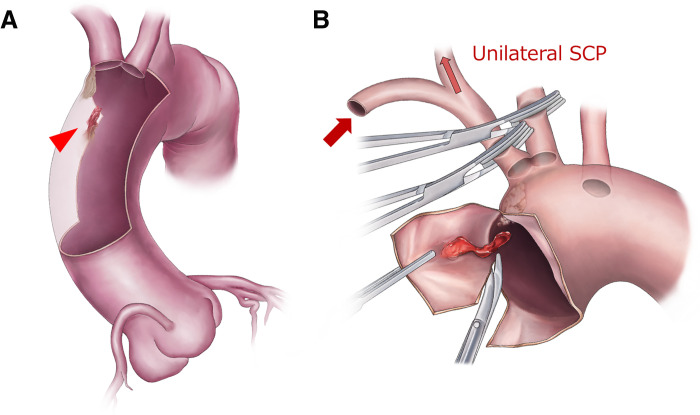 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Thrombus and Embolism · Cardiac tumors and thrombi · Aortic Disease and Treatment Approaches
Abbreviations
AMT aortic mural thrombus CPB cardiopulmonary bypass ECG electrocardiogram LCCA left common carotid artery NIRS near-infrared spectroscopy SCP selective cerebral perfusion TEE transesophageal echocardiography uSCP unilateral selective cerebral perfusion
INTRODUCTION
AMT is an uncommon clinical entity, with more than half of reported cases occurring in the abdominal aorta; only a few percentages arise in the ascending aorta, making ascending AMT exceptionally rare.^1)^ Published surgical cases are extremely scarce, and no standardized diagnostic or surgical strategy has been established for this condition.^2,3)^ Diagnostic evaluation is particularly challenging. Non-ECG-gated contrast-enhanced CT of the ascending aorta is susceptible to motion artifacts, which may obscure or mimic intraluminal lesions.^4)^ Although TEE is often considered in the evaluation of ascending aortic pathology, visualization of certain segments may occasionally be limited, making evaluation difficult in some cases.^5)^
Here, we report a rare case of ascending AMT identified after a transient ischemic neurological event. ECG-gated CT enabled precise characterization of a stalked thrombus, and semi-emergent surgery was safely performed using a brain isolation strategy with uSCP.
CASE PRESENTATION
A 61-year-old man with a history of hypertension presented with sudden left hemiplegia. Emergency MRI revealed an embolic stroke in the right middle cerebral artery. The patient had no documented history of atrial fibrillation or other embolic sources. Although there was a history of acute lower limb arterial occlusion more than 10 years earlier, no underlying thrombophilic disorder, including antiphospholipid antibody syndrome, had been identified. His neurological symptoms improved during the examination, and he was admitted for conservative management. A non-ECG-gated contrast-enhanced CT performed after admission revealed a thrombus-like structure in the ascending aorta, prompting referral to our department (Fig. 1A). Although the initial CT suggested a relatively stable thrombus, an ECG-gated contrast-enhanced CT clearly demonstrated a thin-stalked and potentially mobile thrombus, leading to urgent surgical intervention (Fig. 1B).
Preoperative contrast-enhanced CT findings. (A) Findings on the non-ECG-gated contrast enhanced CT revealed a small thrombus-like lesion that was identified in the ascending aorta, appearing relatively stable in nature (white arrowhead). (B) The ECG-gated contrast-enhanced CT provided clearer visualization of a highly mobile thrombus-like lesion with a thin stalk, reinforcing the indication for surgical treatment (white arrow).ECG, electrocardiogram
The procedure was performed via median sternotomy. CPB was established using bilateral axillary arterial cannulation and bicaval venous drainage. To confirm that clamping of the LCCA would not reduce cerebral oxygen saturation, the artery was temporarily clamped before and after CPB initiation under NIRS monitoring. This strategy also helped prevent neurological complications during initiation of CPB. Preoperative MRA demonstrated an incomplete circle of Willis, with no communication between the anterior and posterior circulations, while robust bilateral communication was present within both the anterior and posterior circulations.
After cooling to 26°C, circulatory arrest was initiated with clamping of the brachiocephalic artery and left common carotid artery. uSCP was employed at a flow rate of 600 mL/min (Fig. 2). Given the presence of a bovine aortic arch, a common trunk reconstruction of the brachiocephalic artery and left common carotid artery had initially been planned. Under this strategy, uSCP without left subclavian artery perfusion was considered sufficient. However, due to unsuitable arterial wall for reconstruction at the common trunk, the surgical strategy was modified intraoperatively to a two-branch reconstruction. As regional cerebral oxygen saturation monitored by NIRS remained stable, uSCP was continued throughout the procedure.
Schematic illustration of the surgical procedure. (A) The ascending aortic thrombus was located just proximal to the brachiocephalic artery (red arrowhead), with adjacent calcified lesions. The brachiocephalic artery and the left common carotid artery were in close proximity. (B) During establishment of cardiopulmonary bypass, the left common carotid artery was clamped, and during circulatory arrest the brachiocephalic artery was also clamped to achieve unilateral selective cerebral perfusion (unilateral SCP). The thrombus-like lesion was excised with an adequate margin.SCP, selective cerebral perfusion
Upon opening the ascending aorta, a highly mobile thrombus-like mass was identified just proximally to the brachiocephalic artery. The lesion was excised with an adequate margin because a small possibility of malignancy could not be excluded. As the LCCA was in close proximity to the brachiocephalic artery, partial arch replacement with reconstruction of both arch branches was performed.
The aortic cross-clamp time was 63 min, and the circulatory arrest time was 39 min. The operation was completed without complications. Postoperative recovery was uneventful, with no new neurological deficits. After consulting with neurologists, the patient was discharged on POD 13, maintained on clopidogrel and warfarin for antithrombotic therapy. Pathology revealed atherosclerosis with fresh thrombi showing early organization, consistent with thrombotic etiology.
DISCUSSION
We successfully performed surgery for this rare condition of ascending AMT. This case highlights two key clinical points. First, ECG-gated contrast-enhanced CT is essential for accurate diagnosis of ascending AMT. Second, a modified brain isolation strategy using uSCP allows safe surgical management without neurological complications.
While large ascending aortic thrombi described in previous reports generally pose little diagnostic uncertainty, smaller lesions—such as in this case—may easily be mistaken for motion artifacts. This suggests that similar cases may go unrecognized, underscoring the clinical relevance of this report. Although TEE was considered, the distal ascending aorta is a well-known “blind spot,” where visualization is hindered by interposed tracheal air.^5)^ In this patient, the non-ECG-gated CT suggested a small, stable thrombus, whereas the ECG-gated contrast-enhanced CT clearly demonstrated a thin stalk, strongly indicating the need for surgery. These findings support ECG-gated contrast-enhanced CT as essential when AMT is suspected.
Preventing neurological complications is crucial when operating for ascending AMT. The brain isolation technique was originally developed for high-risk cases—such as those with a shaggy aorta—undergoing arch surgery, where complete separation of cerebral circulation reduces embolic risk.^6,7)^ In this case, although achieving relatively stagnant flow in the ascending aorta via femoral artery perfusion may be considered, bilateral axillary artery cannulation combined with left common carotid artery occlusion was selected to prioritize cerebral protection at the initiation of CPB. This strategy was chosen to reduce the risk of cerebral embolization associated with thrombus dislodgement during CPB initiation, despite the thrombus being located near the brachiocephalic artery. Alternative perfusion strategies, including femoral artery perfusion alone or in combination with left axillary artery perfusion, may represent reasonable options in selected cases and warrant further consideration. Furthermore, using right axillary artery perfusion for uSCP minimized cerebral embolization and provided an uncluttered operative field, facilitating graft anastomosis. Although some studies suggest that uSCP provides outcomes comparable to bilateral SCP, including neurological results, uSCP may also reduce the risk of embolic events associated with additional cannulation.^8)^ However, there are limitations in determining the safety of uSCP based solely on NIRS monitoring. NIRS reflects only regional oxygenation of the superficial frontal cortex and does not adequately assess global cerebral perfusion, particularly in the posterior circulation, including the cerebellum and brainstem, as reported in previous studies.^9)^ Therefore, in select cases, bilateral selective cerebral perfusion may be required to ensure more definitive and comprehensive cerebral protection, and further investigation is warranted to clarify the indications for unilateral versus bilateral SCP.
CONCLUSIONS
ECG-gated contrast-enhanced CT is the preferred diagnostic modality for ascending AMT. The CPB strategy used in this case—bilateral axillary artery cannulation with LCCA occlusion—together with the modified brain isolation technique using uSCP may provide an effective and safe approach for surgical treatment without neurological complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bowdish ME, Weaver FA, Liebman HA, et al. Anticoagulation is an effective treatment for aortic mural thrombi. J Vasc Surg 2002; 36: 713–9.12368731 · pubmed ↗
- 2Li G, Chen Y, Wang H, et al. Case report: surgical strategies of a giant thrombus from the ascending aorta to the arch. Front Cardiovasc Med 2023; 10: 1091303.36910530 10.3389/fcvm.2023.1091303 PMC 9996118 · doi ↗ · pubmed ↗
- 3Zivkovic I, Milacic P, Mihajlovic V, et al. Surgical treatment of ascending aorta floating thrombus in a patient with recent SARS-Co V-2 infection. Cardiovasc Diagn Ther 2021; 11: 467–71.33968624 10.21037/cdt-20-1010 PMC 8102247 · doi ↗ · pubmed ↗
- 4Lumia D, Carrafiello G, Laganà D, et al. Diagnosis with ECG-gated MDCT of floating thrombus in aortic arch in a patient with type-A dissection. Vasc Health Risk Manag 2008; 4: 735–9.18827925 10.2147/vhrm.s 2311 PMC 2515435 · doi ↗ · pubmed ↗
- 5Sharma M, Pathak A, Shoukat A, et al. Blind areas of cardiac imaging during transesophageal echocardiogram/endoscopic ultrasound. Endosc Ultrasound 2017; 6: 352–4.27824023 10.4103/2303-9027.193585 PMC 5664860 · doi ↗ · pubmed ↗
- 6Kikuchi Y, Kikuchi Y, Kamiya H. A simplified isolation technique for atherosclerotic aortic arch aneurysms surgery. J Surg Case Rep 2021; 2021: rjab 082.33897995 10.1093/jscr/rjab 082PMC 8055174 · doi ↗ · pubmed ↗
- 7Shiiya N, Kunihara T, Kamikubo Y, et al. Isolation technique for stroke prevention in patients with a mobile atheroma. Ann Thorac Surg 2001; 72: 1401–2.11603483 10.1016/s 0003-4975(01)02922-8 · doi ↗ · pubmed ↗
- 8Tian DH, Wilson-Smith A, Koo SK, et al. Unilateral versus bilateral antegrade cerebral perfusion: a meta-analysis of comparative studies. Heart Lung Circ 2019; 28: 844–9.30773323 10.1016/j.hlc.2019.01.010 · doi ↗ · pubmed ↗