Optimizing Large-Volume Paracentesis in a Gastroenterology Ward: A Two-Cycle Quality Improvement Project
Lok Man Chuen, Aditi Sinha, Salonee Dhungana, Inez McCurley, Rehan Khan

TL;DR
This study improved efficiency in preparing for and documenting large-volume paracentesis procedures in a gastroenterology ward using checklists and digital tools.
Contribution
A resident-led QIP introduced a checklist poster and smart text proforma to streamline paracentesis preparation and documentation.
Findings
A checklist poster reduced equipment preparation time and improved resident knowledge of required items.
A smart text proforma improved documentation speed and consistency, with all users finding it helpful.
Qualitative feedback showed increased trainee confidence and reduced uncertainty after the interventions.
Abstract
Background In a busy gastroenterology ward in a London district general hospital, delays were frequently encountered when preparing large-volume paracentesis, mainly due to difficulties in locating and gathering equipment. This Quality Improvement Project (QIP) aimed to standardize equipment preparation, improve perceived efficiency, and enhance post-procedure documentation. Methodology A resident doctor-led, two-cycle QIP was conducted using the Plan-Do-Study-Act (PDSA) methodology. Cycle one focused on equipment preparation. Baseline data were collected via surveys, followed by the introduction of a standardized equipment checklist poster displayed at the doctors’ office. Self-reported time taken to locate and gather equipment was collected pre- and post-intervention. Cycle two focused on post-procedure documentation through the development of a smart text proforma within the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
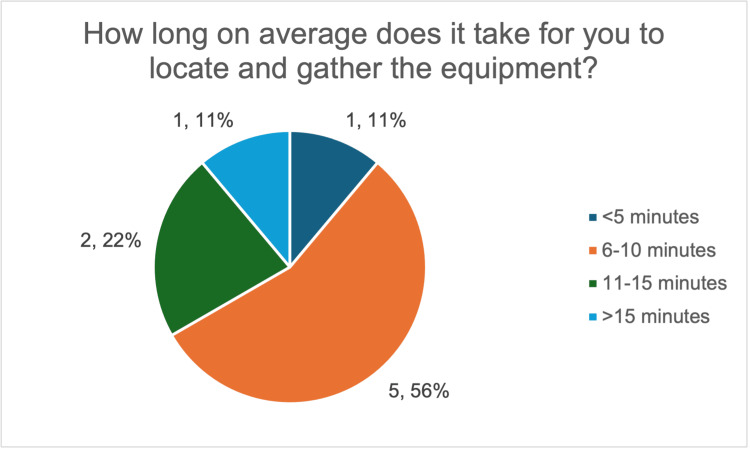 Figure 1
Figure 1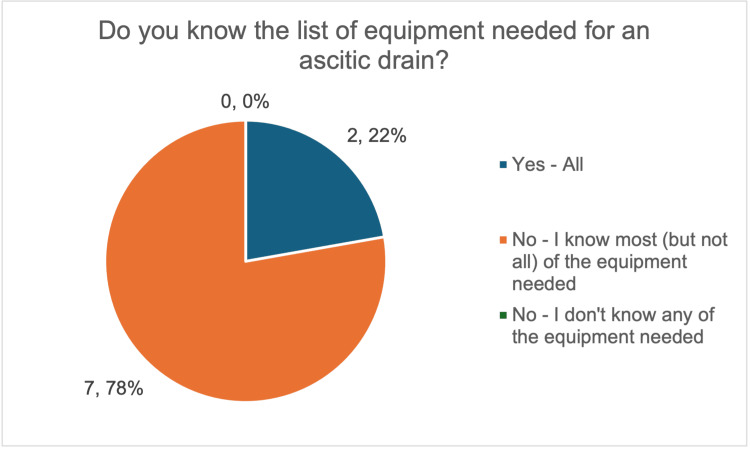 Figure 2
Figure 2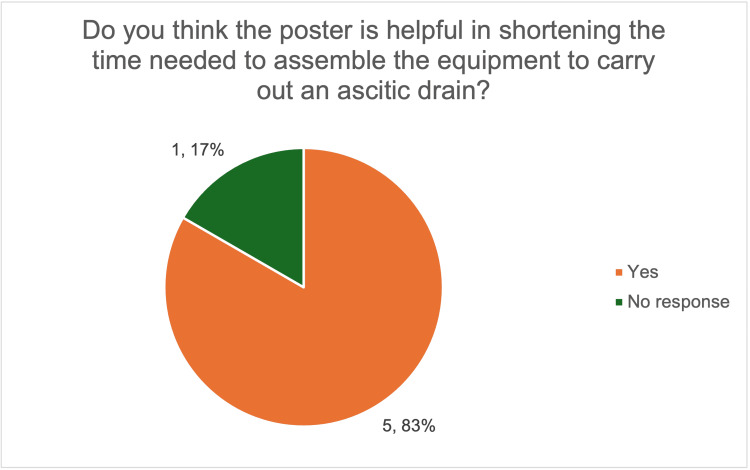 Figure 3
Figure 3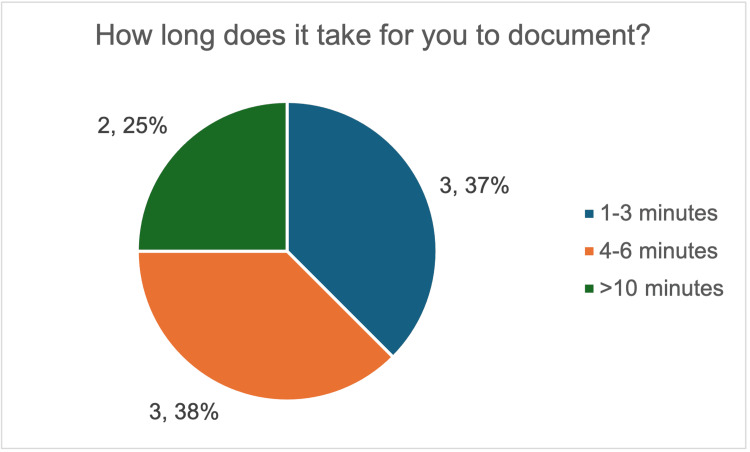 Figure 4
Figure 4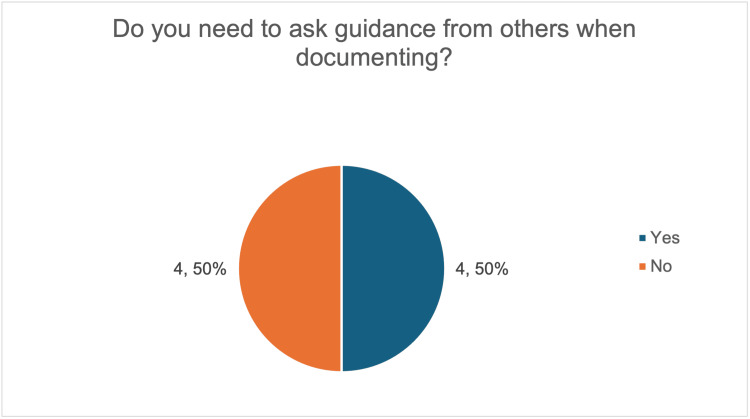 Figure 5
Figure 5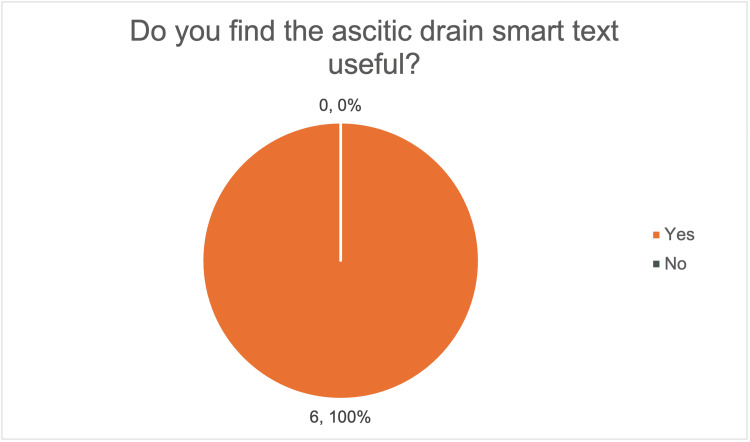 Figure 6
Figure 6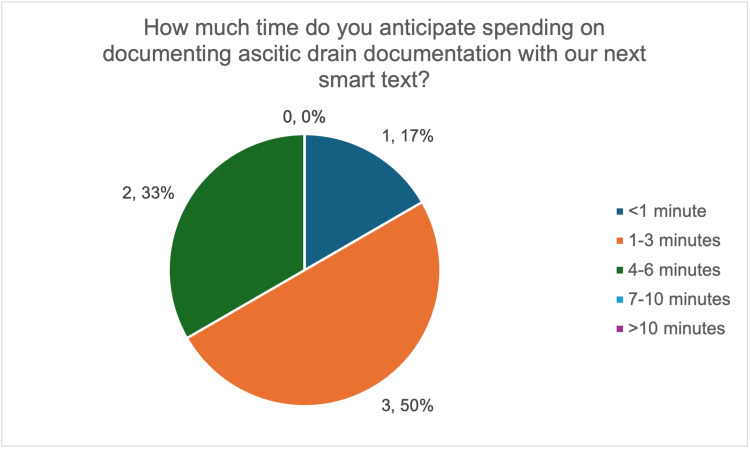 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Screening and Detection · Sepsis Diagnosis and Treatment · Healthcare cost, quality, practices
Introduction
Large-volume paracentesis (LVP) is a common but time-sensitive ward-based procedure for the management of symptomatic ascites in patients with liver disease and other conditions [1]. It involves multiple steps and requires familiarity with specific equipment. Clear and comprehensive documentation of consent, procedural details, and post-procedure care is essential to ensure patient safety and support continuity of care. International and specialty guidelines, such as those from the British Society of Gastroenterology (BSG), emphasize the importance of consistent practice and documentation for invasive procedures, including the BSG eight-point checklist for LVP [2].
In a busy gastroenterology ward in a London district general hospital, preparation of equipment and documentation is performed by several resident doctors who rotate regularly, so new doctors may be unfamiliar with ward-specific equipment and processes. Verbal feedback from resident doctors highlighted repeated delays when preparing for ascitic drain insertion, predominantly due to difficulty identifying, locating, and gathering the required equipment, especially at the start of new rotations. The lack of a consistent, easily accessible, and updated equipment list was identified as a potential contributor.
In addition, clinicians have individual preferences in post-procedure documentation, and some doctors require senior input to ensure notes are complete and safe. These factors are perceived to contribute to further delays and inconsistencies in clinical records. Audits of abdominal paracentesis have identified gaps in quality measures, including inconsistent documentation of key elements such as consent and post-procedure care [3]. Evidence from quality improvement projects (QIPs) in similar procedural settings suggests that simple standardization measures, such as formalized equipment lists, checklists, and structured documentation, can improve safety, efficiency, staff confidence, and adherence to guidelines [3-5].
This resident doctor-led QIP aimed to improve both the efficiency and consistency of ascitic drain preparation and documentation and is reported in accordance with the Standards for QUality Improvement Reporting Excellence (SQUIRE) 2.0 guidelines. Specifically, the project sought to improve workflow efficiency and reduce perceived delays for resident doctors in gathering the required equipment, and to improve the quality and efficiency of post-procedure documentation through the introduction of standardized interventions. These help reduce avoidable delays, support trainee growth, and improve the quality of patient care.
Materials and methods
This QIP was conducted in the Gastroenterology Department at Ealing Hospital, part of London North West University Healthcare NHS Trust, London, United Kingdom. Cycle one was conducted from September 17, 2025, to October 26, 2025, and cycle two from November 10, 2025, to December 2, 2025. Data were collected anonymously using structured questionnaires distributed to the nine eligible gastroenterology resident doctors at baseline and after each intervention; locum doctors were also involved where applicable. Baseline data were obtained before the introduction of the equipment checklist poster (Appendix A) and documentation smart text (Appendix B), with follow-up data collected after each Plan-Do-Study-Act (PDSA) cycle to assess change.
The survey questionnaires were developed by the resident doctor project team in line with the aims of each PDSA cycle. The pre-intervention questionnaire for cycle one (Appendix C) identified barriers to efficient equipment preparation and assessed interest in a standardized equipment checklist poster, including perceived usability. The post-intervention questionnaire (Appendix D) evaluated poster visibility, accessibility, and perceived usefulness. For cycle two, the pre-intervention questionnaire (Appendix E) established baseline self-reported documentation time and explored barriers to clear post-procedure documentation. The post-intervention questionnaire (Appendix F) assessed the usefulness of the smart text proforma, its perceived impact on efficiency, self-reported documentation time when using the proforma, and whether it reduced the need for senior guidance. Formal psychometric validation was not undertaken as this was a QIP. Face validity was ensured through review and approval by the supervising consultant before implementation. However, the questionnaires were reviewed to ensure they were appropriate and covered all key areas relevant to the project objectives.
Senior gastroenterology clinicians were consulted throughout to ensure clinical accuracy and acceptability of the interventions, and registrar feedback on equipment preferences informed checklist refinement. Patients and the public were not involved, no patient-identifiable data were used, and the project was exempt from institutional review board approval.
PDSA cycle one: equipment preparation for ascitic drains
The primary outcome measure for PDSA cycle one was the self-reported time taken by resident doctors to identify, locate, and gather the equipment required for an ascitic drain. This was defined as the self-reported time, in minutes, from starting to gather equipment to being ready to perform the procedure. Doctors’ self-reported knowledge of the required equipment and its location was included as a secondary outcome measure. These measures were chosen as they directly reflected perceived sources of delay and were practical to collect in a busy ward environment.
Delays were thought to arise mainly from uncertainty about which items were required and where they were stored. To address this, a formalized, easily accessible, and updated equipment checklist was designed. It listed all items required for ascitic drain insertion, along with guidance on appropriate ascitic fluid investigations, and was displayed in the gastroenterology doctors’ office. The aim was to support more efficient preparation.
A follow-up survey was distributed after implementation to assess change. Data collected included self-reported preparation time, awareness of required equipment and its location, and perceived usefulness of the poster. Feedback from registrars regarding individual preferences for specific equipment prompted further revision of the checklist. The poster was actively signposted to new doctors joining the ward to encourage consistent use.
PDSA cycle two: post-procedure documentation
For PDSA cycle two, the primary outcome measure was the self-reported time taken to complete post-procedure documentation following ascitic drain insertion. Secondary measures included whether doctors needed to seek guidance from colleagues and the perceived usefulness of the smart text proforma, as well as to assess efficiency, confidence, usability, and consistency of post-procedure documentation.
Inconsistencies and delays were thought to result from uncertainty about expected documentation content rather than reluctance to document. A smart text documentation proforma was then developed within the electronic patient record system (CERNER), aligned with the BSG eight-point checklist for LVP. The proforma included consent, key procedural details, post-procedure care, and nursing instructions, aimed to reduce documentation time and improve confidence among resident doctors.
A follow-up survey was distributed to assess documentation time using the proforma and its perceived usefulness. No significant barriers to implementation were identified. To support sustainability, the smart text proforma was made accessible to all resident doctors on the gastroenterology team to encourage routine use.
Results
Equipment preparation (PDSA cycle one)
At baseline, there was marked variation in the time taken to prepare equipment for ascitic drain insertion. Most respondents (five out of nine, 56%) reported requiring 6-10 minutes, 22% (two out of nine) reported taking 11-15 minutes, while 11% (one out of nine) reported taking more than 15 minutes, demonstrating variability in preparation times; only one respondent was able to prepare equipment within five minutes (Figure 1). Moreover, 78% (seven out of nine) reported knowing most, but not all, of the required equipment (Figure 2), highlighting an incomplete knowledge of required equipment.
Survey responses on the average time taken by resident doctors to locate and gather equipment for large-volume paracentesis.The image was created by the authors.
Survey responses on resident doctors’ knowledge of the equipment required for large-volume paracentesis.The image was created by the authors.
After the introduction of the equipment checklist poster, all six respondents reported having seen the poster and found it useful. Most doctors (five out of six, 83%) felt that the poster helped reduce preparation time (Figure 3). Preparation time was not objectively measured; however, most respondents reported that preparation felt quicker following the introduction of the poster, reflecting perceived rather than objectively measured improvement.
Survey responses on the perceived usefulness of the poster in reducing equipment preparation time for ascitic drains.The image was created by the authors.
Initially, differences in individual clinician preferences for equipment introduced variability. This was addressed by refining the checklist after discussion with senior clinicians to ensure accuracy. There were no delays, safety concerns, or negative impacts on patient care reported because of the intervention.
Post-procedure documentation (PDSA cycle two)
Baseline data demonstrated wide variation in both documentation time and confidence. Overall, 38% (three out of eight) reported spending four to six minutes completing notes, while 25% (two out of eight) reported spending more than 10 minutes (Figure 4). Half of the respondents (four out of eight) also needed guidance from colleagues to complete documentation (Figure 5).
Survey responses on the time taken by resident doctors to complete post-procedure documentation for large-volume paracentesis.The image was created by the authors.
Survey responses on whether resident doctors required guidance from colleagues or seniors when completing post-procedure documentation for large-volume paracentesis.The image was created by the authors.
Following the introduction of the smart text proforma, all six respondents reported that it was useful (Figure 6) and expected it to reduce documentation time. Most respondents (five out of six, 83%) anticipated being able to complete documentation within one to six minutes, with 50% (three out of six) expecting it to take less than four minutes (Figure 7), suggesting a perceived improvement.
Survey responses on the perceived usefulness of the ascitic drain smart text documentation proforma.The image was created by the authors.
Survey responses on anticipated time to complete ascitic drain documentation using the smart text proforma.The image was created by the authors.
Respondents also reported increased confidence, with all six respondents indicating that they could independently perform post-procedure documentation. This suggested that delays were mainly due to uncertainty about what needed to be included, rather than reluctance to document.
Data completeness and unintended consequences
Response rates were high across both PDSA cycles, although overall numbers were small due to the limited number of resident doctors in the department. Minor variation in respondent numbers occurred due to staff availability at the time of data collection.
No unintended negative consequences were identified. Anticipated benefits included improved trainee confidence and reduced reliance on senior colleagues. Both interventions were cost-effective and improved efficiency. Further areas of improvement, such as the addition of visual aids to the poster, were also identified, which will help guide future refinements.
Discussion
This QIP highlighted unfamiliarity with local equipment and documentation requirements as one of the key contributors to delays in procedural preparation and post-procedure documentation for LVP. Our findings are consistent with the literature describing the potential benefits of standardization, such as checklists and procedural kits, in improving procedural quality and adherence to best practice. For example, Fyson et al. demonstrated that introducing a standardized paracentesis procedure checklist and equipment kit significantly improved documentation of informed consent and aseptic technique, with reduced complication rates, suggesting procedural tools can enhance both quality and safety in paracentesis practice [3].
Structured checklist interventions have a well-established evidence base across clinical domains, including procedural interventions similar to paracentesis. For example, the World Health Organization Surgical Safety Checklist has been shown to reduce morbidity and mortality and increase compliance with procedural standards [6]. Beyond surgery, checklists and bundles have improved process measures and reduced adverse events in critical care and procedural specialties, such as central line-associated bloodstream infections and bronchoscopy [7-9].
The active involvement of resident doctors in developing and refining the equipment checklist and documentation proforma in this project likely contributed to its effectiveness. Engagement of frontline clinicians in intervention design is recognized as a key driver of sustainable improvement, and it has been associated with greater engagement, improved patient safety outcomes, and more successful implementation compared with top-down approaches [10-13]. This approach aligns with broader quality improvement methodologies that emphasize iterative testing, stakeholder engagement, and co-design to accelerate the adoption and sustainability of effective tools.
By combining continuous refinement through PDSA cycles with clear alignment to SMART goals and measurable outcomes, the project employed evidence-based quality improvement methods shown to increase the likelihood of success, and the findings suggest perceived improvements following the two interventions [14]. As there is significant variability among resident doctors in performing LVP, the poster and the proforma reinforce education on what and why to send samples for analysis after the procedure, the diagnostic criteria for spontaneous bacterial peritonitis, the importance of documenting consent, early recognition of common post-procedural complications, and post-procedural checks. Structured preparation has been shown to reduce procedural stress and improve cognitive support, contributing to safer and more efficient practice [15].
Our finding of variability in baseline practice and documentation echoes observations in other QIP reports: structured templates and documentation proformas have been shown to significantly increase the completeness and consistency of clinical records. For example, standardized forms in pediatric inflammatory bowel disease increased structured documentation from 21% to 72% post‑intervention [16], while structured admission templates improved general admission note completeness [17]. Electronic templates and checklists in electronic health records have also been shown to reduce variability, improve workflow, and enhance documentation quality [15,18].
Despite these supportive findings, there were several limitations identified in this project, including a small sample size and outcomes relying on self-reported timing rather than objective measurement. No observational, audit, or electronic health record-derived data were collected. As the project was conducted on a single gastroenterology ward, the applicability to other settings may be difficult to predict. Differences between individual practices, the rotational nature of resident doctors, and changes to locations of equipment storage over time also meant that ongoing review and refinement of the interventions were necessary.
Future QIP cycles could address these limitations by expanding sample size and incorporating objective timing measures. Evaluation could also compare documentation completed with and without the smart text template, assessing inclusion of consent, procedural details, and post-procedure care, providing a more objective measure of template effectiveness. Embedding structured preparation checklists and documentation proformas into routine clinical workflows across departments may increase uptake and sustainability, as demonstrated in other internal medicine quality improvement initiatives [19]. Broader implementation and multisite collaboration could further assess generalizability and scalability, while regular review ensures tools remain accurate, up-to-date, and aligned with evolving clinical standards.
Conclusions
Delays in procedural preparation and documentation for ascitic drains are common on busy gastroenterology wards and are often related to unfamiliarity with local equipment and documentation requirements. This QIP provides practical, ward-based evidence that simple, low-cost interventions, such as an equipment checklist poster and a smart text documentation template, can improve feasibility, usability, and perceived workflow benefit. Post-intervention data showed reduced perceived equipment preparation time and improved efficiency of post-procedure documentation. Although outcomes were primarily based on self-reported timing and perceived usefulness, consistent qualitative feedback demonstrated that both interventions were helpful, well accepted, and refined effectively through iterative PDSA cycles and user feedback. The project was cost-effective, with expenses limited to poster printing and minor IT configuration. By reducing time spent on equipment gathering and documentation, the interventions may have the potential to improve workflow efficiency and support more efficient use of clinical resources; however, formal cost or operational analysis was not performed. Sustainability has been addressed through visible poster placement, verbal signposting for new doctors, and planned updates to maintain accuracy. Overall, this project demonstrates that resident doctor-led quality improvement, focused on small and practical changes, can sustainably improve everyday clinical workflow, with potential for adaptation across other wards or institutions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guidelines on the management of ascites in cirrhosis Gut Aithal GP Palaniyappan N China L 9297020213306733410.1136/gutjnl-2020-321790 PMC 7788190 · doi ↗ · pubmed ↗
- 2British Society of Gastroenterology. Large volume paracentesis in cirrhosis: safety toolkik 12 2025 British Society of Gastroenterology 2025 https://www.bsg.org.uk/clinical-resource/large-volume-paracentesis-in-cirrhosis
- 3Abdominal paracentesis: use of a standardised procedure checklist and equipment kit improves procedural quality and reduces complications Intern Med J Fyson J Chapman L Tatton M Raos Z 5725794820182934540510.1111/imj.13741 · doi ↗ · pubmed ↗
- 4Scottish Society of Physicians. Ascitic drain insertion in practice - is our documentation up to scratch? 2 2026 Clegg F Gauci J Fraser A Mc Leman L 2019 https://abdn.elsevierpure.com/en/publications/ascitic-drain-insertion-in-practice-is-our-documentation-up-to-sc/
- 5Enhancing emergency department safety: implementation of a dedicated chest drain trolley to optimize care for pneumothorax patients Cureus Elramlawy M Parmar S Yue A 016202410.7759/cureus.76489 PMC 1168197039734559 · doi ↗ · pubmed ↗
- 6WHO Surgical Safety Checklist 2 2026 World Health Organization 2026 https://www.who.int/teams/integrated-health-services/patient-safety/research/safe-surgery/tool-and-resources
- 7Quality improvement in respiratory medicine: designing and implementing a bronchoscopy checklist at Southend University Hospital BMJ Qual Improv Rep Thillai M Powrie D 2201310.1136/bmjquality.u 201878.w 997PMC 465272226734191 · doi ↗ · pubmed ↗
- 8Implementation of systematic safety checklists in a neurocritical care unit: a quality improvement study BMJ Open Qual Escamilla-Ocañas CE Torrealba-Acosta G Mandava P 011202210.1136/bmjoq-2022-001824 PMC 974337936588320 · doi ↗ · pubmed ↗