Development and validation of the polycystic ovary syndrome-related complaint severity scale
Özlem Kaplan, Mürüvvet Başer, Nurseli Soylu Erener, Ali Kaplan, Busra Emir, Gökhan Açmaz

TL;DR
This study created and validated a new scale to measure the severity of complaints in women with polycystic ovary syndrome.
Contribution
A novel and validated scale for assessing PCOS-related complaints was developed and tested for reliability and validity.
Findings
A four-factor structure was identified, explaining 57.416% of the variance.
The scale showed good model fit with RMSEA=0.065 and CFI=0.913.
High internal consistency (Cronbach’s alpha=0.897) and strong test–retest reliability were confirmed.
Abstract
The aim of this study was to develop and validate the Severity of the Complaints Related to Polycystic Ovary Syndrome Scale. This methodological study employed exploratory factor analysis and confirmatory factor analysis. Internal consistency was assessed through item–total correlations and the test–retest method. Exploratory factor analysis revealed a four-factor structure explaining 57.416% of the variance. Confirmatory factor analysis results confirmed a good model fit (χ2/df=3.094, RMSEA=0.065, CFI=0.913, GFI=0.910). The overall Cronbach’s alpha coefficient was 0.897. In the test–retest reliability analyses, significant correlations were found between all items and factor scores across the two administrations (p<0.001). The scale is a valid and reliable measure for assessing the severity of complaints related to Polycystic Ovary Syndrome Scale.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
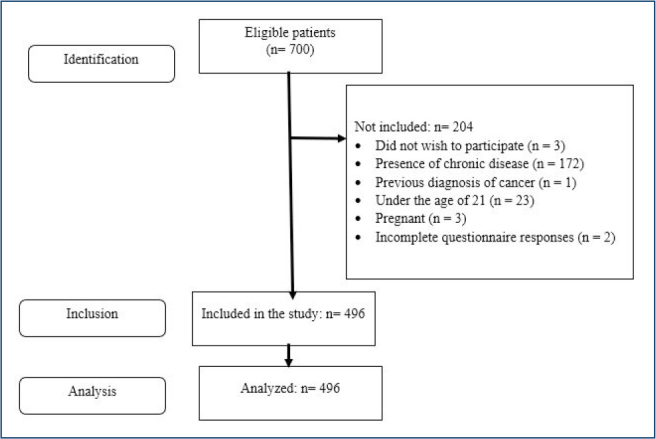 Figure 1
Figure 1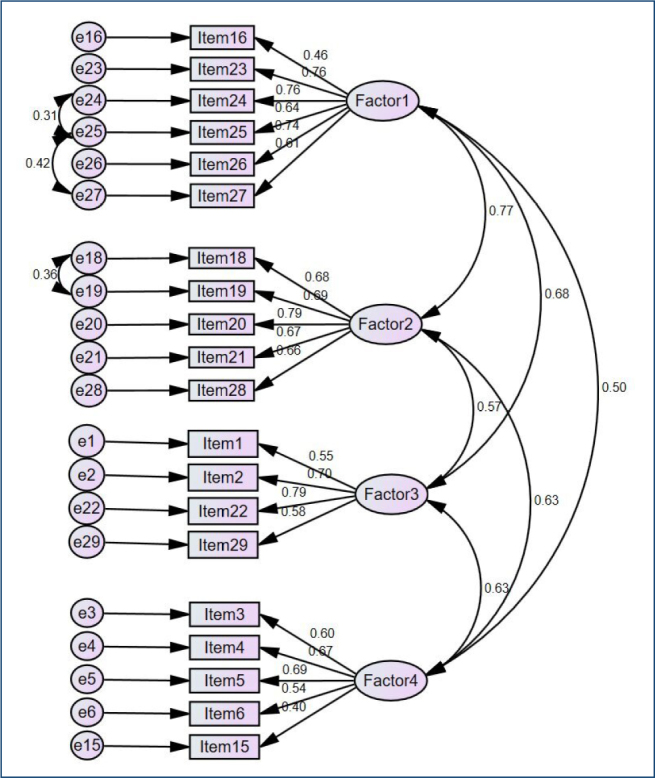 Figure 2
Figure 2| First step | Last step | |||||||
|---|---|---|---|---|---|---|---|---|
| Scale mean if item deleted | Scale variance if item deleted | Corrected item–total correlation | Cronbach’s alpha if item deleted | Scale mean if item deleted | Scale variance if item deleted | Corrected item–total correlation | Cronbach’s alpha if item deleted | |
| Item-1 | 92.4758 | 276.969 | 0.448 | 0.892 | 64.1774 | 166.954 | 0.458 | 0.894 |
| Item-2 | 92.0585 | 275.708 | 0.418 | 0.892 | 63.7601 | 165.476 | 0.444 | 0.894 |
| Item-3 | 92.9234 | 273.138 | 0.454 | 0.891 | 64.6250 | 165.415 | 0.412 | 0.895 |
| Item-4 | 92.9536 | 270.198 | 0.500 | 0.891 | 64.6552 | 163.265 | 0.455 | 0.894 |
| Item-5 | 92.1754 | 274.707 | 0.519 | 0.891 | 63.8770 | 166.011 | 0.497 | 0.893 |
| Item-6 | 92.2500 | 275.638 | 0.468 | 0.891 | 63.9516 | 167.840 | 0.403 | 0.895 |
| Item-7 | 92.6956 | 275.735 |
| 0.893 | – | – | – | – |
| Item-8 | 92.9758 | 277.660 |
| 0.894 | – | – | – | – |
| Item-9 | 94.5484 | 281.283 |
| 0.894 | – | – | – | – |
| Item-10 | 93.5444 | 281.550 |
| 0.896 | – | – | – | – |
| Item-11 | 92.7944 | 277.602 |
| 0.893 | – | – | – | – |
| Item-12 | 92.7984 | 278.270 |
| 0.894 | – | – | – | – |
| Item-13 | 92.7036 | 278.629 |
| 0.895 | – | – | – | – |
| Item-14 | 92.8488 | 274.533 |
| 0.894 | – | – | – | – |
| Item-15 | 92.7056 | 274.653 | 0.417 | 0.892 | 64.4073 | 165.854 | 0.400 | 0.896 |
| Item-16 | 94.2823 | 272.607 | 0.467 | 0.891 | 65.9839 | 163.685 | 0.469 | 0.894 |
| Item-17 | 92.6431 | 278.347 |
| 0.896 | – | – | – | – |
| Item-18 | 92.2319 | 273.855 | 0.609 | 0.889 | 63.9335 | 164.854 | 0.609 | 0.890 |
| Item-19 | 92.3891 | 271.111 | 0.571 | 0.889 | 64.0907 | 162.935 | 0.561 | 0.891 |
| Item-20 | 92.5786 | 273.792 | 0.576 | 0.890 | 64.2802 | 163.952 | 0.612 | 0.890 |
| Item-21 | 92.4839 | 274.703 | 0.505 | 0.891 | 64.1855 | 164.729 | 0.534 | 0.892 |
| Item-22 | 92.1310 | 270.280 | 0.571 | 0.889 | 63.8327 | 160.673 | 0.621 | 0.889 |
| Item-23 | 93.4536 | 264.357 | 0.610 | 0.888 | 65.1552 | 156.447 | 0.640 | 0.888 |
| Item-24 | 93.5988 | 265.748 | 0.596 | 0.888 | 65.3004 | 157.136 | 0.639 | 0.888 |
| Item-25 | 93.8508 | 268.903 | 0.496 | 0.891 | 65.5524 | 159.185 | 0.547 | 0.891 |
| Item-26 | 93.1472 | 264.530 | 0.602 | 0.888 | 64.8488 | 156.504 | 0.634 | 0.888 |
| Item-27 | 93.6653 | 269.985 | 0.461 | 0.891 | 65.3669 | 160.354 | 0.500 | 0.893 |
| Item-28 | 92.1694 | 275.559 | 0.558 | 0.890 | 63.8710 | 165.414 | 0.593 | 0.891 |
| Item-29 | 92.6815 | 270.044 | 0.510 | 0.890 | 64.3831 | 162.245 | 0.494 | 0.893 |
| Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 | % of variance explained | Cronbach’s alpha | |
|---|---|---|---|---|---|---|---|
| Item-25 | I hesitate to have romantic relationships. | 0.849 | 0.094 | 0.075 | 0.123 | 35.053 | 0.842 |
| Item-27 | I hesitate to have sexual intimacy. | 0.816 | 0.113 | 0.072 | 0.041 | ||
| Item-24 | I avoid going into social environments. | 0.754 | 0.223 | 0.146 | 0.218 | ||
| Item-23 | I don’t really feel like a woman anymore. | 0.603 | 0.314 | 0.070 | 0.390 | ||
| Item-26 | I think that my complaints affect my family life negatively. | 0.552 | 0.467 | 0.130 | 0.192 | ||
| Item-16 | There are times when my breathing stops (apnea), I feel choked, or I wake up with a feeling of suffocation. | 0.358 | 0.236 | 0.306 | 0.124 | ||
| Item-19 | I experience sudden changes in emotion such as laughing, crying, or getting angry. | 0.047 | 0.821 | 0.221 | 0.150 | 9.577 | 0.833 |
| Item-20 | I feel unhappy. | 0.333 | 0.772 | 0.074 | 0.122 | ||
| Item-18 | I feel tense and nervous. | 0.140 | 0.748 | 0.181 | 0.253 | ||
| Item-21 | I have difficulty concentrating. | 0.311 | 0.579 | 0.278 | -0.021 | ||
| Item-28 | I feel tired during the day. | 0.289 | 0.471 | 0.467 | 0.060 | ||
| Item-2 | I gain weight quickly and have difficulty losing weight. | 0.074 | 0.031 | 0.159 | 0.854 | 7.331 | 0.746 |
| Item-22 | I am not satisfied with my physical appearance. | 0.317 | 0.249 | 0.151 | 0.694 | ||
| Item-29 | I have a swelling (edema) problem in different parts of my body such as hands, face, and legs. | 0.163 | 0.188 | 0.204 | 0.610 | ||
| Item-1 | I can’t control my appetite. | 0.117 | 0.060 | 0.386 | 0.534 | ||
| Item-4 | I experience symptoms such as sudden hunger, trembling hands and feet, cold sweating. | 0.073 | 0.134 | 0.787 | 0.061 | 5.455 | 0.704 |
| Item-3 | I am experiencing thirst and dry mouth. | 0.065 | 0.060 | 0.685 | 0.160 | ||
| Item-5 | I feel sleepy and heavy after eating. | 0.065 | 0.258 | 0.670 | 0.150 | ||
| Item-6 | I have gastrointestinal problems such as indigestion, gas, and bloating. | 0.041 | 0.105 | 0.582 | 0.230 | ||
| Item-15 | I have a sleep disorder. | 0.199 | 0.169 | 0.367 | 0.183 | ||
| Total | 57.416 | 0.897 | |||||
| Confirmatory factor analysis results | |||||||
| Goodness-of-fit indices | χ2/df | RMSEA | SRMR | CFI | GFI | NNFI | |
| Reference value | <3 (<0.05) | ≤0.08 | ≤0.10 | ≥0.90 | ≥0.85 | ≥0.90 | |
| Model | 3.094 (<0.001) | 0.065 | 0.060 | 0.913 | 0.910 | 0.883 | |
| Correlation coefficient p-value | Total | Factor 1 | Factor 2 | Factor 3 | Factor 4 | BMI | Age | Time of married | PCOS month | PCOS treatment month | Menstrual cycle duration day | Menstrual bleeding duration day | How many days ago was your last period | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Rho | 1.000 | ||||||||||||
| p-value | ||||||||||||||
| Factor 1 | Rho | 0.846 | 1.000 | |||||||||||
| p-value |
| |||||||||||||
| Factor 2 | Rho | 0.792 | 0.585 | 1.000 | ||||||||||
| p-value |
|
| ||||||||||||
| Factor 3 | Rho | 0.755 | 0.523 | 0.467 | 1.000 | |||||||||
| p-value |
|
|
| |||||||||||
| Factor 4 | Rho | 0.716 | 0.386 | 0.497 | 0.510 | 1.000 | ||||||||
| p-value |
|
|
|
| ||||||||||
| BMI | Rho | 0.324 | 0.254 | 0.084 | 0.522 | 0.193 | 1.000 | |||||||
| p-value |
|
| 0.061 |
|
| . | ||||||||
| Age | Rho | -0.080 | -0.015 | -0.135 | -0.011 | -0.104 | 0.106 | 1.000 | ||||||
| p-value | 0.076 | 0.737 |
| 0.805 |
|
| ||||||||
| Time of marriage | Rho | 0.047 | 0.120 | -0.001 | 0.067 | -0.034 | 0.167 | 0.695 | 1.000 | |||||
| p-value | 0.468 | 0.062 | 0.991 | 0.298 | 0.600 |
|
| |||||||
| PCOS month | Rho | 0.06 | 0.115 | -0.017 | 0.044 | 0.002 | 0.068 | 0.384 | 0.274 | 1.000 | ||||
| p-value | 0.182 |
| 0.704 | 0.327 | 0.970 | 0.130 |
|
| . | |||||
| PCOS treatment month | Rho | 0.075 | 0.067 | 0.034 | 0.079 | 0.068 | -0.017 | -0.091 | -0.211 | 0.116 | 1.000 | |||
| p-value | 0.109 | 0.156 | 0.475 | 0.094 | 0.152 | 0.715 | 0.053 |
|
| |||||
| Menstrual cycle duration, days | Rho | 0.071 | 0.040 | 0.086 | 0.027 | 0.081 | 0.050 | -0.067 | -0.045 | 0.077 | -0.149 | 1.000 | ||
| p-value | 0.113 | 0.378 | 0.055 | 0.553 | 0.073 | 0.270 | 0.136 | 0.489 | 0.088 |
| . | |||
| Menstrual bleeding duration day | Rho | -0.101 | -0.049 | -0.047 | -0.082 | -0.148 | -0.024 | 0.021 | 0.163 | 0.027 | -0.065 | 0.133 | 1.000 | |
| p-value |
| 0.273 | 0.295 | 0.069 |
| 0.601 | 0.64 |
| 0.542 | 0.168 |
| . | ||
| How many days ago was your last period | Rho | 0.085 | 0.100 | 0.071 | 0.054 | 0.029 | 0.078 | -0.033 | -0.049 | 0.061 | -0.036 | 0.425 | 0.026 | 1.000 |
| p-value | 0.059 |
| 0.113 | 0.231 | 0.517 | 0.081 | 0.460 | 0.450 | 0.178 | 0.449 |
| 0.562 | . |
| First measurement Mean±SD Median (IQR) | Second measurement Mean±SD Median (IQR) | Test statistics | p-value | ICC | p-value | |
|---|---|---|---|---|---|---|
| Factor 1 | 16.42±5.82 | 15.94±6.14 | 3.136 | 0.002 | 0.987 (0.977–0.992) |
|
| Factor 2 | 19.64±2.73 | 19.72±2.99 | 0.703 | 0.482 | 0.936 (0.889–0.963) |
|
| Factor 3 | 15.78±3.61 | 15.78±3.61 | 1.659 | 0.097 | 0.971 (0.949–0.983) |
|
| Factor 4 | 18.74±3.47 | 18.90±3.63 | 1.171 | 0.242 | 0.959 (0.929–0.977) |
|
| Total | 70.38±11.47 | 70.34±12.47 | 0.212 | 0.832 | 0.982 (0.968–0.990) |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Ovarian cancer diagnosis and treatment · Reproductive Biology and Fertility
INTRODUCTION
Polycystic ovary syndrome (PCOS) is a multifactorial endocrine disorder affecting women of reproductive age^ 1 ^. PCOS can be seen in approximately 9.2% of women of reproductive age^ 2,3 ^. Women diagnosed with PCOS have an increased risk of insulin resistance, type 2 diabetes, cardiovascular diseases, and infertility, as well as depression and anxiety^ 3,4,5 ^. Symptoms such as dyslipidemia, hypertension, hyperinsulinemia, sugar cravings, frequent urination, delayed healing of wounds, fatigue, blurred vision, tingling, mood changes, obesity, skin fat, and spotting are commonly seen in these patients. In addition, complaints such as pelvic pain, fever, nausea, vomiting, urinary system problems, irritable bowel syndrome, constipation, sleep apnea, and deterioration in body image are also frequently experienced^ 6,7 ^.
PCOS is a multifaceted condition that negatively impacts women’s quality of life and can lead to serious short- and longterm health issues. Currently, no reliable and valid tool in the literature measures the physiological, psychological, and social complaints specific to PCOS. This study aims to fill this critical gap by developing a new measurement instrument to quantitatively assess the severity of PCOS-related complaints.
METHODS
Study design and procedure
This prospective, cross-sectional, and descriptive study was conducted in Türkiye between May and August 2024, involving 496 women diagnosed with PCOS.
Conceptual framework
The conceptual framework of the scale development study focused on determining the severity of complaints experienced by patients due to PCOS. It creates a structure for determining women’s physiological, psychological, and social complaints that may lead to short- and long-term health problems due to PCOS. In line with this conceptual framework, a literature review was conducted on a large number of articles, including systematic reviews, meta-analyses, guidelines, and qualitative studies, in which PCOS symptoms and complaints were determined^ 3,4,5,7,8 ^. In addition, the development process benefited from the experiences, observations, and insights gained through patient care practices by physicians and researchers, ensuring that the scale items were grounded in real-world clinical contexts. The qualitative findings obtained from these interviews were analyzed using inductive content analysis^ 9 ^, resulting in 32 preliminary items for the initial version of the scale.
Content analysis
Content validity was assessed using the Lawshe technique^ 10 ^. Expert evaluations were conducted in two stages to review the 32 preliminary items. Based on feedback, three items were removed and others revised. For 20 experts, a CVR≥0.42 was acceptable at α=0.05^ 11 ^. Item CVRs ranged from 0.85 to 1.0, with an overall CVI of 0.96. Language revisions by three experts finalized the scale as a 29-item scale, and responses were rated on a five-point Likert scale ranging from 1 (never) to 5 (always).
Participants
Women diagnosed with PCOS by a physician were included in the study. Based on the recommendation of having at least 10 participants per item for a 29-item scale, a minimum sample size of 290 was required^ 12 ^, and a final sample of 496 was confirmed adequate via the KMO test.
A total of 700 women were contacted, but 204 were excluded (Figure 1). Inclusion criteria were women aged 21 or older, diagnosed with PCOS by a physician, who gave informed consent online, and completed all forms. Exclusion criteria included pregnancy, menopause, chronic diseases (e.g., non-classical 21-hydroxylase deficiency, type 1 diabetes mellitus, acute or chronic renal failure, thyroid dysfunction, Cushing’s syndrome, hyperprolactinemia), and history of cancer.
Study flow diagram.
Data collection
Data were collected in Türkiye between May and August 2024 from women diagnosed with PCOS. The questionnaire, prepared via Google Forms, was sent by text message. To prevent duplicate entries, responses were restricted to one per IP address. For reliability assessment, a test–retest procedure was conducted with 50 participants, and the second administration of the scale was performed four weeks after the first one. Data were collected through two instruments: an 18-item Descriptive Characteristics Form and the 29-item draft of the PCOS-Related Complaints Scale.
Data analysis
Statistical analyses were conducted using IBM SPSS Statistics v.25 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as frequency (n), percentage (%), mean ± standard deviation, minimum–maximum, or median (IQR). The Shapiro-Wilk test and Q-Q plots were used to assess the normality of numerical variables. Content validity ratios were calculated. For the PCOS-Related Complaints Scale, construct validity, internal consistency reliability, test–retest reliability, and item analysis were performed. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to assess construct validity. It was assumed that the four latent factors in the model (Factor 1, Factor 2, Factor 3, and Factor 4) could be conceptually related to each other, and therefore, correlations among them were allowed. Before EFA, Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) test were conducted to determine data suitability and sample adequacy^ 13 ^. EFA was performed using the principal components method with varimax rotation, resulting in a four-factor structure. Cronbach’s alpha coefficient was calculated for internal consistency reliability. Spearman correlation analysis was used to evaluate the relationship between total and subscale scores. CFA was performed using IBM AMOS v.23 to test whether the factor structure identified in the EFA fit the observed data. Model fit was assessed using fit indices including χ^2^/df, SRMR, RMSEA, CFI, GFI, AGFI, NFI, and NNFI. A significance level of p<0.05 was considered statistically significant^ 14 ^.
Ethical considerations
This study was performed following the Helsinki Declaration and has been approved by the Kayseri University’s Ethics Committee University’s Ethics Committee (approval date/number: 26.03.2024/94141). All participants were provided with detailed information about the study’s purpose and scope. Informed consent was obtained through an online consent checkbox labeled “I Agree” on the survey form.
RESULTS
The mean age of the women was 27.20±4.34 (min: 20–max: 45) years, and the mean body mass index was 27.73±6.25 kg/m^2^. On average, they had been married for 4.54±4.55 years, and 52.4% were single. The mean diagnosis of PCOS was 83.83±66.42 months, and 62.1% of the participants had not received any medical treatment for this condition before. The mean duration of treatment for PCOS was 13.32±26.68 months. In addition, the mean menstrual cycle duration was 55.12±62.34 days, and the mean menstrual bleeding duration was 6.06±3.72 days. It was also determined that the participants experienced their last menstrual bleeding an average of 31.62±55.99 days prior.
A corrected item–total correlation above 0.40 is recommended in the literature^ 15 ^. Items 7–14 and 17, which fell below this threshold, were removed step by step, and scale statistics were recalculated. The final analysis was conducted on the remaining 20 items (Table 1).
ANOVA with Tukey’s test for non-additivity revealed that the scale has a summable structure (F=78.542, p<0.001). The KMO value was 0.904, and Bartlett’s test of sphericity was significant (χ^2^=4002.377, p<0.001), confirming the suitability of the data for factor analysis. Principal component analysis with varimax rotation revealed a four-factor structure explaining 57.416% of the total variance. These factors were identified as systemic and social impact complaints (items 16, 23–27), emotional complaints (items 18–21, 28), complaints related to physical appearance (items 1, 2, 22, 29), and physiological complaints (items 3–6, 15). Cronbach’s alpha values for the subscales ranged from 0.704 to 0.842, indicating good internal consistency. CFA confirmed the four-factor model, and fit indices demonstrated an acceptable model fit according to standard criteria (Table 2 and Figure 2)^ 16 ^.
Path diagram.
As a result of the CFA, it was observed that the four latent variables in the model (Factor 1: Systemic and Social Impact Complaints, Factor 2: Emotional Complaints, Factor 3: Complaints Related to Physical Appearance, and Factor 4: Physiological Complaints) were positively and significantly correlated with each other. The correlation coefficients among the factors ranged from 0.50 to 0.77. The highest correlation between Factor 1 and Factor 2 (r=0.77) indicated a strong conceptual relationship between these two dimensions. The correlations between Factor 1 and Factor 4, Factor 2 and Factor 4, Factor 3 and Factor 4, and Factor 2 and Factor 3 were r=0.50, r=0.63, r=0.63, and r=0.57, respectively. These findings suggest that the factors are not entirely independent; however, the structural distinctiveness of the scale is maintained. Therefore, conceptual overlaps among factors are expected and consistent with the nature of multidimensional scales (Figure 2).
Regarding the relationships between the scale and continuous variables, a weak positive correlation was found between the total score and body mass index (BMI) (r=0.324; p<0.001), while a weak negative correlation was found between the total score and menstrual bleeding duration (r=-0.101; p=0.024). No significant correlations were found between the total score and age, duration of marriage, duration of PCOS diagnosis, duration of PCOS treatment, menstrual cycle length, or the time since the last menstrual period (p>0.05). Among the sub-dimensions, Factor 1 was weakly and positively correlated with BMI (r=0.254; p<0.001) and duration of PCOS diagnosis (r=0.115; p=0.010). Factor 2 was weakly and negatively correlated with age (r=-0.135; p=0.003). Factor 3 was weakly and positively correlated with BMI (r=0.522; p<0.001). Factor 4 was weakly and positively correlated with BMI (rho=0.193; p<0.001) and negatively correlated with age (rho=-0.104; p=0.020) and menstrual bleeding duration (rho=-0.200; p=0.001). No other significant correlations were detected between the sub-dimensions and continuous variables (p>0.05) (Table 3).
A small but statistically significant difference was observed in Factor 1 between the test and retest. The first measurement mean rank score was higher than the second measurement mean rank score (p=0.012). However, this reflected only a systematic yet minimal mean shift that did not impair reliability (ICC=0.987). For Factor 2, Factor 3, Factor 4, and total scores, similarity was found between the first and second scores obtained from the scale (p>0.05). There was a high level of agreement between the first and second measurements, as indicated by the ICC values. Additionally, the Cronbach’s alpha value of the scale was found to be 0.856 in the analysis performed using the test–retest method. According to these findings, the scale is reliable (Table 4).
DISCUSSION
The PCOS-related complaint severity scale was developed to fill the gap in measuring the specific intensity of PCOS-related symptoms. Unlike quality-of-life tools^ 17 ^, this scale focuses on symptom severity and supports multidisciplinary care. It consists of four factors and 20 items. Content validity refers to how well scale items represent the targeted construct and is typically evaluated by experts^ 18 ^. In this study, the Lawshe technique was applied, which recommends involving 5–40 experts^ 19 ^. Feedback from 20 experts indicated that all items had CVR values ≥0.85 (threshold=0.42)^ 17 ^, and the overall CVI was 0.96, confirming strong content validity.
Item analysis evaluates how well each item contributes to the overall reliability and internal structure of a scale^ 20 ^. A corrected item–total correlation above 0.40 is recommended in the literature^ 21 ^. In this study, nine items below this threshold were removed. The remaining 20 items had correlations ranging from 0.400 to 0.640, indicating that they are distinctive and consistently measure the intended construct^ 12 ^. Factor analysis is used to identify the underlying structure of observed variables by grouping-related items into core factors^ 22 ^. To assess sample adequacy, the KMO and Bartlett’s tests were applied. A KMO value above 0.80 is acceptable; in this study, it was 0.904^ 23 ^, and Bartlett’s test was statistically significant (p<0.001). These results indicate that the sample was sufficient and appropriate for factor analysis.
In factor analysis, axis rotation clarifies factor structure, and a total explained variance of at least 30% is recommended for multidimensional scales^ 12 ^. In this study, four factors emerged from 20 items, explaining 57.416% of the total variance (35.053, 9.577, 7.331, and 5.455%, respectively). Out of which, 40–60% of the variance is considered sufficient in scale development^ 24 ^, indicating a strong internal structure. The scale also demonstrated high reliability, with a Cronbach’s alpha of 0.897.
As shown in Table 2, factor analysis grouped the items into four dimensions: systemic and social impact complaints (6 items), emotional complaints (5 items), complaints about physical appearance (4 items), and physiological complaints (5 items). Cronbach’s alpha values for the factors were 0.842, 0.833, 0.746, and 0.704, respectively. Since values above 0.70 indicate acceptable reliability^ 16 ^, the scale and sub-dimensions demonstrate strong internal consistency and reliability. CFA tests whether the proposed factor structure fits the data and confirms the sub-dimensions identified during construct validity assessment. Acceptable fit is indicated by χ^2^/df between 2 and 3, RMSEA≤0.08, p<0.05, SRMR<0.10, and CFI, GFI, NNFI≥0.90^ 16 ^. The analysis results showed that the model demonstrated an acceptable fit to the data (χ^2^/df=3.094, p<0.001, RMSEA=0.065, SRMR=0.060, CFI=0.913, GFI=0.910, NNFI=0.883). Although the NNFI value was slightly below the ideal threshold, it was close to the acceptable limit, and all other indices indicated a satisfactory model fit, supporting the adequacy of the four-factor structure.
The test–retest method, commonly used to assess reliability, expects a correlation above 0.70 between repeated measurements^ 20,25 ^. In this study, test–retest correlations were 0.987 (Factor 1), 0.936 (Factor 2), 0.971 (Factor 3), 0.959 (Factor 4), and 0.982 for the total score, all statistically significant (p<0.001). These results confirm the scale’s high reliability. The severity of complaints related to PCOS Scale is a valid and reliable 20-item tool with four sub-dimensions, scored on a 5-point Likert scale. The total score ranges from 20 to 100, with higher scores indicating greater severity of PCOS-related complaints.
Convergent validity refers to the extent to which a newly developed instrument correlates positively with other measures that assess similar or related constructs, thereby demonstrating that it measures the intended concept. In the literature, convergent validity is typically evaluated by examining correlations between the new scale and existing validated instruments. However, in the absence of a gold-standard or comparable tool measuring the same construct, it is also acceptable to assess convergent validity through correlations with relevant clinical or psychological variables that are theoretically expected to be associated with the construct^ 16,22 ^. In this study, convergent validity was examined through correlation analyses between the scale scores and continuous variables, including age, BMI, menstrual characteristics, and duration of PCOS diagnosis and treatment. These associations provided empirical support consistent with theoretical expectations regarding PCOS-related symptom severity. Although this approach offers preliminary evidence of construct validity, future research could further evaluate convergent validity by comparing the scale scores with other standardized psychological or clinical measures, such as instruments assessing depression, anxiety, body image, or hyperandrogenism.
Limitations
This study has some limitations. Although the scale development process included interviews with patients conducted by physicians and experienced researchers, more extensive qualitative studies could further enrich the item pool and enhance content validity. The sample primarily consisted of Turkish women; therefore, the findings may not be generalizable to other cultures. The criterion validity of the scale was not evaluated against a gold-standard measure. However, convergent validity was partially examined through correlation analyses with continuous variables within this study. Future studies are recommended to further assess convergent validity by comparing the scale scores with other established psychological or clinical instruments.
CONCLUSION
This study introduced a valid and reliable scale to assess the severity of PCOS-related complaints. It provides a practical tool for clinical and research settings, facilitating symptom evaluation, individualized care planning, and monitoring interventions to improve patient outcomes and satisfaction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baracat EC Baracat MCP José MSJ Are there new insights for the definition of PCOS?Gynecol Endocrinol 2022389703410.1080/09513590.2022.212138736102342 · doi ↗ · pubmed ↗
- 2Giordano LA Giordano MV Célia Teixeira Gomes R Santos Simões R Baracat MCP Giordano MG Effects of clinical and metabolic variables and hormones on the expression of immune protein biomarkers in the endometrium of women with polycystic ovary syndrome and normal-cycling controls.Gynecol Endocrinol 20223865081510.1080/09513590.2022.206145435393909 · doi ↗ · pubmed ↗
- 3Sadeghi HM Adeli I Calina D Docea AO Mousavi T Daniali M Polycystic ovary syndrome: a comprehensive review of pathogenesis, management, and drug repurposing.Int J Mol Sci 202223258310.3390/ijms 2302058335054768 PMC 8775814 · doi ↗ · pubmed ↗
- 4Gomez JMD Van Hise K Stachenfeld N Chan JL Merz NB Shufelt C Subclinical cardiovascular disease and polycystic ovary syndrome.Fertil Steril 202211759122310.1016/j.fertnstert.2022.02.02835512975 PMC 10322116 · doi ↗ · pubmed ↗
- 5Lorenzo M Cacciapuoti N Lonardo MS Nasti G Gautiero C Belfiore A Pathophysiology and nutritional approaches in polycystic ovary syndrome (PCOS): a comprehensive review.Curr Nutr Rep 20231235274410.1007/s 13668-023-00479-837213054 PMC 10444658 · doi ↗ · pubmed ↗
- 6Bazarganipour F Taghavi SA Asemi Z Allan H Khashavi Z Safarzadeh T The impact of irritable bowel syndrome on health-related quality of life in women with polycystic ovary syndrome.Health Qual Life Outcomes 202018122610.1186/s 12955-020-01428-732660493 PMC 7358924 · doi ↗ · pubmed ↗
- 7Loh HH Yee A Loh HS Kanagasundram S Francis B Lim LL Sexual dysfunction in polycystic ovary syndrome: a systematic review and meta-analysis.Hormones (Athens)20201934132310.1007/s 42000-020-00210-032462512 · doi ↗ · pubmed ↗
- 8Salari N Nankali A Ghanbari A Jafarpour S Ghasemi H Dokaneheifard S Global prevalence of polycystic ovary syndrome in women worldwide: a comprehensive systematic review and meta-analysis.Arch Gynecol Obstet 2024310313031410.1007/s 00404-024-07607-x 38922413 · doi ↗ · pubmed ↗