Comparing Efficacy and Safety of Itraconazole Solution Versus Posaconazole for Antifungal Prophylaxis After Heart Transplant
Ralph Tayyar, Darra Drucker, Roy Lee, Thu Le, Jeff Teuteberg, Kiran Khush, Helen Luikart, Tyler Intrieri, Yasbanoo Moayedi, William Alegria, Thomas Dieringer, Erik Henricksen, Aruna Subramanian

TL;DR
This study compared itraconazole and posaconazole for preventing fungal infections in heart transplant patients and found posaconazole to be more effective with fewer therapy changes.
Contribution
The study provides new comparative data on the efficacy and safety of itraconazole versus posaconazole in heart transplant recipients.
Findings
Posaconazole was associated with a lower rate of fungal infections compared to itraconazole.
Fewer patients on posaconazole required a change to alternative antifungal therapy.
Abstract
Posaconazole and itraconazole are 2 oral agents that are commonly prescribed for heart transplant recipients requiring Aspergillus prophylaxis; however, there are limited data comparing their efficacy and tolerability. This was a single-center, retrospective cohort study comparing itraconazole and posaconazole for the prevention of invasive fungal infections in heart transplant recipients between January 2015 and May 2022. The primary efficacy outcome was incidence of fungal infection. The primary safety outcome was incidence of hepatic dysfunction after initiation of therapy. Standard duration of prophylaxis therapy was 3 months for both cohorts. A total of 134 patients received itraconazole prophylaxis and 98 received posaconazole prophylaxis. Patients receiving itraconazole were more likely to have received induction immunosuppression (P < .001) and more likely to have received a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
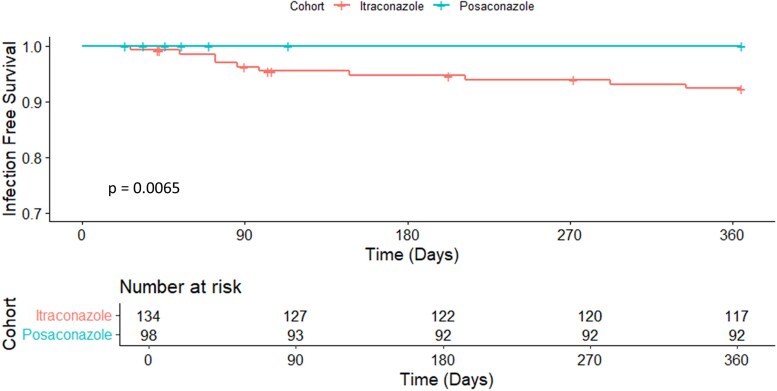 Figure 1
Figure 1| Baseline Characteristic | Itraconazole | Posaconazole |
|
|---|---|---|---|
| Male sex, no. (%) | 96 (71.6) | 76 (77.6) | .36 |
| Race, no. (%) | .11 | ||
| White | 73 (54.5) | 54 (55.1) | |
| Black or African American | 11 (8.2) | 12 (12.2) | |
| Asian | 20 (14.9) | 14 (14.3) | |
| Native Hawaiian or Other Pacific Islander | 8 (6.0) | 0 (0) | |
| Unknown/Other | 22 (16.4) | 18 (18.4) | |
| Ethnicity, no. (%) | 1 | ||
| Hispanic/Latino | 25 (18.7) | 18 (18.4) | |
| Non-Hispanic or Latino | 109 (81.3) | 80 (81.6) | |
| BMI (kg/m2), median (IQR) | 27.2 (24.3–31.0) | 27.3 (23.9–30.8) | .95 |
| Antithymocyte globulin use, no. (%) | 119 (88.8) | 57 (58.2) | <.001 |
| Transplant type, no (%) | .045 | ||
| Heart | 116(86.6) | 93 (94.9) | |
| Heart-kidney | 18 (13.4) | 5 (5.1) | |
| Primary transplant diagnosis | .75 | ||
| Congenital heart disease | 6 (4.5) | 5 (5.1) | |
| Dilated cardiomyopathy | 71 (53.0) | 46 (46.9) | |
| Ischemic cardiomyopathy | 31 (23.1) | 23 (23.5) | |
| Other | 26 (19.4) | 24 (24.5) | |
| Initial drug level therapeutic, no. (%) | 21 (15.7) | 80 (81.6) | <.001 |
| Outcomes | Itraconazole | Posaconazole |
|
|---|---|---|---|
| Primary safety outcome | |||
| AST > 200 IU/mL, no. (%) | 14 (10.4) | 6 (6.1) | .25 |
| ALT > 200 IU/mL, no. (%) | 16 (11.9) | 8 (8.2) | .35 |
| Secondary safety outcome | |||
| AST > 150 IU/mL, no. (%) | 22 (16.4) | 10 (10.2) | .18 |
| ALT > 150 IU/mL, no. (%) | 21 (15.7) | 11 (11.2) | .33 |
| Early discontinuation of antifungal prophylaxis, no. (%) | .68 | ||
| Total | 16 (11.9) | 10 (9.6) | |
| Elevated LFTs | 5 (3.7) | 3 (3.1) | |
| Cost | 1 (0.7) | 1 (1.0) | |
| Clinical condition | 3 (2.2) | 2 (2.0) | |
| Formulation | 0 (0) | 1 (1.0) | |
| Drug interaction | 2 (1.5) | 1 (1.0) | |
| Alternative infection | 1 (0.7) | 0 (0) | |
| Unknown/other | 4 (2.9) | 1 (1.0) | |
| Converted to alternative antifungal agent, no. (%) | |||
| Total | 28 (20.9) | 10 (10.2) | .03 |
| Adverse effect | 4 (2.9) | 0 (0) | |
| Subtherapeutic antifungal levels | 12 (9.0) | 0 (0) | |
| Concern for Infection | 8 (6.0) | 0 (0) | |
| Insurance cost/access/adherence | 3 (2.2) | 3 (3.1) | |
| Drug shortage | 0 (0) | 2 (2.0) | |
| Formulation | 1 (0.7) | 4 (4.1) | |
| Drug interaction | 1 (0.7) | 0 (0) | |
| Unknown/other | 1 (0.7) | 1 (1.0) | |
| QTc prolongation within 2 wks after antifungal initiation, no. (%) | 16 (11.9) | 6 (6.1) | .14 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Renal Transplantation Outcomes and Treatments
Heart transplant (HT) recipients are at increased risk of infection due to receiving immunosuppressive therapy to reduce the risk of allograft rejection [1, 2]. Aspergillosis is the most common invasive mold infection in solid-organ transplant recipients, with incidence ranging from 1.7% to 14% (average 6%) and the mortality attributed to aspergillosis is up to 67% in HT recipients. The American Society of Transplantation recommends targeted Aspergillus prophylaxis with itraconazole, voriconazole, or echinocandin in patients with additional risk factors, such as thoracic reoperation, cytomegalovirus disease, and posttransplant hemodialysis [1, 3].
Posaconazole has been shown to be noninferior to voriconazole for the treatment of invasive aspergillosis and has been used by some transplant centers as prophylaxis in patients after solid-organ transplant [4].
Itraconazole and posaconazole are both associated with hepatotoxicity [5, 6], but in studies comparing itraconazole and posaconazole as antifungal prophylaxis following allogeneic hematopoietic stem cell transplant, there was no significant difference in the percentage of potential drug-related adverse events between the 2 broad-spectrum triazole agents [7, 8]. Beyond Mucorales, posaconazole shows broader and more potent activity than itraconazole against Candida spp. (generally 2–4 fold lower minimum inhibitory concentration, including improved activity against Candida glabrata) and Cryptococcus neoformans [9]. Moreover, posaconazole has comparable or slightly superior activity against Aspergillus spp., with retained activity against some itraconazole-resistant A fumigatus isolates and modestly better activity against select non-Aspergillus molds such as Scedosporium and some Fusarium spp [10, 11]. However, a recent study comparing these 2 antifungal agents as systemic prophylaxis in critically ill lung transplant recipients found fewer fungal infections in patients on posaconazole compared to those on itraconazole [12].
Although previous studies have investigated antifungal prophylaxis in hematopoietic stem cell and lung transplant recipients, there are limited comparative data on the safety and efficacy of itraconazole and posaconazole as antifungal prophylaxis after HT. Historically, our center experienced an increase in non-Candida fungal infections, which resulted in addition of systemic antifungal therapy being given to our heart transplant recipients. Given the change in our center's postoperative HT Aspergillus prophylaxis protocol from itraconazole to posaconazole, we aimed to compare the relative safety and efficacy of these 2 agents after heart transplantation. The protocol change was implemented to improve patient quality of life (due to difficult administration of itraconazole solution), expanded availability of oral anticoagulant options in patients with kidney dysfunction when treated with posaconazole, and the reduced cost of generic formulations of posaconazole [13].
MATERIALS AND METHODS
This was a single-center, retrospective cohort study at Stanford Health Care comparing itraconazole and posaconazole for the prevention of invasive fungal infections in HT recipients from January 2015 through May 2022. Patients were followed for 12 months posttransplant. Data were manually collected through chart review from the electronic medical record. The antifungal per protocol was itraconazole from 2015 through 2019, and posaconazole from 2020 forward. However, patients were not excluded if they received itraconazole or posaconazole outside of their protocol cohort. The Stanford Institutional Review Board approved the study. Patients at least 18 years of age were eligible if they were initiated on itraconazole or posaconazole posttransplant for Aspergillus prophylaxis. Patients were excluded if they received a combined heart-lung or heart-liver transplant, transitioned to another institution within the first year posttransplant, expired within 7 days of heart transplant, or were initiated on an alternative antifungal agent posttransplant.
At our institution, patients receive three months of antifungal prophylaxis with a triazole antifungal agent, as well as inhaled amphotericin b as adjunctive mold prophylaxis during their index hospitalization. Patients initiated on posaconazole received 300 mg daily, and those initiated on itraconazole received 200 mg daily in the morning and 100 mg in the evening, along with nystatin oral suspension. Use of posaconazole oral solution and itraconazole oral tablet formulations was avoided because of poor and variable bioavailability. Therapeutic drug levels for prophylaxis were defined as greater than 0.7 mcg/mL for posaconazole and greater than 0.5 mcg/mL for itraconazole [14, 15].
The primary efficacy outcome was the incidence of fungal infections posttransplant, defined by the 2020 consensus definitions of invasive fungal disease by the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium [16]. Proven, probable, and possible invasive fungal infections were included. Infection-free survival through the first year after initiation of antifungal prophylaxis was evaluated as an additional efficacy outcome. The primary safety outcome was incidence of hepatic injury, defined as elevations in liver transaminases greater than 200 IU/mL (about 5 times the upper limit of normal) [17]. Secondary outcomes included elevations in liver transaminases above 150 IU/mL (about 3 times the upper limit of normal), incidence of prolonged corrected QT interval (QTc) greater than 500 ms within 2 weeks and 3 months after initiation of the antifungal agent, percentage of switch in antifungal prophylaxis agents, percentage of discontinuation of antifungal prophylaxis earlier than the planned 3-month course, median duration of antifungal prophylaxis, and the median time to therapeutic antifungal serum drug levels. Laboratory tests including aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, and total bilirubin were evaluated at baseline (before antifungal agent initiation), 14 ± 3 days after antifungal agent initiation, and at the maximum value within the first 14 ± 3 days after antifungal agent initiation. Concomitant medications commonly associated with drug-induced liver injury administered within 2 weeks of antifungal agent initiation were recorded and included: amoxicillin-clavulanate, disulfiram, diclofenac, carbamazepine, ibuprofen, erythromycin, HMG CoA reductase inhibitors, and anabolic steroids. Additionally, concomitant medications commonly known to prolong the QTc interval administered within 2 weeks of antifungal agent initiation were recorded and included: ondansetron, fluoroquinolone and macrolide antibiotics, amiodarone, methadone, sumatriptan, metoclopramide, sotalol, dofetilide, antipsychotics, and antidepressants [18, 19].
Chi-squared and Fisher exact tests were used to analyze categorical data, and the t-test was used to evaluate continuous data. The level of significance (alpha) was set at 0.05. Descriptive data were reported as medians with interquartile ranges. We used the Kaplan-Meier method to evaluate infection-free survival within the first year after initiation of antifungal prophylaxis and time to discontinuation of antifungal prophylaxis. Data were collected using the online REDCap data management tool [20, 21]. Statistical analysis was performed using R studio version 4.3.3.
RESULTS
A total of 472 patients were screened for inclusion into this study. After excluding 14 patients who received a heart-liver transplant, 213 patients who transitioned care to another institution, and 13 patients who received an alternative or no antifungal prophylaxis agent, 232 patients were included in the analysis, of whom 134 received itraconazole and 98 patients received posaconazole. Table 1 shows baseline patient characteristics. Patients receiving itraconazole were significantly more likely to have been induced with antithymocyte globulin (ATG) than patients receiving posaconazole (88.8% vs 58.2%, P < .001), and there was a significantly higher percentage of heart-kidney transplants in patients receiving itraconazole compared to those receiving posaconazole (13.4% vs 5.1%, P = .045). Otherwise, baseline characteristics were similar. The median age was 55 years (interquartile range, 46–61) in patients receiving itraconazole and 46 years (interquartile range, 47–62) in patients receiving posaconazole, and majority of patients were male, 71.6% and 77.6% in patients receiving itraconazole and posaconazole, respectively. The most frequent underlying disease leading to heart transplantation was dilated cardiomyopathy.
A total of 8 (6%) breakthrough fungal infections were observed in the itraconazole cohort compared to 0 (0%) infections in the posaconazole cohort (Supplementary Table 1). Patients receiving itraconazole were significantly more likely to develop a fungal infection within a year after transplant (P & .014) (Figure 1). Of the 8 observed breakthrough infections, 7 patients received induction with antithymocyte globulin (88%). Two additional late fungal infections occurred 292 and 334 days after transplant, both in the itraconazole group. In a Firth penalized logistic regression adjusting for triazole therapy, race, induction therapy, and transplant type, posaconazole prophylaxis was independently associated with significantly lower odds of 1-year fungal infection (odds ratio, 0.08; 95% confidence interval, ∼0.001–0.72; P = .019). No other covariates demonstrated statistically significant associations.
Fungal infection-free survival within 1 year after transplant.
There was no significant difference observed in elevations in ALT > 200 IU/mL (P & 1.0) or AST > 200 IU/mL (P & .135) 2 weeks after antifungal initiation between patients receiving itraconazole and posaconazole (Table 2). Similarly, incidence of elevations in ALT > 150 IU/mL (P = 1.0) or in AST > 150 IU/mL (P = .4703) was similar between the cohorts 2 weeks after antifungal initiation. Itraconazole was associated with significantly higher rates of switching antifungal prophylaxis agents in comparison to posaconazole (P = .03), most commonly because of subtherapeutic antifungal levels (9%), concern for infection (6%), and adverse effects (2.9%). There was no observed statistical difference in the early discontinuation of antifungal prophylaxis before 3 months from adverse effects (P > .05).
A higher percentage of posaconazole drug levels were therapeutic at initial check compared to itraconazole drug levels (81.6% vs 52.6%, P < .001). Twenty patients receiving itraconazole (14.9%) and 14 patients receiving posaconazole (14.3%) had no therapeutic antifungal drug levels obtained.
DISCUSSION
To the best of our knowledge, this single-center, retrospective cohort study comparing the efficacy and safety of itraconazole and posaconazole for Aspergillus prophylaxis is the first investigation of these agents used after heart transplantation. Our study demonstrated posaconazole to be significantly more effective in the prevention of fungal infection after HT in comparison to itraconazole. These results are similar to previous findings from a study comparing posaconazole and itraconazole for antifungal prophylaxis in lung transplant recipients [9]. Additionally, significantly more patients receiving itraconazole switched to an alternative antifungal agent than those receiving posaconazole because of concern for infection.
Significantly more patients receiving itraconazole prophylaxis received ATG induction compared to patients receiving posaconazole prophylaxis. This could be a confounding factor because ATG can increase patient's risk of infection. One randomized trial analyzing data from the United Kingdom Cardiothoracic Transplant Audit including 1143 heart transplant recipients induced with ATG reported 18% higher number of infection episodes of any type, in the first year after transplant in the ATG group compared to those who did not receive ATG, and this difference was statistically significant [22].
Among patients receiving itraconazole who developed infectious complications, only 2 breakthrough infections were caused by Aspergillus. Itraconazole and posaconazole are both active against Aspergillus, though posaconazole provides additional benefit with added activity against non-Aspergillus species, including mucoromycetes [5, 6].
Similar to findings in previous studies comparing itraconazole and posaconazole in hematopoietic stem cell transplantation [7], our results demonstrate no significant difference in safety outcomes of these 2 antifungal agents, including drug-drug interactions with transplant medications [23].
The various formulations of posaconazole and itraconazole demonstrate differences in drug absorption, and our center preferentially uses posaconazole oral tablets and itraconazole oral solution. Original oral itraconazole formulations are 55% bioavailable, and itraconazole oral solution is associated with greater exposure in comparison to itraconazole oral capsules. However, high interpatient variability in itraconazole exposure is observed for these formulations and can be affected by concomitant food administration and stomach acidity [5]. Oral formulations of posaconazole include an oral solution and delayed-release tablets. Posaconazole delayed-release tablets are more bioavailable and are less affected by stomach acidity and gut motility in comparison to the solution formulation. Similar to the itraconazole formulations, the posaconazole formulations demonstrate high interpatient variability [6, 24]. Our study showed a higher percentage of posaconazole drug levels were therapeutic compared to itraconazole drug levels and a significantly shorter time to therapeutic drug levels was achieved with posaconazole compared to itraconazole. These differences in therapeutic antifungal levels may also contribute to the higher incidence of fungal infections in patients receiving itraconazole. In our study, liquid formulation was used for all patients, and counseling to take on an empty stomach was provided around the time of transplant. We believe part of the associated lower rates of fungal infections in the posaconazole cohort is likely due to patients being therapeutic for a greater amount of time with improved pharmacokinetics of posaconazole.
Recently a new formulation of itraconazole has become available in the United States with improved bioavailability, and may result in improved efficacy, but as a generic formulation is not available, this therapy may be cost prohibitive for many patients.
Our study has several limitations. External validity of results is limited by the single-center design of this study and relatively small sample size. Additionally, bias related to unobserved confounders cannot be excluded due to the retrospective study design. Last, although this study attempted to account for confounding concurrent medications that can cause similar adverse effects to those caused by itraconazole and posaconazole, including medications that can cause hepatic injury and prolong QTc intervals, the lists of these medications were not exhaustive.
CONCLUSION
The use of posaconazole as antifungal prophylaxis for heart transplant recipients within the first three months of transplantation was associated with significantly improved fungal infection-free survival at 1 year posttransplant and fewer fungal breakthrough infections compared to itraconazole solution. Itraconazole and posaconazole demonstrated comparable safety for this indication.
Supplementary Material
ofag104_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Husain S, Camargo JF. Invasive aspergillosis in solid-organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 2019; 33:e 13544.30900296 10.1111/ctr.13544 · doi ↗ · pubmed ↗
- 2Shields RK, Nguyen MH, Shullo MA, et al Invasive aspergillosis among heart transplant recipients is rare but causes rapid death due to septic shock and multiple organ dysfunction syndrome. Scand J Infect Dis 2012; 44:982–6.22830948 10.3109/00365548.2012.705018 PMC 3686283 · doi ↗ · pubmed ↗
- 3Singh N, Paterson DL. Aspergillus infections in transplant recipients. Clin Microbiol Rev 2005; 18:44–69.15653818 10.1128/CMR.18.1.44-69.2005 PMC 544171 · doi ↗ · pubmed ↗
- 4Maertens JA, Rahav G, Lee DG, et al Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: a phase 3, randomised, controlled, non-inferiority trial. Lancet 2021; 397:499–509.33549194 10.1016/S 0140-6736(21)00219-1 · doi ↗ · pubmed ↗
- 5Itraconazole [Package Insert]. Research Triangle Park, NC: Stiefel Laboratories, Inc.; 2010.
- 6Posaconazole [Package Insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2014.
- 7Sánchez-Ortega I, Patiño B, Arnan M, et al Clinical efficacy and safety of primary antifungal prophylaxis with posaconazole vs itraconazole in allogeneic blood and marrow transplantation. Bone Marrow Transplant 2011; 46:733–9.20697369 10.1038/bmt.2010.185 · doi ↗ · pubmed ↗
- 8Döring M, Blume O, Haufe S, et al Comparison of itraconazole, voriconazole, and posaconazole as oral antifungal prophylaxis in pediatric patients following allogeneic hematopoietic stem cell transplantation. Eur J Clin Microbiol Infect Dis 2014; 33:629–38.24173819 10.1007/s 10096-013-1998-2PMC 3953550 · doi ↗ · pubmed ↗