Clinical Characteristics, Management and Outcomes of Nonintensive Care Unit Candidemia: Subanalysis of the ECMM Candida III Multinational European Observational Cohort Study
Stella Wolfgruber, Carolina Garcia-Vidal, Sarah Sedik, Jon Salmanton-García, Sevtap Arikan-Akdagli, Jean-Pierre Gangneux, Riina Rautemaa-Richardson, Valentina Arsić-Arsenijević, Sonia Martín-Pérez, Julio Dávila-Valls, Nurettin Erben, Emin Halis Akalin, Lubos Drgona

TL;DR
A study of candidemia cases outside the ICU found higher survival rates despite more comorbidities, with certain factors linked to better outcomes.
Contribution
The study provides new insights into candidemia management and outcomes in non-ICU settings across Europe.
Findings
Non-ICU candidemia patients had higher survival rates despite higher comorbidity burdens.
Older age and hematological malignancies were associated with increased mortality risk.
Infectious disease consultation and echinocandin therapy improved survival outcomes.
Abstract
The European Confederation of Medical Mycology Candida III was a pan-European, multicenter observational study of adult patients with blood culture–proven candidemia. Among a total of 632 patients with candidemia across 64 institutions in 20 European countries, a subanalysis of 396 (63%) cases occurring outside the intensive care unit (ICU) was conducted. Compared with ICU patients, non-ICU patients had a higher comorbidity burden (median Charlson comorbidity index [CCI] 6 vs 5 in ICU patients, P = .006). Hematologic and oncologic malignancies were more frequent among non-ICU cases (45.5% vs 28.4%, P < .001), whereas both chronic kidney and cardiovascular disease were more prevalent in ICU patients (P < .001). Non-ICU patients had significantly lower mortality in Kaplan–Meier survival analysis (P > .001). Postsurgical non-ICU patients (n = 45) had the highest survival rate (73.3%, P =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
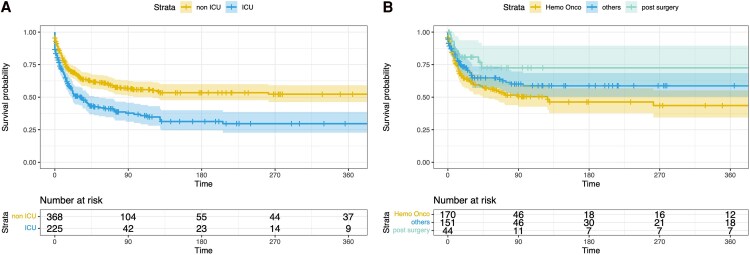 Figure 1
Figure 1| Study Cohort (n = 632) | Non-ICU (n = 396) | ICU (n = 236) |
| |
|---|---|---|---|---|
| Sex | .505 | |||
| Male | 369 (58.4%) | 227 (57.3%) | 142 (60.2%) | |
| Female | 263 (41.6%) | 169 (42.7%) | 94 (39.8%) | |
| Age at candidemia diagnosis | .400 | |||
| 18–29 y | 17 (2.7%) | 13 (3.3%) | 4 (1.7%) | |
| 30–49 y | 101 (16.0%) | 65 (16.4%) | 36 (15.3%) | |
| 50–69 y | 299 (47.3%) | 180 (45.5%) | 119 (50.4%) | |
| 70–89 y | 197 (31,2%) | 124 (31.3%) | 73 (30.9%) | |
| >90 y | 18 (2.8%) | 14 (3.5%) | 4 (1.7%) | |
| Underlying diseases | ||||
| Hemato-oncologic malignancy | 248 | 181 (45.7%) | 67 (28.4%) | <.001 |
| Chronic cardiovascular disease | 149 | 58 (14.6%) | 91 (38.6%) | <.001 |
| Chronic liver disease | 60 | 35 (8.6%) | 25 (11.0%) | .466 |
| Chronic pulmonary disease | 62 | 32 (8.1%) | 30 (12.7%) | .072 |
| Acute or chronic renal disease | 137 | 64 (16.2%) | 73 (30.9%) | <.001 |
| Diabetes mellitus | 139 | 72 (18.2%) | 67 (28.4%) | .002 |
| Rheumatoid disease/autoimmune disorder | 32 | 14 (3.5%) | 18 (7.6%) | .037 |
| HIV/AIDS | 10 | 7 (1.8%) | 3 (1.3%) | .751 |
| COVID-19 | 26 | 1 (0.3%) | 25 (10.6%) | <.001 |
| Risk factors for candidemia | ||||
| Solid organ transplantation | 15 | 8 (2.3%) | 7 (2.5%) | .450 |
| Other disorders requiring or causing immunosuppression | 27 | 16 (4.0%) | 11 (4.7%) | .690 |
| Charlson comorbidity index, median (IQR) | 5 (3–8) | 6 (3–8) | 5 (3–7) | .006 |
| Major surgery (not including surgery as antifungal therapy) | 165 | 77 (19.4%) | 88 (37.3%) | <.001 |
| Other risk factors (eg, prosthetic material, prosthetic valve/foreign body) | 78 | 45 (11.4%) | 33 (14.0%) | .382 |
| Trauma | 24 | 12 (3.0%) | 12 (5.1%) | .202 |
| Alcoholism | 44 | 27 (6.8%) | 17 (7.2%) | .872 |
| Burn | 6 | 2 (0.5%) | 4 (1.7%) | .203 |
| IV drug abuse | 16 | 12 (3.0%) | 4 (1.7%) | .434 |
| Low albumin level | 251 | 123 (31.1%) | 128 (54.2%) | <.001 |
| Obesity (BMI > 30) | 69 | 27 (6.8%) | 42 (17.8%) | <.001 |
| Underweight (BMI < 18.5) | 33 | 28 (6.6%) | 5 (2.1%) | .009 |
| CVC | 399 | 192 (48.5%) | 207 (87.7%) | <.001 |
| Positive Ostrosky-Zeichner score | 224 | NA | 30/224 (13.4%) | NA |
| Study Cohort (n = 632) | Non-ICU (n = 396) | ICU (n = 236) |
| |
|---|---|---|---|---|
| Consultation | ||||
| Infectious diseases consultation | 317 | 203 (51.3%) | 114 (48.3%) | .511 |
| Microbiology consultation | 185 | 115 (29.0%) | 70 (29.7%) | .928 |
| No consultation | 118 | 76 (19.2%) | 42 (17.8%) | .752 |
| Diagnostics | ||||
| Initial blood cultures (≥40 mL) | 557 | 346 (87.4%) | 211 (89.4%) | .525 |
| Species identification | 570 | 352 (88.9%) | 218 (92.4%) | .169 |
| Susceptibility testing | 520 | 333 (84.1%) | 187 (79.2%) | .197 |
| Echocardiography | 267 | 174 (43.9%) | 93 (39.4%) | .280 |
| Ophthalmoscopy | 219 | 162 (40.9%) | 57 (24.2%) | <.001 |
| Management | ||||
| Initial echinocandin treatment | 353 | 213 (53.8%) | 140 (59.3%) | .186 |
| Stepdown to fluconazole | 186 | 133 (33.6%) | 53 (22.5%) | .003 |
| Treatment for ≥14 d after the first negative blood culture | 325 | 208 (52.5%) | 117 (49.6%) | .511 |
| CVC removal ≤24 h from diagnosis | 216 | 112/192 (58.3%) | 104/207 (50.2%) | .109 |
| CVC removal >24 but <72 h from diagnosis | 82 | 49/80 (61.3%) | 33/103 (32.0%) | <.001 |
| EQUAL | 0.68 (0.50–0.84) | 0.68 (0.50–0.86) | 0.68 (0.49–0.82) | .187 |
| Outcome | ||||
| Total duration of hospitalization after day 0, days, median (IQR) | 15 (4–30) | 15 (5–30) | 15 (2–33) | .987 |
| Total duration of hospitalization for survivors at day 30, median (IQR) | 21 (10–43) | 21 (10–35) | 27 (14–49) | .016 |
| Ocular involvement | 19 | 13 (3.3%) | 6 (2.5%) | .397 |
| Cardiac involvement | 25 | 15 (3.8%) | 10 (4.2%) | .664 |
| Mortality | ||||
| 14-d mortality | 166/556 | 93/342 (27.2%) | 73/214 (34.1%) | .083 |
| 30-d mortality | 212/498 | 119/304 (39.1%) | 93/194 (47.9%) | .053 |
| 90-d mortality | 251/415 | 140/246 (56.9%) | 111/169 (65.7%) | .072 |
| 180-d mortality | 261/354 | 144/198 (72.7%) | 117/156 (75%) | .629 |
| Patient alive at last follow-up | 331 | 233/386 (60.4%) | 98/230 (42.6%) | <.001 |
|
| ||||
| | 287 | 175 (44.2%) | 112 (47.5%) | .458 |
| | 133 | 87 (22.0%) | 46 (19.5%) | .482 |
| | 83 | 52 (13.1%) | 31 (13.1%) | 1.000 |
| | 46 | 33 (8.3%) | 13 (5.5%) | .208 |
| | 16 | 14 (3.5%) | 2 (0.8%) | .038 |
| | 15 | 1 (0.3%) | 14 (5.9%) | <.001 |
| | 10 | 4 (1.0%) | 6 (2.5%) | .187 |
| | 6 | 6 (1.5%) | 0 | .089 |
| | 5 | 3 (0.8%) | 2 (0.8%) | 1.000 |
| | 6 | 0 | 6 (2.5%) | .003 |
| Others | 13 | 12 (3.0%) | 1 (0.4%) | .061 |
| Non-ICU Cohort (n = 396) | Hemato-oncologic Malignancies (n = 181) | Post Major Surgery (n = 45) | Others (n = 170) |
| |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 227 | 100 (55.2%) | 22 (48.9%) | 105 (51.1%) | .223 |
| Female | 167 | 81 (44.8%) | 23 (51.1%) | 65 (38.2%) | |
| Causative species | |||||
| | 173 | 80 (44.2%) | 14 (31.1%) | 79 (46.5%) | .178 |
| | 85 | 36 (19.9%) | 12 (26.7%) | 37 (21.8%) | .607 |
| | 51 | 21 (11.6%) | 6 (13.3%) | 24 (14.1%) | .777 |
| | 33 | 21 (11.6%) | 2 (4.4%) | 10 (5.9%) | .093 |
| | 1 | 0 | 1 (2.2%) | 0 | - |
| | 14 | 9 (5.0%) | 0 | 5 (2.9%) | .232 |
| | 4 | 1 (0.6%) | 1 (2.2%) | 2 (1.2%) | .581 |
| | 6 | 2 (1.3%) | 1 (1.3%) | 3 (1.8%) | .940 |
| | 3 | 2 (1.1%) | 0 | 1 (0.6%) | .705 |
| Risk factors | |||||
| Central venous catheter | 192 | 104 (57.5%) | 24 (53.3%) | 64 (37.6%) | <.001 |
| Low albumin level | 124 | 67 (37.0%) | 10 (22.2%) | 47 (27.6%) | .063 |
| Obesity (BMI > 30) | 27 | 15 (12.3%) | 2 (11.8%) | 10 (12.7%) | .994 |
| Underweight (BMI < 18.5) | 28 | 18 (14.9%) | 1 (5.9%) | 9 (11.4%) | .516 |
| Diabetes mellitus | 72 | 26 (14.4%) | 9 (20.0%) | 37 (21.8%) | .188 |
| Chronic liver disease | 35 | 7 (3.9%) | 5 (11.1%) | 23 (13.5%) | .005 |
| Solid organ transplantation | 8 | 0 | 1 (2.2%) | 7 (4.1%) | .23 |
| Charlson comorbidity index | 6 (3–8) | 6 (4–9) | 5 (3–8) | 5 (3–8) | .041 |
| Consultation | |||||
| Infectious diseases consultant | 203 | 99 (54.7%) | 23 (51.1%) | 81 (47.6%) | .870 |
| Microbiology consultant | 115 | 39 (21.5%) | 14 (31.1%) | 62 (36.5%) | .820 |
| No consultation | 76 | 42 (23.3%) | 8 (17.8%) | 26 (15.3%) | .835 |
| Diagnostics | |||||
| Initial blood cultures (40 mL) | 346 | 171 (94.5%) | 32 (71.1%) | 143 (84.1%) | <.001 |
| Species identification | 352 | 170 (93.9%) | 35 (77.8%) | 147 (86.5%) | .004 |
| Susceptibility testing | 333 | 163 (90.1%) | 33 (73.3%) | 137 (80.6%) | .006 |
| Echocardiography | 174 | 75 (41.4%) | 17 (37.8%) | 82 (48.2%) | .297 |
| Ophthalmoscopy | 162 | 70 (38.7%) | 20 (44.4%) | 72 (42.4%) | .686 |
| Management | |||||
| Initial echinocandin treatment | 213 | 100 (55.2%) | 19 (42.2%) | 94 (55.3%) | .255 |
| Stepdown to fluconazole | 133 | 64 (35.4%) | 12 (26.7%) | 57 (33.5%) | .543 |
| Treatment for ≥14 d after the first negative blood culture | 208 | 89 (49.2%) | 23 (51.1%) | 96 (56.5%) | .384 |
| CVC removal ≤24 h from diagnosis | 112 | 53/104 (51.0%) | 18/24 (75.0%) | 41/64 (64.1%) | .101 |
| CVC removal >24 <72 h from diagnosis | 49 | 26/51 (51.0%) | 5/6 (83.3%) | 18/23 (78.3%) | .541 |
| EQUAL | 0.68 (0.50–0.86) | 0.68 (0.50–0.84) | 0.64 (0.29–0.86) | 0.73 (0.45–0.86) | .635 |
| Outcome | |||||
| Total duration of Hospitalization after day 0, days, median (IQR) | 15 (5–30) | 13 (5–29) | 17 (9–45) | 15 (2–27) | .035 |
| Total duration of hospitalization for survivors at day 30, median (IQR) | 21 (10–35) | 21 (10–36) | 32 (14–53) | 20 (7–31) | .037 |
| Ocular involvement | 13 | 8 (14.0%) | 1 (6.3%) | 4 (7.3%) | .426 |
| Cardiac involvement | 15 | 5 (8.1%) | 1 (7.1%) | 9 (13.2%) | .575 |
| Mortality | |||||
| 14-d mortality | 93 | 49/158 (31%) | 8/41 (19.5%) | 36/143 (25.2%) | .262 |
| 30-d mortality | 119 | 62/147 (42.2%) | 8/34 (23.5%) | 49/123 (39.8%) | .131 |
| 90-d mortality | 140 | 75/122 (61.5%) | 10/23 (43.5%) | 55/101 (54.5%) | .226 |
| 180-d mortality | 144 | 78/96 (81.3%) | 10/17 (58.8%) | 56/85 (65.9%) | .028 |
| Patient alive at last follow-up | 233/383 | 98/179 (54.7%) | 33/45 (73.3%) | 102/159 (64.2%) | .003 |
| Univariable HR (95% CI) |
| |
|---|---|---|
| Sex (male vs female) | 0.81 (0.58–1.12) | .196 |
| Age at candidemia diagnosis (per year) | 1.02 (1.01–1.03) | <.001 |
| Underlying diseases | ||
| Hemato-oncologic malignancies | 1.45 (1.05–2.00) | .025 |
| Rheumatic disease/autoimmune disorder | 1.51 (0.74–3.08) | .259 |
| Chronic cardiovascular disease | 1.12 (0.73–1.74) | .599 |
| Chronic liver disease | 1.85 (1.14–3.00) | .013 |
| Solid organ transplantation | 0.47 (0.12–1.88) | .283 |
| Acute or chronic renal disease | 1.10 (0.72–1.68) | .668 |
| Diabetes mellitus | 0.72 (0.46–1.12) | .147 |
| COVID-19 | 6.03 (0.81–45.05) | .169 |
| Risk factors for candidemia | ||
| Charlson comorbidity index | 1.11 (1.06–1.16) | <.001 |
| Major surgery (not including surgery as antifungal therapy) | 0.60 (0.38–0.95) | .029 |
| Trauma | 1.45 (0.68–3.10) | 0.365 |
| Alcoholism | 1.50 (0.85–2.65) | .189 |
| Low albumin level | 1.27 (0.91–1.77) | .172 |
| Central venous catheter | 1.11 (0.80–1.53) | .539 |
| Diagnostics and management | ||
| EQUAL | 0.14 (0.08–0.23) | <.001 |
| Initial blood cultures (>40 mL) | 0.71 (0.44–1.17) | .197 |
| Echocardiography performed | 0.39 (0.27–0.55) | <.001 |
| Ophthalmoscopy performed | 0.31 (0.22–0.45) | <.001 |
| Start with an echinocandin | 0.53 (0.38–0.73) | <.001 |
| Stepdown to fluconazole | 0.38 (0.26–0.57) | <.001 |
| Treatment consultation by an infectious diseases or microbiology consultant | 0.49 (0.34–0.71) | <.001 |
| Model 1 | Multivariable adjusted HR (95% CI) |
|
| Treatment consultation by an infectious diseases or microbiology consultant | 0.38 (0.21–0.69) | .001 |
| Chronic liver disease | 3.47 (1.51–7.98) | .003 |
| Age (per year) | 1.02 (1.00–1.04) | .032 |
| EQUAL | 0.06 (0.02–0.21) | <.001 |
| COVID-19 | 13.33 (1.62–109.81) | .016 |
| Hemato-oncologic malignancies | 2.21 (1.18–4.15) | .014 |
| Model 2 | ||
| Treatment consultation by an infectious diseases or microbiology consultant | 0.32 (0.18–0.56) | <.001 |
| Chronic liver disease | 3.39 (1.48–7.80) | .004 |
| Age (per year) | 1.03 (1.01–1.04) | .005 |
| Initial echinocandin treatment | 0.45 (0.25–0.80) | .007 |
| COVID-19 | 14.22 (1.71–118.06) | .014 |
| Hemato-oncologic malignancies | 2.01 (1.10–3.68) | .024 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Bacterial Identification and Susceptibility Testing · Neutropenia and Cancer Infections
Invasive candidiasis (IC) and candidemia remain the most common invasive fungal diseases in many parts of the world [1–3]. Candidemia accounts for ∼626 000 cases worldwide each year and is associated with high morbidity and mortality [4, 5]. In Europe, the all-cause 90-day mortality rate among adults with candidemia remains above 40% [6].
Candida albicans remains the most frequently isolated species in cases of candidemia and IC. However, over the past decades, there has been a global shift toward non-albicans Candida species, such as Nakaseomyces glabratus (formerly known as Candida glabrata), Candida tropicalis, Candida parapsilosis, as well as the emerging multidrug-resistant Candida auris (also referred to as Candidozyma auris) [5, 7–9]. Across Europe, significant differences in species distribution are observed. In Northern Europe, C. glabrata was the second most common isolated species, whereas C. parapsilosis was less common. In contrast, in Southern and Mediterranean countries (eg, Italy, Spain, and Greece), C. parapsilosis and, in some countries, C. auris have been predominant among non-albicans Candida spp., while C. glabrata was less frequent [10]. Species distribution and antifungal resistance patterns also differ between ICU and non-ICU settings, supporting separate subgroup analysis by care setting [11].
Over the past 25 years, the European Confederation of Medical Mycology (ECMM) has conducted 3 large-scale, multicenter cohort studies (ECMM Candida I, II, and III) to investigate the epidemiology, risk factors, and outcomes associated with IC in Europe [6, 12, 13].
Throughout these studies, ICU admission has remained one of the most important risk factors for candidemia [2], and ICU-associated candidemia has been the subject of numerous studies in recent decades [14, 15]. In contrast, candidemia occurring outside the ICU has received less attention, with larger investigations focusing on this subgroup being rare [16, 17]. In this subanalysis of the ECMM Candida III study, the primary objective was to compare the clinical characteristics, management, and outcomes of candidemia in non-ICU versus ICU settings. As a secondary objective, we aimed to explore heterogeneity within the non-ICU population by stratifying patients into 3 subgroups: patients with hematologic or oncologic malignancies, postsurgical patients, and other non-ICU patients not included in the first 2 categories.
METHODS
Study Design
For the ECMM Candida III study, data were collected from 64 institutions across 20 countries in Europe [2, 6–8, 10, 18]. During the study period from 1 July 2018 to 31 March 2022, each participating hospital included the first 10 consecutive adult patients diagnosed with candidemia. Non-ICU patients were defined as those not located in an ICU at the time the first positive blood culture was drawn. Patients transferred to the ICU after the blood culture was drawn were classified according to their location at the time of first blood culture collection and were not reclassified. Malnutrition was assessed solely based on body mass index (BMI). Underweight was defined as a BMI < 18.5 kg/m^2^, in accordance with standard WHO definitions. Patient data were systematically recorded using an electronic case report form integrated into the ECMM Candida Registry (FungiScope, CandiReg; NCT01731353) [19], resulting in a total cohort of 632 patients. The EQUAL Candida score, developed by the ECMM in 2018, was used to evaluate the quality of candidemia management and measure adherence to key diagnostic and therapeutic recommendations from the 2 major American and European clinical guidelines [6, 20, 21]. Scores were normalized according to the presence or absence of a central venous catheter (CVC). The Ostrosky-Zeichner score was calculated as follows: a patient was considered positive if any systemic antibacterial agent was administered or a CVC was present and at least 2 of the following factors were present: total parenteral nutrition, dialysis, major surgery, use of steroids, or use of other immunosuppressive agents [22]. The study complied with the Declaration of Helsinki. The University of Cologne (EK 17-485) granted central ethical approval, in addition, local confirmation or approval was required in accordance with local regulations.
This subanalysis used the full dataset from the parent study [6], focusing specifically on patients treated outside the ICU. We investigated risk factors, underlying diseases, causative species, treatment, and clinical outcomes, comparing the results with those of the ICU population. For this purpose, the complete dataset was filtered to include non-ICU patients only. These cases were then categorized into 3 groups: patients with hematologic malignancies or solid tumors, patients who had undergone major surgery and the remaining patients who could not be categorized into the other groups. Patients in the hemato-oncologic malignancies group included those with a hematologic malignancy or a solid tumor, regardless of whether they had undergone major surgery. Patients who had undergone major surgery but did not have a malignancy were assigned to the postsurgery group. This group included individuals who had abdominal or visceral surgery, urologic, or gynecologic surgery, cardiothoracic, neurosurgical, orthopedic, or trauma surgery, head and neck surgery, wound surgery, as well as major endoscopic or interventional procedures.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, NY) and SAS 9.4 (2002–2016 by SAS Institute Inc., Cary, NC).
Descriptive statistics were used to summarize the data, presenting categorical variables as counts and percentages and continuous variables as median with interquartile range (IQR). Group comparisons for categorical variables were performed using Pearson χ^2^ test with Fisher's exact test applied when the χ^2^ requirements were not met. Continuous variables were compared using the Mann–Whitney U test. For comparisons among the 3 non-ICU subgroups categorical variables were analyzed using the χ^2^ test or Fisher's exact test, while continuous variables were compared using the Kruskal–Wallis test.
The day of diagnosis was defined as the day when the first positive blood culture results for Candida spp. became available to the treating physician. For time-specific mortality analyses at 14, 30, 90, and 180 days from the day of diagnosis, only patients with documented vital status at the respective time point were included. Patients who were alive at the last day of follow-up but had no documented follow-up beyond the respective time points were excluded from the denominator.
For the Cox regression analyses, the patients were followed until they died or had their last documented date of study follow-up. They were censored on the date of their last follow-up if they had not died.
Variables were separately analyzed using univariable Cox proportional hazard models. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. Assumptions for the models were checked, and in case of nonproportional hazards, time-dependent covariates were included in the model. Variables showing a univariate P-value of <.2 were considered for further analysis. Within the set of significant predictors, multicollinearity was analyzed and parameters were excluded if multicollinearity or reverse causation bias was evident. The resulting variables were analyzed using a backwards strategy to obtain a parsimonious model.
A P-value of <.05 was considered statistically significant.
RESULTS
The entire study cohort included 632 patients from 20 European countries (Supplementary Figure 1 and Supplementary Table 1) with blood culture–proven candidemia. Of these patients, 396 (62.7%) were not in the ICU at the time of diagnosis, and there was no missing data regarding ICU admission status.
Table 1 displays patient demographics, underlying diseases, and risk factors for candidemia among non-ICU versus ICU patients. Of 396 patients diagnosed with candidemia outside the ICU, 88 (22.2%) were admitted to the ICU after diagnosis of candidemia. There were no significant differences in sex distribution or age between ICU and non-ICU patients. Hemato-oncologic malignancies were significantly more prevalent in non-ICU patients than in ICU patients (P < .001). Conversely, chronic cardiovascular disease (P < .001), acute or chronic renal disease (P < .001), diabetes mellitus (P = .002), rheumatoid diseases (P = .037), and COVID-19 infection (P < .001) were less prevalent in non-ICU patients. Major surgery was more common among ICU patients compared with non-ICU patients (P < .001). Low serum albumin levels were observed more frequently in ICU patients versus non-ICU patients (P < .001). Obesity (BMI > 30) was more prevalent in ICU patients than in non-ICU patients (P < .001). Underweighted individuals (BMI < 18.5) were more prevalent in the non-ICU cohort (P < .001).
The median Charlson comorbidity index (CCI) was higher in non-ICU patients than in ICU patients (median 6, IQR 3–8 vs median 5, IQR 3–7; P = .006).
Causative Candida species are displayed in Table 2. Species distribution by participating country is provided in Supplementary Table 2. Candida albicans was the predominant causative species isolated in 44.2% of non-ICU patients. This was followed by N. glabratus, identified in 22% of non-ICU patients. No difference was observed between the groups for either species. However, a significant group-specific distribution was observed for Pichia kudriavzevii (formerly known as Candida krusei) which was predominantly isolated in the non-ICU group (3.5% vs 0.8% in ICU patients; P = .038). In patients with P. kudriavzevii candidemia, the 30-day mortality rate was significantly higher in the non-ICU cohort (66.7%) compared with ICU patients (33.3%, P = .035), a finding that was not attributable to inadequate first-line therapy as all patients with fatal outcomes received echinocandins as first-line therapy. Candida auris was significantly more prevalent in the ICU cohort (5.9%) than in non-ICU patients (0.3%; P = <.001). Similarly, Meyerozyma guilliermondii (formerly known as Candida guilliermondii) was only found in the ICU group (2.1%), whereas Clavispora lusitaniae (formerly known as Candida lusitaniae) only in non-ICU patients (1.5%), although the numbers of cases were small and the differences not statistically significant (Table 2).
Details on management and outcomes of candidemia are shown in Table 2. Antifungal susceptibility testing was performed on isolates from 64% of non-ICU patients and 79.2% of ICU patients. Ophthalmoscopy was performed more frequently in non-ICU patients (P < .001). Central venous catheter removal within 24 hours of diagnosis was observed in 58.3% of non-ICU cases that were not admitted to the ICU, compared with 50.2% of ICU patients (P = .109). Delayed CVC removal between 24 and 72 hours after diagnosis was more common in non-ICU patients (61.2% vs 32.0% of those in whom CVC was not removed within 24 hours, P < .001). An echinocandin, as recommended in current guidelines, was used as the initial therapy in 53.8% of non-ICU patients and 59.3% of ICU patients (P = .186). Stepdown to fluconazole occurred significantly more often in the non-ICU group than in the ICU group (33.4% vs 22.8%; P = .005). Among patients who survived ≥14 days after the diagnosis (n = 442), stepdown therapy was performed in 41.0% of non-ICU and 29.2% of ICU patients (P = .017).
The median duration of hospitalization among those who survived at least 30 days after diagnosis (Table 2) was significantly shorter in non-ICU patients versus ICU patients (21 days, IQR 10–35 days vs 27 days, IQR 14–49 days, P = .016).
EQUAL Candida scores, normalized to the maximum possible score (19 for those without CVC and 22 for those with CVC) were comparable between the groups (Table 2). Ostrosky-Zeichner score positivity was met by 13.4% (30/224) of ICU patients.
Mortality tended to be consistently lower in the non-ICU cohort at all time points except day 180 (Table 2). Non-ICU patients also had significantly higher survival rates at the last follow-up compared with ICU patients (60.4% vs 42.6%; P < .001). Kaplan–Meier survival analysis (Figure 1A) confirmed a significantly lower survival probability (P < .001) in the ICU group.
A, Kaplan–Meier survival curve showing the probability of survival of nonintensive care unit (ICU) (yellow) and ICU patients (blue). P < .001. B, Kaplan–Meier survival curve showing the probability of survival in non-ICU patients. Groups: HemOnc malignancy (yellow), post major surgery (green), others (blue). P = .039 (log rank test).
Results of the Cox regression analysis (Supplementary Table 3) showed that treatment in the ICU at the time of candidemia diagnosis was associated with a significantly increased mortality risk in univariable analysis (HR 1.76, 95% CI 1.39–2.23, P < .001), and remained an independent predictor in multivariable analysis (adjusted HR 1.90, 95% CI 1.49–2.41, P < .001), together with higher CCI (adjusted HR 1.10, 95% CI 1.06–1.14, P < .001).
Subanalysis of the Nonintensive Care Unit Cohort
To further analyze the non-ICU cohort (n = 396), patients were stratified into 3 subgroups: patients with hemato-oncologic malignancies (n = 181), those with major surgery (post major surgery, n = 45), and all other patients (others, n = 170; Table 3).
While there was no significant difference in Candida spp. distribution across the 3 subgroups, C. tropicalis tended to be detected more frequently in patients with hemato-oncologic malignancies (P = .093).
Central venous catheter presence was more frequent in the hemato-oncologic malignancies (57.5%) and post major surgery groups (53.3%) compared with others (37.6%; P < .001). The hemato-oncologic malignancy group had a higher CCI (P = .041), while median hospital stay (in those who survived at least 30 days) was longest in the postsurgery group (median 32 days IQR 14–53 days), compared with hemato-oncologic malignancy patients (median 21 days, IQR 10–36 days) and other patients (median 20 days, IQR 7–30 days, P = .037). In a small subgroup of 11 patients (5 hemato-oncologic malignancies, 2 post major surgery, and 4 others), no antifungal therapy was reported, despite survival for at least 2 days after diagnosis. All these patients ultimately died, suggesting a potential palliative treatment setting in this subgroup. Survival rates at the last follow-up were highest in postsurgery patients (73.3%), followed by others (64.2%) and hemato-oncologic malignancy patients (54.7%; P = .003). Thirty-day mortality was 42.2% in the hemato-oncologic malignancy group, 23.5% in the post major surgery group, and 39.8% in the others group (P = .132).
Figure 1 B shows Kaplan–Meier survival curves for the 3 different subgroups of non-ICU patients. Patients with hemato-oncologic malignancies had the lowest survival probability (P = .039).
Univariable Cox regression analysis of non-ICU patients (Table 4) showed that CCI was significantly associated with increased mortality risk (HR per point increase 1.11, 95% CI 1.06–1.16, P < .001), as were chronic liver disease (HR 1.85, 95% CI 1.14–3.00, P = .013) and hemato-oncologic malignancies (HR 1.45, 95% CI 1.05–2.00, P = .025), whereas major surgery was associated with lower mortality risk (HR 0.60, 95% CI 0.38–0.95, P = .029). Treatment consultations by an infectious disease consultant or microbiology consultant were associated with significantly lower risk for mortality (HR 0.49, 95% CI .34–.71, P < .001), as were multiple individual variables of the EQUAL Candida scores, such as echocardiography, ophthalmoscopy, and initial treatment with an echinocandin (all P < .001), and, consequently, also higher EQUAL Candida scores (HR 0.14 per percent increase relative to max, 95% CI .08–.23, P < .001).
In the multivariable Cox regression models (Table 4), absence of treatment consultation by an infectious disease or clinical microbiology consultant, older age, hemato-oncologic malignancies, chronic liver disease, COVID-19, and the absence of initial treatment with an echinocandin, respectively, lower EQUAL Candida scores were independently associated with higher mortality.
DISCUSSION
We performed a subanalysis of the multicenter, observational ECMM Candida III study, which included 632 candidemia patients from 64 hospitals across 20 European countries. We found that non-ICU patients had a higher burden of hemato-oncologic malignancies and higher CCI scores. Kaplan–Meier survival analysis confirmed a significantly lower survival probability (P < .001) in the ICU group. Multivariable analysis of ICU and non-ICU patients confirmed that ICU treatment and higher CCI were independent predictors of mortality. Within the cohort of non-ICU patients, postsurgical non-ICU patients had the highest survival rate and the longest hospital stay, while patients with hemato-oncologic malignancies had the lowest survival probability (P = .007). In the multivariable Cox regression analysis, the absence of treatment consultation by an infectious disease or clinical microbiology consultant, older age, hemato-oncologic malignancies, chronic liver disease, COVID-19, and initial treatment with another drug than an echinocandin, respectively, lower EQUAL Candida scores remained independently associated with mortality.
In addition, nutritional status appears to be an important factor, as malnutrition was a relevant predictor in non-ICU patients and has previously been associated with higher mortality [23]. Conversely, obesity may prolong the duration of infection and hospital stay but without consistently affecting mortality [24]. In contrast to previous reports describing non-ICU patients also as older [16, 17], our study showed no significant differences in age or sex distribution between ICU and non-ICU groups. Non-ICU patients underwent more ophthalmologic examinations (40.1% vs 24.2%; P < .001) and tended to receive more infectious disease consultations, although that finding was not statistically significant. As ocular candidiasis can be asymptomatic in early phases [25, 26], relying on patient-reported symptoms as a trigger for ophthalmologic examinations may prove unreliable and is naturally not possible in sedated ICU patients. Therefore, ICU patients who cannot report their symptoms are generally considered a prime population for receiving ophthalmoscopic screening.
Our findings show that stepdown to fluconazole occurred significantly more often in non-ICU patients than in ICU patients. Even after excluding patients who died within the first 14 days after diagnosis, non-ICU patients still underwent stepdown therapy more frequently than ICU patients.
In our cohort, C. albicans remained the most common fungal isolate in both ICU and in non-ICU patients. However, despite low absolute numbers, P. kudriavzevii was significantly more frequent in non-ICU, while C. auris was predominantly isolated from ICU patients. Similar results have been reported previously. For example, a post hoc analysis of the CANDIPOP project in Spain, which focused on candidemia acquired outside the ICU, identified P. kudriavzevii as 1 of the 5 most common isolated species after C. albicans, C. parapsilosis, N. glabratus, and C. tropicalis [16]. The SENTRY Antimicrobial Surveillance Program did not identify a significant difference in P. kudriavzevii prevalence between ICU and non-ICU cohorts [27]. In contrast, another study reported P. kudriavzevii more frequently in non-ICU patients compared with ICU patients (5.3% vs 2.2%) [28]. An Italian study also reported that P. kudriavzevii was associated with the highest mortality rate in both ICU and non-ICU patients, although not statistically significant [29]. In our cohort, 30-day mortality was significantly higher for non-ICU patients with P. kudriavzevii infection (66.3%) compared with ICU patients. Of note, this increased mortality cannot be attributed to an inadequate first-line therapy, as all patients with P. kudriavzevii infection received echinocandins as initial treatment, except 4 non-ICU patients (1.0%) who were treated with fluconazole. Notably, all 4 of these patients were alive at the last follow-up of the study. Furthermore, our observation of C. auris predominance in ICU patients is consistent with existing literature, which shows a rise in C. auris infections in ICUs, particularly during the COVID-19 pandemic [30, 31].
Candida tropicalis tended to be more prevalent in the hemato-oncologic malignancies group, consistent with previous reports. One study identified C. tropicalis as the most commonly isolated species in hematologic patients, and a study in pediatric hematologic malignancy patients reported C. tropicalis as the most frequently isolated species, accounting for 30% of cases [32]. The median duration of hospitalization among those who survived at least 30 days after diagnosis was significantly shorter in non-ICU patients versus ICU patients (21 days, IQR 10–35 days vs 27 days, IQR 14–49 days, P = .016). Postsurgical non-ICU patients had the longest hospitalization, likely reflecting the complexity of their underlying surgical conditions and the need for repeated interventions, rather than prolonged treatment of IC or candidemia. These patients were initially sufficiently stable to undergo surgical procedures and often required prolonged recovery due to IC [16, 33].
Among non-ICU patients, those with hemato-oncologic malignancies had the highest mortality (P < .001 in Kaplan–Meier analysis), while the lowest mortality was observed in patients post major surgery.
This finding is consistent with previous reports demonstrating higher mortality rates for candidemia in medical wards compared with surgical wards [16, 34]. One possible explanation is that surgical patients may have fewer chronic comorbidities, and their candidemia may be more related to perioperative factors rather than advanced underlying disease [35].
For the whole group of non-ICU patients, older age, hemato-oncologic malignancies, chronic liver disease, and COVID-19 remained significant independent baseline predictors of mortality. The COVID-19 pandemic in its early phase was not only associated with high mortality rates among those with acute respiratory failure in the ICU but also with an uptick in candidemia rates, triggered by overwhelmed and overcrowded ICUs [36]. Interestingly, our study found that COVID-19 was also a major factor associated with mortality risk in non-ICU patients, as was chronic liver disease, a known risk factor for candidemia and associated mortality, triggered by fungal translocation through the gut- and liver disease–associated immunocompromise [37]. In terms of management, consultation by an Infectious Diseases or Microbiology consultant, as shown previously [38], and higher EQUAL Candida scores reflecting guideline adherence in diagnosis and treatment, respectively, initial treatment with an echinocandin [21] remained strong independent predictors of survival.
The following limitations of our study should be noted. Data were not consistently available for all patients, and the results shown here reflect a realistic scenario without the use of standardized diagnostic strategies or treatment protocols for candidemia. Also, most participating centers were tertiary reference hospitals; therefore, results may be less applicable to district hospitals or other secondary care settings. Differences in access to diagnostics and antifungal treatment options in individual countries may limit the comparability of the results [39], and local diagnostic and treatment pathways may have influenced patient management and outcomes. While the sampling strategy, which included only the first ten consecutive candidemia patients per center and a limitation of centers per country depending on population size, ensured that the study sample was representative of candidemia across Europe, limitations may include underrepresentation of potential seasonal or outbreak-related variations. While the geographical distribution of the data reflects Europe and its overall laboratory capacity [6], centers with better access to diagnostics and antifungal therapies might be overrepresented. As this subanalysis is observational, residual confounding factors cannot be ruled out. While the number of cases per center and centers per country were restricted, we did not adjust for clustering by center or for differences in diagnostics and therapy availability between countries, which may have affected the accuracy of the P-values, HRs, and the interpretation of treatment patterns and outcomes. Another limitation was that the calculation of some other clinical scores, like the Candida score [40], was not possible as the necessary clinical data, for example, on colonization were not systematically collected, and that the Ostrosky-Zeichner score could not be evaluated for prediction of candidemia as no unmatched control group (ie, ICU patients without candidemia) was available. Finally, due to the small absolute number of P. kudriavzevii and C. auris cases some of the findings from subgroup analyses should be interpreted with caution.
CONCLUSIONS
Patients with candidemia outside the ICU had more chronic comorbidities, including hematologic or oncologic diseases, but a higher survival rate than ICU patients, likely due to lower acute illness severity. While C. albicans was the predominant species in all groups and C. auris predominantly detected in the ICU, P. kudriavzevii was generally more common outside the ICU. Non-ICU patients more often underwent ophthalmoscopy, and postsurgical non-ICU patients had the highest survival rates and the longest hospital stays. In the non-ICU cohort, mortality was highest among hemato-oncologic malignancy patients.
Besides older age, hemato-oncologic malignancies, chronic liver disease, and COVID-19 were independently associated with mortality in non-ICU patients. In addition, several care-related factors were independently associated with mortality: the absence of consultation with an infectious disease or clinical microbiology specialist, the absence of initial treatment with an echinocandin, and lower EQUAL Candida scores. These findings could inform future guidelines and targeted interventions for non-ICU patients with candidemia, such as the implementation of systematic expert consultation or the emphasis on appropriate first-line antifungal therapy.
Supplementary Material
ofag133_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vazquez JA, Whitaker L, Zubovskaia A. Invasive candidiasis in the intensive care unit: where are we now? J Fungi (Basel) 2025; 11:258.40278079 10.3390/jof 11040258 PMC 12028288 · doi ↗ · pubmed ↗
- 2Wolfgruber S, Sedik S, Klingspor L, et al Insights from t 3 pan-European multicentre studies on invasive Candida infections and outlook to ECMM Candida IV. Mycopathologia 2024; 189:70.39088098 10.1007/s 11046-024-00871-0PMC 11294264 · doi ↗ · pubmed ↗
- 3Hoenigl M, Enoch DA, Wichmann D, Wyncoll D, Cortegiani A. Exploring European consensus about the remaining treatment challenges and subsequent opportunities to improve the management of invasive fungal infection (IFI) in the intensive care unit. Mycopathologia 2024; 189:41.38704761 10.1007/s 11046-024-00852-3PMC 11070387 · doi ↗ · pubmed ↗
- 4Denning DW . Global incidence and mortality of severe fungal disease. Lancet Infect Dis 2024; 24:e 428–38.38224705 10.1016/S 1473-3099(23)00692-8 · doi ↗ · pubmed ↗
- 5Lass-Flörl C, Kanj SS, Govender NP, Thompson GR, Ostrosky-Zeichner L, Govrins MA. Invasive candidiasis. Nat Rev Dis Primers 2024; 10:20.38514673 10.1038/s 41572-024-00503-3 · doi ↗ · pubmed ↗
- 6Hoenigl M, Salmanton-Garcia J, Egger M, et al Guideline adherence and survival of patients with candidaemia in Europe: results from the ECMM Candida III multinational European observational cohort study. Lancet Infect Dis 2023; 23:751–61.37254300 10.1016/S 1473-3099(22)00872-6 · doi ↗ · pubmed ↗
- 7Salmanton-García J, Cornely OA, Stemler J, et al Attributable mortality of candidemia—results from the ECMM Candida III multinational European observational cohort study. J Infect 2024; 89:106229.39025408 10.1016/j.jinf.2024.106229 · doi ↗ · pubmed ↗
- 8Egger M, Salmanton-García J, Barac A, et al Predictors for prolonged hospital stay solely to complete intravenous antifungal treatment in patients with candidemia: results from the ECMM Candida III multinational European observational cohort study. Mycopathologia 2023; 188:983–94.37566212 10.1007/s 11046-023-00776-4PMC 10687104 · doi ↗ · pubmed ↗