Triple-Dose Furmonertinib for Leptomeningeal Metastases in Advanced Epidermal Growth Factor Receptor (EGFR) L858R-Mutated Lung Adenocarcinoma: A Case Report
Hong Wu, Lei Li, Jing Yang, Yuan Tian, Hui Wang

TL;DR
A 73-year-old woman with advanced lung cancer achieved long-term survival using high-dose furmonertinib after other treatments failed.
Contribution
Demonstrates the potential of triple-dose furmonertinib as a salvage therapy for leptomeningeal metastases in EGFR L858R-mutated lung cancer.
Findings
High-dose furmonertinib combined with bevacizumab provided symptom relief and extended survival in a patient with LM.
The patient's overall survival exceeded six years from initial diagnosis, highlighting the effectiveness of the treatment strategy.
Sequential and multimodal management is crucial for advanced EGFR-mutant NSCLC with CNS involvement.
Abstract
Leptomeningeal metastases (LM) represent a severe and life-threatening manifestation of advanced non-small cell lung cancer (NSCLC). Despite advances in epidermal growth factor receptor (EGFR)-targeted therapies, central nervous system involvement continues to present major therapeutic challenges. We report a 73-year-old woman with EGFR L858R-mutated NSCLC who developed LM after multiple lines of therapy, including gefitinib, osimertinib, chemotherapy, anti-angiogenic therapy, and radiotherapy. Treatment with high-dose furmonertinib (240 mg daily) combined with bevacizumab resulted in symptom relief and additional survival. Remarkably, her overall survival exceeded six years from initial diagnosis. This case highlights the potential role of dose-escalated furmonertinib as salvage therapy in LM after osimertinib resistance and underscores the importance of sequential and multimodal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
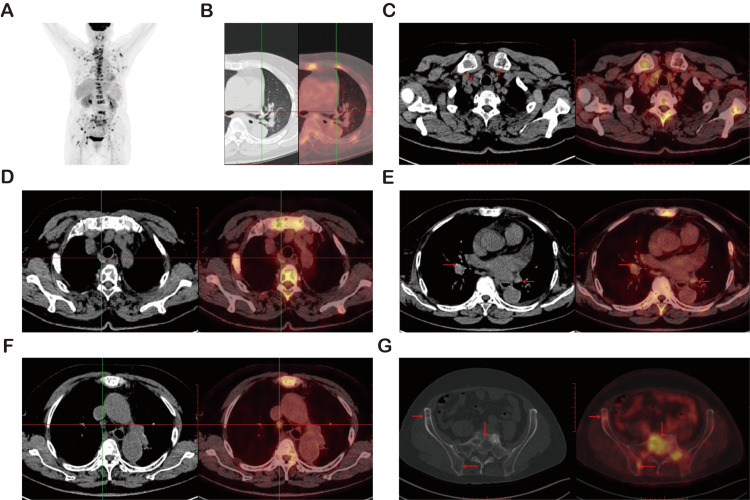 Figure 1
Figure 1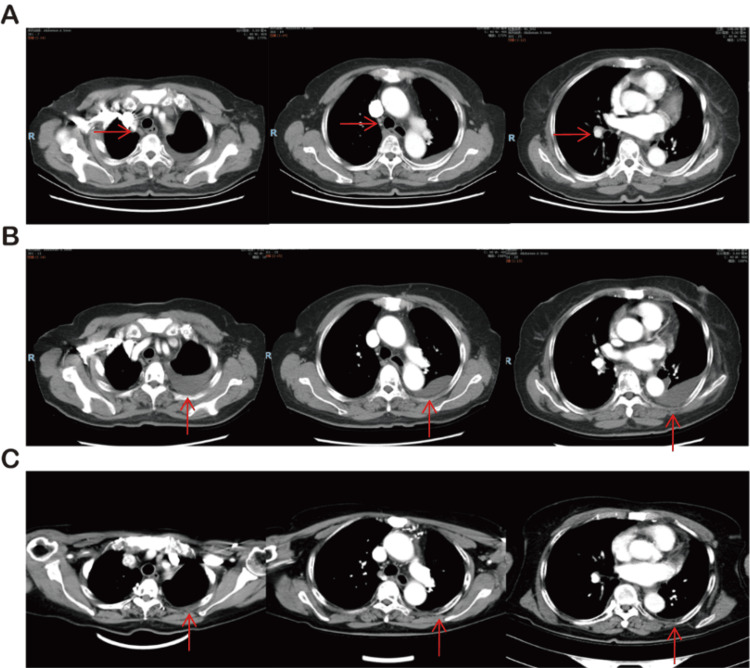 Figure 2
Figure 2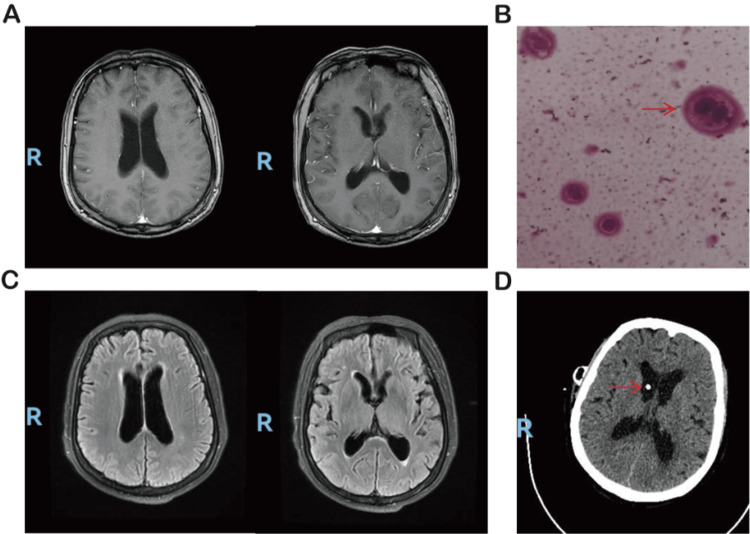 Figure 3
Figure 3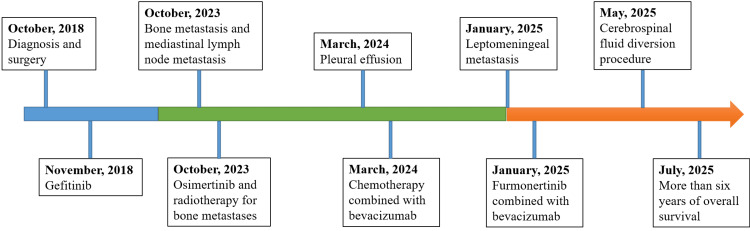 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Brain Metastases and Treatment · Lung Cancer Research Studies
Introduction
Leptomeningeal metastases (LM) represent one of the most challenging forms of central nervous system (CNS) progression in lung cancer. Non-small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) mutations are at higher risk of LM compared to EGFR wild-type cases, with an incidence approaching 9% [1,2]. In clinical practice, LM is typically diagnosed based on characteristic findings on contrast-enhanced magnetic resonance imaging (MRI), such as leptomeningeal enhancement, while cerebrospinal fluid (CSF) cytology serves as a supportive or confirmatory diagnostic tool. Historically, LM was associated with a median survival of less than one year, even with intrathecal chemotherapy, whole-brain radiotherapy (WBRT), or systemic chemotherapy [3].
Third-generation EGFR tyrosine kinase inhibitors (TKIs), especially osimertinib, have improved CNS control. However, LM progression remains a critical barrier, with limited effective treatment options after osimertinib resistance [4,5]. Furmonertinib, a third-generation EGFR-TKI with favorable CNS penetration, has shown encouraging efficacy in both clinical trials and real-world studies, particularly at higher doses [6]. A daily dose of 240 mg is commonly referred to as a “triple-dose” regimen, corresponding to three times the standard recommended dose of 80 mg. Nevertheless, detailed case reports describing its use in EGFR L858R-mutated NSCLC with LM remain scarce.
We present a patient with EGFR L858R-mutated lung adenocarcinoma who survived more than six years after initial diagnosis, including additional survival following LM managed with high-dose furmonertinib and bevacizumab.
Case presentation
A 73-year-old nonsmoking woman was admitted to the thoracic surgery department in October 2018 with complaints of chest and back pain. She underwent video-assisted thoracoscopic left upper lobectomy with mediastinal lymph node dissection. Intraoperatively, a 5 × 4 × 4 cm mass with ill-defined margins and visceral pleural indentation was observed in the left upper lobe. Postoperative pathology confirmed invasive adenocarcinoma with visceral pleural invasion, and one of seven lymph nodes was positive for metastasis. Molecular testing revealed an EGFR exon 21 L858R mutation, and the patient was diagnosed with left lung adenocarcinoma, staged as T2bN1M0 (stage IIB) according to the American Joint Committee on Cancer (AJCC) 8th edition TNM classification [7].
Following surgery, the patient received adjuvant gefitinib starting in November 2018. She remained on gefitinib until January 2022, during which regular follow-up demonstrated no evidence of recurrence or metastasis.
In October 2023, she presented again with recurrent chest and back pain. PET-CT revealed mediastinal and hilar lymphadenopathy together with widespread skeletal metastases, indicating postoperative recurrence (Figure 1).
PET-CT Findings Suggestive of Widespread Lymphatic and Skeletal Metastases(A) PET-CT demonstrates multiple hypermetabolic lesions involving lymph nodes and bones throughout the body. (B) No abnormal FDG uptake detected at the previous surgical site. (C) Increased FDG uptake in right paratracheal lymph nodes (SUVmax 4.3). (D) Hypermetabolic activity in upper paratracheal lymph nodes (SUVmax 3.8). (E) Bilateral hilar lymph nodes with elevated FDG uptake (SUVmax 4.5). (F) Marked uptake in lower paratracheal lymph nodes (SUVmax 6.2). (G) High FDG uptake in the sacrum, indicative of osseous metastasis (SUVmax 7.2).
She was started on osimertinib 80 mg daily, administered from October 2023 to March 2024, along with palliative radiotherapy to the T2-T3 vertebrae (30 Gy in 10 fractions). Follow-up CT scans showed partial regression of nodal disease, consistent with a partial response by RECIST (Response Evaluation Criteria in Solid Tumors) criteria, but progressive left pleural effusion developed (Figure 2). The patient experienced chest tightness and dyspnea and underwent thoracentesis, followed by intrapleural chemotherapy to control malignant effusion.
From March to December 2024, she received a total of 12 cycles of pemetrexed- and cisplatin-based chemotherapy combined with bevacizumab, followed by maintenance therapy. Bevacizumab was administered every 21 days at a weight-based dose. Imaging demonstrated stable disease in the mediastinum and hilum and a reduction in pleural effusion compared with previous assessments (Figure 2).
Serial CT imaging illustrating the evolution of mediastinal lymphadenopathy and pleural effusion.(A) Chest CT on December 29, 2023, after two months of osimertinib treatment, shows a reduction in mediastinal lymph node size. (B) On March 1, 2024, malignant pleural effusion was identified, prompting initiation of bevacizumab combined with chemotherapy. (C) On December 16, 2024, follow-up CT revealed improved mediastinal lymphadenopathy and reduced pleural effusion after treatment.
In January 2025, the patient developed new neurological symptoms, including dizziness and headache. Cranial MRI was unremarkable. Lumbar puncture revealed an elevated opening pressure of 26 cmH2O, and cerebrospinal fluid cytology was positive for malignant adenocarcinoma cells, consistent with leptomeningeal metastasis (Figure 3). Cerebrospinal fluid-based molecular testing for resistance mechanisms was not performed. She was therefore started on high-dose furmonertinib (240 mg daily) in combination with bevacizumab, resulting in progressive relief of neurological symptoms within the first several weeks after treatment initiation. No long-term corticosteroids or opioid analgesics were required during the initial neurological response.
During treatment with high-dose furmonertinib, the patient experienced decreased appetite and fatigue. No grade ≥3 treatment-related adverse events were observed, and the treatment was generally well tolerated.
In May 2025, she experienced recurrent severe headache and vomiting, and a cerebrospinal fluid diversion procedure was performed to relieve intracranial hypertension (Figure 3).
Neuroimaging and cerebrospinal fluid findings associated with leptomeningeal metastases.(A) Brain MRI on January 1, 2025, revealed no significant abnormalities. (B) Cerebrospinal fluid cytology showed large atypical cells with abundant cytoplasm and eccentrically located, hyperchromatic nuclei. (C) After initiating furmonertinib 240 mg daily, the patient’s dizziness improved; follow-up MRI on April 14, 2025, remained unremarkable. (D) On May 19, 2025, cerebrospinal fluid diversion was performed to relieve intracranial hypertension; high-density shadow in the ventricle represents the drainage catheter.
Despite initial improvement, she developed persistent high fever and delirium in July 2025 and eventually died of presumed intracranial infection.
A chronological overview of the disease trajectory, treatment interventions, and outcomes is summarized in Figure 4, highlighting the sequential application of surgery, targeted therapies, chemotherapy, radiotherapy, and neurosurgical procedures, as well as the dynamic adaptation of strategies in response to evolving disease progression.
Chronological timeline of the patient’s clinical course, treatment interventions, and key clinical events.
Discussion
LM are a devastating complication of NSCLC, often resulting in severe neurological symptoms, limited therapeutic options, and shortened survival [8]. Patients with EGFR-mutant NSCLC are particularly vulnerable, with an incidence of LM approaching 9%, compared to 3%-5% in the general NSCLC population [9]. Historically, prognosis has been poor, with a median overall survival (OS) of only 3-11 months despite intrathecal chemotherapy, whole-brain radiotherapy, or systemic chemotherapy [10]. The development of third-generation EGFR tyrosine kinase inhibitors (TKIs), which can penetrate the blood-brain barrier, has significantly improved CNS outcomes, yet LM continues to represent a major clinical challenge [11].
Furmonertinib is a novel, third-generation EGFR-TKI designed to achieve higher CNS drug exposure. Preclinical studies have demonstrated that its concentrations in brain tissue substantially exceed those in plasma [12]. Clinical evidence has confirmed these findings. In the pivotal phase III FURLONG trial, furmonertinib showed superior CNS progression-free survival (20.8 vs. 9.8 months) and higher CNS response rates compared with gefitinib [11]. Real-world studies have further supported its CNS activity, particularly at higher doses. In one prospective study of 48 patients with LM, high-dose furmonertinib (240 mg daily) achieved a CNS disease control rate of 92% and a median OS of 8.4 months [6]. Several case reports also support dose escalation after osimertinib failure, with rapid neurological improvement and survival benefits [13,14]. These findings highlight the potential of furmonertinib as a salvage therapy for LM.
The present case provides several important insights. First, our patient achieved an OS exceeding six years from initial diagnosis, far longer than typically reported in stage IIB EGFR-mutant NSCLC with LM. This outcome underscores the value of sequential, individualized treatment strategies incorporating surgery, adjuvant EGFR-TKI, systemic chemotherapy, anti-angiogenic therapy, radiotherapy, and finally high-dose furmonertinib. Second, after failure of osimertinib and multiple systemic therapies, the initiation of furmonertinib 240 mg daily combined with bevacizumab provided meaningful neurological improvement and extended survival. This clinical benefit aligns with emerging evidence suggesting that high-dose furmonertinib can achieve therapeutic CNS concentrations and overcome some mechanisms of resistance. Third, the case illustrates the potential utility of combining furmonertinib with anti-angiogenic therapy, which may further enhance CNS disease control, as suggested in recent retrospective analyses [15,16].
Conclusions
This report highlights a rare clinical course of EGFR L858R-mutant non-small cell lung cancer characterized by late-onset LM after multiple lines of therapy. LM remain a critical therapeutic challenge in EGFR-mutant disease, often developing despite prior tyrosine kinase inhibitor treatment. The patient’s favorable response suggests that high-dose furmonertinib (240 mg daily), particularly in combination with anti-angiogenic therapy, was associated with meaningful neurological symptom control in this clinical context, even after osimertinib failure. It should be noted that the observed clinical course occurred in the setting of multiple therapeutic interventions, including prior systemic treatments and cerebrospinal fluid diversion, which may have contributed to symptom improvement. Comprehensive and individualized sequencing of multimodal therapies appears crucial for sustained disease control, and dose-escalation strategies integrated within multidisciplinary management may represent a potential option for selected patients. Future prospective studies are warranted to further define the optimal role of high-dose furmonertinib in this difficult-to-treat population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leptomeningeal metastasis from non-small cell lung cancer and current landscape of treatments Clin Cancer Res Ozcan G Singh M Vredenburgh JJ 11292920233597243710.1158/1078-0432.CCR-22-1585 · doi ↗ · pubmed ↗
- 2Advancing leptomeningeal metastases treatment in EGFR-mutated non-small cell lung cancer: lessons from the BLOSSOM trial Transl Lung Cancer Res Bortolot M Huijs JW Brandsma D Compter A van Geel RM Hendriks LE 7131420253995821710.21037/tlcr-24-1006 PMC 11826264 · doi ↗ · pubmed ↗
- 3Therapeutic role of EGFR - tyrosine kinase inhibitors in non-small cell lung cancer with leptomeningeal metastasis Transl Oncol Jia C Xu Q Zhao L Kong F Jia Y 1018323920243800676110.1016/j.tranon.2023.101832 PMC 10728707 · doi ↗ · pubmed ↗
- 4Differential clinicopathological features, treatments and outcomes in patients with Exon 19 deletion and Exon 21 L 858R EGFR mutation-positive adenocarcinoma non-small-cell lung cancer BMJ Open Respir Res Batra U Biswas B Prabhash K Krishna MV 10202310.1136/bmjresp-2022-001492 PMC 1027753337321664 · doi ↗ · pubmed ↗
- 5Phase II efficacy and safety of 80 mg osimertinib in patients with leptomeningeal metastases associated with epidermal growth factor receptor mutation-positive non-small cell lung cancer (Blossom)J Clin Oncol Park S Baldry R Jung HA 274727564220243882895910.1200/JCO.24.00708 PMC 11315406 · doi ↗ · pubmed ↗
- 6High-dose Furmonertinib in patients with EGFR-mutated NSCLC and leptomeningeal metastases: a prospective real-world study J Thorac Oncol Chen H Yang S Wang L 65752020253926052110.1016/j.jtho.2024.09.1385 · doi ↗ · pubmed ↗
- 7The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging CA Cancer J Clin Amin MB Greene FL Edge SB 93996720172809484810.3322/caac.21388 · doi ↗ · pubmed ↗
- 8Chinese expert consensus on leptomeningeal metastases of lung cancer Thorac Cancer Lin G Wang Y Xin T 016202510.1111/1759-7714.70088 PMC 1214598640484812 · doi ↗ · pubmed ↗