Identifying ambulatory care sensitive conditions: a systematic review of studies defining sets of diseases with avoidable hospitalisations in European countries
Daniel Martinho-Dias, Bernardo Sousa-Pinto, Mariana Canela-Pais, Ana Garrido-Oliveira, Dulce Pinto, Altamiro Costa-Pereira, Tiago Taveira-Gomes, João Almeida Fonseca, António José de Almeida Soares

TL;DR
This study reviews how ambulatory care sensitive conditions are defined in Europe to avoid unnecessary hospitalizations.
Contribution
The paper systematically identifies and compares ACSC lists across six European countries using diverse methodologies.
Findings
263 unique ACSCs were identified for general populations using ICD-10 codes.
Infection-related and chronic diseases were most commonly listed as ACSCs.
Most ACSC lists used Delphi methods and ICD-10, but none fully met Solberg and Weissman criteria.
Abstract
Ambulatory care sensitive conditions (ACSC) are health conditions that can be adequately managed in the outpatient setting. Timely treatment and interventions may avoid the need for hospitalisation and emergency department visits. We aimed to identify ACSC lists developed for European populations. Systematic review. We included primary studies that aimed to develop a list of ACSC for the general population or subpopulations within European countries. Studies reporting a formal methodology were eligible. Systematic or narrative reviews, and protocols were excluded. PubMed, Web of Science and Scopus were searched on 21 October 2025. Data search was complemented with the search for ‘ambulatory OR preventable’ in the websites of the WHO Regional Office for Europe, OECD (Organisation for Economic Co-operation and Development) and NHSOF (British National Health Service Outcomes Framework).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
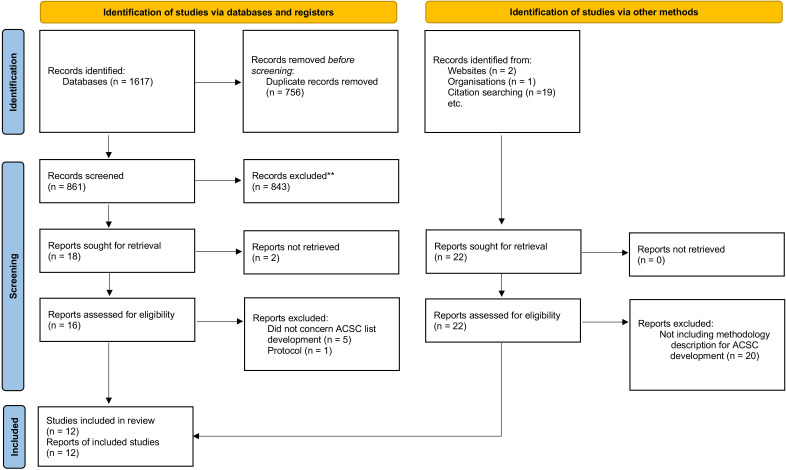 Figure 1
Figure 1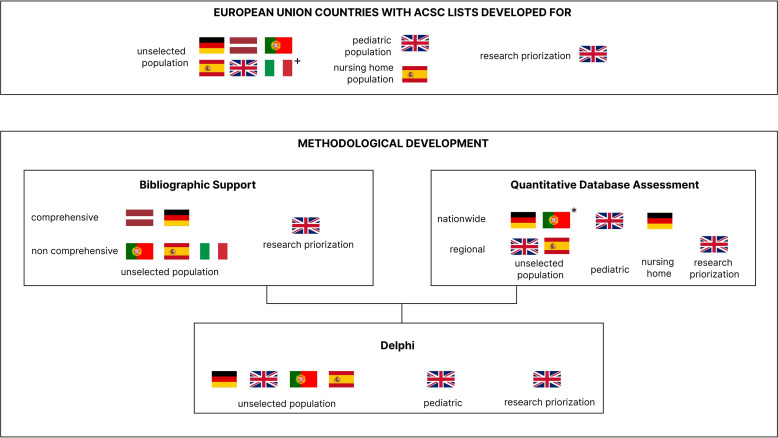 Figure 2
Figure 2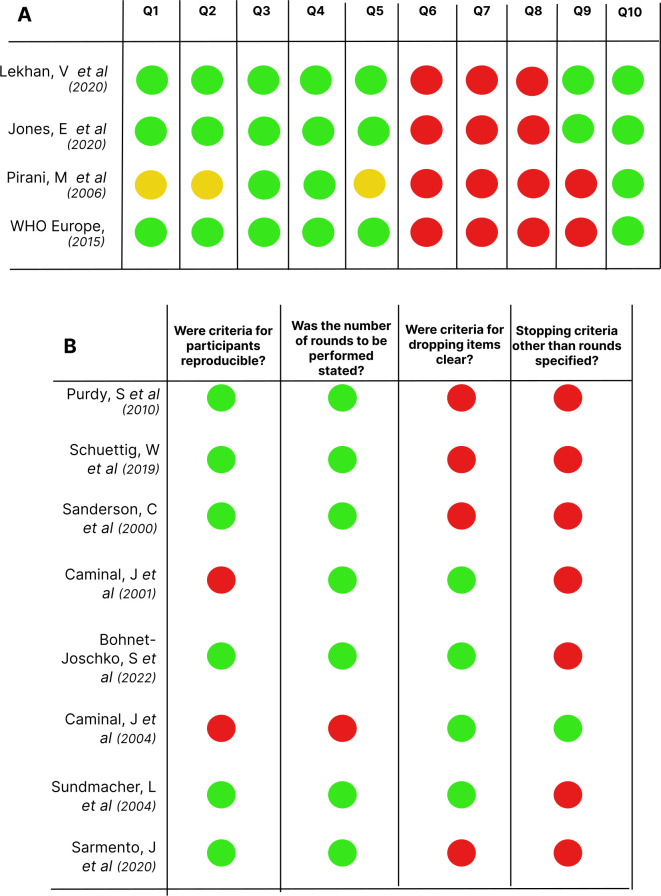 Figure 3
Figure 3| Target population | Authors | Main setting | Bibliographic support | Qualitative | Quantitative | A posteriori evaluation | Code system |
|---|---|---|---|---|---|---|---|
| General population | |||||||
| Germany | Schuettig and Sundmacher | ER-related ACSC | No | Yes (Delphi) | Yes. Nationwide insurance claims database | Yes. Evaluated the relationship between patient characteristics, ambulatory care settings, and the ER rate | ICD-10 |
| Latvia | WHO European Regional Officer | Admission-related ACSC | Yes. Based on a comprehensive search. | Yes (survey) | No | Frequency of patients hospitalised per condition; assessment of the frequency of readmissions | ICD-10 |
| UK | Sanderson and Dixon | Admission-related ACSC | No | Yes (Delphi) | Yes. Database of discharge diagnosis codes for the North West Thames Region | No | ICD-9 |
| Portugal | Sarmento | Admission-related ACSC | Yes. Based on a non-comprehensive search. | Yes (Delphi) | Yes. A frequency-based validation of Delphi results (national admissions database) | Two lists were developed. An extended list with Delphi’s ACSC+a core list with only frequency validated ACSC | ICD-10 |
| Spain | Caminal | Admission-related ACSC | Yes. Based on a non-comprehensive search. | Yes (Delphi) | Yes. Using a Catalonia admission database for the year 1996 | No | ICD-9 |
| Italy | Pirani | Admission-related ACSC | Yes. Based on a non-comprehensive search. | Yes (expert discussion without formal consensus panel) | No | Yes. Quantitative assessment of standardised rates of admissions in Emilia-Romagna Region | ICD-9 |
| Spain | Caminal | Admission-related ACSC | Yes. Based on a non-comprehensive search. | Yes (Delphi) | Yes. Database of hospital discharges obtained from the Catalan Health Service | Yes. Grouping of diagnosis codes and classification into type of intervention in ambulatory care | ICD-9 |
| Germany | Sundmacher | ER-related ACSC | Yes. Based on a comprehensive literature review | Yes (Delphi) | Yes. Database of all German hospital cases | Yes. A degree of preventability of selected ACSC and specified the medical actions and systemic changes | ICD-10 (ICD-9 mapped to ICD-10) |
| Ukraine | Lekhan | Admission-related ACSC | Yes. Based on a non-comprehensive search | Yes (survey) | Yes. Centralised databases of hospitalisations | Yes. Yearly preventable hospitalisation rates | ICD-10 |
| Paediatric population | |||||||
| UK | Jones | Admission-related ACSC | No | Yes (advisory panel) | Yes. Database of inpatient data from Hospital Episode Statistics for all NHS hospitals | Yes. Evaluation of rate of admission variation for identified ACSC | ICD-10 |
| Italy | Pirani | Admission-related ACSC | Yes. Based on a non-comprehensive search | Yes (expert discussion without formal consensus panel) | No | Yes. Quantitative assessment of standardised rates of admissions in Emilia-Romagna Region | ICD-9 |
| Nursing home population | |||||||
| Germany | Bohnet-Joschko (2022) | Admission-related ACSC | No | Yes (Delphi) | Yes. Database of health insurance claims data | Yes. Condition frequency and costs’ evaluation | ICD-10 |
| Research prioritisation | |||||||
| UK | Purdy | Admission-related ACSC | Yes. Based on a comprehensive literature review | Yes (Delphi) | Yes. Hospital discharge data (Hospital Episode Statistics) for south west area | Yes. Resource impact evaluation | ICD-10 |
| Parent category | Reported ICD-9 codes | Reported ICD-10 codes |
|---|---|---|
| Other bacterial diseases | 032, 033, 037 | A33, A34, A35, A36, A37, A46 |
| Diabetes mellitus | 250, 251, 250.1, 250.2, 250.3, 250.4, 250.5, 250.6, 250.7, 250.8, 250.9 | E10, E10.0, E10.1, E10.2, E10.3, E10.4, E10.5, E10.6, E10.7, E10.8, E10.9, E11, E11.0, E11.1, E11.2, E11.3, E11.4, E11.5, E11.6, E11.7, E11.8, E11.9, E12, E12.0, E12.1, E12.2, E12.3, E12.4, E12.5, E12.6, E12.7, E12.8, E12.9, E13, E13.0, E13.1, E13.2, E13.3, E13.4, E13.5, E13.6, E13.7, E13.8, E13.9, E14, E14.0, E14.1, E14.2, E14.3, E14.4, E14.5, E14.6, E14.7, E14.8, E14.9 |
| Chronic lower respiratory diseases | 490, 491, 492, 493, 494, 496, 493.9 | J40, J41, J42, J43, J44, J45, J46, J47 |
| Infections of the skin and subcutaneous tissue | 681, 682, 683, 686 | L00, L01, L02, L03, L03.0, L04, L05, L08, L08.0, L08.8, L08.9 |
| Renal tubulo-interstitial diseases | 590, 599, 590.1, 590.2, 590.3, 590.4, 590.5, 590.6, 590.7, 590.8, 590.9 | N10, N11, N12, N13.6 |
| Hypertensive diseases | 401, 402, 403, 404, 405, 402.01, 402.1, 402.11, 402.91 | I10, I10.0, I10.9, I11, I11.0, I11.9, I12, I13, I13.0, I13.1, I13.2, I13.9, I15 |
| Other forms of heart disease | 428 | I48, I49.8, I49.9, I50 |
| Diseases of oesophagus, stomach and duodenum | 531, 532, 533, 531.2, 531.4, 531.6, 531.9, 532.2, 532.4, 532.6, 533.2, 533.4, 533.6, 535.5, 536.8 | K21, K25, K25.0, K25.1, K25.2, K25.4, K25.5, K25.6, K25.9, K26, K26.0, K26.1, K26.2, K26.4, K26.5, K26.6, K27, K27.0, K27.1, K27.2, K27.4, K27.5, K27.6, K28.0, K28.1, K28.2, K28.4, K28.5, K28.6, K29, K29.7, K29.9, K30, K31 |
| Influenza and pneumonia | 481, 483, 485, 486, 482.2, 482.3, 482.9 | J09, J10, J11, J12, J13, J14, J15, J15.3, J15.4, J15.7, J15.8, J15.9, J16, J16.0, J16.8, J18, J18.0, J18.1, J18.8, J18.9 |
- —National Funds through FCT – Fundação para a Ciência e a Tecnologia, I.P., within the project RISE-Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrimary Care and Health Outcomes · Medical Coding and Health Information · Chronic Disease Management Strategies
Introduction
Ambulatory care sensitive conditions (ACSC) can be defined as health conditions that can undergo adequate management in the outpatient setting if treatment and interventions are timely delivered, with the potential avoidance of the need for hospitalisation and emergency department visits.1
Hospitalisations for ACSC are currently used as an outcome indicator of access to primary care and its quality.27 Indeed, the use of ACSC as a performance indicator is currently endorsed by many international organisations.1 These include the WHO Regional Office for Europe,8 the Organisation for Economic Co-operation and Development (OECD),9 10 the British National Health Service Outcomes Framework (NHSOF)11 and the American Agency for Healthcare Research on its Quality Prevention Quality Indicators.12 13 The conditions deemed as ACSC are not uniform, and the published lists are mostly directly endorsed by governmental programmes.
Estimates of the economic relevance of ACSC hospitalisations vary across Europe, with different magnitudes according to used methods and the size of the health systems. ACSC-related hospital costs account for several billion euros annually in large health systems and hundreds of millions in smaller countries.1417 Despite their relevance from the public health and economic standpoints, one of the earliest attempts to analyse avoidable hospitalisations started with Billings et al,18 who analysed a list of conditions they deemed as preventable. The authors concluded that patients with poor socioeconomic status and those uninsured or with basic coverage insurance were susceptible to increased hospitalisation rates for ambulatory sensitive conditions. The work of Billings et al followed that of Solberg et al and Weissman et al,19 20 who attempted to establish formal criteria for the definition of an ACSC. These criteria include (1) bibliographic support (ie, the existence of previous studies indicating that a certain condition may be an ACSC); (2) yearly hospitalisation rates of 1/10 000 population or higher; (3) clarity of condition definition and coding of diagnoses (4) potentially avoidable admission through primary care; and (5) hospitalisation is needed when the health problem occurs. Rooted in the development of these criteria is the idea that ACSC lists are not necessarily universally applicable either across countries nor across subpopulations with different characteristics. That is, what can be considered an ACSC depends on the country or population which is being considered. In addition, ACSC are consistently identified as relevant for primary care assessment, although specific lists have not been developed for all countries.
We need to better understand current evidence on ACSC, and how it has been generated and validated, particularly when used in primary care performance assessment or to inform health policy. To the best of our knowledge, evidence synthesis efforts on ACSC and on methodologies employed for the development of ACSC lists have not been made for European settings. In this study, we aim to systematically identify and characterise the methodological development of ACSC lists developed for populations in European countries.
Methods
This systematic review was written in accordance with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis)-2020 reporting guidelines.21
Eligibility criteria
We included primary studies that aimed to develop an ACSC list for the general population or subpopulations within European countries. Only studies that reported the methodology used for the development of the ACSC list were considered. Systematic or narrative reviews, and protocols were excluded. There were no language, date or publication status restrictions.
Information sources and search strategy
We searched three electronic bibliographic databases—PubMed, Web of Science and Scopus—on 21 October 2025. A search strategy was developed for each searched database. Terms were selected from primary studies on ACSC and from other systematic reviews.162227 The final search strategies can be consulted in online supplemental appendix 1. The electronic bibliographic search was complemented with the search for ‘ambulatory OR preventable’ in the websites of the WHO Regional Office for Europe, OECD and NHSOF. The references of included studies were checked for other studies that could have been missed from search strategy results. We manually searched for new ACSC lists within the studies identified during the screening phase that did not aim at list development per se. Those lists were to be included if the primary study developing them was found.
Selection process
Search results were deduplicated and screened independently by two reviewers first by title and abstract and subsequently by full-text reading.28 Final deduplication was manual but supported by Rayyan's built-in duplicates finder feature. Screening was conducted within the Rayyan platform, but no decision automation tools were used. Conflicts between reviewers were solved by consensus. Authors were contacted whenever available information was not sufficient to allow a decision on the study inclusion. A 4-week window for reply was provided.
Data collection process
Data was independently collected by two reviewers and introduced into a purposely-built Excel file. A pilot version of the form was initially developed and modified after testing. Collected data was merged into a single file and conflicts were resolved through consensus between the two reviewers. In the case of unclear records or definitions, authors were contacted for clarification and a 4-week window for reply was provided. There was no data imputation. Collected variables per study were listed as ACSC as well as variables related to study metadata, study design and characteristics of studied databases and Delphi panels. We also collected data on the presence of Solberg and Weissman criteria. The full set of variables is reported in online supplemental appendix 2. Studies in languages that the authors were not fluent in were translated to English using the DeepL system. We made translations from the Italian, German, Spanish and Finnish languages. We did not collect or treat individual patient data.
Risk of bias assessment
All studies with a qualitative component were assessed using Joanna Briggs Institute (JBI) critical appraisal tool for qualitative studies. Most studies included a consensus process through the Delphi method. Quality assessment of the Delphi method was based on the following questions by Diamond et al29 ‘Were criteria for participants reproducible?’. ‘Was the number of rounds to be performed stated?’, ‘Were criteria for dropping items clear?’, ‘Stopping criteria other than rounds specified?’. Both risk of bias assessment and Delphi quality were independently conducted by two reviewers and conflicts were solved by consensus.
Data analysis
Descriptive statistics are presented for each variable of interest (please address online supplemental appendix 2 for further detail). Studies characteristics, such as study designs, target population, setting, the number of conditions identified, their variation across lists and across subpopulations were tabulated. For each study, we assessed the five Solberg and Weissman criteria19 20 for ACSC establishment.
Identified conditions in each list were grouped in larger categories for improved information management. To create these categories, we identified all second-level parent International Classification of Diseases (ICD) codes and created new categories that would map for both ICD-9 and ICD-10 tables. Identified ACSC were then included under these new categories (with information on studies supporting them). A study without a code system30 has been manually attributed an ICD-10 code. Original codes were kept for traceability regarding condition grouping. No meta-analysis was conducted due to its inadequacy to answer the research question.
Regarding Delphi studies characterisation, we considered the panel members that completed all rounds and excluded pilot panels. If the consensus threshold was asymmetric between rounds, we considered the average threshold.
Patient and public involvement
There was no involvement of patient or public during the elaboration of this systematic review.
Results
Study selection
Our electronic bibliographic search retrieved a total of 1617 articles, of which 756 deduplicated records were screened for inclusion. A total of 10 primary studies meeting eligibility criteria were included. Two extra articles were included from manual reference checking, on authors’ contacts for clarification or via health authorities’ webpages search. Therefore, a total of 12 included articles were included163040 (figure 1).
Preferred Reporting Items for Systematic Review and Meta-Analysis flow diagram on primary studies including the development of lists of ambulatory care sensitive conditions for Europe.21 All included countries are described in online supplemental appendix 1. ACSC, ambulatory care sensitive conditions.
Study characteristics
Study characteristics are summarised in table 1. Included ACSC lists had different target populations—nine lists developed for the general population of their target country/region,163137 40 two lists were developed for paediatric patients,36 38 one for nursing home residents39 and one for research prioritisation purposes.30 Most lists considered hospital admissions and/or discharge diagnoses for ACSC definition, while two considered emergency department episodes for defining ambulatory care.31 37 Germany,31 37 39 UK,33 Portugal,16 Latvia,32 Spain35 and Ukraine40 were the only European countries with developed ACSC lists for their general population with a national scope. In Italy, an ACSC list has been developed, but for the Bologna region.36
Regarding Solberg and Weissman criteria: (1) a literature support was found in 8 lists,1630 32 3437 40 but only three were based on a comprehensive literature search30 32 37 (2) 10 lists provided have clarity in definitions163136 38 (3) 5 lists had a relevance for public health criteria of 1/10 000 population or stricter16 34 35 39 40 (4) all lists made assessments on whether the diagnosis is potentially avoidable by timely and effective ambulatory care (5) 7 lists described that ACSC would be considered if there was a need for hospitalisation once the health problem produced.333840
Eight lists used a database of admissions, discharges or emergency room episodes. Although the nationwide scope of seven out of eight lists, three did not use a nationwide database, but rather a regional database.3335
A Delphi method was employed in eight studies,1630 31 3335 37 39 usually as the main driver of ACSC selection. Four lists did not employ formal Delphi consensus methods.8 32 36 38 40 A median (IQR) of 3.0 (2.0–3.25) Delphi rounds were conducted per study, with a median (IQR) threshold for consensus of 75 (70–75) % of panellists. The median number of panellists that completed all rounds was 36.5 (32.75–42.5). Three studies included a pre-round pilot.30 31 34 Figure 2 ensues the European countries in which list development has been conducted, along with the respective methodological phases.
*European countries in which list development has been conducted and respective methodological phases. +Regional population, nationwide frequency validation post-consensus method. ACSC, ambulatory care sensitive conditions.
All lists referred to ACSC by using coding systems. The most frequently used coding system was ICD-10 (eight lists)163032 37 followed by ICD-9.3336
Conditions identified as ambulatory care sensitive conditions
Studies were heterogeneous in number and degree of detail with which the identified conditions were reported.
Amidst all included studies, a total of 1137 unique codes corresponding to 347 unique conditions were identified as ACSC. Each list identified on average 94.8 (73.7) codes and 28.9 (16.7) conditions.
The smallest list38 had six identified conditions while the biggest listed 64.37
Considering only second-level ICD-10 or their ICD-9 equivalents, a total of 114 ACSC were identified. Box 1 and table 2 list these conditions if they are present in at least half of the included lists. Further conditions and different overviews are presented as supplementary material, which is accessible at https://marianacpais.github.io/ambulatory_tables/.
Box 1Identified ambulatory care sensitive conditions (ACSC) present across 50% or more of included primary studies (groupings of conditions). The full list of conditions and origins is available at ambulatorycare.med.up.pt.Multicountry ACSCFull list of conditions available at: ambulatorycare.med.up.pt.
- Anaemias.
- Chronic lower respiratory diseases.
- Diabetes mellitus.
- Diseases of oesophagus, stomach and duodenum.
- Episodic and paroxysmal disorders.
- General symptoms and signs.
- Hypertensive diseases.
- Infections of the skin and subcutaneous tissue.
- Inflammatory diseases of female pelvic organs.
- Influenza and pneumonia.
- Intestinal infectious diseases.
- Ischaemic heart diseases.
- Metabolic disorders.
- Non-infective enteritis and colitis.
- Renal tubulo-interstitial diseases.
- Symptoms and signs involving the circulatory and respiratory systems.
- Tuberculosis.
- Viral and prion infections of the central nervous system.
- Viral infections characterised by skin and mucous membrane lesions.
No conditions were common to all lists; 37 (31.2%) of conditions were present in at least one-third of developed lists, with 9 (7.8%) present in over two-thirds of all lists.
Regarding general populations only, a total of 263 unique ACSC have been defined (932 codes). For the paediatric age, 28 conditions (70 codes) were identified,36 38 and 37 diagnoses (58 codes) for the nursing homes population.38 A research prioritisation exercise for the UK identified 18 unique codes (10 conditions).38
The identified ACSC are summarised in supplementary table S2 (http://ambulatorycare.med.up.pt/) according to their closest general term, as lists varied in the degree of specificity. Most commonly identified ACSC (in at least nine lists) were cardiovascular or with cardiovascular complications (‘Diabetes mellitus’, ‘Hypertensive diseases’, ‘Other forms of heart disease’), chronic respiratory (‘Chronic lower respiratory diseases’) and infectious (‘Influenza and pneumonia’, ‘Infections of the skin and subcutaneous tissue’, ‘Other bacterial diseases’).
Risk of bias in studies
No ACSC list identified in the primary studies explicitly fulfilled all five criteria defined by Solberg et al38 and Weissman et al,19 20 but ten lists fulfilled at least 3/5 criteria. Most studies provided clarity in the definition of conditions (11/12),163238 40 defined ACSC as potentially avoidable by timely and effective ambulatory care (10/12)1631 3338 40 and were supported on previous literature (9/12).163032 34 Seven studies explicitly mentioned defining ACSC regarding the necessity of hospitalisation once the health problem occurs.333840 Only four studies required a condition to be relevant for public health (a yearly hospitalisation rate of at least 1 per 10 000 population) to define it as a potential ACSC.163436 39
Application of the JBI critical appraisal tool for qualitative results yielded a median 6.5 (6.0–7.0) points out of 10 possible points. No studies reported on question 6 (regarding locating the research culturally), on question 7 (regarding the influence of the researcher on the research, and vice versa), nor on question 8 (related to patient involvement) of the appraisal tool. All studies were consistent regarding question 4 (on congruity between the research methodology and data analysis), and question 10 (conclusions drawn from analysis).
Eight studies including Delphi methods were evaluated according to Diamond et al tool for quality of methodological reporting and were attributed a quality score.29 Regarding the final quality score, six studies achieved two points1630 31 3335 and two studies received three points37 39 (out of four possible points) according to Diamond et al criteria.29 The item most frequently classified as ‘low risk of bias’ was that on the statement of the number of rounds (7/8).16 30 31 33 34 37 Reproducibility of participant criteria for panels was present in six studies,16 30 31 33 37 39 while four stated criteria for dropping items.34 35 37 39 Only one article specified stopping criteria other than rounds.37 The risk of bias assessment as well as the reporting quality for Delphi studies is summarised in figure 3.
(A) Risk of bias assessment using Joanna Briggs Institute critical appraisal tool for qualitative studies. Green— yes; yellow—unclear; red—no. (B) Quality of qualitative reporting for each included study with a Delphi component (n=8), according to Diamond et al items.29 Green—risk of bias not present; red—risk of bias present or no information available regarding item.
Discussion
Findings
In this study, we systematically identified available ACSC for European populations and methodologically characterised them. We identified lists covering six European countries (Germany, Latvia, the UK, Portugal, Spain, Ukraine). We learnt that most primary studies included lists which are diagnosis-based, aim at national, general populations and include Delphi components to define ACSC. The most consensual conditions across lists were infectious diseases, chronic cardiovascular (diabetes, hypertension) and chronic respiratory diseases. However, eligible primary studies did not follow all desirable methodological steps for list development. Previous bibliographic support, as defined by Solberg and Weissman as relevant criteria for ACSC development, is not present in all studies: only one-third report conducting a comprehensive literature search prior to ACSC list development, with another third not reporting any search prior to qualitative or quantitative study implementations. Support from real-world evidence databases is limited as most studies did not include a nationwide database or a representative sample of nationwide cases. Often, consensus panels attempt to establish ACSC for all countries and their general populations1631 3335 37 having the support of regional databases or insurance claim databases. We did not find the use of any database including primary care data, which we believe could prove of benefit to establish referrals processes and the health user pathway within the healthcare system. We also found some relevant limitations in the employed methodologies for achieving consensus (figure 2). List development frequently relies on Delphi assessments. The Delphi method is an iterative, multiround process designed to achieve expert consensus and is widely applied in guideline development and priority setting. While it is valuable in contexts where empirical evidence is limited, the methodology is subject to limitations, including variability in consensus definitions and risks of selection bias and unrepresentative expert input.264144 Despite this, almost all Delphi components included over 20 experts, which is in line with a previous recommendation that the panel must include at least 20 experts to provide robust estimates in a Delphi exercise.45 Overall, we consider the available evidence on list development to be mostly qualitative, in low quantity and of low-medium quality.
Strengths and limitations
To the best of our knowledge, this is the first systematic review on the topic to include a methodological characterisation of developed lists and to focus on the European setting. We believe our eligibility criteria to be clear and appropriate to answer our question, and our search was comprehensive. We have identified available primary evidence, its quantity, discrepancy in methods and its potential flaws, informing on risk of bias for qualitative components and measuring the application of Solberg19 and Weissman criteria.20 We consider the aggregation of conditions under the ICD coding system to be useful for clearer definitions. We have created a webpage for easier data access and increased readability https://ambulatorycare.med.up.pt.
We also have important limitations. The evidence supporting ACSC list development is limited and methodologically heterogeneous. Few studies report comprehensive literature reviews or the use of nationally representative data, and none incorporate primary care databases. Furthermore, we also did not have access to individual patient data or to explore publication bias.
Comparison with previous literature
The literature on application of previously developed lists for admission rates and temporal trends of diagnosis4649 is larger than literature reporting the development of ACSC reviews, which have focused on primary care accessibility,50 organisational aspects22 and continuity of ambulatory care.51 Previous syntheses of evidence have also been focused on specific populations, such as the paediatric patients,52 53 migrants54 and those in need of palliative care.55 Interventions aimed at reducing ACSC hospitalisations have also been evaluated,24 as well as costs.56 None of these reviews address the topic of methodological characterisation and assessment, nor do they focus on European population.
Meaning of the study
This work has some relevant implications. The evidence for European countries has methodological fragilities, with insufficient external validity and generalisability. This calls for caution when interpreting literature on temporal or regional trends in ACSC. It also calls for caution when employing ACSC-related hospitalisations to assess primary care and establish pay-for-performance models. Although the evaluation of this relationship is commonly used in diverse countries,2711 57 we believe these assessments would largely benefit from stronger evidence to yield fairer evaluations and to safely improve ambulatory care. We also found that all developed lists are diagnosis-based. While this may be extremely relevant from the public health perspective, their relevance for the referring physician in the primary care setting may be less relevant. The primary care clinicians are most likely the most relevant stakeholders in determining whether the patient will be treated in the ambulatory care setting or referred. Their decision is frequently based on clinical presentation rather than raw diagnosis, and in their ability to timely access diagnostic tools that safely exclude the need for urgent care in doubtful cases.5860
Unanswered questions and future research
We have mapped available lists for European countries, but quantitative validation from individual patient data is missing and some methodological fragilities identified by risk of bias tools should be addressed in future studies. It also remains unclear which are the variables that influence consensus, and the reasons for the large variations in lists observed across countries. We believe some effort should be put towards the creation of a common framework for the development of validated lists per population.
From a direct public health perspective, future research should be directed into improving ACSC condition selection and definition, including both clinical and user perspectives in the selection of conditions and in the identification of barriers to ambulatory care.
From a primary care standpoint, we consider that future research should focus on generating and aggregating evidence for primary care referral. This could reduce clinical uncertainty at the ambulatory settings. Improved decision-making at the referral decision time could then lead to a safer and more efficient shift of certain patients from the hospital to the ambulatory care setting.
Conclusion
Despite the public health and economic relevance of ACSC, there is a low volume of lists defining these conditions in Europe, with low agreement between lists and diverse methodologies employed for list development, mostly consisting of qualitative or mixed methods designs, with non-negligible risk of bias. There is a need for more robust evidence regarding ambulatory care sensitive conditions. Such data would better inform policymakers, thereby facilitating future policies designed to safely streamline patient journeys within the healthcare system.
Supplementary material
10.1136/bmjopen-2025-112777online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rocha JVM Santana R Tello JE Hospitalization for ambulatory care sensitive conditions: What conditions make inter-country comparisons possible? Health Policy Open 2021210003010.1016/j.hpopen.2021.10003037383514 PMC 10297774 · doi ↗ · pubmed ↗
- 2Partanen V-M Arffman M Manderbacka K et al Mortality related to ambulatory care sensitive hospitalisations in Finland Scand J Public Health 2020488394610.1177/140349482094472232755271 · doi ↗ · pubmed ↗
- 3Kozak LJ Hall MJ Owings MF Trends in avoidable hospitalizations, 1980-1998 Health Aff (Millwood)2001202253210.1377/hlthaff.20.2.22511260947 · doi ↗ · pubmed ↗
- 4Rizza P Bianco A Pavia M et al Preventable hospitalization and access to primary health care in an area of Southern Italy BMC Health Serv Res 2007713410.1186/1472-6963-7-13417760976 PMC 2045098 · doi ↗ · pubmed ↗
- 5Harrison MJ Dusheiko M Sutton M et al Effect of a national primary care pay for performance scheme on emergency hospital admissions for ambulatory care sensitive conditions: controlled longitudinal study BMJ 2014349 g 642310.1136/bmj.g 642325389120 PMC 4228282 · doi ↗ · pubmed ↗
- 6Cartier T Naiditch M Lombrail P Avoidable hospitalizations: the sole responsibility of primary care?Rev Epidemiol Sante Publique 2014622253610.1016/j.respe.2014.04.00525026885 · doi ↗ · pubmed ↗
- 7Regula o índice de desempenho da equipa multiprofissional das unidades de saúde familiar de modelo B, e a atribuição dos incentivos institucionais a estas e às unidades de cuidados de saúde personalizados, Portaria n.° 411-A/20232023
- 8WHO Assessing Health Services Delivery Performance with Hospitalizations for Ambulatory Care Sensitive Conditions. Health Services Delivery Programme, Division of Health Systems and Public Health 2016