Comparison of tissue acquisition techniques for Next-Generation Sequencing of non-small cell lung cancer (NSCLC)
Amyn Bhamani, Sindhu Bhaarrati Naidu, Naimish Adroja, Lucy Rogers, Lavanya Anandan, Phil Bennett, Tanya Ahmad, Martin D Forster, Asia Ahmed, Ricky Thakrar, Sam M Janes, David A Moore, Neal Navani

TL;DR
This study compares different tissue sampling methods for lung cancer sequencing, finding that some techniques are less reliable and may delay treatment.
Contribution
The study identifies specific tissue acquisition methods associated with higher success rates for NGS in non-small cell lung cancer.
Findings
DNA-based NGS was successful in 87.1% of specimens, with endobronchial ultrasound-guided techniques showing the highest success rate.
Pleural fluid cell blocks and percutaneous pleural biopsies had the lowest success rates for NGS processing.
Actionable genomic alterations were found in 28% of specimens, with RNA-based analysis revealing additional fusion gene events.
Abstract
Next-Generation Sequencing (NGS) allows the use of more efficacious targeted treatments for lung cancer; however, sample inadequacy can cause delays in patient pathways. Here, we compare various methods of tissue acquisition used in clinical practice and identify factors associated with inadequate sampling. Specimens submitted for NGS from a large single-centre UK academic institution following confirmation of lung cancer were reviewed. The primary objectives were to assess the proportion in which such analysis was successfully completed and identify factors, including the method of tissue acquisition, associated with sample inadequacy for, or failure of, the analysis. Secondary analyses included an assessment of genomic alterations identified by NGS-based analysis and specimen processing times. DNA-based NGS analysis was successfully completed in 87.1% (n=511/587) of all specimens,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
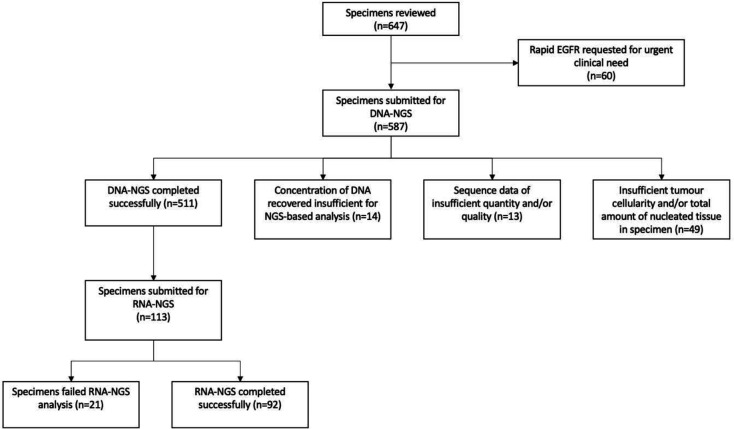 Figure 1
Figure 1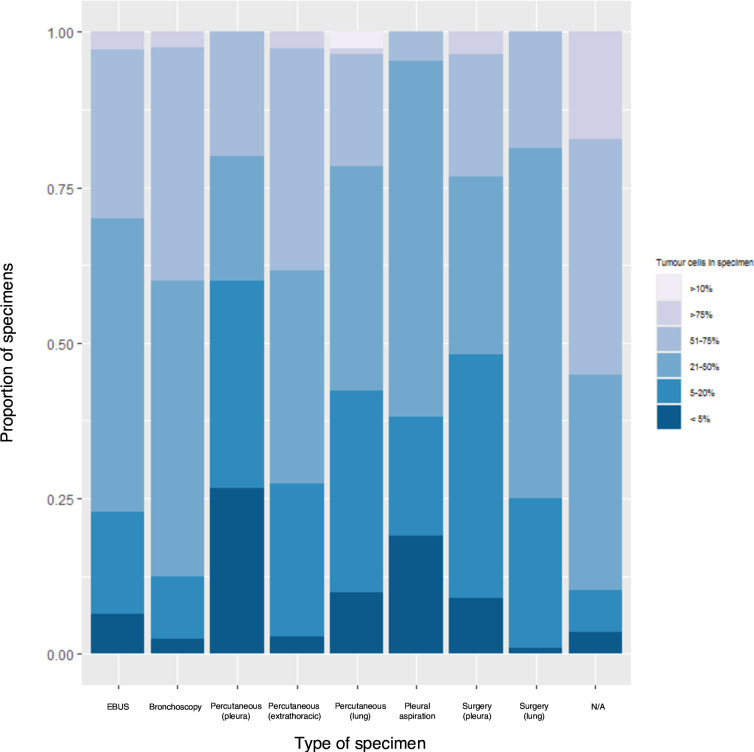 Figure 2
Figure 2| Frequency (n) | Percentage (%) | |
|---|---|---|
| Sex | ||
| Female | 279 | 47.5 |
| Male | 308 | 52.5 |
| Median patient age (years) | 69.0 (IQR 58.0–75.0) | |
| Median specimen age (days) | 11.0 (IQR 8.0–18.0) | |
| Age groups | ||
| <50 | 52 | 8.9 |
| 50–59 | 113 | 19.3 |
| 60–69 | 148 | 25.2 |
| 70–79 | 200 | 34.1 |
| ≥80 | 74 | 12.6 |
| Stage | ||
| 1 | 83 | 14.1 |
| 2 | 27 | 4.6 |
| 3 | 111 | 18.9 |
| 4 | 321 | 54.7 |
| Missing | 45 | 7.7 |
| Type of lung cancer | ||
| Adenocarcinoma | 535 | 91.1 |
| Non-small cell carcinoma, not otherwise specified (NSCLC—NOS) | 15 | 2.6 |
| Squamous cell carcinoma | 13 | 2.2 |
| Large cell neuroendocrine (NEC) | 9 | 1.5 |
| Other | 15 | 2.6 |
| Type of specimen | ||
| Flexible bronchoscopy | 40 | 6.8 |
| EBUS-TBNA | 140 | 23.9 |
| Percutaneous image-guided pleural biopsy | 15 | 2.6 |
| Percutaneous image-guided extra thoracic tissue and lymph node biopsy | 73 | 12.4 |
| Percutaneous image-guided peripheral lung and mediastinal mass biopsy | 111 | 18.9 |
| Other | 29 | 4.9 |
| Pleural fluid cell block | 21 | 3.6 |
| Thoracic surgery—pleural biopsy | 56 | 9.5 |
| Thoracic surgery—lung and lymph node specimens | 96 | 16.4 |
| Missing | 6 | 1.0 |
| NGS panel | ||
| MGP-1 | 425 | 72.4 |
| MGP-4 | 162 | 27.6 |
| Total specimens | DNA-based NGS successful (%) | DNA-based NGS successful | P value | DNA-based NGS successful | P value | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Female | 279 | 237 (84.9) | 0.700 (0.431 to 1.137) | 0.149 | 0.734 (0.436 to 1.237) | 0.246 |
| Male | 308 | 274 (89.0) | 1.00 | – | 1.00 | – |
| Patient’s age | ||||||
| Per increasing year | – | – | 0.982 (0.962 to 1.003) | 0.090 | 0.986 (0.964 to 1.007) | 0.193 |
| Specimen age | ||||||
| Per increasing day | – | – | 1.002 (0.998 to 1.005) | 0.334 | 0.999 (0.996 to 1.003) | 0.583 |
| Stage | ||||||
| Missing | 45 | 39 (86.7) | 1.087 (0.436 to 2.713) | 0.858 | 0.720 (0.256 to 2.024) | 0.534 |
| 1 | 83 | 71 (85.5) | 0.990 (0.498 to 1.967) | 0.976 | 1.102 (0.416 to 2.918) | 0.844 |
| 2 | 27 | 25 (92.6) | 2.091 (0.479 to 9.128) | 0.327 | 1.002 (0.179 to 5.606) | 0.998 |
| 3 | 111 | 101 (91.0) | 1.689 (0.822 to 3.474) | 0.154 | 1.001 (0.429 to 2.337) | 0.997 |
| 4 | 321 | 275 (85.7) | 1.00 | – | 1.00 | – |
| Type of specimen | ||||||
| Flexible bronchoscopy | 40 | 36 (90.0) | 1.000 (0.310 to 3.226) | 1.000 | 0.936 (0.287 to 3.054) | 0.913 |
| Percutaneous image-guided—pleural biopsy | 15 | 9 (60.0) |
|
|
|
|
| Percutaneous image-guided—extra thoracic tissue and lymph node | 73 | 63 (86.3) | 0.700 (0.294 to 1.664) | 0.420 | 0.719 (0.283 to 1.829) | 0.489 |
| Percutaneous image-guided—peripheral lung and mediastinal mass | 111 | 88 (79.3) |
|
| 0.432 (0.176 to 1.062) | 0.068 |
| Other | 29 | 25 (86.2) | 0.694 (0.211 to 2.285) | 0.549 | 0.645 (0.181 to 2.295) | 0.498 |
| Pleural fluid cell block | 21 | 14 (66.7) |
|
|
|
|
| Thoracic surgery—pleural biopsy | 56 | 50 (89.3) | 0.926 (0.337 to 2.545) | 0.881 | 0.905 (0.303 to 2.706) | 0.858 |
| Thoracic surgery—lung and lymph node | 96 | 94 (97.9) |
|
|
|
|
| Endobronchial ultrasound | 140 | 126 (90.0) | 1.00 | – | 1.00 | – |
| Missing | 6 | 6 (100) | – | – | – | |
| NGS panel | ||||||
| MGP-4 | 162 | 144 (88.9) | 1.264 (0.720 to 2.220) | 0.414 | 1.273 (0.680 to 2.383) | 0.451 |
| MGP-1 | 425 | 367 (86.4) | 1.00 | – | 1.00 | – |
| Total, n (%) | Co-mutation with TP53, n (%) | |
|---|---|---|
| KRAS (total specimens) |
|
|
| KRAS—G12C | 54 (10.6) | 23 (4.5) |
| KRAS—dual mutations | 2 (<1.0) | 2 (<1.0) |
| EGFR (total specimens) |
|
|
| EGFR—exon 19 deletions | 31 (6.1) | 17 (3.3) |
| EGFR—exon 19 single nucleotide variant | 1 (<1.0) | 0 (0.0) |
| EGFR—exon 20 insertions | 2 (<1.0) | 0 (0.0) |
| EGFR—exon 20 single nucleotide variant | 7 (1.4) | 3 (<1.0) |
| EGFR—exon 21 single nucleotide variant | 32 (6.3) | 17 (3.3) |
| EGFR—other mutations | 5 (1.0) | 3 (<1.0) |
| EGFR—dual mutations | 9 (1.8) | 4 (<1.0) |
| BRAF |
|
|
| ERBB2 (HER2) |
|
|
| MET (total specimens) |
|
|
| MET (exon 14 skipping mutations) | 3 (1.0) | 2 (<1.0) |
| MET—dual mutations | 1 (<1.0) | 1 (<1.0) |
| STK11 | 17 (3.3) | 10 (2.0) |
- —Longfonds BREATH Consortia
- —MRC UKRMP2 Consortia
- —Garfield Weston Trust
- —University College London Hospitals Charitable Foundation
- —http://dx.doi.org/10.13039/100004331Johnson and Johnson
- —Ruth Strauss Foundation
- —http://dx.doi.org/10.13039/100009730Stand Up To Cancer
- —http://dx.doi.org/10.13039/501100000289Cancer Research UK
- —http://dx.doi.org/10.13039/501100020252CRUK Lung Cancer Centre of Excellence
- —CRUK City of London Centre
- —http://dx.doi.org/10.13039/501100000833Rosetrees Trust
- —Horizon Europe
- —http://dx.doi.org/10.13039/100001003Boehringer Ingelheim
- —UCL/UCLH NIHR Biomedical Research Centre
- —http://dx.doi.org/10.13039/501100000265Medical Research Council
- —http://dx.doi.org/10.13039/100004334Merck
- —http://dx.doi.org/10.13039/100014013UK Research and Innovation
- —MSD
- —http://dx.doi.org/10.13039/100004325AstraZeneca
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Cancer Genomics and Diagnostics · Lung Cancer Treatments and Mutations
Introduction
Lung cancer is the leading cause of cancer death in the UK1 and remains a condition that is predominantly diagnosed at late stage.2 Next-Generation Sequencing (NGS) encompasses a range of massively parallel DNA sequencing technologies that have revolutionised genomic testing by way of simultaneously capturing a much wider spectrum of genetic information than can be obtained from assessing single genes.3 In turn, this can enable the use of more efficacious targeted treatment strategies for individuals with advanced lung cancer and also reduce tissue requirements when compared with performing multiple less informative tests independently. In 2020, European Society for Medical Oncology guidelines recommended the routine use of NGS for the analysis of tumour samples in advanced non-squamous non-small cell lung cancer (NSCLC).4
Tissue NGS-based tests are typically associated with high sensitivity and specificity5 6 and a targeted DNA-based NGS panel has been shown to detect known oncogenic driver events in 65% of individuals with NSCLC.7 In addition, up to 26% of individuals with lung adenocarcinoma who previously tested negative for genomic alterations using non-NGS techniques have been found to have clinically relevant alterations on subsequent NGS-based testing.8 By enabling multiple target genes to be assessed simultaneously, NGS can also reduce the overall time to receive results that are fully informative with regards to therapeutic selection, as well as the need for retesting and/or repeat biopsies which may be associated with exclusionary sequential testing.9 Indeed, modelling undertaken in the USA suggests that NGS is associated with a lower overall cost and a significant reduction, of up to 4 weeks, in the time to initiation of appropriate targeted therapy, when compared with using sequential PCR-based testing strategies.10
The treatment landscape for NSCLC has rapidly evolved since the identification of gefitinib as targeted therapy for individuals harbouring EGFR mutations in 2004.11 In the UK, therapies targeting oncogenic variants in genes including anaplastic lymphoma kinase (ALK), BRAF, EGFR, KRAS, MET, NTRK, ROS1 and RET are now available in routine clinical practice.12 In addition, therapies for additional mutations such as ERBB2 (HER2)13 have been approved for use in the European Union and the USA, while new targets and associated targeted therapies are currently under evaluation in clinical trials. Consequently, NGS is likely to play an increasingly important role as we move further forward in the era of precision medicine.
Routine clinical practice incorporates a range of tissue acquisition techniques with overlapping roles in lung cancer management. For instance, endobronchial and peripheral lung biopsies are primarily undertaken for histological confirmation of malignancy, while pleural fluid aspiration and biopsies of pleura and extra-thoracic tissue (eg, peripheral lymph nodes or distant metastases) also help inform clinical staging. Pleural aspiration may also provide symptomatic relief to patients with large effusions. Similarly, endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is also essential to accurately stage the mediastinum and support decision making regarding suitability for surgical resection and neo-adjuvant treatment. Finally, surgical resection remains the gold standard treatment for early-stage lung cancer, but also provides definitive diagnostic confirmation of malignancy when lesions are unsuitable for preoperative biopsy due to size or location.
These factors must be considered by lung cancer multidisciplinary teams (MDTs) when planning tissue acquisition for lung cancer. However, as some NGS technologies require a higher quality and concentration or even greater total DNA input than quantitative PCR, it is imperative that this is also considered when planning tissue acquisition to ensure that samples sufficient to facilitate successful NGS processing are obtained. However, data on the suitability of various tissue acquisition techniques used in clinical practice for NGS are limited.
A pathway for NGS and fusion gene testing implemented at our institution has previously been described.14 In this follow-up analysis, we assessed the adequacy of a range of biopsy techniques used in clinical practice for NGS and identified novel factors associated with inadequate sampling.
Materials and methods
All cases of non-squamous NSCLC diagnosed at our institution are submitted for DNA-based NGS (DNA-NGS) analysis as routine standard of care. Testing was initially performed using Multi-Gene-Panel-1 (MGP-1) until mid-2020, when this was changed to an expanded Multi-Gene-Panel-4 (MGP-4).15 Both panels were ISO accredited to the international standard 15 189 and included EGFR, KRAS, BRAF, NRAS and ERBB2 as well as other less commonly mutated genes. Before 2021, all cases in which DNA-NGS was uninformative were also reassessed, and those suitable for further processing based on the amount of residual tumour tissue were submitted for fusion gene analysis by RNA-based analysis (RNA-NGS). The ISO-15189 scope of this fusion assay was restricted to inter-genic or intra-genic rearrangement involving ALK, BRAF, EGFR, MET, ROS1, RET, NTRK1 and NTRK3.
Percutaneous image-guided biopsies, including pleural biopsies, were primarily performed by three consultant thoracic radiologists cumulatively undertaking, on average, over 120 peripheral lung and 35 pleural or chest wall soft tissue biopsies per year. Biopsies were performed under CT or ultrasound (US) guidance using semi-automated spring activated cutting devices and 18G needles. Between three and eight passes were typically obtained per procedure. Percutaneous pleural biopsies included both targeted and non-targeted procedures. EBUS-TBNAs and bronchoscopies were performed by seven consultant respiratory physicians. Between four and six passes per lymph node were typically obtained during each EBUS procedure using 21G or 22G needles. Intranodal forceps and cryobiopsies were not used for EBUS procedures during the study period.
Specimens obtained via percutaneous image-guided biopsy, surgery and EBUS-TBNA were placed directly in formalin and processed for histological analysis. Pleural fluid specimens were sent fresh to the laboratory and processed onto slides using a 95% ethyl alcohol fixative to make the initial diagnosis. Following this, a formalin-fixed cell block was made from the fluid to facilitate further testing. All histology and cytology specimens were reviewed by consultant thoracic pathologists. Rapid onsite evaluation was not available.
We carried out a retrospective observational study of specimens submitted for NGS analysis, following confirmation of a lung cancer diagnosis, between 1 January 2018 and 31 December 2020. Specimens submitted for rapid PCR-based EGFR mutation analysis only (either on account of high clinical urgency or low DNA concentration) were excluded from the analysis. The primary objective was to assess the proportion of specimens in which DNA-based NGS analysis was successfully completed and identify factors, including the method of tissue acquisition and stage of disease, associated with inadequate sampling. The stage of disease was obtained from lung cancer MDT documentation (based either on pathological confirmation or by radiological consensus) at the time of biopsy. This included previously obtained surgical specimens submitted for NGS analysis in individuals subsequently presenting with recurrent disease. Missing stage was analysed as a separate category.
Secondary analyses included assessing the number of specimens in which known oncogenic driver mutations were identified and the processing time for each specimen. The latter was defined as the number of working days between specimen receipt in the molecular diagnostics laboratory and the date that the report was issued. The date of specimen receipt was termed ‘Day 0’.
Multivariable logistic regression analysis was used to explore factors associated with a successful analytical outcome. In addition to the method of tissue acquisition, the multivariable analysis was adjusted for patient and specimen age (defined as the number of days between biopsy and specimen receipt in the molecular diagnostic laboratory) as continuous variables, sex, disease stage and type of NGS panel. Complete case (listwise) analysis was used where the method of tissue acquisition was missing. χ^2^ analysis was used to compare differences between groups with categorical variables. A p value of <0.05 was considered significant. Statistical analyses were performed using R (V 4.4.1).
Full ethics committee approval was not required, as confirmed by the National Health Service (NHS) Health Research Authority decision tool.16 Informed patient consent was not obtained due to the retrospective, observational and non-interventional nature of the study.
Patient and public involvement
Patients and members of the public were not involved in the design, conduct, analysis or dissemination of this study.
Results
We reviewed 647 specimens from 560 individuals with NSCLC. 60 specimens underwent rapid PCR-based EGFR only testing on account of high clinical urgency and were excluded from subsequent analysis, meaning that 587 were included in the final analysis.
Baseline demographic and clinical data
Median patient age was 69.0 years (IQR 58.0–75.0) with 52.5% (n=308/587) of specimens obtained from men. Most specimens were from individuals aged ≥60 years (71.9%, n=422/587) and those with late stage (3 or 4) disease at the time of biopsy (73.6%, n=432/587). Staging was not available in a minority (7.7%, n=45/587) of cases (table 1).
EBUS-TBNAs were the most common method of tissue acquisition (23.9%, n=140/587) followed by percutaneous image-guided (CT or US) lung and mediastinal mass biopsies (18.9%, n=111/587) and thoracic surgical specimens (16.4%, n=96/587).
Association between tissue acquisition technique and the likelihood of successful DNA-based NGS analysis
DNA-based NGS analysis was successfully completed in 87.1% (n=511/587) of cases, with 8.3% (n=49/590) of specimens rejected outright due to insufficient tumour cellularity and/or the total amount of nucleated tissue in the sample. After fluorometric quantitation, the concentration of DNA recovered from a further 2.4% (n=14/587) of specimens that were initially accepted for processing was found to be insufficient for NGS-based analysis, and where possible, these were submitted for PCR-based EGFR testing. Finally, 2.2% (n=13/587) of specimens proved refractory to DNA-based NGS analysis, yielding sequence data of an insufficient quantity and/or quality. Consequently, DNA-based NGS analysis could not be completed in a total of 12.9% (n=76/587) of specimens overall (figure 1). The mean turnaround time in the molecular diagnostics lab for samples processed successfully was 5.9 working days from date of specimen receipt to date of report (SD 1.6).
Summary of specimens reviewed and submitted for next generation sequencing. NGS, next generation sequencing.
Pleural fluid cell blocks and percutaneous image-guided pleural biopsies were associated with the lowest rate of analytical success (66.7%, n=14/21 and 60.0%, n=9/15, respectively, table 2). By contrast, DNA-based NGS analysis was successfully completed in 97.9% (n=94/96) of specimens obtained via thoracic surgery, 90.0% (n=126/140) obtained via EBUS-TBNA and 79.3% (n=88/111) obtained via percutaneous image-guided lung biopsy. Multivariable analysis (table 2) showed that these differences were statistically significant (table 2).
No significant associations were identified between analytical failure and sex, participant or specimen age, stage of disease at the time of tissue acquisition or type of NGS panel.
Association between percentage tumour cellularity and the likelihood of successful DNA-based NGS analysis
Specimens with a histologically estimated tumour cellularity below the assay’s validated limit of detection (LOD) of 5% were considered unsuitable and rejected in all cases. DNA-based NGS analysis was completed successfully in all 15 (100%) specimens with a tumour cellularity >75%, and while lower, there was no significant difference (p=0.52) in likelihood of analytical success between specimens with tumour cellularities in the following ranges: 5%–20% (92.0% success), 21%–50% (93.1% success) and 51%–75% (95.2% success) (online supplemental table 1).
Percutaneous image-guided pleural biopsies (26.7%, n=4/15) and pleural fluid cell blocks (19.1%, n=4/21) were the collection techniques most frequently associated with the lowest tumour cellularity (<5%). In comparison, only 8.9% (n=5/56) of surgical pleural biopsies were associated with the lowest tumour cellularity (figure 2).
Percentage of tumour cells within specimen, stratified by tissue acquisition technique. EBUS, endobronchial ultrasound.
Mutations identified by DNA-based NGS analysis
DNA-based NGS analysis identified known oncogenic driver variants in 60.6% (n=310/511) of specimens. KRAS mutations specifically were identified in 34.2% (n=175/511), including 10.6% (n=54/511) with the now actionable G12C variant and 0.4% (n=2/511) with dual mutations (KRAS A11T/G12V and KRAS G12V/G13) (table 3).
EGFR mutations were identified in 13.7% (n=70/511) of specimens, with 13.3% (n=68/511) considered targetable with EGFR-tyrosine kinase inhibitors (TKIs) (online supplemental table 2). Dual EGFR mutations were reported in 1.8% (n=9/511). Exon 21 mutations were most common (6.3%, n=32/511), followed by exon 19 deletions (6.1%, n=31/511). Other, less commonly identified mutations included BRAF (3.5%, n=18/511), ERBB2 (HER2) (2.2%, n=11/511) and MET (1.8%, n=9/511). The MET aberrations included single nucleotide variants and three exon 14 skipping mutations associated with increased sensitivity to selected MET inhibitors. STK11 mutations were identified in 17 (3.3%) specimens—this included three (<1%) with KRAS/ STK11 co-mutations.
Structural variants identified by RNA-based NGS analysis
Following uninformative DNA-based NGS analysis, 113 specimens were reflexed for RNA-based NGS analysis in an attempt to identify inter-genic and intra-genic fusions. 21 (18.6%) of these were unsuccessful, 1 being rejected as the remaining nucleated tissue had cut out during prior DNA extraction, 17 being rejected as unsuitable for processing due to insufficient RNA quality/quantity, and 3 which yielded inadequate sequencing data for any meaningful analysis. Of the remaining 92 specimens, 20 fusion events were identified in 19 samples, including six involving MET Exon 14 skipping and five involving ALK-EML4 fusion. Four fusions involving ROS1 were identified (online supplemental table 3).
Overall, known oncogenic driver variants were identified in 63.8% (n=326/511) of specimens following both DNA and reflex RNA-based NGS analyses, with 28.0% (n=143/511) of these being considered currently therapeutically actionable—this includes ALK fusion, BRAF V600E, KRAS G12C, MET-Exon 14 skipping, RET fusion, ROS-1 fusion and TKI-sensitive EGFR mutations.17
Discussion
In this analysis of 587 specimens submitted for NGS analysis following confirmation of NSCLC, DNA-based NGS was successfully completed in 87% of cases. DNA-based NGS could not be completed in 13% of cases due to low tumour cellularity, insufficient total nucleated tissue, inadequate DNA yield (concentration/integrity) or actual NGS assay failure, likely due to additional DNA quality issues. Pleural fluid cell blocks (67%) and percutaneous image-guided pleural biopsies (60%) were associated with the lowest success rate, with 19% and 27% of specimens obtained via these techniques, respectively, rejected outright due to insufficient tumour cellularity. As expected, surgical lung and lymph node specimens were associated with the highest success rate, with only 2% unable to be analysed successfully.
Guidelines in the UK recommend pleural fluid analysis as the first line investigation for individuals presenting with suspected secondary pleural malignancy.18 However, a national study of molecular testing found that individuals with late-stage lung cancer who underwent pleural aspiration or biopsy were more likely to require a second biopsy compared with those who had an EBUS-TBNA.19 In keeping with these results, DNA-based NGS analysis was successful in only two-thirds of pleural fluid specimens in our series. In addition, while details on the number of patients with negative pleural fluid cytology prior to confirmation of lung cancer via alternative methods of specimen acquisition were not available for analysis, the sensitivity of pleural fluid cytology for diagnosing a malignant pleural effusion (MPE) in lung cancer is reported to be 62%.20 Extrapolating our results to these data suggests that only about 40% of pleural fluid specimens obtained from individuals with lung cancer and MPE would yield both a diagnosis and a cell block adequate for NGS-based analysis. Data from the USA also show that individuals requiring multiple biopsies may have up to 90 days added to their pre-treatment timeline on account of a significant time lag between each procedure, while multiple biopsies are associated with a higher incidence of complications such as pneumothorax and bleeding.21
Despite these considerations, it is important to acknowledge that pleural fluid analysis plays an important role in informing clinical lung cancer staging, particularly for patients with pleural effusions but an otherwise low probability of malignant pleural disease based on imaging features and clinical history. For these patients, negative pleural fluid cytology may enable them to have treatment with curative intent. However, timely initiation of treatment is also associated with a reduced risk of death among patients with lung cancer,22 and delays in NGS processing due to inadequate sampling may have a detrimental prognostic impact. Our data suggest that in otherwise well patients with a high probability of malignant pleural disease, pleural aspiration should be carried out for therapeutic purposes where possible, but referral for further specimen acquisition should not be delayed while awaiting the outcome of pleural fluid analysis. In such cases, an early referral for surgical pleural biopsy or local anaesthetic thoracoscopy, when more easily accessible sites for tissue acquisition are not present, would also allow definitive pleural fluid management (eg, in the form of pleurodesis or the insertion of a tunnelled indwelling pleural catheter) in the same sitting.
Over the past few years, EBUS-TBNA has become an increasingly accessible and important method of tissue acquisition for both diagnostic and staging purposes in the context of suspected lung cancer. While there have previously been concerns about the suitability of tissue acquired via this technique for subsequent NGS-based analysis, a recent meta-analysis of 1175 participants showed EBUS-TBNA was associated with a yield of 86.5% for NGS.23 In our cohort, 90% of specimens obtained via EBUS-TBNA were adequate for DNA-based NGS analysis, confirming the importance of this technique in the context of lung cancer diagnostics.
Underscoring the importance of NGS in ensuring the optimum treatment for individuals with lung cancer, 28% of specimens had actionable genomic alterations following both DNA and reflex RNA-based NGS analysis. Over 50% of specimens with EGFR mutations also harboured TP53 co-mutations, a combination associated with poor outcomes in individuals treated with EGFR-directed TKIs.24 Similarly, seven cases identified co-existing STK11 and KRAS mutations, with STK11 alteration previously identified as the most prevalent genomic driver of primary resistance to PD-1 axis inhibitors in KRAS-mutant lung adenocarcinoma25 and shown to be associated with a poor prognosis.26
RNA-based NGS analysis was associated with a lower rate of success (82%) compared with DNA-based (87%), despite specimens with insufficient tumour cellularity having already been excluded. This was partially due to the sequential extraction strategy employed during the period studied—specifically, the recall ‘batch’ testing of RNA only if required following initial DNA testing14—which meant that some samples may have been several months old at the time of RNA analysis, increasing the chance of tissue being exhausted. RNA is also known to be more unstable and prone to degradation by both natural and artificial processes such as those used during tissue processing into FFPE material.27 28 With regard to the former, techniques for the combined extraction of both DNA and RNA together are available; however, previous work by the laboratory (data not shown) had revealed a slightly higher failure rate due to lower average RNA quality from such combined extractions. Considering this and other factors such as cost, a sequential strategy was retained.
Limitations of this study are recognised. These data are from a specialist thoracic oncology centre with expertise in tissue acquisition, processing and on-site molecular testing. Additionally, both the minimum acceptable tumour cellularity, based on the assay’s validated LOD, and the quality/total amount of input DNA required by different laboratories can vary significantly. The latter depends on the library generation methodology, sequencing platform and the size of the gene panel used. Consequently, these findings may not be directly applicable to other centres. On the other hand, this is an NHS-based clinical cohort with genuine representation across a large selection of individuals with NSCLC, unbiased by factors such as medical insurance coverage/reimbursement, which may affect the make-up of cohorts from countries with different healthcare systems. In addition, despite the retrospective nature of the study, it is the largest to date to examine the efficacy of sampling techniques for NGS, there were clear criteria for patient inclusion, consecutive patients were included and NGS testing was standardised. The number of percutaneous image-guided pleural biopsies and pleural fluid cell blocks included in this analysis was also relatively small, and both targeted and non-targeted pleural biopsies were included in the analysis. However, this reflects the low prevalence (approximately 15%) of MPEs at presentation among patients with NSCLC reported in international thoracic oncology cohorts.29
In conclusion, 87% of lung cancer specimens obtained via a range of tissue acquisition techniques and submitted for DNA-based NGS analysis were successfully processed. Pleural fluid cell blocks and percutaneous image-guided pleural biopsies were techniques least likely to result in success, and other sites for tissue acquisition could be considered in these individuals. NGS is increasingly vital to provide important therapeutic and prognostic information for individuals with lung cancer and can be delivered in routine clinical practice.
Supplementary material
10.1136/bmjresp-2025-003793online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer Research UK Lung cancer statistics 2022 Availablehttps://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer
- 2National lung cancer audit: NLCA state of the nation report 2024 Availablehttps://www.lungcanceraudit.org.uk/wp-content/uploads/2024/04/NLCA-State-of-the-Nation-Report-2024.pdf
- 3Behjati S Tarpey PS What is next generation sequencing?Arch Dis Child Educ Pract Ed 201398236810.1136/archdischild-2013-30434023986538 PMC 3841808 · doi ↗ · pubmed ↗
- 4Mosele F Remon J Mateo J et al Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group Ann Oncol 202031149150510.1016/j.annonc.2020.07.01432853681 · doi ↗ · pubmed ↗
- 5Chin ELH da Silva C Hegde M Assessment of clinical analytical sensitivity and specificity of next-generation sequencing for detection of simple and complex mutations BMC Genet 20131410.1186/1471-2156-14-6PMC 359921823418865 · doi ↗ · pubmed ↗
- 6Lih C-J Harrington RD Sims DJ et al Analytical Validation of the Next-Generation Sequencing Assay for a Nationwide Signal-Finding Clinical Trial: Molecular Analysis for Therapy Choice Clinical Trial J Mol Diagn 2017193132710.1016/j.jmoldx.2016.10.00728188106 PMC 5397672 · doi ↗ · pubmed ↗
- 7Moore DA Balbi K Ingham A et al Analysis of a large cohort of non-small cell lung cancers submitted for somatic variant analysis demonstrates that targeted next-generation sequencing is fit for purpose as a molecular diagnostic assay in routine practice J Clin Pathol 2018711001610.1136/jclinpath-2018-20531930054375 · doi ↗ · pubmed ↗
- 8Drilon A Wang L Arcila ME et al Broad, Hybrid Capture–Based Next-Generation Sequencing Identifies Actionable Genomic Alterations in Lung Adenocarcinomas Otherwise Negative for Such Alterations by Other Genomic Testing Approaches Clin Cancer Res 2015213631910.1158/1078-0432.CCR-14-268325567908 PMC 4917003 · doi ↗ · pubmed ↗