Prioritizing Health in War and Conflict: The 2025 War in Iran and the Call for Global Peace
Azam Raoofi, Elham Ehsani-Chimeh, Amirhossein Takian

Abstract
Click any figure to enlarge with its caption.
 Figure
FigurePeer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth and Conflict Studies · Disaster Response and Management · Nuclear Issues and Defense
The Israel-Iran war, intensified by the U.S. involvement, highlights the devastating toll of war on health systems, social unity, and public well-being. The conflict claimed 1062 lives and left 5800 injured, including 126 women, 47 children, 26 healthcare personnel and 28 emergency vehicles and facilities, ie, ambulances, hospitals, and healthcare centers damaged (Table).^1^ This paper reports the amplifying effects of pre-existing sanctions on the war harms, and applies the World Health Organization (WHO) Global Health and Peace Initiative (GHPI) as the guiding framework for the tailored policy recommendations.
Reported strikes on healthcare facilities, eg, on a hospital in Kermanshah, underscores the humanitarian toll and endangering civilians and healthcare workers.^5^ Such attacks violate Geneva Conventions and International Humanitarian Law, including WHO Resolution WHA65.20, and call for international accountability.^6^ Such destruction weakens health systems, jeopardizes population health, and compounds humanitarian crises by collapsing care, worsening mental health burdens, and forcing families into unsafe, crowded shelters.^1^ It is recommended that the WHO and the United Nations Human Rights Council initiate an independent fact-finding mission or monitoring mechanism to investigate health-targeted attacks and ensure accountability, where appropriate.^6,7^ Even before June 2025 hostilities, Iran’s healthcare system was strained by prolonged sanctions, intensified since 2018, which impeded access to essential medicines, diagnostics, and medical technologies, undermining care for millions and compromised the country’s ability to respond to public health emergencies, a situation worsened by COVID-19 and other crises.^8,9^ Sanctions have also exacerbated provincial health disparities, hindered chronic disease management, and weakened supply chains.^10^ The war further destabilizes this fragile infrastructure, elevating humanitarian and public health risks. Targeting healthcare facilities—seen in Syria and Gaza—exacts a heavy toll on vulnerable populations and undermines recovery and rebuilding.^11^ Sanctions weakened health system resilience during the June 2025 strikes by delaying medicines, degrading equipment, and reducing surge capacity—turning limited damage into excessive morbidity and mortality.
Beyond immediate casualties, the conflict causes severe physical and mental harm. Survivors face limited access to care due to the destruction or repurposing of healthcare facilities, leading to long-term disabilities and worsening chronic illnesses, straining the health system.^1^ Persistent violence creates trauma, including chronic stress, anxiety, and post-traumatic stress disorder,^11,12^ undermining resilience as mental health services collapse amid facility closures and medicine shortages.^11^ In Gaza, since October 2023, and Syria, psychotropic drug stock-outs and facility shutdowns increased depression and post-traumatic stress disorder prevalence by up to 26.5%.^12^ In Iran, memories of the Iran–Iraq War (1980–1988) amplify collective trauma, shaping national responses.^13^ This may intensify current psychological distress, shape help-seeking behaviors, and constrain community resilience, thereby magnifying the mental-health burden following the recent strikes.^12,13^ With only 2.48 psychiatrists per 100 000 people in 2020^14^ and frequent disruptions, community-based mental health initiatives stall, deepening the care gap. The crisis also deepens the political fault lines, as the loss of military and security leaders adds strain to the social fabric and heightens national trauma. Recent aggressive actions raise concerns about long-term public health threats.
Iran’s situation presents a distinct challenge compared to other contemporary health crises, eg, Ukraine and Gaza. Unlike Ukraine, which benefits from external aid, Iran, isolated by sanctions and political constraints, faces an uphill battle in accessing critical medical supplies and humanitarian aid.^9,10,15^ In Gaza, the blockade and conflict since October 7, 2023, have nearly collapsed the healthcare system.^16,17^ While both Gaza and Iran face systemic fragility under sustained shocks, Iran’s relative functionality potentially might be attributed to its decentralized structure and legacy of community health workers. Nonetheless, sanctions and conflict disrupt supply chains and threaten Iran’s care delivery. Iran’s health system has shown resilience in past emergencies, with nurses, physicians, and community health workers continuing to provide care during COVID-19 and sanctions.^9,10^ Yet sanctions plus conflict create a double vulnerability, intensifying supply-chain breakdowns and workforce pressures demanding targeted international intervention.
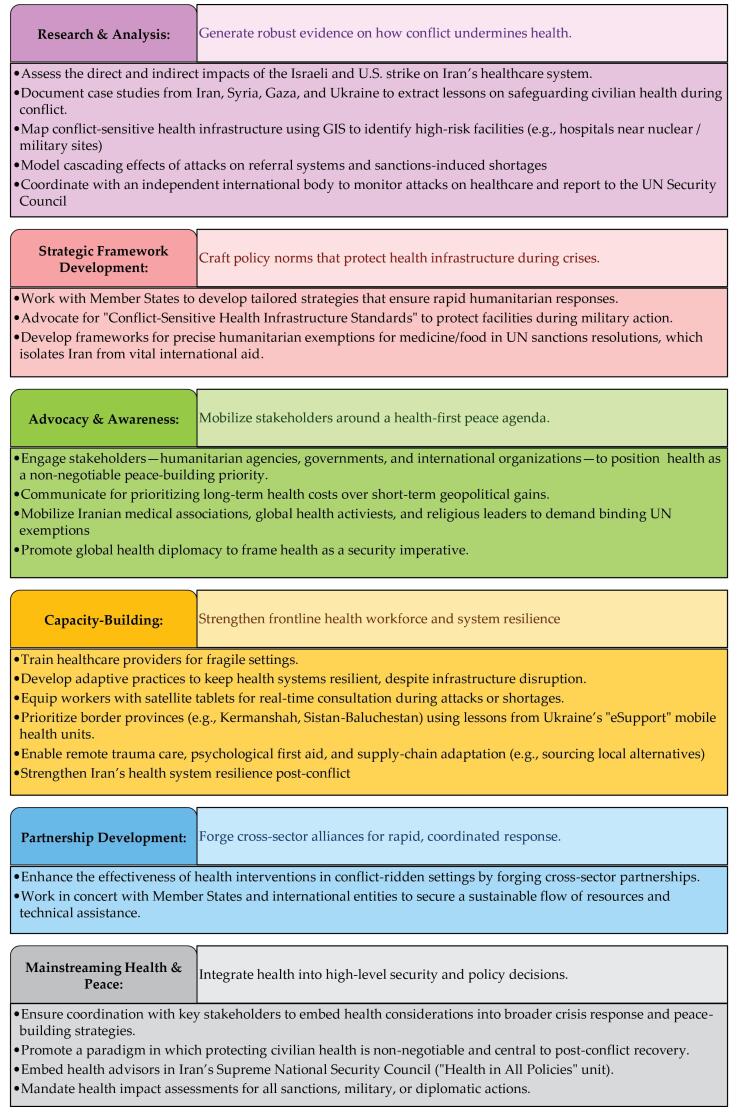
Lessons from global crises emphasize that conflict’s toll goes beyond the battlefield. The World Health Summit 2024 panel on “Health in War and Conflict” urged integrated health governance to address injuries, infrastructure loss, and psychological distress. The WHO’s GHPI provides an operationally focused framework for this integration focusing on health as a bridge for peace and a platform for collaboration. To translate health into a practical unifying force three concrete mechanisms are focused on feasible measures derived from this approach are essential for maintaining essential health services under conflict and sanctions:
A paradigm shift must place health at the center of crisis response and long-term stability.^18^
Moving Forward: Global Accountability and a New Peace Paradigm
GHPI repositions health in peacebuilding initiatives and offers concrete applications to mitigate conflict’s health impacts (Figure). Despite decades of research, health in conflict zones remains compromised by global decisions. We urge world leaders to safeguard civilian health through stronger global health governance, recognizing that the costs of conflict—mortality, chronic illness, and mental health disorders—outweigh any short-term military gains. Studies link conflict to increased mortality, chronic illnesses, and mental health disorders.^11,19^ We advocate for health to be prioritized as a fundamental right during conflicts; protecting human rights and post-conflict resilience. To reduce casualties and rebuild trust, we invite the international community, policy-makers, and humanitarian agencies to act immediately on these tailored priorities (Figure).
**
Iran’s experience highlights the broader global health challenges posed by war. It reveals how marginalizing health and humanitarian concerns in politics yields lasting consequences. Ukraine and Gaza show neglect harms nations and health systems worldwide through globalization. Enforcing frameworks, enabling agile financing, and prioritizing health in sanctions can mitigate harm. The principles of the GHPI must become enforceable policy—health is a fundamental right that must be protected.
Conclusion
Health is a fundamental right that must not be subordinated to political agendas. The international community has the tools and obligation to protect health systems through three concrete actions. First, enforce health neutrality in conflict with robust multilateral mechanisms: the WHO, with the UN Security Council, should monitor attacks on medical facilities per WHA65.20, and the ICRC is expected to establish protected health zones around treatment centers. Second, sanctions must exempt essential medicines and equipment; the UN should reform policies to ensure uninterrupted humanitarian access, overseen by an independent body such as the Global Health Cluster. Emergency funds from the World Bank and WHO should bypass sanctions for health-infrastructure repairs. Third, mental health needs to be integrated into all humanitarian responses, scaling WHO programs with local health authorities to train workers in psychological first aid, especially in border regions; UNHCR and UNICEF must prioritize mental health services in displacement settings.
Iran’s resilient healthcare system and its dedicated health workers demonstrates that health can unify communities if supported by targeted international action.
In a world where nationalism often overwhelms global citizenship and human rights, we urge the international community to prioritize future generations over short-term gains. By incorporating a health-first perspective into conflict resolution and peacebuilding, we hope that tomorrow’s world can be built on pillars of human dignity and sustainable prosperity. Accountability for leaders is essential. To global health policy-makers, we emphasize: integrate conflict-sensitive health planning into emergency preparedness; ensure sanctions never obstruct humanitarian access to medicines and supplies; invest in scalable mental health infrastructure for war-affected populations; and uphold the neutrality of health systems in international law and diplomatic practice. Global governance must protect civilian health in practice.
Disclosure of artificial intelligence (AI) use
We used AI tools to enhance the readability and grammatical accuracy of this work. Specifically, we employed Microsoft Copilot with the prompt: “Please revise the text below grammatically,” and DeepSeek-V3 with the prompt: “Please shorten the text below,” to refine our initial draft. These tools were used for improving clarity, conciseness, and grammatical precision.
Ethical issues
Not applicable.
Conflicts of interest
Authors declare that they have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martini M Valchi L Massaro E Parrella R Orsini D War and health: the devastating impact of conflict on wellbeing and humanitarian crises J Prev Med Hyg 2024653 E 464E 46810.15167/2421-4248/jpmh 2024.65.3.341239758762 PMC 11698113 · doi ↗ · pubmed ↗
- 2Aftab News. [Announcement of Exact Figures of Martyrs and Wounded in the 12-Day War with Israel]. 2025. https://aftabnews.ir/004Cf O. Accessed July 16, 2025.
- 3Shahraranews. The Latest Accurate Statistics of Martyrs and Wounded in the 12-Day War. 2025. https://shrr.ir/001Rjt. Accessed July 14, 2025.
- 4Ministry of Health and Medical Education. [Announcement No. 5 of the Crisis Information Headquarters of the Ministry of Health and Medical Education]. 2025. https://behdasht.gov.ir/Zhn Po.
- 5Mac Donald A. Israeli Strike Damages Hospital in West Iran as Mutual Attacks Kill Dozens. Middle East Eye; 2025. https://www.middleeasteye.net/news/israeli-strike-damages-hospital-west-iran-mutual-attacks-kill-dozens. Accessed June 16, 2025.
- 6World Health Organization (WHO). WHO’s Response, and Role as the Health Cluster Lead, in Meeting the Growing Demands of Health in Humanitarian Emergencies. Geneva: WHO; 2012. https://apps.who.int/gb/ebwha/pdf_files/wha 65/a 65_r 20-en.pdf.
- 7World Health Organization (WHO). Attacks on Health Care Initiative. WHO; 2020. https://www.who.int/news-room/questions-and-answers/item/attacks-on-health-care-initiative. Accessed September 21, 2025.
- 8Yazdi-Feyzabadi V Zolfagharnasab A Naghavi S Behzadi A Yousefi M Bazyar M Direct and indirect effects of economic sanctions on health: a systematic narrative literature review BMC Public Health 2024241224210.1186/s 12889-024-19750-w 39154171 PMC 11330615 · doi ↗ · pubmed ↗