The role of interleukin-17 inhibition in systemic lupus erythematosus—paradoxical hindrance or new therapeutic potential? Results from a systematic literature review and mendelian randomization
Deepak Nagra, Benjamin Zuckerman, Joy Odia, Samir Patel, Melissa Ong, Maryam Adas, Zijing Yang, Katie Bechman, Mark Russell, Sijan Bhandari, Chamith Rosa, Siwalik Banerjee, Tim Blake, Nicola Gullick, Ganesh Kasavkar, Chris Wincup

TL;DR
This study explores whether blocking interleukin-17 could help treat lupus or cause it, based on a review of clinical cases and trials.
Contribution
The paper provides a systematic review and analysis of IL-17 inhibition's potential therapeutic role in SLE and its paradoxical risks.
Findings
No new-onset SLE was reported in clinical trials of IL-17 inhibitors in non-SLE indications.
A few case reports suggest IL-17 inhibitors may be effective in treating active SLE symptoms.
Patients with drug-induced lupus generally recover after stopping IL-17 inhibitors.
Abstract
Systemic lupus erythematosus (SLE) is a disease with few licensed drugs when compared to rheumatoid arthritis, axial spondyloarthropathies, and psoriatic arthritis. We report on results of a systematic literature review of IL-17i in SLE with appraisal of published cases of both efficacy of treatment and the risk of developing new SLE following treatment with IL-17i through investigation of adverse events in the setting of clinical trials of IL-17i in non-SLE indications. We performed a PubMed, EMBASE, and MEDLINE search from inception till 30 June 2025 for case reports of IL-17i–induced SLE. The four EMA-licensed IL-17 inhibitors secukinumab, bimekizumab, brodalumab, and ixekizumab were included for analysis. All four monoclonal antibodies block IL-17A, with bimekizumab having the dual functionality of blocking IL-17A/F. Furthermore, the clinical trial data for secukinumab in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
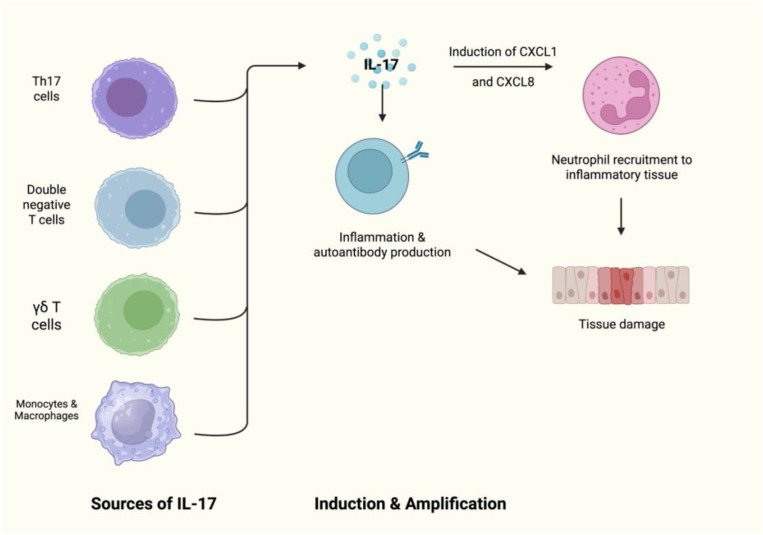 Figure 1
Figure 1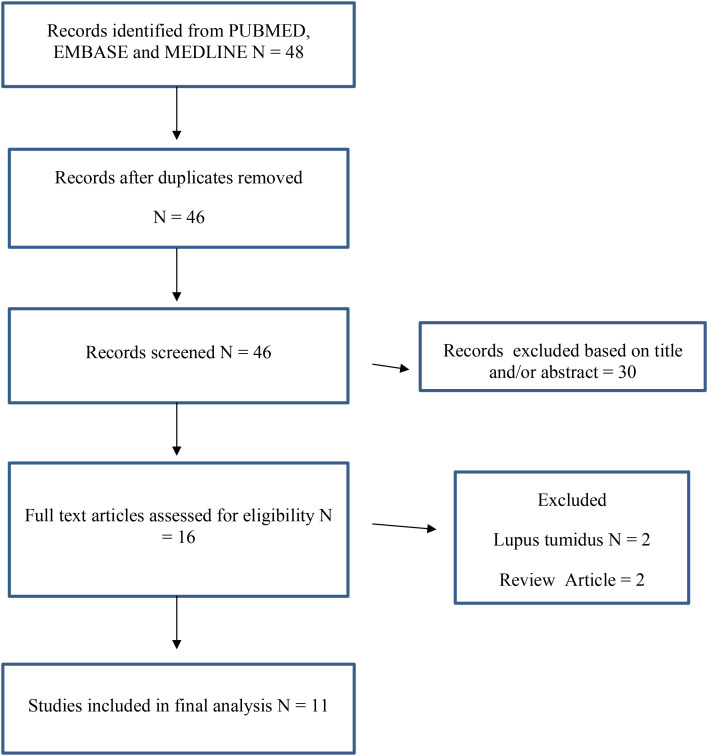 Figure 2
Figure 2| SLE patients treated with IL-17i | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | IL-17i | IL-17 indication | Gender | Age | Ethnicity | SLE phenotype | Antibody profile | Biopsy | Exposure length | Management | Notes |
| Costa 2021 ( | Secukinumab | Lupus Nephritis class 4 | Female | 29 | Unknown | Arthritis, Raynaud’s, photosensitivity, malar rash, alopecia | Low C3/C4, dsDNA, ANA | Renal | 8 | Secukinumab. Previous therapy hydroxychloroquine 400mcg, azathioprine, leflunomide, methotrexate, thalidomide, rituximab, mycophenolate, IVIG and belimumab | Complete remission after 8 months of treatment with normalisation of proteinuria. |
| Dai 2023 ( | Secukinumab | Psoriasis | Female | 23 | China | Arthritis | ANA, dsDNA, RNP, rheumatoid factor, Cardiolipin IgG, anti-glycoprotein antibody | Nil | 1 | Secukinumab | Reduction in dsDNA by 50% and normalisation of CRP and symptoms. |
| Satoh 2018 ( | Secukinumab | Psoriasis | Female | 62 | Japan | Cutaneous, alopecia, anasarca, lupus nephritis | ANA, dsDNA, low C3/C3 | Renal and skin | 1 | Secukinumab 300mg weekly. Previous MMF, prednisolone, cyclophosphamide | Resolution after 45 weeks. Flow cytometry revelated elevate CD38, CCR6 suggesting TH17 involvement. Renal biopsy showed lymphocytic infiltration with IL-17. |
| Sato 2020 ( | Secukimumab | Psoriatic arthritis | Male | 36 | Japan | Arthritis, cutaneous, lupus nephritis | ANA, dsDNA, beta-glycoprotein antibodies | 2 | Secukinumab 300mg weekly. Previous methotrexate. | Normalisation of CRP and ESR. dsDNA did not normalise. | |
| Author ( Year) / JBI Domain | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Costa 2021 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Dai 2023 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Satoh 2018 ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Sato 2020 ( | Yes | Unknown | Yes | Yes | Yes | Yes | Yes | No | Moderate |
| Author (Year)/ JBI Domain | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Ang 2021 | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Moderate |
| Avila-Riberiro 2023 ( | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Chatzimichai 2020 ( | Yes | No | Yes | No | Yes | No | Yes | Yes | Moderate |
| Conforti 2020 ( | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Hu 2024 | Yes | No | Yes | No | Yes | No | Yes | Yes | Moderate |
| Kaler 2021 ( | No | Yes | No | No | No | No | Yes | Yes | High |
| Louise Koller 2021 | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Moderate |
| Paradoxical reactions to IL-17i | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | IL-17i | IL-17 indication | Gender | Age | Ethnicity | SLE phenotype | Antibody profile | Biopsy | Exposure length | Management | Notes |
| Ang 2021 ( | Brodalumab | Psoriasis | Male | 51 | Caucasian | Ulcer,rash | ANA, dsDNA, Ro/LA | Skin | 5 | Discontinuation of Il-17A | |
| Avila-Riberiro 2023 ( | Secukinumab | Psoriatic arthritis | Male | 68 | Unknown | Arthritis, pleural effusion, pulmonary embolus and lupus nephritis | Low c3, ANA, dsDNA | Nil | 4 | Discontinuation with 0.5mg/kg prednisolone, hydroxychloroquine, enoxaparin, enalapril, mycophenolate | Remission after 33 months |
| Chatzimichai 2020 ( | Secukinumab | Psoriasis | Male | 39 | Caucasian | Cutaneous, arthritis, | ANA | Skin | 2 | Discontinuation, mometaose furoate | Clinical response after 8 weeks |
| Conforti 2020 ( | Secukinumab | Psoriasis | Male | 62 | Caucasian | Cutaenous | ANA, SSA/Ro, antihistone antibodies | Skin | 1 | Hydroxychloroquine, topical clobetasol propionate | Clinical improvement after 45 days |
| Hu 2024 ( | Secukinumab | Psoriasis | Male | 57 | Chinese | Lupus nephritis (membranous) | SSA, PM-Scl | Renal | 2 | Cessation of IL-17A, tacrolimus 1mg od switching to cyclosporine 100mg od and belimumab 600mg with prednisolone 15mg, hydroxychloroquine 200mg. | |
| Kaler 2021 ( | Secukinumab | Psoriasis | Female | 58 | Unknown | Cutaneous | n/a | Skin | 8 | Cessation of IL7i | |
| Louise Koller 2021 ( | Secukinumab | Ankylosing spondylitis | Male | 40 | Caucasian | Pericardial effusion, arthritis | ANA, dsDNA | n/a | 1 | 15mg prednisolone, cessation of IL-17A. and transition to adalimumab | B27 negative, previous TNFi 24 months prior to IL-17. Remission after 4 months with dsDNA and ANA negative after 15 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpondyloarthritis Studies and Treatments · Systemic Lupus Erythematosus Research · Rheumatoid Arthritis Research and Therapies
Introduction
1
Systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease defined by anti-nuclear antibody (ANA) positivity, with common manifestations being arthritis, malar rash, nephritis, pleural effusions, and in more severe cases, central nervous system involvement.
Targeted treatments in SLE have primarily focused on B cells through the use of rituximab and, more recently, obinutuzumab; however, additional inflammatory cytokines may be potential therapeutic targets. In comparison to other rheumatic diseases, such as rheumatoid arthritis, axial spondyloarthropathies, and psoriatic arthritis, SLE has few licensed therapies. Given that the pathogenesis of the disease involves abnormal activation of both the innate and adaptive immune responses, there are several potential targets for therapeutic intervention. The development of targeted treatments in SLE has primarily focused on B cells, such as those directed against CD20 (rituximab and obintuzumab) and BAFF inhibition (belimumab). More recently, targeting the type 1 interferon receptor has shown efficacy in active disease, with anifrolumab achieving primary endpoints in clinical trials. However, other cytokine targets, including interleukin-17 (IL-17), remain a possible option to target in SLE.
A number of T-cell subsets produce IL-17, including Th17 cells. IL-17 is a key cytokine involved in autoimmunity and inflammation, with serum IL-17A being increased in those with SLE (1). Furthermore, tissue deposition of IL-17 has been found in kidney and skin biopsy samples in those with SLE (1). IL-17 combined with BAFF is involved in the survival of B cells and their differentiation (2) (Figure 1). Inhibition has been explored in SLE with limited success. IL-17 has been proposed as a key mechanism in the pathogenesis of SLE and therefore is an ideal potential target for therapy (2).
The role of IL-17 in B-cell survival and differentiation.
The SELUNE trial (NCT05232864) for lupus nephritis was terminated early due to futile results of the interim analysis of the core study. Initially, 275 patients were randomized to receive secukinumab 300 mg or placebo. Amongst the 137 patients receiving secukinumab, only 24% of patients met the primary response with a reduction in proteinuria to under 0.5 mg over 24h, maintaining a glomerular filtration rate of over 60 ml/min, and treatment continuation with no corticosteroid use. In comparison, this was achieved by 36.3% of the placebo group. In a further sub-study analysis of 33 patients, no viable conclusion could be sought on the efficacy of secukinumab (3). In addition, a single trial in discoid lupus was also withdrawn (NCT03866317) (4) without the reason being publicly available. There is limited evidence provided by a small number of case reports describing the use of secukinumab (an IL-17i) in SLE and other systemic autoimmune rheumatic diseases (5).
In parallel paradoxical reactions (onset of disease from a medicine that treats the disease), sarcoidosis and psoriasiform reactions are well-known phenomena amongst IL-17 inhibitors (6, 7). Mechanistically, these reactions are felt to be potentially explained due to epigenetic, genetic (HLA class 2 genes), and T cell–mediated factors (8). Drug-induced lupus, another phenomenon occurring from T-cell disruption, has been widely described for decades. Amongst the monoclonal antibodies, only tumor necrosis factor inhibitors (TNFi) have had an association with drug-induced SLE to date.
There is currently a significant unmet need and major uncertainty relating to the potential role of IL-17 inhibition in the treatment of SLE, and further knowledge is required relating to the potential induction of other immune phenomena in the setting of treatment with drugs that target IL-17, including secukinumab. Herein, we report on the results of a systematic literature review of IL-17i in SLE with an appraisal of published cases of both the efficacy of treatment and the risk of developing new SLE. Further, we evaluated the incidence of new-onset SLE in case reports of patients treated with IL-17 inhibitors for non-SLE indications and also the risk of worsening SLE symptoms in the setting of patients who have been treated with IL-17i for off-label indications.
To date, ixekiuzumab, secukinumab, and bimekizumab are licensed by both the FDA and EMAI for the treatment of psoriasis, psoriatic arthritis, and axial spondylarthritis. Brodalumab is only licensed for psoriasis and psoriatic arthritis.
Methods
2
Systematic literature review
2.1
Database, sources, eligibility, and data extraction
2.1.1
We performed a PubMed, EMBASE, and MEDLINE search from inception until 30 June 2025 for case reports of IL-17i–induced SLE [PRISMA, Figure 2 (9)]. The four EMA-licensed IL-17 inhibitors secukinumab, bimekizumab, brodalumab, and ixekizumab were included for analysis. All four monoclonal antibodies block IL-17A, with bimekizumab having the dual functionality of blocking IL-17A/F. The review was registered on PROSPERO (ID 1243558).
PRISMA.
The search terms used were secukinumab, bimekizumab, brodalumab, ixekizumab, interleukin-17 inhibitor, IL-17, IL-17 inhibitor, IL-17i, SLE, and lupus.
Furthermore, the clinical trial data for secukinumab in psoriasis, psoriatic arthritis, and axial spondylarthritis from inception until 2024 were reviewed for adverse event reporting of new cases of SLE. Both systemic and cutaneous SLE were reported on. We also reported on case reports of the use of secukinumab in the treatment of SLE (10). Data collection was performed by four reviewers (DN, MA, JO, and MO), and discrepancies were resolved with a fifth reviewer (CW).
Data analysis & selection criteria
2.1.2
Descriptive statistics were used to calculate frequency and percentages amongst the data, with reporting on continuous variables as median and interquartile range (IQR) or mean (SD) as appropriate.
The definitions of paradoxical reaction when compared to drug-induced lupus or new-onset SLE were used as per individual authors from the case reports.
Risk of bias
2.1.3
Two authors (D.N. and B.Z.) independently reviewed the data for risk of bias using the Joanna Briggs Institute (JBI) tool for critical appraisal of case reports & series (11) (Tables 1, 2). The Cochrane risk of bias 2 (ROB2) score was used for randomized controlled trials. Any discrepancies were discussed with a third reviewer (C.W.).
Ethics
2.1.4
No ethical approval was required for this project; data were collected from published material. No patient identifiable data were requested or collected.
Mendelian randomization
2.1.5
Two sample Mendelian randomization was used to assess the association between IL-17 proteins and SLE. Genetic associations for SLE were identified from the largest genome-wide association study of 4,036 cases and 6,969 controls (12). Ethical approval had been obtained in all original studies, with relevant citations detailed. Genetic proxies for IL-17 proteins (A, C, D, F, receptor A, and receptor B) were identified from 54,306 participants in the UK Biobank Pharma Proteomics Project (13). Single-nucleotide polymorphisms within 200 kb of each gene, which encodes the relevant protein, were selected, and thresholds of p-value < 5 × 10^−6^ and r^2^ < 0.1 were incorporated. The strength of the instrument was evaluated through F-statistics estimation using beta^2^/standard error^2^ (F > 10 suggests minimal weak instrumental bias). We used the two-sample MR Wald ratio, inverse-variance-weighted, to estimate a weighted average of individual variant estimates. Pairwise conditional colocalization was performed to assess genetic confounding through linkage disequilibrium. Bonferroni corrections were applied to account for multiple comparisons. Analyses were performed in R using the TwoSampleMR and coloc packages.
Results
3
Clinical efficacy of IL-17i in case reports of active SLE
3.1
In the case of patients treated with secukinumab for known active SLE (10, 14–16) outside of the clinical trial setting (10, 14–16) (n = 4), the average age at time of treatment initiation was 32.5 years old (IQR 26–49), and 75% of those treated were female. The most frequent indication for the use of secukinumab was active cutaneous disease and inflammatory arthritis (75%, n = 3), with a further case treated for lupus nephritis. All four patients had positive antinuclear antibodies (ANA) and anti-dsDNA antibodies (Table 3). One limiting factor amongst these case reports was that response was not defined as either DORIS or Lupus Low Disease Activity State (LLDAS). Response was also not confirmed using conventional validated disease activity scores (e.g., SLEDAI-2K or BILAG) but instead disease inactivity was reported in terms of clinical and biochemical parameters. A median drug exposure time of 6.5 weeks (IQR 5-14) was needed to achieve remission (defined as resolution of symptoms).
The risk of bias amongst these reports was low to moderate, with initial clinical details and serology and histology reports partially missing from the case reports (Table 1).
New-onset SLE following IL-17i in the literature
3.2
Amongst 56 clinical trials for secukinumab, there have been no reports of drug-induced or new-onset SLE following treatment in the reporting periods for each respective trial (n = 12,637). To date, there are no case reports of bimekizumab- or ixekizumab-induced SLE, although two case reports for ixekizumab-induced lupus tumidus were identified and were excluded from this analysis. One case report existed for new-onset SLE in a patient undergoing treatment with brodalumab for psoriasis, and six case reports of SLE following initiation of secukinumab were identified (14, 17–22). The cases are summarized in Table 2.
Among those in whom secukinumab and brodalumab were associated with new-onset SLE (n = 7), the average age was 57 years (IQR 40–62); 86% were male, and the exposure length was 10 weeks from post-initiation of therapy to the time of onset of symptoms (IQR 8–20). One patient had anti-histone antibodies (six patients did not have anti-histone antibodies present). Among the cases with negative anti-histone antibodies, the diagnosis of SLE was supported through histological findings, a positive ANA or dsDNA, and low complement. Six patients had IL-17i for plaque psoriasis, with one patient for axial spondylarthritis. The most common lupus manifestations were cutaneous lesions and inflammatory arthritis. Biopsies of cutaneous lesions were performed in four patients. The features of the biopsy samples were dermal inflammatory infiltrate of lymphocytes and increased mucoid ground substances. Lupus nephritis was confirmed on renal biopsy in one patient who had proteinuria (5.25 g/24h) with thickened glomeruli and staining of IgG, IgM, IgA, and C3, seen as a full-house pattern in keeping with a class 3 membranous nephritis. In all cases, IL-17i therapy was stopped as part of the management to ensure the offending agent did not cause further clinical deterioration. All patients had resolution of their symptoms.
The risk of bias amongst these case reports was generally low, with only one report scoring moderate risk of bias (Sato, 2020) as there was limited exposure time and historical detail of the patient provided (Table 4).
Results of Mendelian randomization
3.3
Of the selected proteins, IL-17A did not have a valid protein quantitative trait locus and was excluded from the analysis. The F-statistic for all other proteins was > 10. Only genetically predicted IL-17D demonstrated an association with SLE: odds ratio 1.17 per standard deviation increase in IL-17D levels (95% confidence interval [CI]: 1.04–1.32, p = 0.007). However, co-localization analyses showed a conditional posterior probability of 6% for a shared causal variant. It is unlikely that the same genetic variant is driving both the increased IL-17D levels and the risk of SLE. This low probability of co-localization suggests that the observed association might be due to genetic confounding rather than a direct causal relationship, meaning that different genetic variants could be influencing IL-17D levels and SLE risk independently.
Discussion
4
Herein, we present seven case reports of IL-17i–induced SLE, alongside four cases of SLE managed with IL-17i, supplemented by additional safety data from wider IL-17i clinical trials, supporting that IL-17i–induced SLE remains a rare entity. This is the first such review collating the evidence base of current IL-17i use in SLE and addressing safety and practical implications for its use in SLE.
Despite a limited number of case reports linking the onset of SLE to the initiation of IL-17 inhibitors, these drugs remain a potential therapeutic option for SLE, particularly for cutaneous and articular manifestations. In cases where de-novo SLE symptoms developed after starting IL-17 inhibitors, all patients fully recovered upon discontinuation of the drug. This outcome aligns with many cases of drug-induced lupus, where discontinuation of the offending drug and symptomatic management are typically sufficient for recovery (23). However, genetic assessment using Mendelian randomization (MR) was unable to clarify the role of IL-17 in the pathogenesis of SLE, due to challenges such as weak instrument bias and genetic confounding (24).
Furthermore, publication bias may lead to positive reports of IL-17i use in SLE being captured, but in parallel there may be reports not available in the literature. Incomplete follow-up in the reported cases affects the interpretation and significance of the reports, and combined with the few reports, precludes subgroup analysis within this review. The risk of bias amongst those who developed SLE was overall moderate compared to those treated with IL-17i for SLE, which was low. Although heterogeneity was not formally assessed, the case reports had a diverse range, ethnicity pool with a mix of different phenotypes of SLE.
The efficacy of IL-17i for use in SLE remains unclear due to the limited data from published case reports. Amongst the case reports included here, there was significant heterogeneity in the reporting of disease activity, with no standardization or use of classic disease activity metrics or response criteria described. This means that the interpretation of these results for wider subtypes of patients with SLE is challenging, particularly with regards to validating the findings of these studies. Short follow-up periods following treatment and lack of control in terms of concurrent therapies similarly hinder the appraisal of the efficacy of secukinumab in this disease area.
Further limitations fall into safety and the definitions of new-onset SLE. It is unclear from the evidence provided as to whether these are truly paradoxical reactions or episodes of drug-induced lupus. It is difficult to evaluate if this is truly new SLE (i.e., lack of reporting on fulfilment of EULAR/ACR classification criteria (25)) and it is unclear if the paradoxical reaction similar to that seen in TNF/drug-induced lupus is due to lack of reporting of anti-histone antibodies and other markers (26). The definition of remission was heterogeneous amongst the case reports, with the absence of SLEDAI and BILAG scores in the reports (27, 28).
Amongst the limitations directly related to Mendelian randomization, our analysis was limited by the absence of a validated pQTL for IL-17A, meaning we relied on eQTLs that may not accurately reflect circulating IL-17A protein levels and increase susceptibility to genetic confounding. Additionally, the lack of co-localization between IL-17A expression signals and SLE risk reduces confidence that both are driven by the same causal variant, weakening causal inference.
To date, serum IL-17 levels have been shown to correlate with SLE disease activity in a directly proportional fashion. In a study of 36 patients with SLE with a wide variety of phenotypes, IL-17 levels were found to be higher in those with renal and central nervous system disease (29). Animal models have demonstrated similar results with increased IL-17 but also IL-10 signatures in those with increased SLE activity (30). In a further study isolating patients with lupus nephritis alone, serum IL-17 levels were found to be higher with disease activity amongst those with class 3, 4, and 5 nephritis (31).
It is also important to consider that IL-17 belongs to the same immunological axis as IL-12/23, with IL-23 known to have a role in stimulating Th17 cells (32). A previous phase 2 trial of ustekinumab (LOTSUS), an IL-12/23 inhibitor for treating SLE (n = 166), showed promise for use in the management of SLE with no safety concerns (33). However, in the phase 3 trial, the interim efficacy data did not demonstrate a significant difference and the trial was discontinued following the analysis due to inefficacy. As is the challenge with many clinical trials in SLE, possible reasons for the failure to meet primary endpoints have been suggested due to small sample sizes, short follow-up durations and placebo response rates (34).
Given the initial positive response from the phase 2 trials on IL-12/23 inhibition in SLE, the question remains as to whether IL-17 inhibition would be of more value in the treatment paradigm for SLE. Serum IL-17 has shown to be present in higher concentrations than IL-12 and 23 in those with SLE (32, 35, 36). With 92 investigational products currently in clinical trials for SLE, IL-17 inhibition remains a potential therapeutic target (37). The current phase 3 SELUNE trial for lupus nephritis (NCT04181762) commenced in 2020 with an estimated 460 participants enrolled, for which the results are due to be published in 2026. The results from this randomized controlled trial will pave the future for whether IL-17 truly has therapeutic potential in SLE.
To date, IL-17i has been primarily used for those with skin and joint disease rather than those with pleural, renal, or SLE affecting the central nervous system (38). In those patients with SLE who are managed with IL-17i, we would suggest some practical points in monitoring with regular serology and urinary protein levels being quantified to assess for worsening disease. The risk of developing SLE from IL-17i exposure based on the literature remains low, with the benefit of using IL-17i to control inflammatory disease and thereby reducing cardiovascular risk with controlled disease, and an improved quality of life equates to IL-17i being a viable option in such selected cases (39)f.
In conclusion, the role of IL-17i in SLE is an area for further investigation (40). As with many targeted therapies in SLE, improvements in scientific research are needed to better understand the role of IL-17 in the pathogenesis of SLE and in which subgroups IL-17i may be effective. Dedicated studies and immunologically stratified trials of clinical efficacy are needed to better understand if there is a role for IL-17i in SLE.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koga T Ichinose K Kawakami A Tsokos GC . Current insights and future prospects for targeting IL-17 to treat patients with systemic lupus erythematosus. Front Immunol. (2020) 11:624971. doi: 10.3389/fimmu.2020.624971, PMID: 33597953 PMC 7882681 · doi ↗ · pubmed ↗
- 2Li D Guo B Wu H Tan L Chang C Lu Q . Interleukin-17 in systemic lupus erythematosus: A comprehensive review. Autoimmunity. (2015) 48:353–61. doi: 10.3109/08916934.2015.1037441, PMID: 25894789 · doi ↗ · pubmed ↗
- 3Zhao MH Cons Molina F Aroca G Tektonidou MG Mathur A Tangadpalli R . Secukinumab in active lupus nephritis: Results from phase III, randomised, placebo-controlled study (SELUNE) and open-label extension study. Rheumatol (Oxford). (2025). doi: 10.1093/rheumatology/keaf 536, PMID: 41092316 PMC 12862366 · doi ↗ · pubmed ↗
- 4Lichtnekert J Anders HJ Lech M . Lupus nephritis: current perspectives and moving forward. J Inflammation Res. (2022) 15:6533–52. doi: 10.2147/JIR.S 363722, PMID: 36483271 PMC 9726217 · doi ↗ · pubmed ↗
- 5Strunz PP Labinsky H Nagler LK Portegys J Froehlich M Gernert M . Case Report: Effectiveness of secukinumab in systemic sclerosis with early skin progress after autologous hematopoietic stem cell transplantation and end-stage kidney disease. Front Immunol. (2023) 14:1294496. doi: 10.3389/fimmu.2023.1294496, PMID: 38045701 PMC 10693324 · doi ↗ · pubmed ↗
- 6Cohen Aubart F Lhote R Amoura A Valeyre D Haroche J Amoura Z . Drug-induced sarcoidosis: an overview of the WHO pharmacovigilance database. J Intern Med. (2020) 288:356–62. doi: 10.1111/joim.12991, PMID: 31612562 · doi ↗ · pubmed ↗
- 7Singla S Luz D . Paradoxical psoriasis with IL-17 inhibitors. Rheumatol Adv Pract. (2024) 8:rkae 082. doi: 10.1093/rap/rkae 082, PMID: 39026520 PMC 11257715 · doi ↗ · pubmed ↗
- 8Toussirot E Aubin F . Paradoxical reactions under TNF-alpha blocking agents and other biological agents given for chronic immune-mediated diseases: an analytical and comprehensive overview. RMD Open. (2016) 2:e 000239. doi: 10.1136/rmdopen-2015-000239, PMID: 27493788 PMC 4964220 · doi ↗ · pubmed ↗