Case Report: Extracorporeal membrane oxygenation in acute coronary syndrome: a rare case of massive left ventricular thrombus
Jian Lan, Yifeng Mao, Chenyang Shi, Jian Ye, Qiang Zhong, Jingjing Li, Xijiang Zhang, Cheng Zheng

TL;DR
A 42-year-old man on VA-ECMO developed a massive heart blood clot despite anticoagulation, highlighting the risks and management challenges in such cases.
Contribution
This case report highlights the rapid formation of a massive left ventricular thrombus in VA-ECMO patients and suggests improved anticoagulation and unloading strategies.
Findings
A massive left ventricular thrombus formed within 14 hours despite therapeutic anticoagulation.
The patient developed refractory multi-organ failure, leading to withdrawal of care.
The case emphasizes the need for multimodal anticoagulation monitoring and advanced LV unloading strategies.
Abstract
Left ventricular (LV) thrombus is a catastrophic complication during veno arterial-extracorporeal membrane oxygenation (VA-ECMO) support for cardiogenic shock, arising from a confluence of hemodynamic stasis, a prothrombotic state, and potential limitations of conventional anticoagulation monitoring. A 42-year-old man with acute inferior-wall ST-elevation myocardial infarction developed refractory cardiogenic shock during percutaneous coronary intervention, necessitating VA-ECMO initiation. Dual antiplatelet therapy and systemic heparinization (targeting an activated partial thromboplastin time of 50–80 s) were maintained. Despite therapeutic anticoagulation, serial echocardiography documented the formation of a massive LV thrombus occupying >90% of the cavity within a 14 h interval on the fourth day of ECMO support. The patient subsequently deteriorated into refractory multi-organ…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
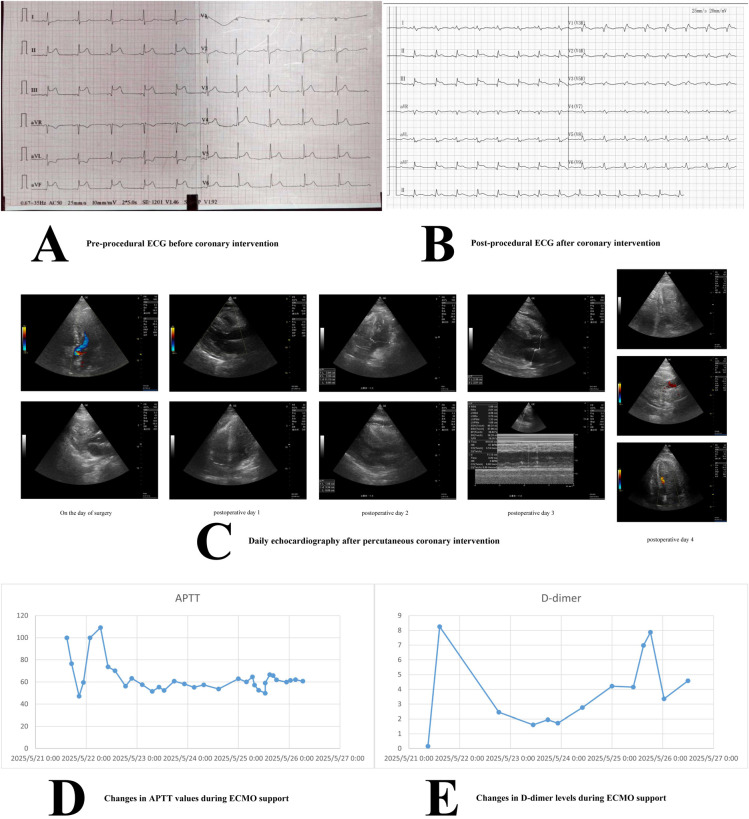 Figure 1
Figure 1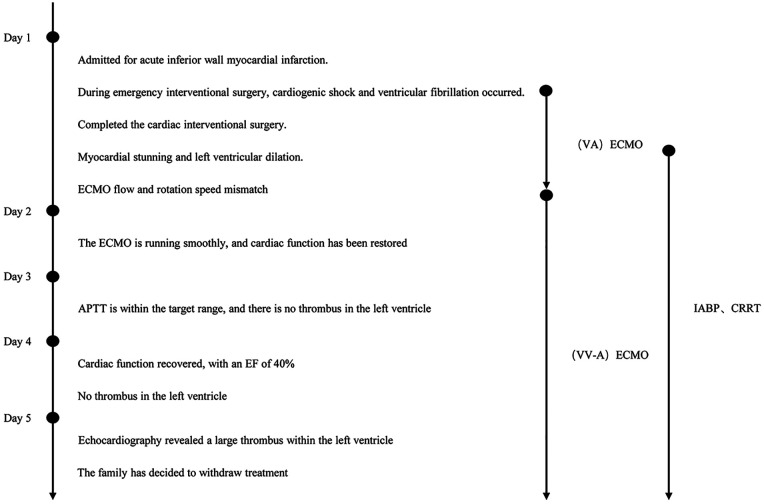 Figure 2
Figure 2- —Science and Technology Plan Project of Taizhou10.13039/501100018552
- —Medical Science and Technology Project of Zhejiang Province10.13039/501100017594
- —Zhejiang Traditional Chinese Medicine Administration10.13039/501100012175
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Heparin-Induced Thrombocytopenia and Thrombosis · Acute Myocardial Infarction Research
Introduction
1
Extracorporeal membrane oxygenation (ECMO) serves as a pivotal salvage therapy for patients with refractory cardiogenic shock and respiratory failure, offering temporary cardiopulmonary support (1, 2). Despite its life-saving potential, ECMO is fraught with complications, among which thrombotic and hemorrhagic events are the most frequent and challenging to manage, with reported thrombosis rates as high as 52% (3). Left ventricular (LV) thrombus formation during veno-arterial (V-A) ECMO represents one of the most devastating thrombotic complications, carrying a mortality rate that approaches 100% in published series (4). Reported in up to 5% of VA-ECMO cases, its fulminant presentation in the early phase of support is particularly ominous and may be under-recognized (5). This case report describes the rapid development of a massive, near-total LV thrombus in a patient on VA-ECMO for post-infarction cardiogenic shock, despite conventional anticoagulation. We analyze the multifactorial pathophysiology and discuss imperative refinements in monitoring and management strategies to avert this fatal complication.
Case presentation
2
Chief complaint
2.1
A 42-year-old man presented to the emergency department with sudden-onset, severe substernal chest pain lasting 40 min.
History of present illness
2.2
The patient was in his usual state of health until the onset of pain. Upon arrival, his blood pressure was 127/89 mmHg. An initial 12-lead electrocardiogram (ECG) (Figure 1A) demonstrated ST-segment elevations in leads II, III, and aVF, consistent with an acute inferior-wall ST-elevation myocardial infarction (STEMI). Point-of-care laboratory testing revealed a markedly elevated high-sensitivity troponin T level of 9.992 µg/L. Serum creatinine was 86 µmol/L. After immediate loading with aspirin (300 mg) and ticagrelor (180 mg), the patient was transferred for emergency coronary angiography.
Imaging information during the treatment course. (A) Pre-procedural electrocardiogram showing ST-segment abnormalities. (B) Post-procedural electrocardiogram with normalized ST segments. (C) Daily echocardiogram images after percutaneous coronary intervention, illustrating cardiac function changes (color Doppler and M-mode included). (D) Activated partial thromboplastin time (APTT) values during extracorporeal membrane oxygenation (ECMO) support. (E) D-dimer levels during ECMO support.
Coronary angiography revealed multi-vessel disease. The most critical lesion was a 99% stenosis in the proximal right coronary artery (RCA), which was deemed the culprit vessel. During percutaneous coronary intervention (PCI) of the RCA, the patient abruptly developed ventricular fibrillation. Prolonged advanced cardiac life support (ACLS), including endotracheal intubation, repeated defibrillation, and vasopressor infusion, was initiated. A cardiac arrest period of approximately 15–20 min preceded the establishment of adequate circulation. Due to persistent, refractory cardiogenic shock despite maximal medical therapy and return of spontaneous circulation, VA-ECMO was emergently instituted. The ECMO circuit was configured with a 21-French drainage cannula in the left femoral vein and a 17-French return cannula in the right femoral artery. An initial heparin bolus was administered, followed by a continuous infusion titrated to an activated partial thromboplastin time (APTT) target. Successful stent placement in the RCA was completed under ECMO support. The patient was then transferred to the intensive care unit (ICU) for ongoing management.
Past medical history
2.3
The patient had a 5-year history of hypertension, managed with regular antihypertensive medication (amlodipine 5 mg daily). There was no known history of diabetes, hyperlipidemia, prior cardiac events, or thromboembolic disease.
Physical examination on ICU admission
2.4
The patient was sedated, intubated, and mechanically ventilated. Vital signs under ECMO support showed a heart rate of 113 beats/min (predominantly ECMO-driven), and a respiratory rate set at 17 breaths/min. His core temperature was 36.1°C. Neurological examination was limited by sedation; pupils were equal and round (2 mm) with a sluggish light reflex. Cardiovascular examination revealed a quiet precordium with no palpable heaves. Heart sounds were distant; no murmurs, rubs, or gallops were audible. Bilateral coarse breath sounds were noted on lung auscultation. The abdomen was soft and non-tender. There was no peripheral edema.
Laboratory studies
2.5
Admission laboratory values were notable for a white blood cell count of 9.90 × 10^9^/L, platelet count of 283 × 10^9^/L, and C-reactive protein of 1.50 mg/L. Coagulation profile showed an APTT of 22.6 s and a D-dimer of 0.15 mg/L. Arterial blood gas on ICU admission revealed severe metabolic acidosis: pH 7.32, PaCO_2_ 26 mmHg, PaO_2_ 145 mmHg, base excess −11.1 mmol/L, lactate 13.6 mmol/L.
Imaging studies
2.6
The admission ECG was diagnostic for acute inferior ST-elevation myocardial infarction (Figure 1A). A follow-up ECG obtained post-intervention upon ICU admission showed improvement (Figure 1B). A concurrent bedside transthoracic echocardiogram revealed severe global left ventricular systolic dysfunction with marked chamber dilation and a severely reduced left ventricular outflow tract velocity-time integral of 9 cm/s. No intracardiac mass or thrombus was identified at this initial assessment.
Hospital course and management
2.7
Post-procedure management included continuation of dual antiplatelet therapy (aspirin and ticagrelor) and titration of the heparin infusion to maintain an APTT between 50 and 80 s. Two hours after ICU admission, the patient became anuric. Acute kidney injury progressed rapidly (creatinine rising to 143 µmol/L), necessitating the initiation of continuous renal replacement therapy (CRRT) connected in parallel to the ECMO circuit.
Four hours after ECMO initiation, the patient continued to exhibit a markedly low pulse pressure (<10 mmHg). Repeat transthoracic echocardiography (TTE) revealed persistent left ventricular distension, poor ejection, and an absence of aortic valve opening. In response, the ECMO pump speed was decreased to reduce left ventricular afterload, and an intra-aortic balloon pump (IABP) was inserted via the left femoral artery and set to 1:1 counter-pulsation to promote forward flow. These interventions led to a modest reduction in vasopressor requirements.
Approximately five hours after the PCI procedure, the ECMO flow began to decline despite stable circuit pressures. A systematic evaluation was undertaken: physical examination ruled out cannula dislodgement or kinking, clinical assessment and hemodynamic parameters suggested adequate volume status, and echocardiography excluded pericardial tamponade. With common causes of low flow addressed, inadequate venous drainage was suspected. To augment drainage, a second drainage cannula was placed in the right internal jugular vein, converting the circuit to a veno veno-arterial (VV-A) configuration, which successfully restored flows.
Over the next three days, the patient required ongoing support with blood products, inotropes, and antibiotics for suspected nosocomial pneumonia. Serial daily TTEs from post-operative days 1–3 showed some improvement in LV filling, with an estimated ejection fraction reaching 40% by day 3, and no evidence of intracardiac thrombus (Figure 1C). Vasopressor support was gradually weaned, and the intensity of IABP and ECMO support was cautiously reduced, though not discontinued.
On the morning of post-operative day 4, a routine bedside TTE was performed approximately 14 h prior to the subsequent catastrophic event. This examination revealed reduced left ventricular systolic function with an estimated ejection fraction of approximately 40%, increased left ventricular wall thickness, structurally normal cardiac valves with adequate opening and closure, normal atrial and ventricular chamber dimensions. Crucially, no intracardiac thrombus was identified at this time (Figure 1C).
Subsequently, the patient experienced an acute, catastrophic hemodynamic collapse. An emergent bedside TTE revealed a new, massive, laminated thrombus occupying over 90% of the LV cavity, with near-complete obliteration of the ventricular lumen (Figure 1C, Supplementary Video S1). The LV ejection fraction had plummeted to approximately 15%. Review of coagulation parameters showed the APTT had been consistently within the target range of 50–80 s (Figure 1D). However, D-dimer levels had shown a significant upward trend beginning 24 h prior to thrombus detection (Figure 1E).
Faced with irreversible multi-organ failure (cardiac, renal, hepatic) and a universally poor prognosis, the family, after extensive counseling regarding the futility of further intervention and considering financial hardships, made the decision to withdraw life-sustaining therapies. The patient passed away shortly thereafter. A detailed timeline of the hospital course is presented in Figure 2.
Timeline of the treatment course.
Final diagnoses
2.8
Acute inferior-wall ST-elevation myocardial infarction, Refractory cardiogenic shock, Massive left ventricular thrombus, Multi-organ failure syndrome (cardiac, respiratory, renal, hepatic), Nosocomial pneumonia, Essential hypertension.
Discussion
3
This case presents a fulminant and fatal example of massive left ventricular thrombus complicating VA-ECMO support, a rare but devastating complication. The sheer rapidity of clot formation—developing to near-total cavity obliteration within 14 hours despite conventional anticoagulation—demands a critical re-examination of the converging pathophysiology and exposes significant limitations in current monitoring and management strategies.
An initial and crucial observation lies in the apparent discordance between the identified culprit lesion and the observed myocardial dysfunction. While angiography pinpointed a 99% proximal RCA stenosis, echocardiography revealed severe global LV systolic dysfunction with marked dilation, a pattern extending beyond the expected regional injury of an inferior MI. This suggests a multifactorial substrate. The patient's history of hypertension may have provided a background of adverse remodeling, reducing ventricular compliance and functional reserve (6, 7). The proximate 15–20 min cardiac arrest and resuscitation likely induced global myocardial stunning secondary to ischemic-reperfusion injury (8). Furthermore, in the setting of cardiogenic shock with low coronary perfusion pressure, even non-occlusive multi-vessel disease can contribute to a diffuse ischemic burden (9). Thus, the profound ventricular impairment was likely the product of a chronic substrate acutely destabilized by infarction, compounded by resuscitation-related injury and shock physiology. This created the foundational milieu—a severely dilated, hypocontractile ventricle—primed for the subsequent thrombotic catastrophe.
The thrombotic event can be pathophysiologically underpinned by Virchow's triad, encompassing endothelial injury from infarction, hemodynamic stasis within the dilated ventricle, and a clinically occult hypercoagulable state (10). The endothelial injury was initiated by the acute myocardial infarction. Stasis was dramatically potentiated by the hemodynamic effects of VA-ECMO (10). The retrograde arterial flow from the ECMO circuit increases LV afterload. In a ventricle already crippled by infarction—evidenced early on by severe dilatation and a VTI of only 9 cm/s—this elevated afterload can lead to profound distension and virtual cessation of ejection, creating a static blood pool (11–13). While our team appropriately responded to signs of LV distension by reducing ECMO flow and inserting an IABP, this case highlights the potential inadequacy of IABP as a sole unloading strategy in cases of severe ventricular dysfunction. IABP improves coronary perfusion and reduces aortic impedance but does not actively decompress the LV chamber or directly alleviate cavity stasis (14–16). For patients exhibiting such severe LV dilation and poor contractility on VA-ECMO, a more proactive approach to unloading may be warranted (17). This could involve the early use of or escalation to devices that provide direct LV decompression (18, 19).The Impella® microaxial pump, for instance, actively unloads the LV by pumping blood from the ventricle into the ascending aorta, effectively reducing ventricular volume and wall stress more definitively than IABP (20–22). Alternatively, percutaneous atrial septostomy can decompress the left heart by creating an interatrial shunt, though it may compromise oxygenation (23, 24). The decision must be individualized, but a low threshold for employing these more aggressive strategies should be considered when echocardiographic signs of persistent stasis (e.g., worsening dilation, spontaneous echo contrast) are present despite IABP support (17). In specialized centers, additional configurations such as left atrial veno-arterial (LAVA) ECMO or percutaneous pulmonary artery drainage may also be considered as alternative unloading strategies in select cases (23, 25, 26).
The third element, hypercoagulability, presents the most insidious challenge (10). Our patient maintained an APTT within the prescribed therapeutic range (50–80 s), yet developed a massive clot, illustrating the phenomenon of “heparin pseudo-adequacy”. (27, 28) This discrepancy can arise from several factors pervasive in ECMO patients. Acquired deficiency of antithrombin III (AT-III), a crucial cofactor for heparin, is common and leads to heparin resistance, rendering standard doses ineffective despite a normal APTT (29, 30). Furthermore, the APTT itself is a flawed monitor in this population; it is influenced by factor deficiencies, elevated factor VIII levels (common in critical illness), and the presence of lupus anticoagulants, all of which can distort its correlation with true heparin effect and thrombin generation (31–33). The rising D-dimer trend in our patient, though non-specific, was a biochemical red flag suggesting ongoing coagulation activation that APTT monitoring failed to capture (34, 35). This case strongly argues against sole reliance on APTT. Incorporating anti-factor Xa (anti-Xa) activity monitoring provides a more direct and reliable measure of heparin's anticoagulant effect and is less susceptible to the confounding variables that affect APTT (36). A multimodal monitoring protocol, incorporating APTT, targeted viscoelastic testing, and anti-Xa levels, alongside periodic assessment of AT-III activity in high-risk or non-responsive patients, represents a more comprehensive and rational approach to guiding anticoagulation therapy during ECMO.
This experience also informs a pragmatic approach to risk mitigation. While exhaustive thrombophilia screening (genetic and extensive phenotypic) is impractical in the emergent ECMO setting, a targeted strategy is feasible and necessary. Routine multimodal coagulation monitoring (APTT + anti-Xa) should be considered standard. Echocardiographic vigilance is paramount, with a low threshold for frequent exams in patients with dilated, poorly ejecting ventricles. LV unloading strategy must be dynamic; IABP is a reasonable first step, but its efficacy must be continuously assessed with clear criteria for escalation to more definitive unloading devices like Impella if stasis is not resolved (37).
In summary, massive LV thrombosis during VA-ECMO is not merely a rare misfortune but a potential culmination of identifiable and modifiable risk factors. This case serves as a critical reminder that conventional endpoints like APTT and supportive IABP may be insufficient guards against this complication in high-risk patients. A fundamental shifts towards early, aggressive LV unloading tailored to ventricular physiology, coupled with sophisticated, multimodal anticoagulation monitoring, is essential to improve outcomes for these critically ill patients.
Conclusion
4
We report a case of rapidly progressive, massive LV thrombus formation in a patient on VA-ECMO for post-STEMI cardiogenic shock, which proved fatal despite standard anticoagulation monitoring and IABP support. The case highlights the lethal synergy between VA-ECMO-induced ventricular stasis and an inadequately monitored prothrombotic state. It underscores the urgent need to move beyond traditional management silos by implementing proactive ventricular unloading strategies that address stasis directly and by adopting multimodal anticoagulation monitoring to ensure true therapeutic efficacy. Integrating these principles into standardized protocols for high-risk VA-ECMO patients could help prevent this devastating complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Combes A Leprince P Luyt CE Bonnet N Trouillet JL Léger P Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. (2008) 36(5):1404–11. 10.1097/CCM.0b 013e 31816 f 7cf 718434909 · doi ↗ · pubmed ↗
- 2Smedira NG Blackstone EH. Postcardiotomy mechanical support: risk factors and outcomes. Ann Thorac Surg. (2001) 71(3 Suppl):S 60–6. discussion S 82–5. 10.1016/S 0003-4975(00)02626-611265868 · doi ↗ · pubmed ↗
- 3Sklar MC Sy E Lequier L Fan E Kanji HD. Anticoagulation practices during venovenous extracorporeal membrane oxygenation for respiratory failure. A systematic review. Ann Am Thorac Soc. (2016) 13(12):2242–50. 10.1513/Annals ATS.201605-364SR 27690525 · doi ↗ · pubmed ↗
- 4Yang XT Chen YJ Zeng H Deng L Chang L Li Y Successful treatment of large left ventricular thrombosis during extracorporeal membrane oxygenation (ECMO): a case report and review of the literature. Clin Case Rep. (2025) 13(1):e 70123. 10.1002/ccr 3.7012339839947 PMC 11748204 · doi ↗ · pubmed ↗
- 5Wang YD Lin JF Huang XY Han XD. Successful treatment of veno-arterial extracorporeal membrane oxygenation complicated with left ventricular thrombus by intravenous thrombolysis: a case report. World J Clin Cases. (2023) 11(14):3323–9. 10.12998/wjcc.v 11.i 14.332337274033 PMC 10237126 · doi ↗ · pubmed ↗
- 6Yoshida Y Nakanishi K Jin Z Daimon M Ishiwata J Sawada N Association between progression of arterial stiffness and left ventricular remodeling in a community-based cohort. JACC Adv. (2023) 2(5):100409. 10.1016/j.jacadv.2023.10040938938996 PMC 11198086 · doi ↗ · pubmed ↗
- 7Saheera S Krishnamurthy P. Cardiovascular changes associated with hypertensive heart disease and aging. Cell Transplant. (2020) 29:963689720920830. 10.1177/096368972092083032393064 PMC 7586256 · doi ↗ · pubmed ↗
- 8Nakamura E Aoki T Endo Y Kazmi J Hagiwara J Kuschner CE Organ-Specific mitochondrial alterations following ischemia-reperfusion injury in post-cardiac arrest syndrome: a comprehensive review. Life (Basel). (2024) 14(4):477. 10.3390/life 1404047738672748 PMC 11050834 · doi ↗ · pubmed ↗