Intraoperative transoesophageal echocardiographic detection of guidewire malposition and incomplete valve expansion in valve-in-valve transcatheter aortic valve implantation for Trifecta bioprosthesis failure: a case report
Ken-ichi Watanabe, Nagataka Yoshihara, Hirokuni Akahori, Taichi Sakaguchi

TL;DR
A case report shows how intraoperative transoesophageal echocardiography helped correct a guidewire issue during a heart valve procedure.
Contribution
Demonstrates the critical role of real-time imaging in avoiding complications during valve-in-valve TAVI for Trifecta bioprosthesis failure.
Findings
Incomplete valve expansion occurred due to guidewire misplacement between degenerated leaflets.
Transoesophageal echocardiography enabled correction and successful valve deployment.
False procedural reassurance is a risk in ViV-TAVI for Trifecta bioprosthesis failure.
Abstract
Valve-in-valve transcatheter aortic valve implantation (ViV-TAVI) is widely used for failed surgical bioprostheses; however, procedural pitfalls remain, particularly in valves prone to early structural deterioration. An 84-year-old woman with a failed 21 mm Trifecta bioprosthesis underwent ViV-TAVI. Although the guidewire crossed smoothly and fluoroscopy appeared reassuring, incomplete valve expansion occurred. Intraoperative transoesophageal echocardiography revealed that the guidewire had passed between degenerated leaflets rather than through the true central orifice. After repositioning under transoesophageal echocardiography guidance, full symmetric valve expansion and optimal haemodynamics were achieved. This case highlights the risk of false procedural reassurance during ViV-TAVI and underscores the importance of actively confirming central guidewire trajectory, particularly in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
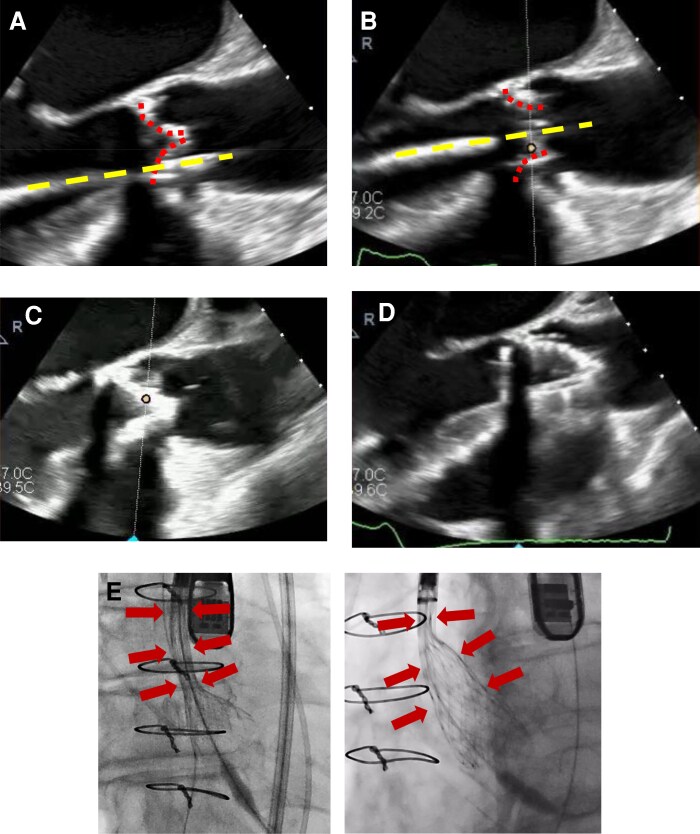 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Orthopaedic implants and arthroplasty
Introduction
Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is an established treatment option for patients with failed surgical bioprostheses who are at high or prohibitive surgical risk.^1^ Despite advances in device technology and imaging, procedural pitfalls remain, particularly in valves prone to early structural valve deterioration, such as the Trifecta bioprosthesis.
Summary figure
Intraoperative identification of guidewire malposition and its impact on valve expansion during valve-in-valve TAVI. (A) Mid-oesophageal long-axis transoesophageal echocardiography (TEE) showing the guidewire coursing between degenerated bioprosthetic leaflets, rather than through the true central orifice (dashed yellow line). (B) TEE image during initial deployment showing incomplete and asymmetric expansion of the transcatheter valve.(C) After repositioning, TEE demonstrates the guidewire passing through the true valve orifice, aligned with the prosthetic valve plane. (D) TEE image after guidewire repositioning showing full and symmetric valve expansion. (E) Fluoroscopic image demonstrating under-expanded valve configuration despite apparently acceptable wire position. (F) Fluoroscopic image after correction, confirming complete valve expansion.
Case presentation
An 84-year-old woman with New York Heart Association Class III dyspnoea presented 10 years after surgical aortic valve replacement with a 21 mm Trifecta bioprosthesis. Transthoracic echocardiography demonstrated severe transvalvular regurgitation with moderate stenosis. Computed tomography showed leaflet calcification and an internal diameter of 22.2 mm but no definitive leaflet tear. Given her prohibitive surgical risk (STS score 31%), ViV-TAVI was planned.
During transfemoral access, the guidewire advanced across the prosthetic valve smoothly without resistance, and deployment of a self-expanding transcatheter valve was attempted. However, the valve failed to expand adequately and was recaptured. Focused review of intraoperative transoesophageal echocardiographic (TEE) revealed that the guidewire had passed between degenerated bioprosthetic leaflets rather than through the true central orifice. After repositioning the guidewire under real-time TEE guidance, redeployment achieved full and symmetric valve expansion. Post-procedural TEE confirmed optimal haemodynamics with no residual regurgitation. The postoperative course was uneventful, and the patient remained asymptomatic at 6-month follow-up.
Discussion
This case does not propose a novel TEE technique. Rather, it highlights a critical procedural pitfall during ViV TAVI: guidewire malposition may occur despite smooth wire passage, reassuring fluoroscopic appearance, and non-diagnostic preprocedural computed tomography, particularly in failed Trifecta bioprostheses. The primary value of this report therefore lies in its preventive and cautionary message, emphasizing the risk of false procedural reassurance.
The Trifecta bioprosthesis is prone to early structural valve deterioration, frequently due to leaflet tears near the commissural posts.^2^ Such leaflet injury may be subtle or occult on preprocedural imaging yet can alter intravalvular anatomy, allowing the guidewire to track between leaflets rather than through the true central orifice. From a practical standpoint, mid-oesophageal long- and short-axis TEE views were particularly helpful in identifying wire trajectory relative to leaflet planes. Systematic interrogation of wire position before deployment and a low threshold for reassessment when valve expansion is incomplete are essential.
This report does not advocate a new TEE protocol but demonstrates a specific application of standard intraoperative TEE that may be underutilized during ViV-TAVI. A simple checklist approach may enhance safety in degenerated surgical bioprostheses.
Limitations
This report is limited by its single-case nature and short follow-up duration. Consequently, the frequency of this complication and predictive markers cannot be determined.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachset J, et al 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 2Fukuhara S, Shiomi S, Yang B, Kim K, Bolling SF, Haft J, et al Early structural valve degeneration of Trifecta bioprosthesis. Ann Thorac Surg 2020;109:720–727.31398357 10.1016/j.athoracsur.2019.06.032 · doi ↗ · pubmed ↗