Assessment of SARS-CoV-2 genome sequence recovery from four lateral flow device products available in the UK
Kuiama Lewandowski, Matthew Stokes, Alexandra Alexandridou, Abigail Fenwick, Mia L. White, Jack Crook, Karly-Rai Rogers-Broadway, Catherine Ryan, Deborah A. Williamson, Richard Vipond, Steven T. Pullan

TL;DR
This paper evaluates the ability to recover and sequence SARS-CoV-2 RNA from lateral flow tests used in the UK, finding it feasible but with variation between devices.
Contribution
The study demonstrates the feasibility of recovering SARS-CoV-2 RNA from lateral flow devices for sequencing, while highlighting the need for device optimization.
Findings
Sequencing from LFD eluates is possible at clinically relevant titres.
Results varied across the four tested devices.
Sequences obtained were consistent with routine methods.
Abstract
Introduction. Lateral flow tests have played a key role in the response to the COVID-19 pandemic and are likely to be a major component of diagnostic strategies to combat future outbreaks of infectious disease. Gap Statement. One challenge posed by widescale use of lateral flow tests in the community is the loss of sequence information to track virus evolution and epidemiology. Aim. Beyond their primary diagnostic function, it has been demonstrated that recovery of viral RNA from positive lateral flow devices (LFDs) for genome sequencing purposes is possible. We, therefore, aimed to assess the robustness and broader applicability of this process. Methodology. We evaluated SARS-CoV-2 RNA recovery and subsequent sequencing from eluates from the four major LFDs in use in the UK, testing both cultured virus and residual clinical nasal swab samples. Results. Our results demonstrated that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
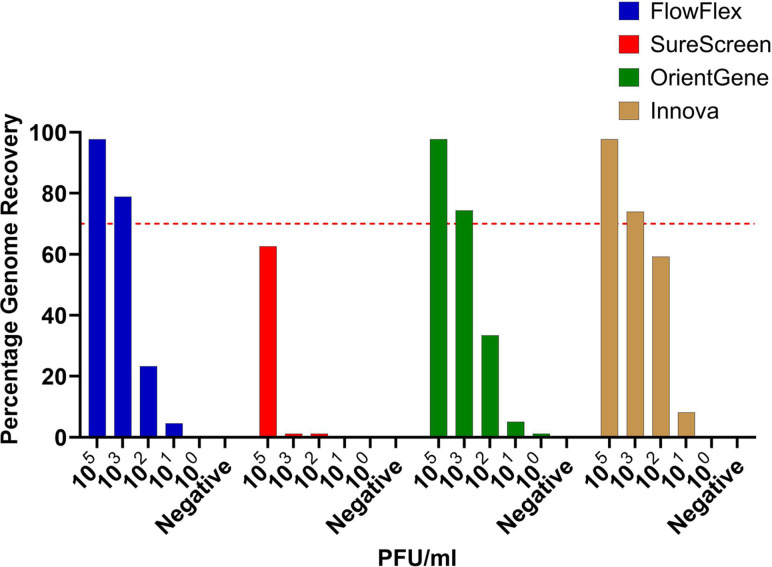 Fig. 1
Fig. 1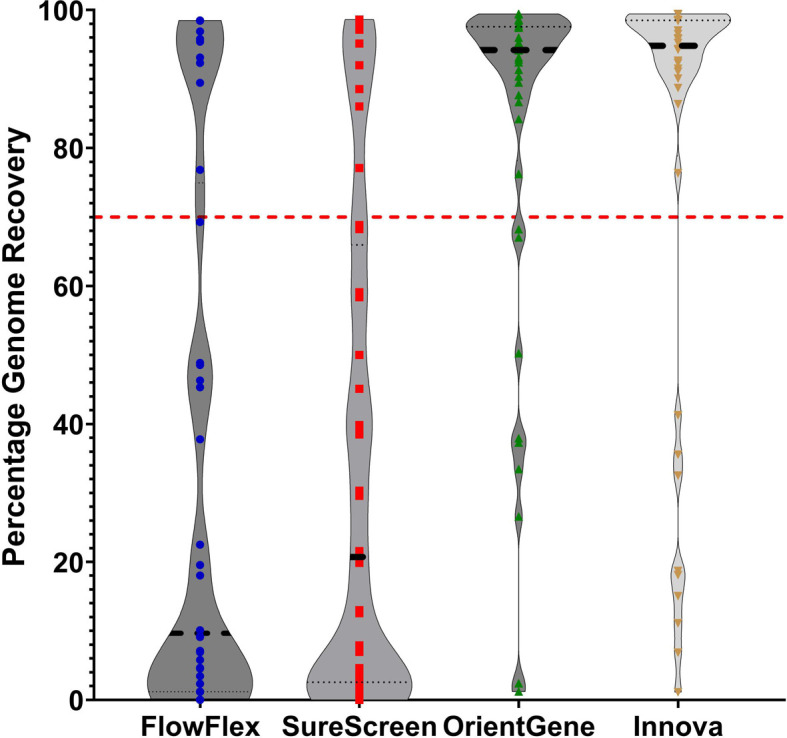 Fig. 2
Fig. 2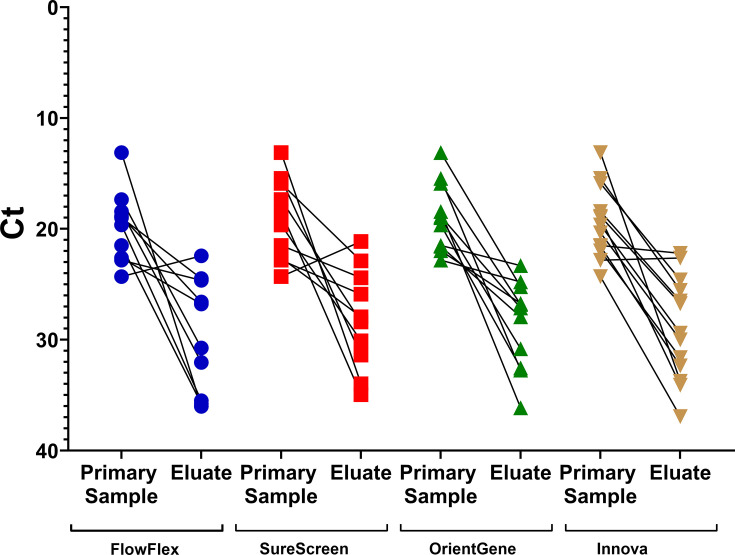 Fig. 3
Fig. 3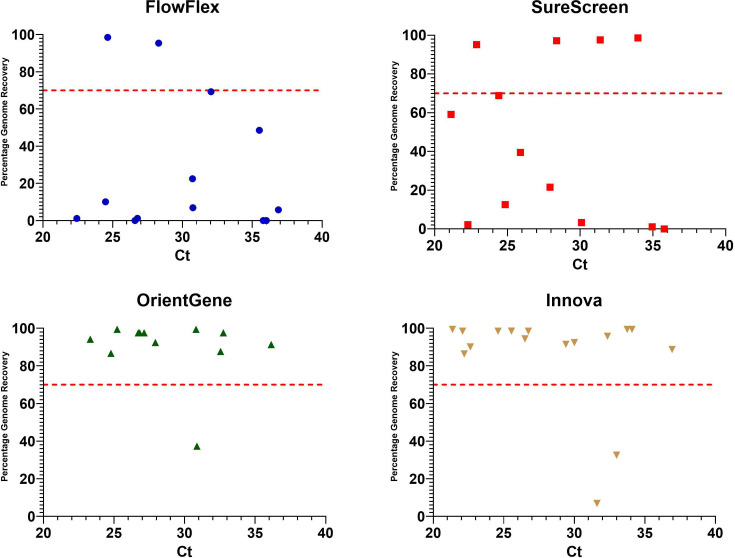 Fig. 4
Fig. 4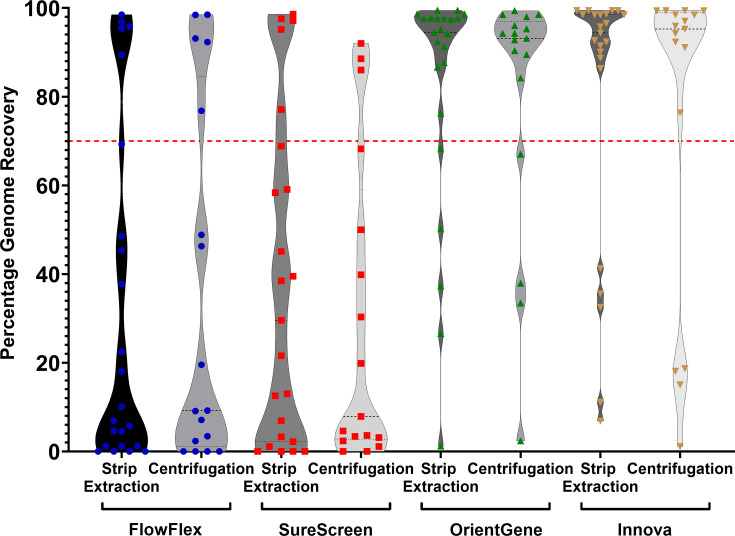 Fig. 5
Fig. 5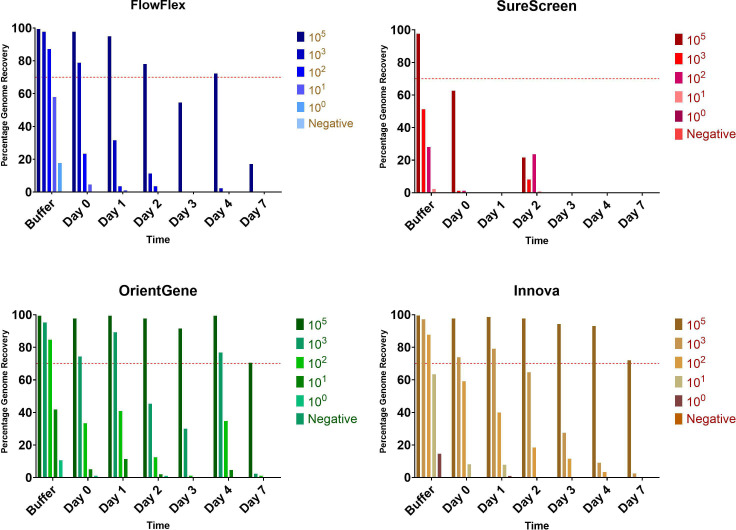 Fig. 6
Fig. 6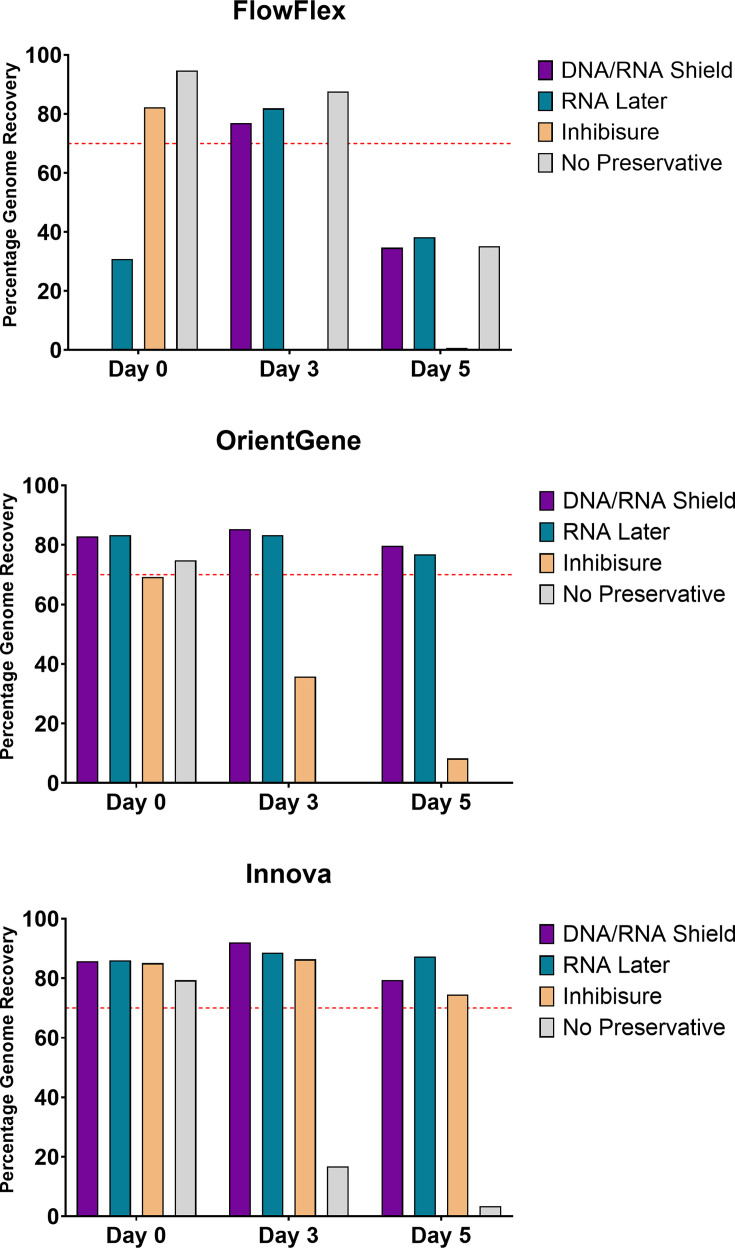 Fig. 7
Fig. 7| Percent of samples with lineage call | |||
|---|---|---|---|
| Day 0 | Day 1 | Day 2 | |
| FlowFlex | 30 | 20 | 0 |
| SureScreen | 30 | 20 | 0 |
| OrientGene | 90 | 60 | 60 |
| Innova | 80 | 70 | 50 |
- —http://dx.doi.org/10.13039/100004423 World Health Organization
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 detection and testing · Molecular Biology Techniques and Applications · SARS-CoV-2 and COVID-19 Research
Introduction
Genomic sequencing of SARS-CoV-2 has had a major role in the public health response to the COVID-19 pandemic, enabling mapping of viral transmission at global and local levels, informing infection control measures and identifying and tracking the emergence of new variants [1].
Viral transport media from nasal/oral swabs have been the most widely utilized sample source for SARS-CoV-2 whole-genome sequencing (WGS) pipelines. Typically, these have been residual material from diagnostic testing, taken forward for genome sequencing (most commonly via whole-genome tiling amplicon-based methods) upon positivity [2]. However, point-of-care lateral flow device (LFD) tests, including self-test kits, are replacing PCR as diagnostics in many settings [3], meaning opportunities for genomic characterization of circulating variants are increasingly limited.
Multiple studies have demonstrated the possibility of retrieving viral nucleic acid from positive LFDs. Martin et al. [4] described an approach for WGS of SARS-CoV-2 from positive LFDs and demonstrated the application of this technique to PanBio and InnoScreen devices collected as part of clinical care. The same device brands were also used to demonstrate detection and whole-genome sequencing of non-SARS-CoV-2 respiratory viruses present on the COVID-19 LFD [5]. Macori et al. [6] demonstrated that SARS-CoV-2 sequencing was possible from PanBio and Clinitest devices. Rector et al. [7] demonstrated that genomic material of SARS-CoV-2, influenza virus, adenovirus and rotavirus can also be retrieved from their corresponding positive LFDs, tested across nine different device brands (Roche, FlowFlex, Newgene, Coris, Alltest, Boson, OrientGene, AMP and Nadal), showing stability for up to 3 months post-use storage at room temperature, but noting that there were significant differences in RNA yields obtained from different device buffers, highlighting the requirement for individual device testing prior to routine use in sequencing.
In this study, we aim to perform an assessment focussed on those LFD brands currently in use in the UK, with a focus on the feasibility of performing the assay in a real-world relevant processing time frame.
Methods
LFDs tested
Four brands of SARS-CoV-2 LFD widely used in the UK were procured for testing:
FlowFlex COVID-19 Antigen Rapid Test (FlowFlex)COVID-19 SureScreen Lateral Flow Self-Test (SureScreen)OrientGene Rapid Covid-19 (Antigen) Self-Test (OrientGene)INNOVA SARS-CoV-2 Rapid Antigen Test (Innova)
Inactivated SARS-CoV-2
Cell-cultured and X-ray-irradiation-inactivated SARS-CoV-2 virions were provided by the Virology and Pathogenesis group, UKHSA Porton Down. A dilution series of samples was produced ranging from 10^5^ to 10^1^ p.f.u. ml^−1^ (Reverse transcription - quantitative PCR(RT-qPCR) C_t_ values of 18, 25, 28, 32 and 35).
Clinical samples
Anonymous residual Viral Transport Medium (VTM) from nasal swab samples was provided from routine UKHSA SARS-CoV-2 surveillance sequencing.
LFD loading
Mock or clinical samples were diluted 1 : 1 v/v with the corresponding LFD sample loading buffer, and 70 µl was applied to the device via pipette. After 15 min, the LFD result was read. Ambient incubation was continued for 45 min before elution.
Addition of preservatives
Where stated, 70 µl of the tested preservative was added to the device via the sample loading port once the result had been read. The viral sample titre used for all preservative testing was 10^3^ p.f.u. ml^−1^ (RT-qPCR C_t_ 25).
LFD elution
Strip removal method
The LFD was opened manually along the join line of the outer casing, and the internal strip was removed using two pairs of tweezers, placed into a 2 ml tube containing 700 µl of MagMAX Viral/Pathogen Binding Solution (extraction buffer) and incubated for 60 min prior to nucleic acid extraction.
Centrifugation method
Seven hundred microlitres of extraction buffer were added to the LFD via the sample loading port. The device was placed inside a 50 ml Falcon tube, laid flat (face up) and incubated for 60 min. The tube containing the LFD was centrifuged at 2,000 r.p.m. for 2 min to elute the extraction buffer from the device into the Falcon tube prior to nucleic acid extraction.
Nucleic acid extraction
Samples were extracted via the KingFisher Flex platform using the MagMAX Viral/Pathogen Nucleic Acid Isolation kits and 700 µl of sample input, as per the manufacturer’s instructions.
SARS-CoV-2 sequencing and lineage calling
Samples were processed by the UKHSA Pathogen Genomics SARS-CoV-2 Sequencing Service, utilizing the ARTIC network tiling amplicon scheme protocol [8], with primer scheme version 5.3.2. (SARS-CoV-2 version 5.3.2 scheme release - Laboratory - ARTIC Real-time Genomic Surveillance) and sequenced on an Oxford Nanopore GridION X5. Data analysis was performed by following the ARTIC network nanopore protocol for nCoV2019 [9], and lineage was determined via Pangolin [10].
RT-qPCR
RT-qPCR was performed using the Luna SARS-CoV-2 RT-qPCR Multiplex Assay Kit (New England Biolabs). Assays were performed as per the manufacturer’s instructions for the multiplex detection of 2019-nCoV_N1 and 2019-nCoV_N2 targets. Reported C_t_ values are for the N1 target.
Results
Preliminary testing of recovery utilizing inactivated SARS-CoV-2
A titration range of inactivated SARS-CoV-2 virions was used to assess the four device brands, with genomic material recovered by removal of the test strip (see methods).
We observed recovery of sufficient sequence information for lineage assignment (typically >70% of total genome) at both 10^5^ and 10^3^ p.f.u. ml^−1^ concentrations (equivalent to a sample C_t_ of 18 and 25, respectively) from three of the four devices tested (Fig. 1). SureScreen is the exception, with reduced genome recovery across all concentrations tested. Samples with a concentration of 10^2^ and above consistently produce a positive LFD on all brands tested.
Percentage of total genome sequence recovered following elution of SARS-CoV-2 virions from four brands of LFDs. Red line indicates 70% genome recovery (approximation of level required for lineage determination).
Clinical sample testing
To assess recoverability from a clinically relevant sample type, we tested 40 residual nasal swab VTM samples (used in COVID-19 surveillance sequencing). Residual material from each sample was loaded upon each of the four LFD types for direct comparison.
Results again varied across devices. From OrientGene and Innova devices, 80% of samples achieved sufficient coverage for variant calling, whereas for FlowFlex and SureScreen devices, only 25 and 20% of samples produced sufficient coverage, respectively (Fig. 2).
Percentage of total genome sequence recovered following elution of clinical samples across each of the four devices. Red line indicates 70% genome recovery.
In all cases where a lineage call was achieved, they were concordant with the expected result from initial sample sequencing.
Elution efficiency and genome recovery
To assess the efficiency of elution of viral nucleic acid from the LFDs, and the effect upon sequence recovery, RT-qPCR was performed on a subset of the clinical samples and corresponding LFD eluates. A similar level of reduction in viral concentration was seen between the primary sample and the LFD eluate for all devices (Fig. 3) with mean C_t_ increases being 14.9 from FlowFlex, 13.3 from SureScreen, 11.4 from OrientGene and 12.5 from Innova.
RT-qPCR Ct from the original sample and in the corresponding material eluted from LFD.
No clear correlation was seen between the C_t_ of the eluted material and the percentage of genome recovered for FlowFlex and SureScreen devices. For OrientGene and Innova devices, a trend was observed of C_t_ below 30 being sufficient to provide >70% genome recovery consistently, with higher C_t_ values providing more mixed results (Fig. 4).
Comparison of percentage consensus genome sequence recovery from clinical samples compared to the viral titre of material eluted from the used LFDs. Red line indicates 70% genome recovery.
Process optimization and evaluation of the centrifugation method using clinical samples
Experiments initially followed the procedure for LFD strip extraction as set out by Martin et al. [4]. This process is time-consuming and labour-intensive; therefore, we set out to test the process of elution of sample in extraction buffer directly from the LFD via centrifugation as described by Macori et al. [6].
For initial comparison, the irradiated SARS-CoV-2 series was processed in triplicate, across three time points, on each device by both methods. LFD centrifugation provided equivalent or improved genome coverage for all device brands (see Table S1, available in the online Supplementary Material). A further comparison between the two extraction methods was made using residual clinical samples. The clinical samples tested were not paired but comprised two batches containing samples with a clinically representative C_t_ range. Results from elution by centrifugation remained comparable to those from the strip removal extraction method when using clinical samples (Fig. 5). The percentage of samples with a positive lineage call, comparing strip removal to centrifugation, was 21.7–29.4%, 21.7–17.7%, 78.2–76.4% and 78.2–76.4%, for FlowFlex, SureScreen, OrientGene and Innova devices, respectively.
Distribution of percentage consensus genome sequence recovery following elution via strip removal (opened) or centrifugation (spun) method from clinical samples for all four LFDs tested. Red line indicates 70% genome recovery.
Assessment of sample viability upon LFDs over 7 days of ambient incubation
Real-world use of LFDs as a sample source for sequencing applications raises logistical issues that are likely to include delays between initial sample LFD testing and laboratory processing, particularly in home-use scenarios. We set out to assess the impact of delayed time of LFD sample receipt and processing on the ability to recover informative genome sequences. An irradiated SARS-CoV-2 dilution series was used to assess the effect of such delays ranging up to 7 days in duration. Stability of the nucleic acid in the used LFD as measured by genome sequence recovery was assessed for each device, from dilution in LFD buffer without being run on the device to running followed by multiple days of incubation upon the device post-use, at room temperature, prior to extraction (Fig. 6).
Percentage consensus genome sequence recovery following elution of a range of titres of SARS-CoV-2 virions from the four LFDs tested. Buffer indicates incubation in buffer without being run on a device. Red line indicates 70% genome recovery.
Decreased genome recovery was seen with increased delay time for all devices. The highest titre tested (equivalent C_t_ 18) provided sufficient genomic coverage for multiple days on FlowFlex, OrientGene and Innova devices (Fig. 4), but the signal rapidly degraded on SureScreen devices. The C_t_ 25 equivalent sample showed an inconsistent signal over multiple days on OrientGene and Innova devices but was rapidly degraded on FlowFlex and SureScreen devices. Decreased genome recovery was also seen for most titration series samples when extracted directly from SureScreen LFD buffer when compared to the other device buffers.
The effect of delayed time to elution on recovery from LFDs using residual clinical sample material
Residual clinical samples were used to assess the effect of delayed time to elution on recovery from LFDs. Ten clinical samples were tested on each of 4 LFD brands over the course of 3 days. Decreased genome recovery is seen over time in all cases, but OrientGene and Innova devices still provided sufficient genome coverage for lineage calling from 60 and 50% of clinical samples tested after 2 days of incubation. FlowFlex and SureScreen produced reduced genome coverage from the samples tested, even in the absence of delayed recovery (Table 1).
The effect of nucleic acid preservatives on recovery from LFDs over 5 days of ambient incubation
Addition of three RNA stabilizing agents to devices post-running of a mid-titre SARS-CoV-2 mock sample (10^3^ p.f.u. ml^−1^) shows varied results. DNA/RNA shield and RNALater preserved RNA and allowed near-complete genome sequencing after 5 days of room temperature incubation on both OrientGene and Innova devices. Inhibisure was similarly effective on the Innova device but showed no preservative effect on OrientGene devices. Results on FlowFlex were inconsistent for all preservatives tested (Fig. 7).
The effect of nucleic acid preservatives on genome recovery from LFDs over 5 days of ambient incubation. Red line indicates 70% genome recovery.
Discussion
In this study, we set out to assess the feasibility of SARS-CoV-2 amplicon sequencing using LFD eluates from four major LFD brands currently in use in the UK, with the aim of generating a protocol that could subsequently be expanded to other potential use settings.
Our testing using inactivated SARS-CoV-2 observed recovery of sufficient sequence information for lineage assignment at titres as low as 10^3^ p.f.u. ml^−1^ (sample Ct ~25) from three of the four tested major devices currently in use within the UK.
Our assessment of genome recovery from 40 residual clinical nasal swab samples (C_t_ range from 13 to 24) for each LFD type found reduced genome recovery for clinical samples from FlowFlex and SureScreen devices (25 and 20% of samples with a lineage call, respectively) when compared to OrientGene and Innova devices (80 and 80% of samples with a lineage call, respectively).
Rector et al. [7] tested a range of LFD brands, using stored nasopharyngeal samples, and they found that LFD buffer components can be deleterious for the viral genetic material, resulting in lower RNA concentrations and interfering with sequencing. In our study, a similar reduction in viral concentration was seen in LFD eluates of all brands compared to the originating clinical samples, indicating that reduced elution efficiency is unlikely to be the cause of poorer genome recovery via amplicon sequencing in some devices. Markedly different levels of genome recovery were seen from titration series samples when extracted and sequenced directly from the buffers of the tested LFD brands. These data indicate that increased levels of degradation or the presence of inhibitors in some device buffers may be significant factors.
The process of removing strips from LFD casings for nucleic acid extraction is time-consuming, labour-intensive and not feasible for use in high-throughput processing. Work by Macori et al. [6] described an extraction method by centrifugation. In our study, we confirmed that LFD centrifugation provided equivalent or improved genome coverage for all device brands.
Decreased genome recovery was seen with increased delay time for all devices. OrientGene and Innova showed the best recovery over time, with 60/70% of samples showing sufficient stability after 2 days to retrieve near-complete genome sequences. For all LFD brands, considerable loss of recovery from clinically representative titrations was seen from day 3 onwards. Interestingly, Martin et al. [4] found that SARS-CoV-2 genomes could be successfully recovered from Abbott and InnoScreen brand test devices up to 8 days after initial sample collection.
The addition of commercial nucleic-acid-stabilizing reagents to devices after run completion showed promise. Both RNALater and DNA/RNA shield showed a preservative effect over several days upon the typically best-yielding devices, OrientGene and Innova, as has been observed by Moso et al. [5] for multiple RNA viruses on the PanBio COVID-19 device. Neither preservative, however, improved the recovery from the FlowFlex device.
LFDs are not designed to be compatible with extracting genetic material suitable for sequencing. However, building on the observations of Martin et al. [4] and others, we have verified that it is feasible to retrieve adequate genetic material for targeted amplicon sequencing from some of these devices. Our work extends this finding to various LFDs currently deployed in the UK, showing that genomic recovery varies across different devices. Accordingly, a comprehensive assessment of each LFD type is required to determine its suitability as a genomic sequencing sample source.
Consideration should be given as to whether future iterations of LFDs should incorporate the capability to efficiently sequence pathogens from the eluate as a design requirement or how this could otherwise be achieved efficiently and effectively.
We suggest the following next steps:
Conduct a comprehensive comparative study to quantify the efficiency of genomic recovery across different LFD brands and models working with representative suppliers. This study should aim to identify factors that influence the variability in recovery rates.Engage with LFD manufacturers to share findings and collaborate on the development of next-generation devices that include the efficient recovery of genetic material as a key design objective.Work towards establishing a set of guidelines or standards for evaluating LFD suitability as sources of genetic material for sequencing. These guidelines may help streamline the assessment process for new or existing LFD types.
Supplementary material
10.1099/jmm.0.002144Uncited Table S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marjanovic S Romanelli RJ Ali GC Leach B Bonsu M et al COVID-19 Genomics UK (COG-UK) Consortium: final report Rand Health Q 2022924 PMC 951909636238008 · pubmed ↗
- 2COVID-19 Genomics UK (COG-UK) consortium An integrated national scale SARS-Co V-2 genomic surveillance network Lancet Microbe 20201 e 99e 10010.1016/S 2666-5247(20)30054-932835336 PMC 7266609 · doi ↗ · pubmed ↗
- 3Eyre DW Futschik M Tunkel S Wei J Cole-Hamilton J et al Performance of antigen lateral flow devices in the UK during the alpha, delta, and omicron waves of the SARS-Co V-2 pandemic: a diagnostic and observational study Lancet Infect Dis 20232392293210.1016/S 1473-3099(23)00129-937001541 PMC 10048397 · doi ↗ · pubmed ↗
- 4Martin GE Taiaroa G Taouk ML Savic I O’Keefe J et al Maintaining genomic surveillance using whole-genome sequencing of SARS-Co V-2 from rapid antigen test devices Lancet Infect Dis 2022221417141810.1016/S 1473-3099(22)00512-6PMC 935227035934015 · doi ↗ · pubmed ↗
- 5Moso MA Taiaroa G Steinig E Zhanduisenov M Butel-Simoes G et al Non-SARS-Co V-2 respiratory viral detection and whole genome sequencing from COVID-19 rapid antigen test devices: a laboratory evaluation study Lancet Microbe 20245 e 317e 32510.1016/S 2666-5247(23)00375-038359857 · doi ↗ · pubmed ↗
- 6Macori G Russell T Barry G Mc Carthy SC Koolman L et al Inactivation and recovery of high quality RNA from positive SARS-Co V-2 rapid antigen tests suitable for whole virus genome sequencing Front Public Health 20221086386210.3389/fpubh.2022.86386235592078 PMC 9113430 · doi ↗ · pubmed ↗
- 7Rector A Bloemen M Schiettekatte G Maes P Van Ranst M et al Sequencing directly from antigen-detection rapid diagnostic tests in Belgium, 2022: a gamechanger in genomic surveillance?Euro Surveill 202328220061810.2807/1560-7917.ES.2023.28.9.220061836862099 PMC 9983067 · doi ↗ · pubmed ↗
- 8Quick J Lansdowne L ARTIC SARS-Co V-2 sequencing protocol v 4 (LSK 114) v 2protocols.io 202410.17504/protocols.io.bp 2l 6n 26rgqe/v 4 · doi ↗