Progressive myocardial metabolic dysfunction after stereotactic arrhythmia radioablation for ventricular tachycardia in hypertrophic cardiomyopathy: a serial multimodality imaging case report
Masafumi Shimojo, Mariko Kawamura, Yasuya Inden, Shinji Naganawa, Toyoaki Murohara

TL;DR
A patient with heart disease showed improved arrhythmia after radiation treatment, but later developed new heart issues, suggesting radiation can have both short-term benefits and long-term risks.
Contribution
This case report provides novel insights into the progressive myocardial injury caused by stereotactic arrhythmia radioablation.
Findings
Progressive metabolic dysfunction and wall motion deterioration occurred after irradiation without changes in perfusion or fibrosis.
Short-term antiarrhythmic effects were observed, but new arrhythmogenic substrates developed over time.
Septal contraction patterns changed progressively over two years following treatment.
Abstract
Stereotactic arrhythmia radioablation (STAR) for ventricular tachycardia (VT) has emerged as a promising treatment for patients in whom catheter ablation is challenging or unsuccessful; however, its underlying mechanisms remain unclear, particularly with respect to early antiarrhythmic effects. A 51-year-old man with hypertrophic cardiomyopathy exhibited extensive mid-septal scar on contrast-enhanced cardiac magnetic resonance imaging (CE-MRI) and suffered from refractory VT. The VT was presumed to originate from the mid-septal scar with preferential conduction towards the outflow region. Stereotactic arrhythmia radioablation was performed, delivering 25 Gy to the core scar and 20 Gy to the surrounding wall and outflow region. Ventricular tachycardia episodes decreased immediately after STAR and disappeared within 3 months, but recurred 24 months later. Serial multimodality imaging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
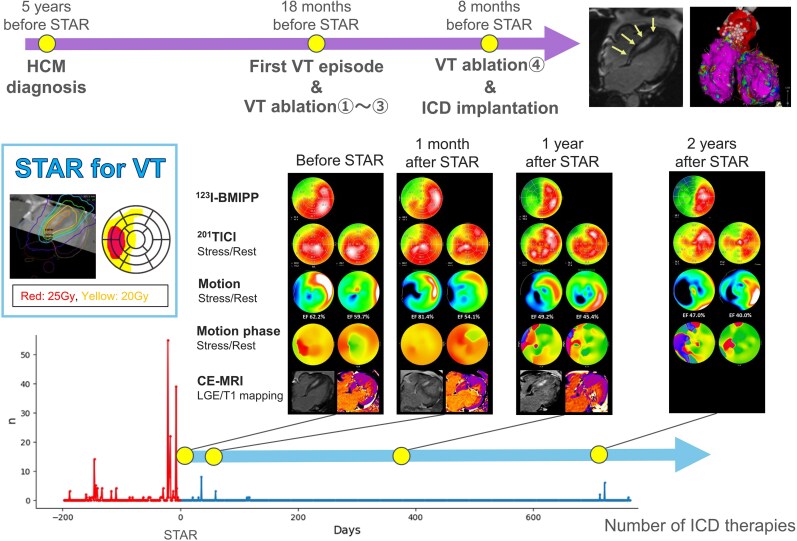 Figure 1
Figure 1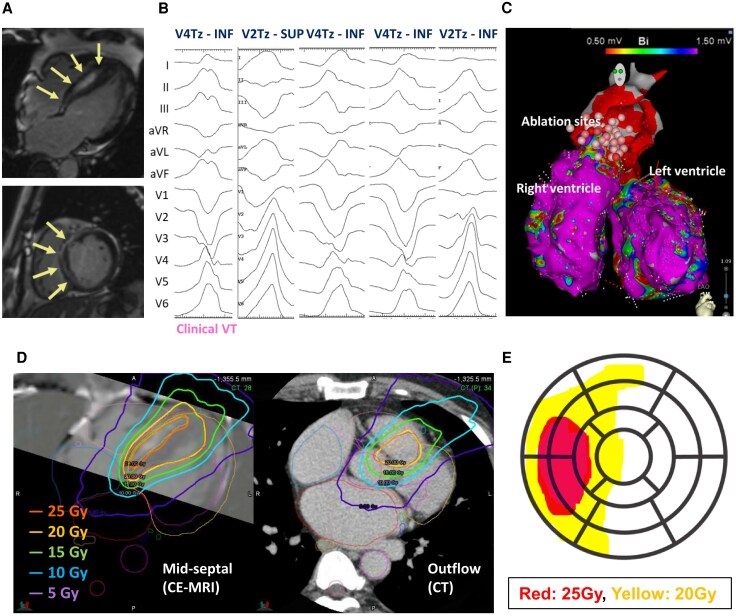 Figure 1
Figure 1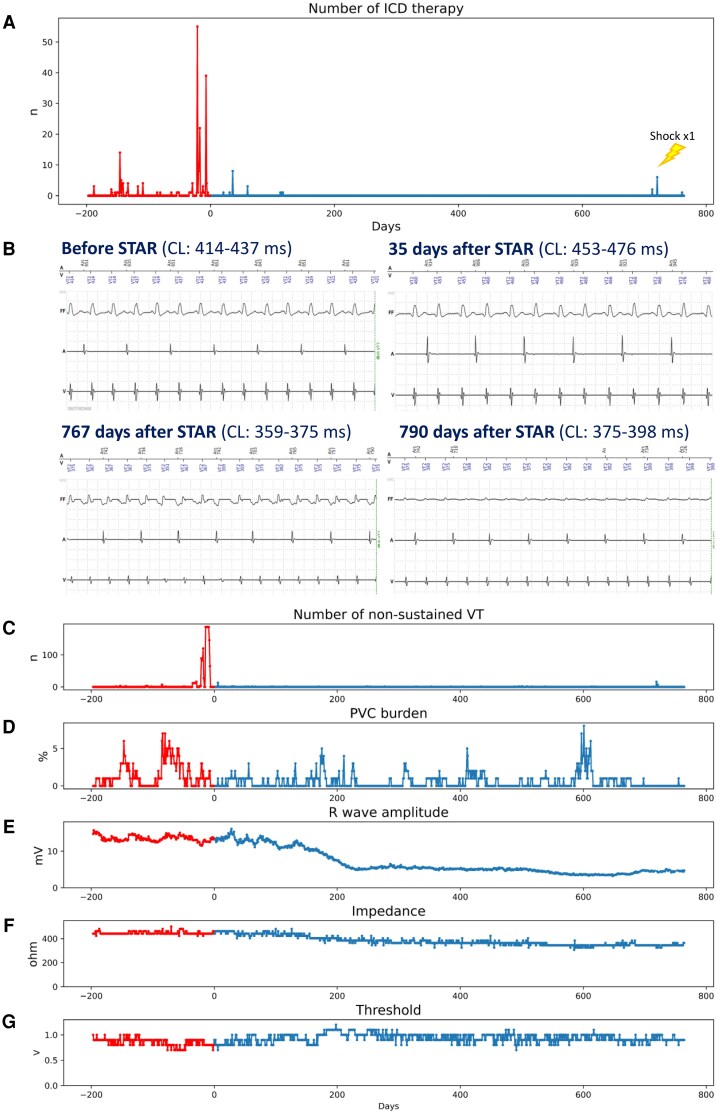 Figure 2
Figure 2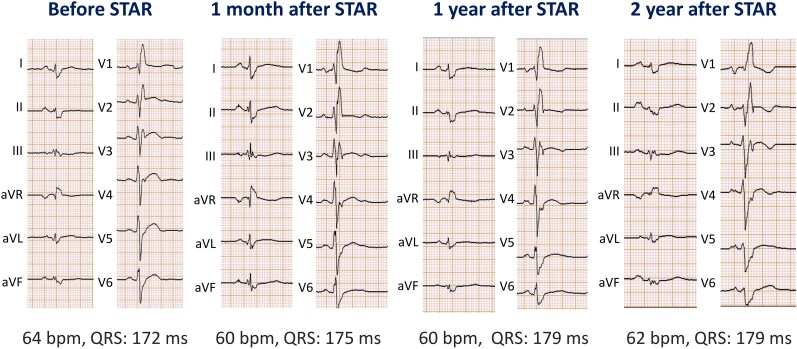 Figure 3
Figure 3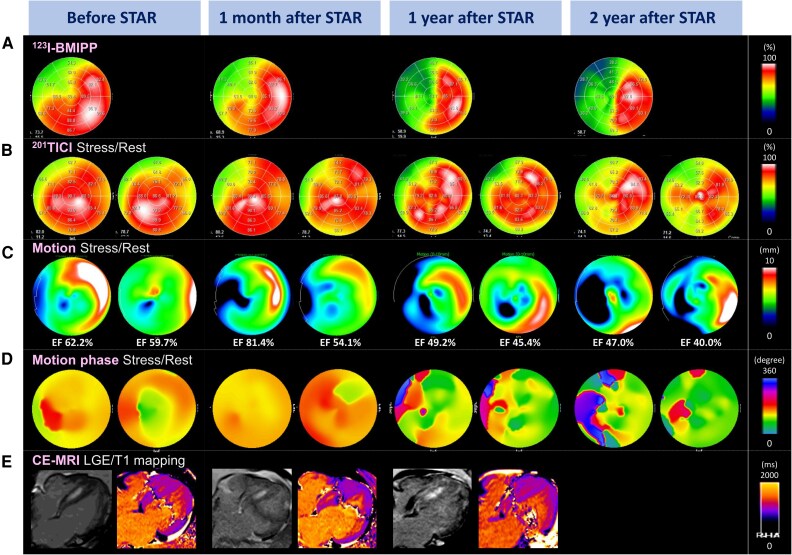 Figure 4
Figure 4- —Academic Clinical Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiomyopathy and Myosin Studies · Cardiac electrophysiology and arrhythmias
Introduction
Stereotactic arrhythmia radioablation (STAR) for ventricular tachycardia (VT) has emerged as a promising option for patients in whom catheter ablation (CA) has failed or is not feasible; however, its therapeutic mechanisms remain poorly understood.^1–5^ Although radiation-induced tissue injury and subsequent fibrosis were initially considered the primary mechanisms,^2,3,6^ clinical observations have demonstrated antiarrhythmic effects that occur far earlier than the expected development of fibrosis.^4,7^ Recent experimental studies have proposed that early effects may involve improved myocardial conduction rather than tissue injury, a concept that contrasts with the traditional understanding.^8–10^ Here, we report a case of STAR for VT in a patient with hypertrophic cardiomyopathy (HCM) in which serial imaging suggested that myocardial injury occurred much earlier than previously assumed, providing new insights into the temporal characteristics of STAR-related tissue response.
Summary figure
**
Case presentation
A 51-year-old man with HCM, diagnosed in 2018, remained asymptomatic until April 2022, when he presented with chest pain accompanied by diaphoresis and was diagnosed with VT, for which he underwent CA. Despite three CAs targeting the left and right coronary cusps and both ventricular outflow tracts, VT recurred, and he was referred to our institution. In February 2023, CA and implantable cardioverter-defibrillator (ICD) implantation were performed. Pre-procedural contrast-enhanced cardiac magnetic resonance imaging (CE-MRI) showed mid-septal late gadolinium enhancement (LGE) of the hypertrophied septum (Figure 1A). The clinical VT demonstrated a V4 transition with an inferior axis, while other inducible VTs showed various precordial transitions and axes (Figure 1B), suggesting a mid-septal scar origin. During CA, both ventricles exhibited normal endocardial voltage, and radiofrequency energy was applied to the earliest activation site of the inducible clinical VT; however, it was ineffective (Figure 1C). Details of CA are shown in Supplementary material online, Figure S1.
(A) CE-MRI. Arrows indicate areas of LGE. (B) Twelve-lead electrocardiogram of VTs induced during ablation. (C) Voltage map and ablation sites. (D) Radiation dose distribution (left, septal region; right, outflow region). (E) Schematic of the 25 and 20 Gy irradiation fields projected onto the 17-segment model. CE-MRI, contrast-enhanced cardiac magnetic resonance imaging; CT, computed tomography; INF, inferior axis; LGE, late gadolinium enhancement; SUP, superior axis; Tz, precordial transitional zone; VT, ventricular tachycardia.
Despite treatment with amiodarone 200 mg and bisoprolol 2.5 mg, the patient continued to experience frequent ICD therapies, and STAR using the CyberKnife® system (Accuray Inc., USA) was performed in October 2023. The treatment was conducted as a specified clinical study approved by the institutional review board. The VTs were thought to originate from the mid-septal arrhythmogenic scar but exit preferentially towards the outflow region. Therefore, the target was planned to cover both the mid-septal scar and the outflow region. Because including the entire transmural wall containing LGE-positive myocardium would have resulted in an excessively large volume, dose planning was as follows: 25 Gy to the LGE-positive core and 20 Gy to the remaining LGE-positive-containing wall and the outflow, without margin expansion (Figure 1D). The 25 Gy volume was 32.2 mL, and the combined 20/25 Gy volume was 133 mL. The 25 and 20 Gy irradiation fields projected onto the 17-segment model are shown in Figure 1E.
Arrhythmic events and ICD lead parameters were collected daily through remote monitoring (Home Monitoring®, Biotronik SE & Co. KG, Germany) for 6 months before and 25 months after STAR. The ICD lead tip was fixed at the right ventricular septum. Implantable cardioverter-defibrillator therapies decreased immediately after STAR and were absent beyond 3 months; however, appropriate ICD therapies, including shock delivery, recurred 24 months later (Figure 2A). One month after STAR, the VT showed a slightly longer cycle length but similar morphology to pre-STAR, whereas the recurrent VT at 24 months had a different morphology and a shorter cycle length (Figure 2B). Non-sustained VT decreased in parallel with VT episodes (Figure 2C), while premature ventricular contraction burden remained almost unchanged (Figure 2D). The R-wave amplitude gradually declined and reached a plateau at around 7 months (Figure 2E). Ventricular pacing thresholds and impedance showed similar trends, with thresholds increasing and impedance decreasing until stabilizing at ∼7 months (Figure 2F and G). The surface electrocardiogram showed no remarkable changes (Figure 3).
(A) Number of ICD therapies. Shock delivery occurred only in the marked episodes, and all therapies were anti-tachycardia pacing. (B) ICD recording during a VT episode. (C) Number of non-sustained VT episodes. (D) Per cent of PVCs per day. (E) R-wave amplitude. (F) Shock lead impedance. (G) Ventricular pacing threshold. CL, cycle length; ICD, implantable cardioverter-defibrillator; PVC, premature ventricular contraction; STAR, stereotactic arrhythmia radioablation; VT, ventricular tachycardia.
Serial 12-lead electrocardiograms. STAR, stereotactic arrhythmia radioablation.
Dual single-photon emission computed tomography using thallium-201 chloride (^201^TlCl) and iodine-123-beta-methyl-p-iodophenyl-pentadecanoic acid (^123^I-BMIPP), along with CE-MRI, was performed before STAR and at 1 month, 1 year, and 2 years. ^123^I-BMIPP imaging demonstrated progressive reduction in tracer uptake within the irradiated area (Figure 4A), whereas ^201^TlCl uptake showed no apparent change on either stress or rest imaging (Figure 4B). Quantitative gated single-photon emission computed tomography (QGS) revealed progressive regional motion deterioration in the irradiated region (Figure 4C). Motion-phase analysis using Heart Risk View software (HRV-F, Nihon Medi-Physics, Japan) showed a septal contraction delay during stress before STAR, which disappeared at 1 month but evolved into a heterogeneous contraction pattern by 1 year, and further deteriorated by 2 years (Figure 4D). On CE-MRI, no substantial change was observed in the areas of LGE or T1-mapping signal intensity (Figure 4E).
Serial imaging changes. (A) 123I-BMIPP uptake. (B) 201TlCl uptake (right, stress; left, rest). (C) Left ventricular wall motion (right, stress; left, rest). (D) Phase analysis of left ventricular motion (right, stress; left, rest). (E) MRI (left: LGE; right: T1 mapping). CE-MRI, contrast-enhanced cardiac magnetic resonance imaging; EF, ejection fraction; 123I-BMIPP, iodine-123-beta-methyl-p-iodophenyl-pentadecanoic acid; LGE, late gadolinium enhancement; STAR, stereotactic arrhythmia radioablation; 201TlCl, thallium-201 chloride.
At 25 months after STAR, the patient continued regular outpatient follow-up without major complications, except for a mild pericardial effusion observed at 6 months. Detailed temporal changes in physical status, mental status, and medication are summarized in Supplementary material online, Figure S2.
Discussion
In this case, STAR demonstrated an early antiarrhythmic effect (Figure 2A), accompanied by early-onset, long-term progressive myocardial injury in the irradiated region. Ventricular tachycardia suppression by STAR may involve not only indirect effects, such as autonomic modulation, but also direct injury to the VT isthmus and altered conduction properties. ^123^I-BMIPP uptake within the irradiated region decreased over time (Figure 4A). Although early post-STAR changes may reflect oedema or intramyocardial haemorrhage,^11^ they likely represent an early phase of progressive, irreversible myocardial injury rather than a transient reversible process. In contrast, ^201^TlCl uptake under both rest and stress conditions was preserved (Figure 4B), suggesting that the myocardial injury was non-ischaemic and reflected radiation-induced damage, possibly mediated by free radicals or apoptosis. There were no findings suggestive of marked fibrotic progression (Figure 4E), consistent with prior studies.^6,10,11^ Progressive wall motion deterioration within the irradiated area on QGS (Figure 4C) and the gradual decline in R-wave amplitude (Figure 2E) further supported progressive myocardial injury. Although R-wave reduction may partly reflect lead–myocardium interface effects, its temporal trend suggested that myocardial injury began immediately after STAR and stabilized around 7 months, consistent with previously reported apoptotic changes following myocardial irradiation.^12,13^
The HRV-F findings also provided important insights into the antiarrhythmic mechanism. The VT was presumed to originate from a septal scar, and pre-STAR phase analysis demonstrated delayed septal activation during stress, which may have served as the arrhythmogenic substrate. This delay disappeared 1 month after STAR, potentially explaining the early antiarrhythmic effect. However, more than 1 year after STAR, heterogeneous phase patterns emerged in the irradiated region (Figure 4D). Given that the recurrent VT differed from the pre-STAR morphology (Figure 2B), a new arrhythmogenic substrate may have developed during the chronic phase due to progressive myocardial injury.
These findings may be unique to HCM; however, similar phenomena could potentially occur in other aetiologies as well. The detection of progressive injury in this case may have been facilitated by the hypertrophied myocardium, which differs from the thinned myocardium often seen in other cardiomyopathies and provides sufficient spatial resolution for detection on both MRI and nuclear imaging. Given that a single-fraction STAR dose of 25 Gy, or even 20 Gy, can induce progressive myocardial injury, irradiation of normal myocardium should be minimized whenever possible. In particular, although transmural irradiation of the ventricular wall has been widely accepted,^14^ the target should be carefully defined when a large proportion of normal myocardium is included in the treatment region.
Supplementary Material
ytag142_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kawamura M, Shimojo M, Tatsugami F, Hirata K, Fujita S, Ueda D, et al Stereotactic arrhythmia radioablation for ventricular tachycardia: a review of clinical trials and emerging roles of imaging. J Radiat Res 2025;66:1–9.39656944 10.1093/jrr/rrae 090PMC 11753837 · doi ↗ · pubmed ↗
- 2Cvek J, Neuwirth R, Knybel L, Molenda L, Otahal B, Pindor J, et al Cardiac radiosurgery for malignant ventricular tachycardia. Cureus 2014;6:e 190.
- 3Loo BW Jr, Soltys SG, Wang L, Lo A, Fahimian BP, Iagaru A, et al Stereotactic ablative radiotherapy for the treatment of refractory cardiac ventricular arrhythmia. Circ Arrhythm Electrophysiol 2015;8:748–750.26082532 10.1161/CIRCEP.115.002765 · doi ↗ · pubmed ↗
- 4Cuculich PS, Schill MR, Kashani R, Mutic S, Lang A, Cooper D, et al Noninvasive cardiac radiation for ablation of ventricular tachycardia. N Engl J Med 2017;377:2325–2336.29236642 10.1056/NEJ Moa 1613773 PMC 5764179 · doi ↗ · pubmed ↗
- 5Kovacs B, Mayinger M, Andratschke N, Saguner AM. Stereotactic arrhythmia radioablation: competitor or adjunct to catheter ablation? Eur Heart J 2022;43:3279–3281.35947872 10.1093/eurheartj/ehac 435 · doi ↗ · pubmed ↗
- 6Blanck O, Bode F, Gebhard M, Hunold P, Brandt S, Bruder R, et al Dose-escalation study for cardiac radiosurgery in a porcine model. Int J Radiat Oncol Biol Phys 2014;89:590–598.24751407 10.1016/j.ijrobp.2014.02.036 · doi ↗ · pubmed ↗
- 7Neuwirth R, Cvek J, Knybel L, Jiravsky O, Molenda L, Kodaj M, et al Stereotactic radiosurgery for ablation of ventricular tachycardia. Europace 2019;21:1088–1095.31121018 10.1093/europace/euz 133 · doi ↗ · pubmed ↗
- 8Amino M, Yoshioka K, Tanabe T, Tanaka E, Mori H, Furusawa Y, et al Heavy ion radiation up-regulates Cx 43 and ameliorates arrhythmogenic substrates in hearts after myocardial infarction. Cardiovasc Res 2006;72:412–421.17054928 10.1016/j.cardiores.2006.09.010 · doi ↗ · pubmed ↗