Case report: Malignant erythema in an ovarian cancer case: an uncommon paraneoplastic syndrome
Xiaolin Liu, Xingyu Wang, Lijie Wang

TL;DR
A woman with ovarian cancer showed a rare skin condition called malignant erythema, which improved after surgery, suggesting a link between the skin symptom and the cancer.
Contribution
This paper presents a rare case of malignant erythema as an initial sign of ovarian cancer, highlighting its potential as a paraneoplastic syndrome.
Findings
Malignant erythema resolved rapidly after surgery for ovarian cancer.
Dermatomyositis in older patients may be linked to underlying cancer.
Cutaneous symptoms can precede cancer diagnosis in some cases.
Abstract
Dermatomyositis is an autoimmune illness that affects the striated muscle and skin. It usually shows muscular and cutaneous manifestation. Age above 40 years and females are risk factors for malignant tumor in patients with dermatomyositis. In our case study, a woman with malignant erythema as her first symptom was reported. She was later diagnosed with ovarian cancer and underwent subtractive surgery, which caused the erythema to rapidly subside. Most similar DM cases suffered from muscular disorders including painless proximal symmetrical weakness as well as weakness of the pharyngeal muscle, often leading to aspiration pneumonia and dysphagia. Here, we reported this case with cutaneous symptoms in detailed clinical information including medicine use and clinical outcome. Cancer screening would be recommended in these intractable cases. On the other side, more researches are needed be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
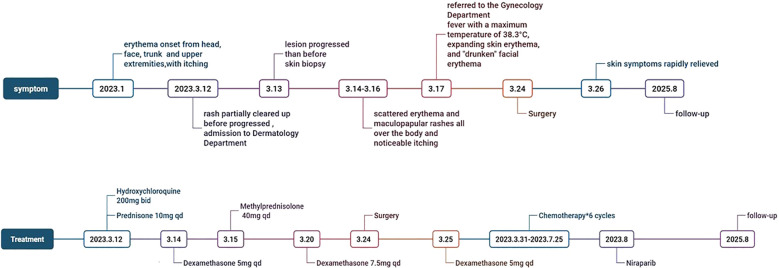 Figure 1
Figure 1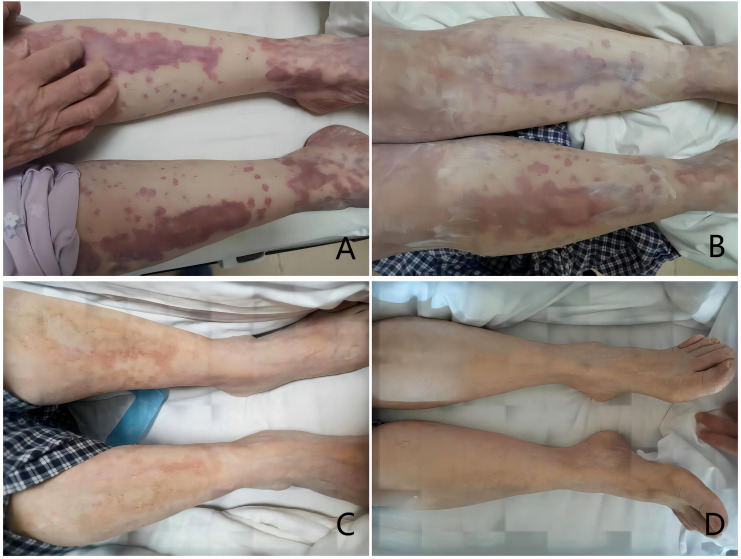 Figure 2
Figure 2| No. | Item | Result | Reference interval | Unit | Detection method |
|---|---|---|---|---|---|
| 1 | Anti-nuclear Antibody (ANA) | Positive | <1:100 Negative | – | Indirect Immunofluorescence |
| 2 | Anti-dsDNA Antibody | <10.00 | 0 - 100 | IU/ml | Enzyme-Linked Immunosorbent Assay |
| 3 | Anti-Sm Antibody | <2.00 | 0 - 20 | RU/ml | – |
| 4 | Anti-nucleosome Antibody (AnuA) | <2.00 | 0 - 20 | RU/ml | Enzyme-Linked Immunosorbent Assay |
| 5 | Anti-ribosomal P Protein Antibody (FRNP) | <2.00 | 0 - 20 | RU/ml | Enzyme-Linked Immunosorbent Assay |
| 6 | Anti-SSA Antibody | 2.43 | 0 - 20 | RU/ml | Enzyme-Linked Immunosorbent Assay |
| 7 | Anti-SSB Antibody | <2.00 | 0 - 20 | RU/ml | Enzyme-Linked Immunosorbent Assay |
| 8 | Creatine Kinase (CK) | 169 | 40 - 200 | U/L | – |
| 9 | Alpha-Hydroxybutyrate Dehydrogenase (HBDH) | 202.7 | 72 - 182 | U/L | – |
| 10 | Creatine Kinase-MB Mass (CK-MB) | 4.6 | 0.6 - 6.3 | pg/ml | – |
| 11 | Myoglobin (MYO) | 43.7 | 14.3 - 65.8 | ng/ml | – |
| 12 | High-Sensitivity Cardiac Troponin I (HS-TnI) | 3.2 | 0 - 17.5 | pg/ml | – |
| 13 | Rheumatoid Factor (RF) | <11.20 | 0 - 20 | KU/L | – |
| 14 | Anti-Myeloperoxidase Antibody (MPO) | 1.2 | 0 - 20 | RU/ml | Chemiluminescence |
| 15 | Proteinase 3 (PR3) | 0.7 | 0 - 20 | CU | Chemiluminescence |
| 16 | Anti-neutrophil Cytoplasmic Antibody - Perinuclear Pattern (pANCA) | Negative | <1:10 Negative | – | Indirect Immunofluorescence |
| 17 | Anti-neutrophil Cytoplasmic Antibody - Cytoplasmic Pattern (cANCA) | Negative | <1:10 Negative | – | Indirect Immunofluorescence |
| 18 | Anti-Glomerular Basement Membrane Antibody (GBM) | 0.3 | 0 - 20 | RU/ml | – |
| 19 | Humoral Immunity Panel Immunoglobulin G (IgG) | 23.8 | 7 -016 | g/l | – |
| 20 | Humoral Immunity Panel Immunoglobulin E1 (IgE1) | 592 | 0 - 100 | IU/ml | – |
| 21 | Lactate Dehydrogenase (LDH) | 300 | 120-230 | U/L | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Myopathies and Dermatomyositis · Parkinson's Disease and Spinal Disorders · Skin Diseases and Diabetes
Introduction
Dermatomyositis is an autoimmune illness that affects the striated muscle and skin. It usually shows muscular and cutaneous manifestation. Age above 40 years and females are risk factors for malignant tumor in patients with dermatomyositis. In our case study, a woman with malignant erythema as her first symptom was reported. She was later diagnosed with ovarian cancer and underwent subtractive surgery, which caused the erythema to rapidly subside. Most similar DM cases suffered from muscular disorders including painless proximal symmetrical weakness as well as weakness of the pharyngeal muscle, often leading to aspiration pneumonia and dysphagia.
Here, we reported this case with cutaneous symptoms in detailed clinical information including medicine use and clinical outcome. Cancer screening would be recommended in these intractable cases. On the other side, more researches are needed be focused on the immunity change of ovarian cancer.
A 68-year-old woman complaining of “erythema with itching on the head, face, trunk, and upper extremities for 2 months” visited the Department of Dermatology. Timetable was showed in Figure 1. The patient had erythema on her head, face, chest, V-zone, back of her hands and the extensor sides of both upper arms two months prior without any apparent cause. She also had edema in both of her eyelids, self-conscious itching, and sporadic water choking. Anti-Ro-52 and anti-nuclear antibodies were positive. Topical pimecrolimus ointment, hydroxychloroquine 200 mg bid, and prednisone 10 mg qd were administered. The patient noted that the rash had partially cleared up and her itching had subsided. The patient began to notice persistent erythematous itching on the top of his head three days ago. One of her sisters passed away from ovarian cancer.
Symptom and treatment timeline.
A skin lesion sample was taken after the patient was admitted, and the postoperative pathology was connective tissue disease. Anomalies in the bilateral H-reflex were observed on electromyography. The blood test showed IgG 23.8g/L, IgE 592IU/mL, ESR 41mm/h and LDH 353U/L, listed in Table 1.
Muscle strength and tone are normal bilaterally. Hormones, vitamin C, cetirizine, and omeprazole were administered with poor results. The lesions on the head and face progressed worse than before, with scattered erythema and maculopapular rashes all over the body and noticeable itching. Computed tomography (CT) scan revealed an enlarged uterus with several hypodense shadows. Cystic solid tumor in the pelvis was detected by gynecologic ultrasonography (O-RADS: grade 5). CA125 level of 325U/ml. The patient was then referred to the gynecology department.
The patient had a fever with a maximum temperature of 38.3 °C, expanding skin erythema, and “drunken” facial erythema on the day when she was referred to the gynecological department. An intense CT scan of the pelvic and abdominal cavity revealed cystic solid occupancy in the left adnexal region (maximum cross-sectional area: approximately 9.4x5.0 cm), which is thought to be ovarian cancer and has a limited, ill-defined demarcation between the uterus’ posterior wall and the nearby intestines. Multi-disciplinary treatment including rheumatology, anesthesiology, and dermatology was sought along with the patient’s medical history. The probable cause of malignant erythema was evaluated, and infectious causes like TROCH and EBV were ruled out. Gynecological surgery was recommended as soon as the skin symptoms had been controlled. The temperature and erythema were controlled after the glucocorticoid dosage was changed. The cytoreductive surgery was performed successfully. R0 was achieved. After the surgery, IgG 12.9g/L, IgE 582IU/mL, and ESR 14mm/h were measured and the skin symptoms were rapidly relieved. The changes were showed in Figure 2. Ovarian hypofractionated endometrioid adenocarcinoma, classified as stage IIB ovarian cancer, was the postoperative pathology. Chemotherapy of paclitaxel and carboplatin was administered. After 6 cycles of chemotherapy, the patient achieved clinical Complete Response of ovarian cancer. During the following 2 years of maintenance treatment with Niraparib, she showed no sign of recurrence of ovarian cancer, as well as the erythema. In the subsequent period, the patient underwent regular follow-up.
*Changes in the patient’s rash ((A) 2023.3.21; (B) 2023.3.23; (C) 2023.3.26; (D) 2023.4.2 Operation date: 2023.3.24).
Discussion
Ovarian cancer ranks the third most frequent malignant tumor of the female reproductive systems (1), following cervical and uterine body malignancy. In China, there were 27,200 fatal cases and 71,100 newly diagnosed cases of ovarian cancer in 2016 (2). Early-stage ovarian cancer typically has no noticeable symptoms, but in its latter stages, it may show up as abdominal fluid, bulk, distension, etc. The most typical symptom is acute onset of abdominal discomfort (3). Rarely, skin symptoms are presented as the initial sign of ovarian cancer. The patient in this case was initially diagnosed with skin connective tissue disease in the dermatology department with skin erythema as the primary symptom. The dermatologist remained cautious and discovered a pelvic tumor through a CT scan. Then the patient went to the gynecology department, where it was subsequently found that she had ovarian endometrioid adenocarcinoma of stage IIB.
The incidence of dermatomyositis (DM), an autoimmune illness with a rash and myopathy, is most prominent in people between the ages of 5–15 and 40 - 60. Typical skin lesions, such as Gottron papules, Gottron signs, and Heliotrope rash, are crucial for diagnosis and frequently come with itching or a burning discomfort (4). A myopathy is present in around 80% of DM patients, usually manifested as acute or subacute episodes of symmetrical proximal muscle weakness, either with or without increased muscle enzyme levels (5). The clinical progression of DM may not always resemble that of muscle disease (5). But in this case, the patient presented with a progressively worsening cutaneous symptom and mild muscle involvement. And in this way, it was a limitation that we did not perform the muscle biopsy and specific myositis antibodies test, including anti-TIF1γ, anti-NXP2, anti-Mi-2, anti-MDA-5 and anti-SAE antibodies.
Many malignancy-related cases of DM patients have been reported (6–8), as well as systematic reviews. After examination, some individuals with DM as the initial symptom may demonstrate recurrence indications, a poor response to immunological treatments, and the existence of hidden tumors (9). Critically, this case highlights the clinical observation that reinforces the link between DM and ovarian cancer: following cytoreductive surgery for ovarian endometrioid adenocarcinoma, which is also a kind of disease might be sensitive to immunity therapy, the patient’s cutaneous symptoms achieved significant improvement, with no sign of recurrence during follow-up. This finding is consistent with previous reports indicating that patients’ DM symptoms are relieved following tumor cytoreductive surgery (10), underscoring the pathogenic interplay between the autoimmune process and the underlying neoplasm. The resolution of the manifestations after surgery not only validates the diagnosis of cancer-associated DM but also suggests that tumor-derived antigens may have been driving the autoimmune response. Moreover, the absence of recurrence during follow-up further supports the efficacy of cytoreductive surgery in this case, emphasizing the importance of prompt tumor detection and intervention in DM patients with suspected malignancy.
The incidence of malignancy in patients with DM is approximately 10% (11). Breast cancer and ovarian cancer are the most common cancers in female DM patients. Additionally, females and age above 40 years are risk factors for combined malignancies in DM patients (12). Clinically, significant anti-TIF1 antibodies can help diagnose and prognosis disease outcomes in people with DM. In DM patients, some inflammatory cytokines (BAFF, sTNF-R1, sTNF-R2, etc.) may be indicators of malignancy (13). Combined DM in ovarian cancer patients has been hypothesized to be a prognostic factor for tumors (14). According to the risk categorization, all DM patients within 3 years of onset must undergo a cancer screening (15).
On the evidence of recent studies, the “second strike theory” has been put out to explain the etiology of cancer-associated DM. The “first strike” occurs when certain autoantibodies are produced in response to an infection, tumor, or damage. The “second strike” will initiate the dermatomyositis autoantigens’ upregulation and lead to an autoimmune response (16). Muscle cells and tumor cells may both express the same antigen, triggering a cross-immune reaction resulting in autoimmunity (16). Additionally, “foreign” antigens encoded by somatic mutations in particular tumor DNA and “wild-type” antigens found in particular tissues (such as skin, muscle, or viscera) might trigger cross-immune reactions (16). Additionally, tumor-infiltrating lymphocytes, PD-1/PD-L1 and CTLA-4 inhibitor pathways may contribute to the development of cancer-related dermatomyositis (16). In the context of this case, the resolution of DM symptoms post-cytoreductive surgery strongly suggests that the ovarian tumor was the primary driver of the autoimmune response, supporting the “second strike theory” and highlighting the clinical significance of targeting the underlying malignancy in managing cancer-associated DM.
Conclusion
DM is an autoimmune disease with an incidence of malignancy of approximately 10%. The pathogenesis of cancer-associated DM is unclear. Malignancy treatment may alleviate symptoms of DM. Patients who have a primary diagnosis of dermatomyositis need to be alerted that an additional cancer may exist. Consequently, based on the risk categorization of DM patients, cancer screening is essential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 2Zheng RS Zhang SW Zeng HM . Cancer incidence and mortality in China, 2016. J Natl Cancer Center. (2022) 2:1–9. doi: 10.1016/j.jncc.2022.02.002, PMID: 39035212 PMC 11256658 · doi ↗ · pubmed ↗
- 3Roett MA Evans P . Ovarian cancer: an overview. Am Fam Physician. (2009) 80:609–16. 19817326 · pubmed ↗
- 4Didona D Fania L Didona B Eming R Hertl M Di Zenzo G . Paraneoplastic dermatoses: A brief general review and an extensive analysis of paraneoplastic pemphigus and paraneoplastic dermatomyositis. Int J Mol Sci. (2020) 21:2178. doi: 10.3390/ijms 21062178, PMID: 32245283 PMC 7139382 · doi ↗ · pubmed ↗
- 5Dewane ME Waldman R Lu J . Dermatomyositis: Clinical features and pathogenesis. J Am Acad Dermatol. (2020) 82:267–81. doi: 10.1016/j.jaad.2019.06.1309, PMID: 31279808 · doi ↗ · pubmed ↗
- 6Piras M Panebianco M Garibaldi M Roberto M Merlonghi G Pellegrini P . A case of pathological complete response and resolution of dermatomyositis following neoadjuvant chemotherapy in HER 2-positive early breast cancer. Curr Oncol. (2021) 28:1957–61. doi: 10.3390/curroncol 28030182, PMID: PMC 816176934073827 · doi ↗ · pubmed ↗
- 7Kuroda H Yamaguchi A Sugata S Hamada T Moriuchi R Wada K . Advanced gallbladder cancer accompanied with cancer-associated dermatomyositis: A case report and literature review. Med (Baltimore). (2022) 101:e 29477. doi: 10.1097/MD.0000000000029477, PMID: 35801780 PMC 9259136 · doi ↗ · pubmed ↗
- 8Yilmaz U Ugurlu S . Dermatomyositis associated with papillary thyroid cancer: systematic review of the literature and a case report. J Clin Rheumatol. (2021) 27:168–71. doi: 10.1097/RHU.0000000000001048, PMID: 32803919 · doi ↗ · pubmed ↗