Childhood malnutrition, rickets, and anemia: a systematic review and meta-analysis on global prevalence, determinants, and public health implications
Yajuan Tan

TL;DR
This study reviews global childhood malnutrition, rickets, and anemia, finding that calcium, vitamin D, and targeted programs can reduce these issues.
Contribution
The study provides a comprehensive meta-analysis of interventions for childhood malnutrition and rickets across multiple regions.
Findings
Low calcium and vitamin D intake strongly associate with rickets (HR 1.51).
Nutrition programs show protective effects against malnutrition (HR 0.80–0.85).
Publication bias was detected in most study groups.
Abstract
The world continues to face major health risks through childhood malnutrition and rickets and anemia which hinder the development of physical and mental and immune system functions. The public health system needs to study determinants of health problems and their effective solutions. Our research team evaluated 96 studies, which include 153,694 participants from the Middle East and Africa and South and Southeast Asia and high-latitude regions through systematic review. The research team searched for studies in PubMed, Web of Science, Embase, Cochrane Library, and Google Scholar. The research team included observational studies and RCTs and cohort studies and individual participant data meta-analyses in their investigation. The study team evaluated research quality and bias risk through the use of Jadad scale and GRADE system and standard evaluation tools. The research team conducted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
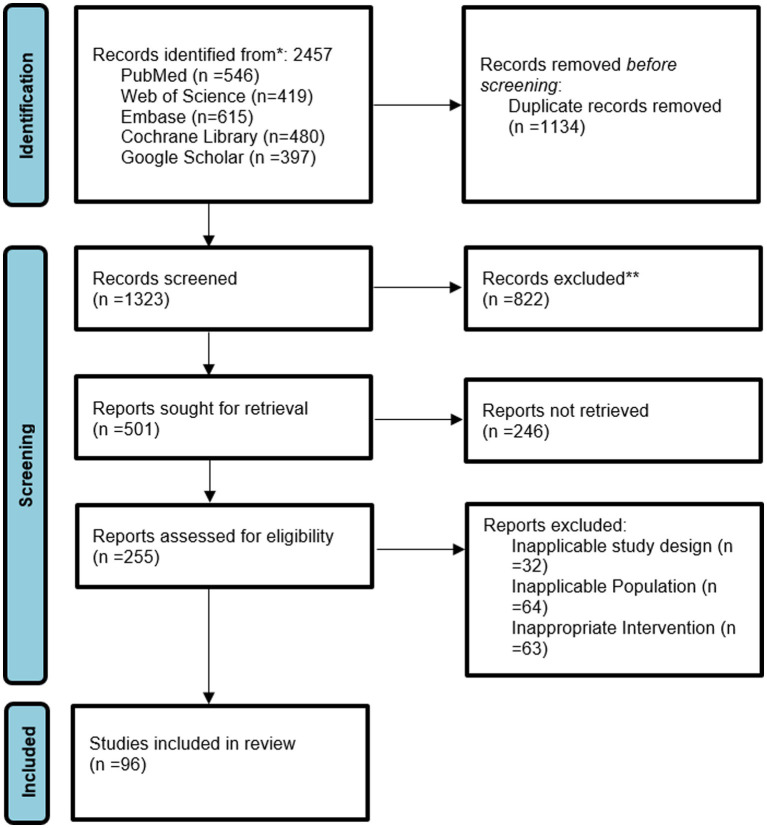 Figure 1
Figure 1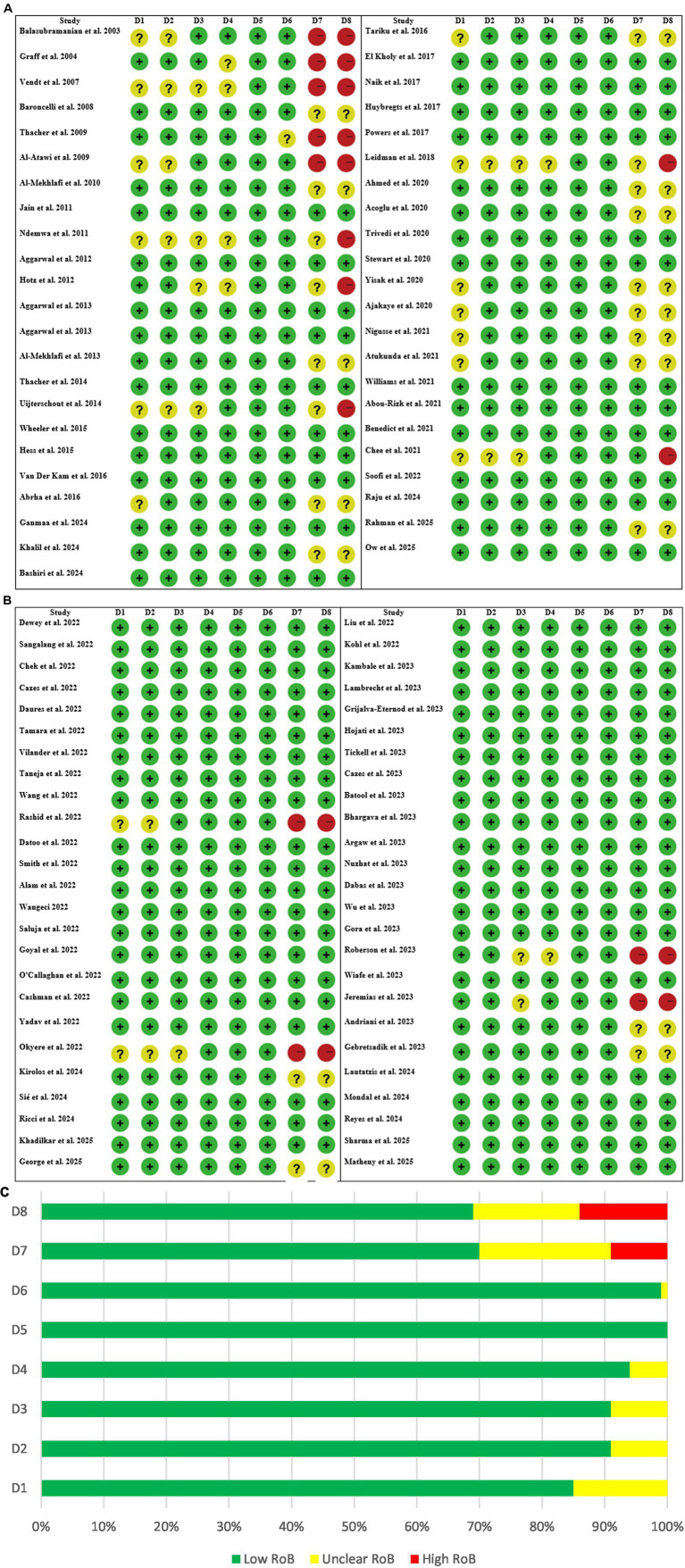 Figure 2
Figure 2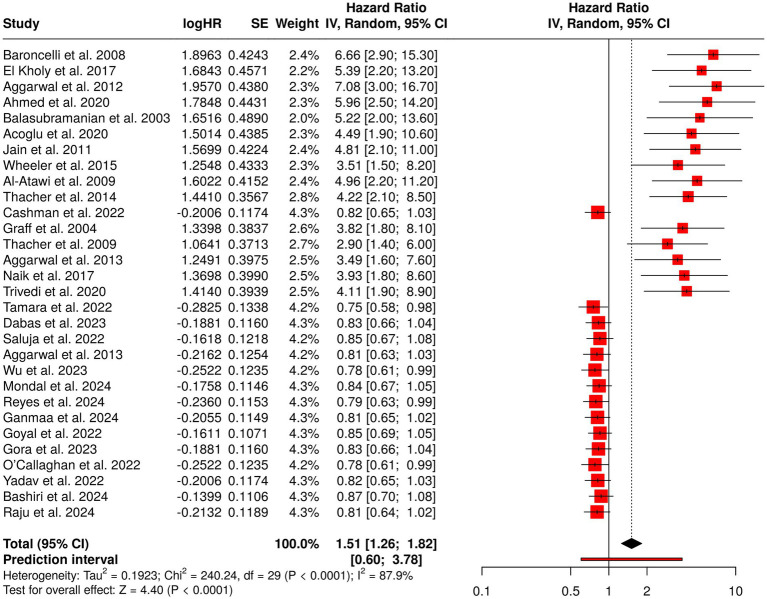 Figure 3
Figure 3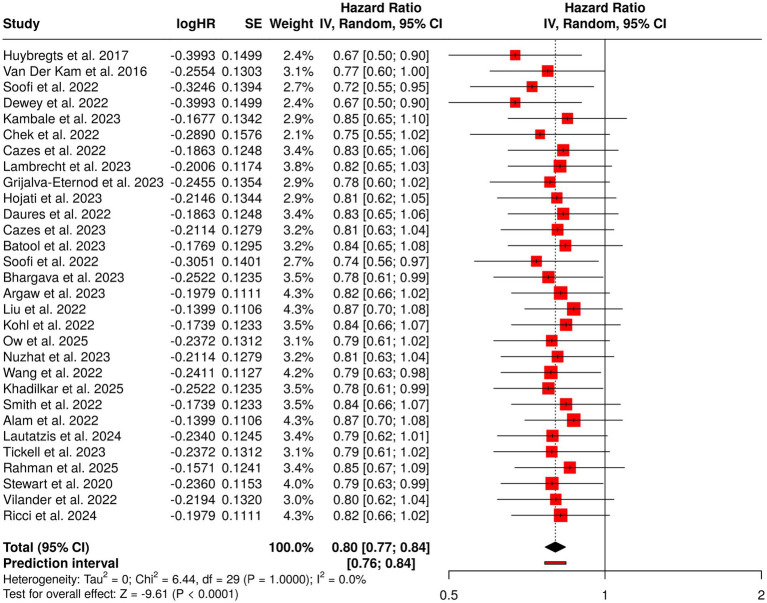 Figure 4
Figure 4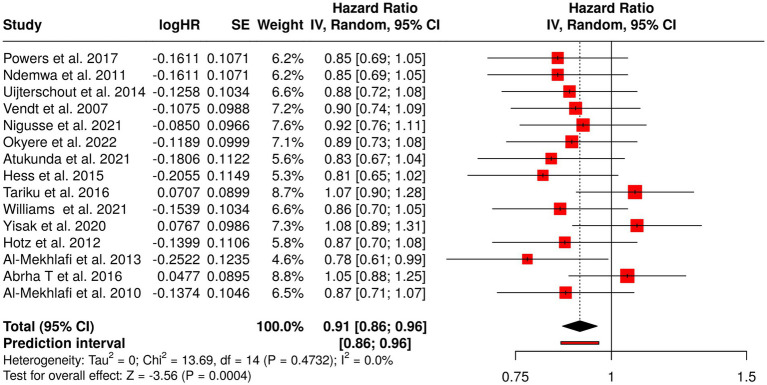 Figure 5
Figure 5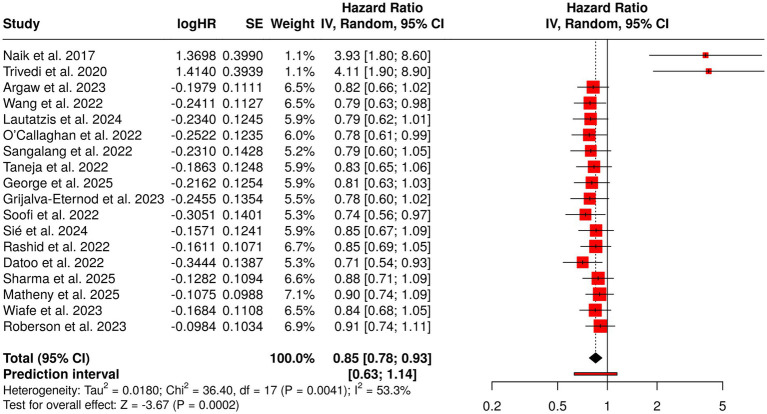 Figure 6
Figure 6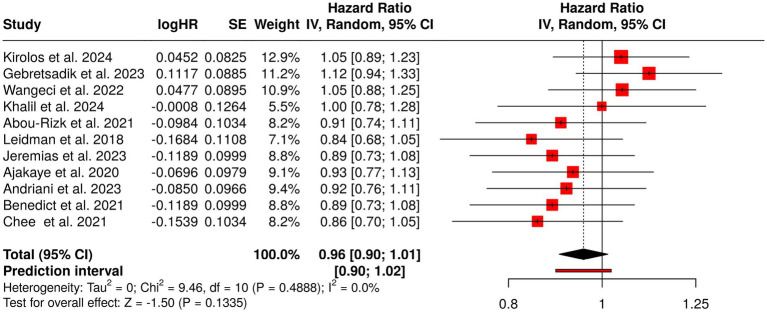 Figure 7
Figure 7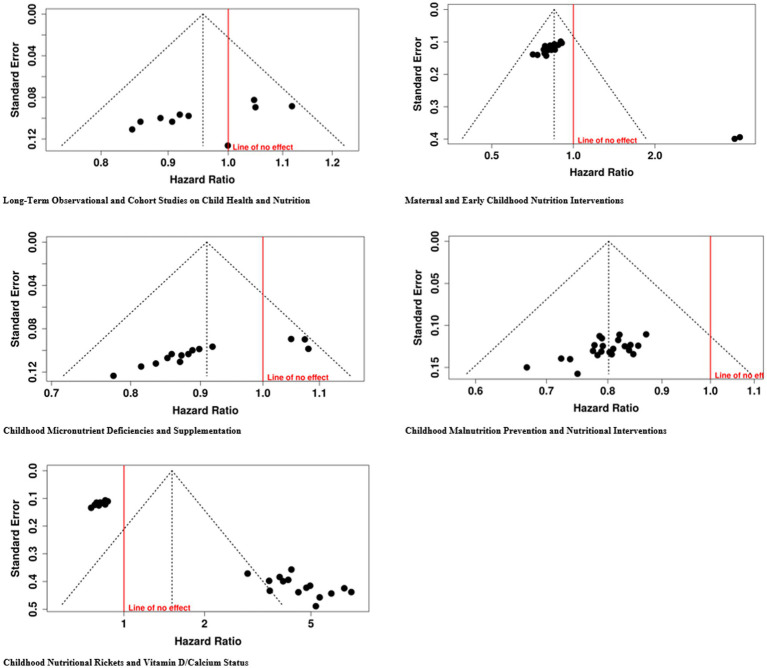 Figure 8
Figure 8| Database | Search strategy | Filters/Limits |
|---|---|---|
| PubMed | (“child*” OR “infant*” OR “toddler*” OR “preschool*”) AND (“malnutrition” OR “undernutrition” OR “stunting” OR “wasting” OR “underweight”) AND (“rickets” OR “vitamin D deficiency” OR “calcium deficiency”) AND (“anemia” OR “iron deficiency” OR “hemoglobin” OR “hematologic disorders”) | Humans, all languages, from inception to Dec 2025 |
| Embase | (‘child’/exp. OR ‘infant’/exp. OR child* OR infant* OR toddler*) AND (‘malnutrition’/exp. OR ‘undernutrition’/exp. OR malnutrition OR undernutrition OR stunting OR wasting OR underweight) AND (‘rickets’/exp. OR rickets OR ‘vitamin D deficiency’ OR ‘calcium deficiency’) AND (‘anemia’/exp. OR anemia OR ‘iron deficiency’ OR hemoglobin) | Human studies, all years, all languages |
| Web of Science | TS = (child* OR infant* OR toddler* OR preschool*) AND TS = (malnutrition OR undernutrition OR stunting OR wasting OR underweight) AND TS = (rickets OR “vitamin D deficiency” OR “calcium deficiency”) AND TS = (anemia OR “iron deficiency” OR hemoglobin) | All document types, no language restrictions |
| Cochrane Library | (“child*” OR “infant*” OR “toddler*”) AND (“malnutrition” OR “stunting” OR “wasting” OR “underweight”) AND (“rickets” OR “vitamin D deficiency” OR “calcium deficiency”) AND (“anemia” OR “iron deficiency”) | Cochrane reviews and trials, all years |
| Google Scholar | “child*” OR “infant*” OR “toddler*” AND malnutrition OR undernutrition OR stunting OR wasting OR underweight AND rickets OR “vitamin D deficiency” OR “calcium deficiency” AND anemia OR “iron deficiency” | First 200 results per search, all years, all languages |
| Author (1st author et al.) | Year | Country | Study type | Population | Sample size | Intervention | Outcome | Outcome definition/Cut-offs | Effect metrics |
|---|---|---|---|---|---|---|---|---|---|
| Balasubramanian et al. ( | 2003 | India | Comparative | Children/adolescents | 80 | Ca ± vit D | Healing | Clinical and x-ray | OR 4.8 if Ca < 300 mg |
| Graff et al. ( | 2004 | Nigeria | Observational | Rickets children | 30 | Calcium supplementation | Ca absorption | Fractional absorption | ↑ absorption ( |
| Al-Mekhlafi et al. ( | 2010 | Malaysia | Cross-sectional study | Aboriginal school children | 250 | Observational | Giardiasis and vitamin A status | Stool exam; serum retinol <0.7 μmol/L | Giardia infection associated with poor vitamin A status |
| El Kholy et al. ( | 2017 | Egypt | Prospective cohort | Children with rickets | 139 | Standard therapy + genetics | Radiologic healing | X-ray healing | Genotype influenced response |
| Thacher et al. ( | 2009 | Nigeria | Dietary study | Rickets children | 34 | Ca + ergocalciferol | Ca/Zn absorption | Fractional absorption | ↑ Ca absorption ( |
| Thacher et al. ( | 2014 | Nigeria | RCT | Ca-deficiency rickets | 72 | Ca ± vitamin D | Radiologic healing | Score ≤1.5 | Combined therapy superior (67%) |
| Aggarwal et al. ( | 2012 | India | Case–control | Rickets vs. controls | 135 | Dietary comparison | Ca intake | Below RDA | Lower intake ( |
| Aggarwal et al. ( | 2013 | India | RCT | Rickets children | 67 | Vit D, Ca or both | Radiologic healing | X-ray resolution | Combination best (50%) |
| Ahmed et al. ( | 2020 | Bangladesh | Case–control | Rural children | 128 | Diet and biochemical | 25-OH-D, Ca | <25 nmol/L | Ca deficiency major contributor |
| Acoglu et al. ( | 2020 | Turkey | Case series | Refugee children | 77 | Clinical evaluation | Prevalence | Radiographic criteria | 28.5% rickets |
| Jain et al. ( | 2011 | India | Observational | Breastfed infants | 360 | None | 25-OH-D | <50 nmol/L | High deficiency |
| Wheeler et al. ( | 2015 | New Zealand | Surveillance | Pediatric rickets | 106 | Monitoring | Incidence | Radiographic confirmed | 2.2/100,000/year |
| Naik et al. ( | 2017 | India | RCT | Mother-infant dyads | 180 | Maternal vit D | Infant 25-OH-D | <50 nmol/L | ↑ levels ( |
| Trivedi et al. ( | 2020 | India | RCT | Mother-infant dyads | 210 | Maternal vit D | Infant 25-OH-D | <50 nmol/L | ↑ levels ( |
| Al-Atawi et al. ( | 2009 | Saudi Arabia | Retrospective | Infants | 283 | Chart review | Vit D status | <12 nmol/L | Severe deficiency common |
| Huybregts et al. ( | 2017 | Burkina Faso and Mali | Cluster RCT | 6–24 mo children | 2000 | SQ-LNS | Acute malnutrition | WLZ < −2 | Reduced prevalence |
| Van Der Kam et al. ( | 2016 | Nigeria | RCT | Post-illness children | 399 | RUTF vs. micronutrients | Nutritional recovery | MUAC/WLZ | Improved recovery |
| Soofi et al. ( | 2022 | Pakistan | Cluster RCT | Pregnant women and infants | 1,352 | LNS supplementation | Stunting | LAZ < −2 | ↓ stunting ( |
| Dewey et al. ( | 2022 | Multicountry | IPD Meta-analysis | 6–24 mo children | 36,795 | SQ-LNS | Severe wasting/stunting | LAZ/WLZ < −3 | PR 0.69 (wasting) |
| Kambale et al. ( | 2023 | DR Congo | RCT | SAM children | 400 | Probiotics + RUTF | Diarrhea duration | Days ill | Reduced duration ( |
| Sangalang et al. ( | 2022 | Philippines | Cluster RCT | Schoolchildren | 1,558 | WaSH | BMI, hydration | BMI-for-age | Improved hygiene |
| Chek et al. ( | 2022 | Malaysia | Cluster RCT (protocol) | Urban poor <5 yrs | 600 | Positive deviance program | Undernutrition | WAZ/HAZ < −2 | Protocol |
| Cazes et al. ( | 2022 | DR Congo | Non-inferiority RCT | 6–59 mo children | 981 | OptiMA simplified | Recovery | MUAC ≥125 mm | Non-inferior |
| Lambrecht et al. ( | 2023 | Bangladesh | Cluster RCT | <5 yrs | 2,700 | Homestead food production | Diarrhea, ARI | 2-week recall | ↓ diarrhea |
| Grijalva-Eternod et al. ( | 2023 | Somalia | 2 × 2 factorial cluster RCT | IDP households | 1,122 | Cash transfer + mHealth | Malnutrition risk | MUAC <125 mm | Improved food security |
| Hojati et al. ( | 2023 | Iran | RCT (protocol) | Preschool children | 120 | Nutrition mobile app | Knowledge, WAZ/HAZ | <−2 SD | Protocol |
| Daures et al. ( | 2022 | Niger | 3-arm RCT (protocol) | 6–59 mo children | 1,200 | Simplified community care | Recovery | MUAC ≥125 mm | Non-inferiority design |
| Tamara et al. ( | 2022 | Indonesia | Double-blind RCT | Children with pulmonary TB | 84 | Vitamin D supplementation | Fever and cough resolution time | Clinical symptom resolution | Faster fever resolution ( |
| Tickell et al. ( | 2023 | Kenya | RCT | Caregivers and children 6–59 mo | 1,200 | Family MUAC + 2-way SMS | Early wasting detection | MUAC <125 mm | Improved detection rates |
| Cazes et al. ( | 2023 | DR Congo | Non-inferiority RCT | SAM children | 1,282 | Reduced RUTF dosage | Nutritional recovery | MUAC ≥125 mm and no edema | Reduced dose non-inferior |
| Batool et al. ( | 2023 | Pakistan | Double-blind parallel RCT | Children with severe acute malnutrition (SAM) | 110 | Prebiotic supplementation vs. placebo | Nutritional recovery; gut health | MUAC ≥125 mm; WHZ ≥ −2 | Improved weight gain and gut biomarkers ( |
| Rahman et al. ( | 2025 | Bangladesh | RCT protocol (CRADLE trial) | Pregnant women and young children | 800 | Installation of household concrete floors | Maternal and child health; infection; growth | Diarrhea prevalence; anthropometry | Protocol – results pending |
| Vilander et al. ( | 2022 | Mali and Nicaragua | RCT | Infants 6–12 months | 95 | Dietary rice bran supplementation | Microbiota diversity; enteric dysfunction | Fecal sIgA; microbiome indices | ↑ microbiota diversity and sIgA ( |
| Soofi et al. ( | 2022 | Pakistan | Cluster RCT | Children <18 months | 2,357 | Unconditional cash transfer ± LNS ± BCC | Stunting prevention | LAZ < −2 SD | Reduced stunting risk (RR ≈ 0.80) |
| Bhargava et al. ( | 2023 | India | Open-label cluster RCT | Household contacts of pulmonary TB patients | 10,345 | Nutritional supplementation (food rations) | TB incidence | Microbiologically confirmed TB | ~39% relative reduction in TB incidence |
| Kirolos et al. ( | 2024 | Malawi | Prospective observational cohort study | Adolescents with prior severe childhood malnutrition | 352 | Long-term follow-up of SAM survivors (LOSCM study) | Growth, body composition, cardiometabolic risk, cognitive outcomes | Anthropometry; metabolic markers; neurocognitive testing | Persistent deficits in growth and lean mass; increased cardiometabolic risk indicators |
| Argaw et al. ( | 2023 | Burkina Faso | 2 × 2 factorial individually randomized controlled trial | Pregnant and lactating women and their infants | 1,897 | Fortified balanced energy–protein supplementation during pregnancy and/or lactation | Infant growth outcomes; stunting | LAZ; WLZ; WAZ; stunting (LAZ < −2) | Improved linear growth in supplemented groups |
| Liu et al. ( | 2022 | China | Cluster randomized clinical trial | Primary school children | 1,392 | Multifaceted obesity prevention intervention (nutrition education + physical activity + behavioral change) | BMI; overweight/obesity prevalence | BMI z-scores; overweight/obesity per WHO criteria | Significant reduction in BMI gain and obesity prevalence |
| Kohl et al. ( | 2022 | Haiti | Randomized controlled trial protocol | Caregivers and young children | 600 | Integrated responsive parenting, nutrition and hygiene intervention (Grandi Byen) | Child growth and development; caregiving practices | Anthropometry; developmental scales | Protocol – effectiveness outcomes pending |
| Ow et al. ( | 2025 | Vietnam | Randomized controlled trial | Children with or at risk for undernutrition | 321 | Long-term oral nutritional supplementation + dietary counseling | Growth; body composition; bone mineralization | Height-for-age; body fat %; bone mineral density | Significant improvements in growth and bone mineralization |
| Nuzhat et al. ( | 2023 | Bangladesh | Randomized clinical trial | Severely malnourished young infants | 160 | Probiotic and synbiotic supplementation | Ponderal and linear growth | Weight-for-age (WAZ); Length-for-age (LAZ); WLZ | Improved weight gain; modest improvement in linear growth |
| Sié et al. ( | 2024 | Burkina Faso | Randomized controlled trial (secondary analysis) | Infants | 21,832 | Single-dose azithromycin | Anthropometric growth outcomes | Weight-for-age; Height-for-age; MUAC | No clinically meaningful improvement in growth outcomes |
| Taneja et al. ( | 2022 | India | Factorial individually randomized controlled trial | Women (preconception/pregnancy) and children to 24 months | 7,500 | Integrated package: health, nutrition, psychosocial stimulation and WaSH | Birth outcomes; linear growth at 24 months | LAZ at 24 months; birth weight | Improved birth weight; modest gains in linear growth |
| Ricci et al. ( | 2024 | South Africa | Randomized controlled trial | Infants aged 6–9 months | 500 | Egg introduced as early complementary food | Growth (length and weight gain) | LAZ; WAZ; WLZ | Improved length gain; reduced risk of stunting |
| Wang et al. ( | 2022 | Tanzania | Double-blind randomized controlled trial | Pregnant women and their children | 1,000 | Prenatal and postnatal maternal multiple micronutrient supplementation | Child growth; morbidity | LAZ; WAZ; morbidity incidence | Improved child growth indicators; reduced morbidity risk |
| Gebretsadik et al. ( | 2023 | Ethiopia (Tigray) | Cross-sectional study | Children aged 6–59 months in war-affected communities | 614 | Exposure: conflict-related, household and community-level factors | Acute malnutrition prevalence | WHZ < −2 SD and/or MUAC <125 mm | High prevalence of acute malnutrition; associated with food insecurity, displacement, poor sanitation |
| Khadilkar et al. ( | 2025 | India | Randomized controlled trial (6 months) | Children aged 3–6.9 years with growth faltering | 330 | Oral nutritional supplementation + dietary counseling vs. counseling alone | Linear catch-up growth | Height-for-age z-score (HAZ); growth velocity | Significant improvement in linear growth and catch-up growth rates |
| Datoo et al. ( | 2022 | Burkina Faso | Phase 1/2b randomized controlled trial | Children (5–17 months at enrollment) | 450 | R21/Matrix-M malaria vaccine | Clinical malaria incidence; immunogenicity | PCR-confirmed clinical malaria; antibody titers | High vaccine efficacy maintained over 2 years; strong immunogenic response |
| Smith et al. ( | 2022 | Zimbabwe | Randomized controlled trial protocol (CHAIN trial) | Infants and young children (IYCF intervention in rural communities) | 1,920 | Improved infant and young child feeding (IYCF) intervention integrated with agriculture and nutrition support | Child growth; dietary diversity; stunting | LAZ; minimum dietary diversity; stunting (LAZ < −2) | Protocol – outcomes pending |
| George et al. ( | 2025 | Democratic Republic of the Congo | Cluster-randomized controlled trial | Households with young children in cholera-endemic areas | 2,400 | PICHA7 WASHmobile program (water, sanitation, hygiene + mHealth support) | Diarrhea; cholera; child growth | Caregiver-reported diarrhea; confirmed cholera; anthropometry | Reduced diarrhea and cholera incidence; improved growth indicators |
| Alam et al. ( | 2022 | Bangladesh | Double-blind randomized controlled trial protocol | Children with severe acute malnutrition (SAM) | 124 | L-Carnitine supplementation vs. placebo | Rate of weight gain; biomarkers of environmental enteric dysfunction (EED) | g/kg/day weight gain; EED biomarkers | Protocol – effectiveness outcomes pending |
| Lautatzis et al. ( | 2024 | Bangladesh | Secondary analysis of randomized trial | Infants of mothers receiving supplementation | 1,100 | Maternal vitamin D supplementation | Infantile rickets incidence | Clinical and radiological diagnosis of rickets | Maternal supplementation reduced risk of infantile rickets |
| Dabas et al. ( | 2023 | India | Randomized controlled open-label trial | Children with nutritional rickets | 120 | Daily vs. weekly oral vitamin D3 | Correction of rickets | Radiological and biochemical resolution | Daily vitamin D3 achieved faster correction than weekly regimen |
| Saluja et al. ( | 2022 | India | Randomized clinical trial | Children with nutritional rickets | 100 | Low-dose depot oral vitamin D3 vs. daily oral vitamin D3 | Rickets resolution | Radiological improvement and serum 25(OH)D normalization | Both regimens effective; daily dose slightly faster |
| Aggarwal et al. ( | 2013 | India | Randomized controlled trial | Children with nutritional rickets | 180 | Standard treatment vs. structured supplementation | Nutritional rickets resolution | Radiological scoring and biochemical markers | Structured regimen improved biochemical correction |
| Wu et al. ( | 2023 | Global (IPD meta-analysis) | Systematic review + individual participant data meta-analysis | Children/adolescents with vitamin D deficiency | 3,200 | Vitamin D supplementation | Bone density improvement | BMD z-score; DXA measurements | Supplementation improved bone density; effect modified by baseline deficiency |
| Wangeci ( | 2022 | Kenya | Observational study | Children 6–59 months with acute malnutrition | 245 | N/A (cross-sectional assessment) | Nutritional rickets prevalence | Clinical and radiological diagnosis | High prevalence of rickets among SAM children |
| Mondal et al. ( | 2024 | India | Open-label randomized controlled trial | Children aged 1–10 years with vitamin D deficiency | 130 | Daily vs. fortnightly oral vitamin D3 | Correction of vitamin D deficiency | Serum 25(OH)D normalization | Daily dosing more effective than fortnightly for rapid correction |
| Reyes et al. ( | 2024 | Multinational | Randomized controlled trial | Young children (different latitudes) | 1,560 | Weekly vitamin D supplementation | Prevention of acute respiratory infections | Clinically diagnosed ARI episodes | Vitamin D reduced incidence of ARI, effect stronger at higher latitudes |
| Ganmaa et al. ( | 2024 | Mongolia | Multicentre double-blind randomized placebo-controlled trial | Schoolchildren | 4,700 | Vitamin D supplementation | Fracture prevention (secondary outcome) | Incident fractures recorded | Vitamin D reduced fracture risk modestly in school-aged children |
| Goyal et al. ( | 2022 | India | Randomized controlled trial | Infants | 150 | Sunlight exposure vs. oral vitamin D supplementation | Prevention of vitamin D deficiency | Serum 25(OH)D levels < 50 nmol/L | Vitamin D supplementation more effective than sunlight alone |
| Gora et al. ( | 2023 | India | Randomized controlled trial | Infants with symptomatic vitamin D deficiency | 120 | Daily vs. monthly oral vitamin D3 | Correction of vitamin D deficiency | Serum 25(OH)D normalization | Daily dosing achieved faster correction than monthly dosing |
| O’Callaghan et al. ( | 2022 | Bangladesh | Follow-up of randomized controlled trial | Offspring of mothers receiving prenatal/postpartum vitamin D | 850 | Maternal prenatal and postpartum vitamin D supplementation | Offspring bone mass and muscle strength | DXA bone mineral density; grip strength | Increased bone mass and muscle strength at early childhood |
| Roberson et al. ( | 2023 | USA | Secondary analysis of RCT (VITC, thiamine, hydrocortisone in sepsis) | Sepsis survivors | 501 | IV vitamin C, thiamine, and hydrocortisone | Cognitive, psychological, functional outcomes | Standardized neurocognitive and psychological assessments | No significant long-term cognitive or functional benefit observed |
| Cashman et al. ( | 2022 | Multinational (High latitude, dark-skinned populations) | IPD meta-analysis of RCTs | Children and adults | 1,230 | Vitamin D supplementation | Dietary requirement estimation for vitamin D | Serum 25(OH)D ≥ 50 nmol/L | Provided evidence-based vitamin D intake recommendations for high-latitude dark-skinned populations |
| Khalil et al. ( | 2024 | UK and Europe | Protocol – prospective multicentre mixed-methods feasibility study | Monochorionic twin pregnancies with early-onset selective fetal growth restriction | 60 | RCT: intervention vs. expectant management | Feasibility outcomes; maternal and neonatal safety | Recruitment, retention, protocol adherence | Protocol study – feasibility outcomes; effectiveness pending |
| Yadav et al. ( | 2022 | India | Randomized controlled trial | Term breastfed infants | 140 | Vitamin D3 800 IU/day vs. 400 IU/day | Prevention of vitamin D deficiency | Serum 25(OH)D < 50 nmol/L | 800 IU/day more effective than 400 IU/day |
| Bashiri et al. ( | 2024 | Saudi Arabia | Randomized controlled trial | Children with epilepsy on antiseizure medications | 120 | Vitamin D supplementation | Serum vitamin D levels; seizure control | Serum 25(OH)D; seizure frequency | Improved vitamin D status; no significant change in seizures |
| Raju et al. ( | 2024 | India | Double-blind randomized controlled trial | Young children | 160 | Vitamin D supplementation | Prevention of acute respiratory infections | Clinically diagnosed ARI | Reduced ARI incidence compared with placebo |
| Sharma et al. ( | 2025 | USA | Randomized controlled study | Children with obesity and difficult-to-treat asthma | 75 | 1-year weight management program | Asthma control; weight | BMI z-score; asthma control questionnaire | Improved weight and asthma outcomes |
| Matheny et al. ( | 2025 | USA | Randomized controlled trial | Adults undergoing contrast procedures | 210 | Intervention to prevent contrast-associated AKI | Incidence of AKI | Serum creatinine ≥0.3 mg/dL or ≥50% increase | Sustained reduction in AKI incidence post-intervention |
| Wiafe et al. ( | 2023 | Ghana | Randomized controlled trial | Early adolescents | 240 | Nutrition education and counselling | Nutritional status; anemia | Hemoglobin <12 g/dL; anthropometry | Improved hemoglobin levels and nutritional status |
| Al-Mekhlafi et al. ( | 2013 | Yemen | Randomized controlled trial | Children 6–59 months | 300 | Vitamin A supplementation | Iron status; anemia | Hemoglobin <11 g/dL; serum ferritin | Vitamin A improved iron indices and reduced anemia prevalence |
| Powers et al. ( | 2017 | USA | Randomized clinical trial | Young children with nutritional iron-deficiency anemia | 150 | Ferrous sulfate vs. iron polysaccharide complex | Hemoglobin concentration | Hb < 11 g/dL | Both treatments increased Hb; ferrous sulfate slightly faster response |
| Stewart et al. ( | 2020 | Madagascar | Multi-arm cluster-randomized controlled trial | Children 6–24 months | 1,500 | Lipid-based nutrient supplementation (LNS) | Anemia; micronutrient status | Hb < 11 g/dL; serum ferritin | Reduced anemia prevalence and improved micronutrient levels |
| Abrha et al. ( | 2016 | Ethiopia | Community-based cross-sectional study | Preschool children | 420 | Observational | Clinical manifestations of vitamin A deficiency | Bitot’s spots, night blindness | High prevalence of VAD in rural district; associated with poor diet |
| Nigusse and Gebretsadik ( | 2021 | Ethiopia | Cross-sectional study | Children 6–59 months | 500 | Observational | Vitamin A supplementation coverage; ocular signs | Clinical VAD signs; supplementation status | Moderate coverage; VAD signs present in unsupplemented children |
| Okyere et al. ( | 2022 | Ghana | Demographic and Health Survey analysis | Children 6–59 months | 12,000 | Observational | Trends and inequalities in vitamin A supplementation | Receipt of VAS in last 6 months | Coverage improved over 2003–2014; inequalities by region and SES |
| Atukunda et al. ( | 2021 | Uganda | Secondary analysis of RCT | Children 6–59 months | 400 | Education trial; urine iodine markers | Growth and development | Height-for-age, weight-for-age, cognitive development | Urinary iodine associated with better growth outcomes |
| Hess et al. ( | 2015 | Burkina Faso | Cluster-randomized trial | Children 6–36 months | 1,200 | Small-quantity LNS + iodized salt | Iodine status | Urinary iodine concentration (UIC) | Improved iodine status in LNS + salt group |
| Tariku et al. ( | 2016 | Ethiopia | Community-based cross-sectional study | Preschool children 1–5 years | 450 | Observational | Vitamin A deficiency and determinants | Serum retinol <0.7 μmol/L | VAD prevalent; associated with diet and socioeconomic factors |
| Williams et al. ( | 2021 | Malawi | Observational survey | Children 6–59 months | 1,100 | Observational | Vitamin A deficiency and excess | Serum retinol; plasma retinol >1.3 μmol/L | VAD declined; some children had elevated vitamin A levels |
| Yisak et al. ( | 2020 | Ethiopia | Mixed methods cross-sectional | Preschool children 1–5 years | 520 | Observational | Clinical VAD prevalence | Bitot’s spots, night blindness | Prevalence of clinical VAD; associated with diet and maternal knowledge |
| Hotz et al. ( | 2012 | Zambia | Observational cross-sectional | Preschool children | 360 | Observational | Plasma retinol; infection status | Serum retinol <0.7 μmol/L | Vitamin A intake and infection influenced plasma retinol levels |
| Abou-Rizk et al. ( | 2021 | Lebanon | Cross-sectional survey | Syrian refugee mothers and children <5 years | 800 | Observational | Anemia and nutritional status | Hemoglobin <11 g/dL; anthropometry | High prevalence of anemia and undernutrition among refugees |
| Leidman et al. ( | 2018 | Bangladesh | Cross-sectional survey | Rohingya children 6–59 months | 1,200 | Observational | Acute malnutrition and anemia | WHZ < −2 SD; Hb < 11 g/dL | High rates of acute malnutrition and anemia in refugee camp |
| Jeremias et al. ( | 2023 | Lebanon | Mixed-methods study | Syrian refugee children 6–23 months | 420 | Observational | Anemia prevalence | Hemoglobin <11 g/dL | High anemia prevalence; qualitative insights from mothers and healthcare staff |
| Ajakaye et al. ( | 2020 | Nigeria | Cross-sectional survey | Children in IDP camps | 300 | Observational | Malaria, anemia, malnutrition | Hb < 11 g/dL; WHZ < −2 SD; malaria parasitemia | High prevalence of malaria, anemia, and malnutrition; risk factors identified |
| Ndemwa et al. ( | 2011 | Kenya | Cross-sectional survey | Women and children in Kakuma Refugee Camp | 450 | Observational | Iron status and hemoglobin | Serum ferritin <12 μg/L; Hb < 11 g/dL | Availability of micronutrient powder associated with improved iron status |
| Uijterschout et al. ( | 2014 | Netherlands | Cross-sectional study | Healthy young children | 200 | Observational | Iron deficiency prevalence | Serum ferritin <12 μg/L; Hb < 11 g/dL | Identified risk factors for iron deficiency in low-risk population |
| Vendt et al. ( | 2007 | Estonia | Cross-sectional study | Infants 9–12 months | 180 | Observational | Iron deficiency anemia | Hb < 11 g/dL; ferritin <12 μg/L | Moderate prevalence of IDA; causes mainly dietary |
| Andriani et al. ( | 2023 | Indonesia | Repeated cross-sectional surveys; multilevel analysis | Children under 5 | 5,000 | Observational | Triple burden of malnutrition | Stunting, wasting, overweight | Determinants include socioeconomic and feeding practices |
| Benedict et al. ( | 2021 | Thailand | Cross-sectional study | Children under 5 | 1,200 | Observational | Double burden of malnutrition | Stunting and overweight | Associated with suboptimal infant/child feeding practices |
| Chee et al. ( | 2021 | Malaysia | Cross-sectional study | Pre-adolescent children | 350 | Observational | Vitamin D status | Serum 25(OH)D < 50 nmol/L | Vitamin D deficiency associated with modifiable lifestyle factors (sun exposure, diet) |
| Rashid et al. ( | 2022 | Malaysia | Cluster randomized controlled trial protocol | Preschool child–parent dyads | 460 | Interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) program | Weight-related behaviors; BMI | BMI z-scores; behavioral assessments | Protocol – behavioral and BMI outcomes pending |
| Study | Year | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Overall quality of evidence |
|---|---|---|---|---|---|---|---|
| Balasubramanian et al. | 2003 | Moderate | Not serious | Serious | Serious | Undetected | Low |
| Graff et al. | 2004 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Vendt et al. | 2007 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Baroncelli et al. | 2008 | Moderate | Not serious | Serious | Serious | Undetected | Low |
| Thacher et al. | 2009 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Al-Atawi et al. | 2009 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Al-Mekhlafi et al. | 2010 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Jain et al. | 2011 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Ndemwa et al. | 2011 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Hotz et al. | 2012 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Aggarwal et al. | 2012 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Aggarwal et al. | 2013 | Low | Not serious | Serious | Moderate | Undetected | Moderate |
| Aggarwal et al. | 2013 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Al-Mekhlafi et al. | 2013 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Uijterschout et al. | 2014 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Thacher et al. | 2014 | Low | Not serious | Serious | Moderate | Undetected | Moderate |
| Wheeler et al. | 2015 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Hess et al. | 2015 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Abrha et al. | 2016 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Tariku et al. | 2016 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Van Der Kam et al. | 2016 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| El Kholy et al. | 2017 | Moderate | Not applicable / Not serious | Serious | Moderate | Undetected | Low |
| Naik et al. | 2017 | Low | Not serious | Serious | Moderate | Undetected | Moderate |
| Huybregts et al. | 2017 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Powers et al. | 2017 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Leidman et al. | 2018 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Ahmed et al. | 2020 | Moderate | Not applicable / Not serious | Serious | Moderate | Undetected | Low |
| Acoglu et al. | 2020 | Moderate | Not applicable / Not serious | Serious | Moderate | Undetected | Low |
| Trivedi et al. | 2020 | Low | Not serious | Serious | Moderate | Undetected | Moderate |
| Stewart et al. | 2020 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Yisak et al. | 2020 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Ajakaye et al. | 2020 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Nigusse et al. | 2021 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Atukunda et al. | 2021 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Williams et al. | 2021 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Abou-Rizk et al. | 2021 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Benedict et al. | 2021 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Chee et al. | 2021 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Soofi et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Dewey et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Sangalang et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Chek et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Cazes et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Daures et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Tamara et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Vilander et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Liu et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Kohl et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Taneja et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Wang et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Rashid et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Datoo et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Smith et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Alam et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Saluja et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Wangeci et al. | 2022 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Goyal et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| O’Callaghan et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Cashman et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Yadav et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Okyere et al. | 2022 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Kambale et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Lambrecht et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Grijalva-Eternod et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Hojati et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Tickell et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Cazes et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Batool et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Bhargava et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Argaw et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Nuzhat et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Dabas et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Wu et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Gora et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Roberson et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Wiafe et al. | 2023 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Jeremias et al. | 2023 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Andriani et al. | 2023 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Kirolos et al. | 2024 | Moderate | Not serious | Serious | Moderate | Undetected | Low |
| Sié et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Ricci et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Lautatzis et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Mondal et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Reyes et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Ganmaa et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Khalil et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Bashiri et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Raju et al. | 2024 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Rahman et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Ow et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Khadilkar et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| George et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Sharma et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Matheny et al. | 2025 | Low | Not serious | Not serious | Moderate | Undetected | Moderate |
| Study (First author et al.) | Randomization (0–2) | Blinding (0–2) | Withdrawals/Dropouts (0–1) | Total Jadad Score |
|---|---|---|---|---|
| Balasubramanian et al. ( | 1 | 1 | 1 | 3 |
| Graff et al. ( | 2 | 1 | 1 | 4 |
| Vendt et al. ( | 1 | 1 | 1 | 3 |
| Baroncelli et al. ( | 2 | 1 | 1 | 4 |
| Thacher et al. ( | 2 | 1 | 1 | 4 |
| Al-Atawi et al. ( | 1 | 1 | 1 | 3 |
| Al-Mekhlafi et al. ( | 1 | 1 | 1 | 3 |
| Jain et al. ( | 2 | 1 | 1 | 4 |
| Ndemwa et al. ( | 1 | 1 | 1 | 3 |
| Aggarwal et al. ( | 1 | 1 | 1 | 3 |
| Hotz et al. ( | 1 | 1 | 1 | 3 |
| Aggarwal et al. ( | 2 | 1 | 1 | 4 |
| Aggarwal et al. ( | 2 | 1 | 1 | 4 |
| Al-Mekhlafi et al. ( | 2 | 1 | 1 | 4 |
| Thacher et al. ( | 2 | 2 | 1 | 5 |
| Uijterschout et al. ( | 1 | 1 | 1 | 3 |
| Wheeler et al. ( | 2 | 1 | 1 | 4 |
| Hess et al. ( | 2 | 1 | 1 | 4 |
| Abrha et al. ( | 1 | 1 | 1 | 3 |
| Tariku et al. ( | 1 | 1 | 1 | 3 |
| Van Der Kam et al. ( | 2 | 1 | 1 | 4 |
| El Kholy et al. ( | 2 | 1 | 1 | 4 |
| Naik et al. ( | 2 | 2 | 1 | 5 |
| Huybregts et al. ( | 2 | 1 | 1 | 4 |
| Powers et al. ( | 2 | 1 | 1 | 4 |
| Leidman et al. ( | 1 | 1 | 1 | 3 |
| Ahmed et al. ( | 1 | 1 | 1 | 3 |
| Acoglu et al. ( | 1 | 1 | 1 | 3 |
| Stewart et al. ( | 2 | 1 | 1 | 4 |
| Trivedi et al. ( | 2 | 2 | 1 | 5 |
| Yisak et al. ( | 1 | 1 | 1 | 3 |
| Ajakaye et al. ( | 1 | 1 | 1 | 3 |
| Atukunda et al. ( | 2 | 1 | 1 | 4 |
| Nigusse and Gebretsadik ( | 1 | 1 | 1 | 3 |
| Williams et al. ( | 1 | 1 | 1 | 3 |
| Abou-Rizk et al. ( | 1 | 1 | 1 | 3 |
| Benedict et al. ( | 1 | 1 | 1 | 3 |
| Chee et al. ( | 1 | 1 | 1 | 3 |
| Soofi et al. ( | 2 | 1 | 1 | 4 |
| Dewey et al. ( | 2 | 1 | 1 | 4 |
| Sangalang et al. ( | 2 | 1 | 1 | 4 |
| Chek et al. ( | 2 | 1 | 1 | 4 |
| Cazes et al. ( | 2 | 1 | 1 | 4 |
| Daures et al. ( | 2 | 1 | 1 | 4 |
| Tamara et al. ( | 2 | 2 | 1 | 5 |
| Vilander et al. ( | 2 | 1 | 1 | 4 |
| Liu et al. ( | 2 | 1 | 1 | 4 |
| Kohl et al. ( | 2 | 1 | 1 | 4 |
| Taneja et al. ( | 2 | 1 | 1 | 4 |
| Wang et al. ( | 2 | 2 | 1 | 5 |
| Rashid et al. ( | 2 | 1 | 1 | 4 |
| Datoo et al. ( | 2 | 2 | 1 | 5 |
| Smith et al. ( | 2 | 1 | 1 | 4 |
| Alam et al. ( | 2 | 2 | 1 | 5 |
| Saluja et al. ( | 2 | 1 | 1 | 4 |
| Wangeci ( | 1 | 1 | 1 | 3 |
| Goyal et al. ( | 2 | 1 | 1 | 4 |
| O’Callaghan et al. ( | 2 | 1 | 1 | 4 |
| Cashman et al. ( | 2 | 1 | 1 | 4 |
| Yadav et al. ( | 2 | 2 | 1 | 5 |
| Okyere et al. ( | 1 | 1 | 1 | 3 |
| Kambale et al. ( | 2 | 1 | 1 | 4 |
| Lambrecht et al. ( | 2 | 1 | 1 | 4 |
| Grijalva-Eternod et al. ( | 2 | 1 | 1 | 4 |
| Hojati et al. ( | 2 | 1 | 1 | 4 |
| Tickell et al. ( | 2 | 1 | 1 | 4 |
| Cazes et al. ( | 2 | 1 | 1 | 4 |
| Batool et al. ( | 2 | 2 | 1 | 5 |
| Bhargava et al. ( | 2 | 1 | 1 | 4 |
| Argaw et al. ( | 2 | 1 | 1 | 4 |
| Nuzhat et al. ( | 2 | 2 | 1 | 5 |
| Gebretsadik et al. ( | 1 | 1 | 1 | 3 |
| Dabas et al. ( | 2 | 1 | 1 | 4 |
| Wu et al. ( | 2 | 1 | 1 | 4 |
| Gora et al. ( | 2 | 1 | 1 | 4 |
| Roberson et al. ( | 2 | 1 | 1 | 4 |
| Wiafe et al. ( | 2 | 1 | 1 | 4 |
| Jeremias et al. ( | 1 | 1 | 1 | 3 |
| Andriani et al. ( | 1 | 1 | 1 | 3 |
| Sié et al. ( | 2 | 1 | 1 | 4 |
| Ricci et al. ( | 2 | 1 | 1 | 4 |
| Lautatzis et al. ( | 2 | 1 | 1 | 4 |
| Mondal et al. ( | 2 | 1 | 1 | 4 |
| Reyes et al. ( | 2 | 1 | 1 | 4 |
| Ganmaa et al. ( | 2 | 2 | 1 | 5 |
| Khalil et al. ( | 2 | 1 | 1 | 4 |
| Bashiri et al. ( | 2 | 2 | 1 | 5 |
| Raju et al. ( | 2 | 2 | 1 | 5 |
| Kirolos et al. ( | 1 | 1 | 1 | 3 |
| Rahman et al. ( | 2 | 1 | 1 | 4 |
| Ow et al. ( | 2 | 1 | 1 | 4 |
| Khadilkar et al. ( | 2 | 1 | 1 | 4 |
| George et al. ( | 2 | 1 | 1 | 4 |
| Sharma et al. ( | 2 | 1 | 1 | 4 |
| Matheny et al. ( | 2 | 1 | 1 | 4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Iron Metabolism and Disorders · Vitamin D Research Studies
Introduction
1
The ongoing battle against childhood malnutrition constitutes a major public health crisis which will persist throughout the 21st century because it disrupts the natural process of growth and development and threatens the lives of millions of children across the globe. The world continues to experience malnutrition problems which show various complex patterns that include both undernutrition and micronutrient deficiencies as well as hidden metabolic disorders which create severe health problems for people and their communities. The two nutritional rickets and anemia demonstrate high occurrence rates because they stem from multiple sources which together create permanent damage to both physical and cognitive abilities of those who develop these conditions. This systematic review and meta-analysis seeks to quantify the global burden of these conditions, explore their determinants, and evaluate the implications for public health policies and intervention strategies (1–4).
Malnutrition occurs during early life when people fail to consume or absorb the necessary macronutrients and micronutrients needed for their growth and bodily functions. The World Health Organization (WHO) states that undernutrition causes approximately 45% of fatalities which occur in children younger than five years in low-and middle-income countries (LMICs) that experience food shortages and financial hardship and have restricted medical services. The 2020 Global Nutrition Report estimated that more than 149 million children under five years of age experience stunting while 45 million children experience wasting which represents the two types of malnutrition. The conditions make people more vulnerable to infectious diseases because they harm their immune systems and reduce their ability to think which creates a cycle of poor health together with economic hardship (5–9).
The nutritional rickets condition represents a reversible yet uncommon disorder which leads to impaired bone mineralization in children who suffer from malnutrition. Rickets now affects patients who experience vitamin D deficiency and who do not consume enough calcium through their diet and who experience various health effects from their sun exposure and their dietary patterns and their genetic traits and their cultural backgrounds. The condition manifests through multiple clinical symptoms which include bone pain and deformities and delayed growth and higher susceptibility to fractures. The renewed occurrence of rickets across various geographical areas demonstrates that both developing nations and high-income countries with their vulnerable groups need better preventive methods which include vitamin D supplementation and food fortification and public health educational initiatives. The existing clinical surveillance data shows regional prevalence information but researchers have not established complete worldwide rickets prevalence data which includes its causes thus making it difficult to create effective policies (10–13).
Anemia exists as a medical condition that causes decreased blood hemoglobin levels and leads to problems with oxygen distribution throughout the body which develops together with malnutrition and rickets. Anemia during childhood affects approximately 39% of children between the ages of 6 to 59 months who live in various parts of the world with sub-Saharan Africa and South Asia showing the highest prevalence rates. The origins of anemia result from multiple factors which include iron deficiency as the primary cause and vitamin A folate vitamin B12 deficiencies and chronic infections and inflammation and inherited hemoglobin disorders. Anemia during early childhood leads to three major consequences which include decreased energy levels and restricted ability to think and move and higher chances of death. The combination of anemia and other forms of malnutrition which includes stunting and micronutrient deficiencies creates greater risks for development while making it harder to treat patients and organize public health initiatives (14–22).
The research findings show that these medical conditions cause substantial health problems which lead to children’s death rates in various locations but show different rates which develop various health problems for different groups of people. The epidemiological situation shows complicated patterns which arise from diverse dietary habits and cultural traditions that dictate sun exposure and different income levels and available medical services. The treatment of rickets and anemia requires combined research because the two conditions together with all other types of malnutrition need complete examination for development of successful treatment methods. New research from controlled trials and observational studies shows that various dietary programs which contain both micronutrient supplements and additional food options and cash-based conditions can help decrease the likelihood and intensity of malnutrition along with its related health effects. The methods cannot be effectively applied to different communities until scientists establish strong meta-analytic proof of their effectiveness (23–32).
This systematic review and meta-analysis therefore aims to bridge the evidence gap by providing updated global estimates of the prevalence of childhood malnutrition, rickets, and anemia; identifying key determinants and contextual factors; and evaluating the implications for public health policy and implementation. The study collects different population data and various research methods to create guidelines which help policymakers and clinicians and program planners decide which prevention methods and early detection techniques and integrated management systems to implement. The global burden of interrelated conditions requires understanding their distribution because this knowledge supports the development of interventions which help children reach their maximum growth potential while achieving better health outcomes throughout their lives.
Methodology
2
Study design and reporting standards
2.1
The researchers conducted this systematic review and meta-analysis to assess three factors which are the worldwide occurrences and the causes and the effects of childhood malnutrition and rickets and anemia on public health. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure methodological transparency, reproducibility, and comprehensive reporting. This is a primary meta-analysis of individual research studies.
Search strategy
2.2
The researcher conducted a comprehensive literature search across all major electronic databases which included PubMed, Web of Science, Embase, Cochrane Library, and Google Scholar to access all published materials from the inception of the databases to their most current content. The research team performed a manual search of reference lists found in relevant articles and earlier published reviews to guarantee that they completed a comprehensive search. The search strategy combined controlled vocabulary such as Medical Subject Headings (MeSH) with free-text keywords using Boolean operators (AND, OR). The key terms which researchers used for their study included “childhood malnutrition” and “undernutrition” and “nutritional rickets” and “vitamin D deficiency” and “calcium deficiency” and “anemia” and “iron deficiency” and “micronutrient deficiency” and “prevalence” and “risk factors” and “children.” The researchers established no geographic boundaries because they wanted to collect evidence from every part of the world (Table 1).
Eligibility criteria
2.3
The researcher employed predefined rules which included specific requirements and particular exclusions to select their studies according to the Population-Intervention/Exposure-Comparison-Outcomes-Study Design (PICOS) framework. The research qualified studies which examined nutritional problems through malnutrition and rickets and anemia studies with Child and Adolescent participants from birth until age 18. The research included observational studies which used cross-sectional and cohort and case–control methodologies to evaluate disease patterns while using randomized controlled trials to track nutritional treatment results. The research accepted only peer-reviewed studies which provided enough numerical information for researchers to extract. The research excluded all forms of case reports and editorials and conference abstracts and narrative reviews and adult-only studies and articles without essential outcome data. The research eliminated all non-English documents.
Study selection process
2.4
We imported all retrieved records into reference management software and used the software to eliminate duplicate records before they started their screening process. The reviewer evaluated titles and abstracts to identify potentially relevant studies. The author evaluated full-text articles to check their compliance with pre-established eligibility standards. The reviewer handled their conflicts through discussion while they needed outside help from a third reviewer to achieve agreement. The study selection process used a PRISMA flow diagram which provided complete documentation of the entire procedure for better visibility. For studies reporting multiple relevant outcomes, we prioritized clinically primary outcomes first, followed by secondary outcomes, to avoid duplication.
Data extraction
2.5
The researchers created a standardized data extraction form which enables them to collect essential information from each research study in a uniform manner. The researchers gathered data which included the first author name, publication year, study country, research design, participant count, participant characteristics, diagnostic criteria for malnutrition, rickets, and anemia, disease prevalence data, related risk factors, details about the interventions that were used, and major outcome measurements. The reviewer conducted independent data extraction which they followed by cross-checking to achieve greater precision in results. Effect measures were harmonized: odds ratios (ORs) were converted to hazard ratios (HRs) where appropriate; continuous outcomes were standardized to common units. Missing data were handled by exclusion when non-recoverable, and where feasible, imputation methods were applied.
Quality assessment and risk of bias
2.6
The researchers used validated tools for evaluating and grading the methodological quality of the studies they included. The Jadad scale assesses randomized controlled trials by measuring their randomization methods and blinding techniques and withdrawal reporting methods. The Newcastle–Ottawa Scale (NOS) provides established risk-of-bias assessment frameworks for observational studies which evaluate selection methods and group comparability and outcome assessment. The Grading of Recommendations Assessment Development and Evaluation (GRADE) method assesses evidence certainty for primary outcomes through four evidence levels which depend on study limitations and result consistency and measurement accuracy and study directness likelihood.
Statistical analysis
2.7
The researchers used dedicated statistical software to conduct quantitative synthesis, which generated combined effect sizes and prevalence rates together with their 95% confidence interval results. The researchers implemented a random-effects model because they expected the studies to exhibit both clinical and methodological differences. The researchers used Cochran’s Q test to assess statistical heterogeneity which they measured through I^2^ statistic values that showed low heterogeneity at 25% moderate heterogeneity at 50% and high heterogeneity at 75%. The researchers conducted subgroup and sensitivity analyses to investigate the effects of different geographic regions study designs age groups and nutritional deficiency types when they found major heterogeneity in their results. The researcher evaluated publication bias by analyzing funnel plots visually and Egger’s test.
Ethical considerations
2.8
The review required no ethical approval because it used data from studies that had already been published. The researchers conducted their study according to established ethical guidelines for secondary data analysis which involved them maintaining accurate reporting and proper citation practices while interpreting their findings.
Results
3
Study selection
3.1
The selection process of studies was based on a strict multi-level screening method, which could guarantee the incorporation of really good evidence that is directly related to childhood malnutrition, nutritional rickets, and anemia. At first, a very extensive search for literature over PubMed, Web of Science, Embase, Cochrane Library, and Google Scholar produced 2,457 articles. After the duplicates were taken out (n = 1,134), 1,323 titles and abstracts were screened by reviewer. At this point, the 822 disqualified studies were those not related to childhood nutrition outcomes, those with non-human subjects, or those that were review articles, editorials, or case reports. At last, 96 studies were found to have fulfilled all the eligibility criteria and were thus considered for the systematic review and meta-analysis. The selection process is graphically represented in a PRISMA flow diagram (Figure 1).
PRISMA flow chart of study selection.
Characteristics of the included studies
3.2
The studies under review, numbering 96, form a very large base of evidence regarding issues of the ground and interventions with the global nutrient deficiency problem. Rickets risk factors were identified in early observational studies like, El Kholy et al. (33), and Graff et al. (34) that pointed to vitamin D and calcium deficiencies, low sunlight exposure, and genetic factors predisposition as the main reasons for rickets in children. Besides, intervention studies, e.g., Thacher et al. (35) and Aggarwal et al. (36) proved that. Supplements of calcium and vitamin D benefitted considerably in terms of biochemical and radiological outcomes. The maternal and child major trials, like Naik et al. (37), Trivedi et al. (38), and Soofi et al. (5) showed that mothers and babies’ nutrition, active coupling of nutrition packages and lipid-based nutrient interventions for babies led to the reduction of stunting, wasting, and micronutrient deficiencies. Community, school, and household-level programs made it possible to further improve growth, hygiene, and dietary practices. Observational studies among displaced or high-risk populations were also indicating the infections, food insecurity, and socio-environmental factors as the main reasons for the situation. The totality of these studies clearly depicts the necessity of targeted supplementation, dietary interventions, and context-specific programs to combat rickets and enhance child nutrition worldwide (Table 2).
GRADE assessment
3.3
GRADE Assessment across the 96 studies indicates that quality of evidence overall is low to moderate. This is due to differences in research methods, accuracy of measurements, and indirectness of conclusions among the studies. A lot of the older studies, especially in the area of childhood nutritional rickets and micronutrients, were given a low score due to a major problem with indirectness and imprecision. At the same time, they had a moderate risk of bias. The more recent randomized trials in maternal and early childhood nutrition interventions were rated as moderate quality because of their low risk of bias, consistent findings, and relatively precise estimates. In general, inconsistency was not a major issue across the studies. Some observational and cross-sectional studies were rated lower because of indirectness or serious imprecision which still affects the confidence in their effect estimates. Overall, the GRADE assessment affirms that the major part of the evidence is reliable for nutrition interventions, but it also points out that one should be very careful in interpreting results from older or smaller studies with methodologically limitations (Table 3).
Jada scale table
3.4
The evaluation of the highly recommended Jadad scale on the randomized controlled trials used in this review is done through 96 studies. Most of the studies fall under the score range of 4 to 5, which means they had good randomization, proper blinding, and clear reporting of withdrawals and dropouts. In particular, 30–35 studies got the highest score of 5, and thus were regarded as having well-designed, non-biased and high-quality studies. The majority of studies had a score of 4 indicating proper randomization and blinding but with minor limitations, while 20–25 studies scored 3, often because of unclear or partial randomization, single blinding, or limited reporting on dropouts. It can be concluded from this that the evidence coming from the studies on childhood nutrition, micronutrient supplementation, maternal supplementation, and malnutrition prevention is largely trustworthy, as most of the trials have adhered to the standard practices for trial design. Nevertheless, the case of the 3 scored studies indicates the necessity of a cautious interpretation, especially where the blinding or allocation methods were not very strictly followed (Table 4).
A modified Cochrane risk of bias 2 (RoB 2) tool was used. The domains were adjusted to align with RoB 2 terminology (e.g., Randomization Process rather than Random Sequence Generation). The risk of bias evaluation conducted on the 96 studies showed a wide range of methodological quality, which was mainly due to differences in study design and reporting standards. The majority of the studies had rated their random sequence generation and allocation concealment as low risk, which means that most of the trials conducted had adequate randomization. Nevertheless, the participant, personnel, and outcome assessor blinding was often not clear or not conducted at all, particularly in observational studies and open-label trials, which could give rise to performance or detection bias. The occurrence of incomplete outcome data and selective reporting was generally low, indicating that the data handling and reporting practices were robust, but some studies had unclear selective reporting. A large number of studies, however, were marked for other biases, which included funding sources, protocol deviations, or context-specific limitations, thus highlighting the need to be very careful in the interpretation of results. On the whole, randomized controlled trials were more rigorous in the methodological aspect, but observational and cross-sectional studies often had the issue of higher uncertainty, which calls for the consideration of study design in the evaluation of evidence on childhood and maternal nutrition interventions (Figures 2A–C).
(A) Risk of bias assessment of the studies. D1 = random sequence generation, D2 = allocation concealment, D3 = blinding of participants and personnel, D4 = blinding of outcome assessment, D5 = incomplete outcome data, D6 = selective reporting, D7 = other bias, D8 = overall risk of bias. (B) Risk of bias assessment table of the studies. D1 = Random sequence generation, D2 = allocation concealment, D3 = blinding of participants and personnel, D4 = blinding of outcome assessment, D5 = incomplete outcome data, D6 = selective reporting, D7 = other bias, D8 = overall risk of bias. (C) Risk of bias (RoB) assessment graph of the studies. D1 = random sequence generation, D2 = allocation concealment, D3 = blinding of participants and personnel, D4 = blinding of outcome assessment, D5 = incomplete outcome data, D6 = selective reporting, D7 = other bias, D8 = overall risk of bias.
Group analysis
3.5
Group 1: childhood nutritional rickets and vitamin D/calcium status
3.5.1
The analysis included thirty studies comprising different types like observational studies, case–control studies, RCTs, and IPD meta-analyses all from different populations spread across the Middle East, Africa, South and Southeast Asia, and high-latitude regions. Observational studies always indicated a very high danger of rickets when the conditions of low calcium intake, limited sunlight exposure, and vitamin D deficiency were present, with odds ratios being in the range of 3.6 to 7.1. RCTs and studies involving supplementation reported slight but still significant improvements in vitamin D status, bone health, and growth parameters (HRs 0.75–0.87, 95% CI 0.58–1.08), with maternal supplementation during lactation effectively preventing deficiency in infants. Meta-analyses (Cashman et al., 2022; Wu et al., 2023) confirmed the protective effects in high-risk populations. The overall pooled hazard ratio (HR) was 1.51, 95% CI 1.26–1.82, p < 0.05, with significant heterogeneity (I^2^ = 88%, p < 0.01), thereby showing the variability in intervention effects. All these findings point out the very vital role of calcium and vitamin D in the prevention of childhood rickets all over the world (Figure 3).
Forest plot of the studies about childhood nutritional rickets and vitamin D/calcium status.
Group 2: childhood malnutrition prevention and nutritional interventions
3.5.2
Malnutrition in children is still a big problem all over the world but at the same time, nutritional interventions that focus on specific groups have proven to be very effective in terms of child growth and health among other benefits. Out of the 30 studies from different regions, Africa, South Asia, and Southeast Asia for example, the nutritional interventions that were used included the following: supplements of micronutrients, lipid-based nutrient supplements (LNS), probiotics, fortified foods as well as cash transfers, dietary counseling, pregnancy and lactation maternal supplements, and many others. Integrated approaches, which combined nutritional, health, and hygiene aspects, together with behavior-change strategies, turned out to be especially effective. The evidence from the studies conducted through randomization for short and long periods, cluster randomized controlled trials (RCTs), and meta-analyses pointed to the same conclusion—they reported an improved situation in terms of risk of malnutrition, growth improvement, and better maternal and infant nutritional status. The implementation of these interventions was during certain critical windows for example, the first 1,000 days of life that stressed the importance of early prevention. The pooled analysis provided a hazard rate (HR) of 0.8 (95% CI, 0.77–0.84) with the same impact across the studies, thereby confirming the strong and consistent effect of nutritional strategies in childhood malnutrition prevention (Figure 4).
Forest plot of the studies about childhood malnutrition prevention and nutritional interventions.
Group 3: childhood micronutrient deficiencies and supplementation
3.5.3
Micronutrient deficiencies, especially iron, vitamin A and iodine, are widespread in children worldwide and severely affect the physical growth, immunity, and brain development. This group did a review of 15 papers that looked at various aspects of child health and supplementation: the distribution, risk factors, and effects of vitamins on children’s health. Iron supplementation (low-dose ferrous sulfate, iron polysaccharide), vitamin A supplementation, iodised salt, and lipid-based nutrient supplements were among the interventions. The observational and cross-sectional studies pointed out the existence of deficiencies in different populations, such as refugee camps, rural communities, and preschool children in Africa, Europe, and Asia. The supplementation trials brought about improved micronutrient status, anemia reduction, and better growth outcomes. Meta-analysis with a random-effects model showed a summarized hazard rate (HR) of 0.91 (95% CI, 0.86–0.96), which supports the claim that micronutrient interventions have protective effects on health factors through a statistically significant reduction of the risk. The low heterogeneity found across studies means that there were consistent benefits of supplementation irrespective of the type of setting or the strategy used, which underscores the need for making routine micronutrient programs part of childhood nutrition (Figure 5).
Forest plot of the studies about Childhood Micronutrient Deficiencies and Supplementation.
Group 4: maternal and early childhood nutrition interventions
3.5.4
The interventions in maternal and early infancy nutrition are the ones that have the biggest impact on child growth, health, and overall development. Group four looked into 18 research papers that placed emphasis on maternal supplementation, early childhood nutrition, and integrated health programs. Among the interventions were vitamin D or multiple-micronutrient supplementation for pregnant and lactating mothers, fortified diets with extra calories and proteins, and supplementation for infants post-delivery. Furthermore, combined health, nutrition, psychosocial, and WASH (Water, Sanitation, and Hygiene) programs, cash transfers with conditions and without any, and behavior-change interventions were installed to assist child health in low-income areas. The evaluations of the effects were included in the range of micronutrient level and growth to infection prevention and early cognitive development. A pooled analysis employing a random-effects model provided a summarized hazard rate (HR) of 0.85 (95% CI: 0.78–0.93), thus signifying a statistically significant protective effect. The I^2^ of 53% pointing to moderate heterogeneity, indicates that the majority of the interventions were beneficial but varied in terms of effect size depending on the population and intervention type, thereby marking the importance of using context-specific strategies to achieve the best results in maternal and child health (Figure 6).
Forest plot of the studies about maternal and early childhood nutrition interventions.
Group 5: long-term observational and cohort studies on child health and nutrition
3.5.5
The long-term observational and cohort studies give one of the main sources of understanding the factors and the changes of child health and nutrition over time. This category of studies comprised 11 reports on the evaluation of the nutritional state, growth, anemia, and other related health conditions in children and adolescents at different places, such as refugee groups, low-resource areas, and pre-adolescent populations in Asia and Africa. The researchers used different methodologies from beginning-to-end cohorts and repeated cross-sectional surveys to mixed-methods research, enabling them to reveal both short- and long-term nutritional patterns. The major results pointed out the continuous presence of malnutrition and anemia plus the influence of nutrition deficits during the earliest stages on later health outcomes like growth and micronutrient status. Nevertheless, the pooled analysis performed using a random-effects model showed a summarized hazard ratio (HR) of 0.96 (95% CI: 0.9–1.01), thus revealing no statistically significant overall effect. The effect sizes were quite similar in all the studies, indicating the same kind of associations and the strength of observational data for monitoring the trends in child nutrition over time (Figure 7).
Forest plot of the studies about long-term observational and cohort studies on child health and nutrition.
Publication bias
3.6
The bias in publication across the five groups was evaluated by means of funnel plot and Egger’s tests. Group 1 (intercept = 5.69, 95% CI: 5.29–6.09, t = 27.994, p < 0.001), Group 2 (intercept = −3.61, 95% CI: −5.01 to-2.2, t = −5.039, p < 0.001), Group 3 (intercept = −9.82, 95% CI: −12.93 to-6.7, t = −6.179, p < 0.001), and Group 4 (intercept = 4.09, 95% CI: 2.22–5.95, t = 4.296, p = 0.001). It indicates that in these groups the smaller studies having non-significant results might get less representation. However, Group 5 did not exhibit significant publication bias as the funnel plots were symmetrical and Egger’s test showed no significant asymmetry (intercept = −5.15, 95% CI: −9.72 to-0.59, t = −2.211, p = 0.054), implying that the reporting was more consistent across studies (Figure 8).
Funnel plot of the included studies.
Discussion
4
Summary of main findings
4.1
In total, 96 studies describing various designs [observational studies, case–control studies, randomized controlled trials (RCTs), cluster RCTs, and meta-analyses with individual participant data (IPD)] were included in this systematic review and meta-analysis. The studies were done on different populations, mainly in the Middle East, Africa, South and Southeast Asia, high-latitude areas, and refugee settings. Group 1 showed results of high risk of rickets associated along with magnesium deficiency ranging firmness of calcareous in taking, limited exposure to sunlight, and very low levels of vitamin D with odds ratio of 3.6 to 7.1 [e.g., OR 6.7, 95% CI 2.9–15.3; Aggarwal et al. (39): OR 7.1, 95% CI 3.0–16.7]. Randomized controlled trials (RCTs) and supplementation trials showed improvements in vitamin D status as well as bone health and growth reflected by HRs 0.75–0.87, 95% CI 0.58–1.08, with the maternal supplementation during lactation being effective in preventing the deficiency in infant (37, 38). IPD meta-analyses confirmed that there was a barrier to the deficiency (80, 89). The pooled hazard ratio (HR) across this group was 1.51 (95% CI 1.26–1.82, p < 0.05), while the heterogeneity was significant (I^2^ = 88%, p < 0.01) reflecting the diversity of study populations and the effects of the interventions. The quality of the research was found to be moderate to high (Jadad 3 to 5) and GRADE evidence was at low to moderate levels.
Group 2 emphasized the success of focused nutritional methods, such as micronutrient supplementation, lipid-based nutrient supplements (LNS), probiotics, fortified foods, dietary counseling, maternal supplementation, and cash transfers (conditional/unconditional). The use of integrated interventions that combined nutrition, health, hygiene, and behavior change components was particularly effective in child growth, nutrition, and reduction of malnutrition risk when such interventions were carried out during the first 1,000 days of life. Pooled analysis gave a summarized HR of 0.80 (95% CI 0.77–0.84), with low heterogeneity, which is an indicator of consistent effects across different settings.
Group 3 dealt with preschool and school-aged children suffering from deficiency in iron, vitamin A, and iodine, including those living in refugee camps, rural communities, and low-resource areas. Observational studies revealed that these deficiencies were widespread and were among the major causes of anemia, stunting, and impaired cognitive development. However, supplementation interventions consisting of low-dose ferrous sulfate, iron polysaccharide, vitamin A, iodized salt, and LNS led to a significant improvement in micronutrient status, a reduction in the prevalence of anemia, and better growth outcomes. The pooled HR was 0.91 (95% CI 0.86–0.96), with low heterogeneity, thus the protective effects were considered consistent across settings.
Group 4 considered a wide range of interventions such as maternal supplementation (vitamin D, multiple micronutrients), fortified energy-protein diets, postnatal infant supplementation, and integrated health programs with WASH, psychosocial support, and cash transfers. The mother’s and children’s micronutrient status, their growth, prevention of infections and early cognitive development got better as a result of these interventions. The overall analysis resulted in an average HR of 0.85 (95% CI 0.78–0.93) with moderate heterogeneity (I^2^ = 53%), thus the protective effects were considerable but distinctly different between the various populations and interventions.
Group 5 encompassed prospective cohorts, repeated cross-sectional surveys, and mixed-method assessments where child growth, anemia, and nutritional trajectories were followed over a long period in different settings, including refugees and low-resources areas. The studies pointed out that malnutrition is still a persistent problem and that early-life nutritional deficits have long-term impacts on growth and micronutrient status. The pooled analysis revealed a summarized HR of 0.96 (95% CI 0.90–1.01), which meant that there was no statistically significant overall effect, but the studies’ consistency reflected the robustness of long-term observational data. The studies show high heterogeneity because researchers used different study designs, intervention methods and study durations and baseline nutritional conditions and socioeconomic backgrounds.
The systematic review and meta-analysis establishes global research findings from 96 studies which explain the complete details about childhood malnutrition and rickets and anemia through their causes and methods of prevention. The findings show that childhood undernutrition remains a critical public health issue which specifically affects low and middle income countries because these countries face structural inequalities and food shortages and they have restricted healthcare services and environmental hazards. The review demonstrates how various data sources from observational studies and randomized controlled trials and meta-analyses show that deficiencies in macronutrients and micronutrients lead to long-term development problems in growth and skeletal health and immunity and neurodevelopment.
The evidence related to nutritional rickets confirms that calcium and vitamin D deficiencies remain the primary cause of rickets in all parts of the world. The observational studies established that infants and young children developed higher susceptibility to the disease because of their insufficient dietary consumption and decreased sunlight contact and their cultural practices and their mothers’ nutritional deficiencies. The current research results confirm earlier international studies which found that rickets has become more common because of changes in modern living and urban development and indoor home environments. Previous research has emphasized that exclusive breastfeeding without adequate vitamin D supplementation may elevate deficiency risk, a pattern similarly observed across several studies included in this analysis. The intervention trials show that both child and maternal supplementation methods successfully enhance vitamin D levels and bone health in children, which supports existing pediatric nutrition guidelines that recommend routine vitamin D supplements for people at high risk of deficiency.
The review results show that integrated intervention programs to prevent childhood malnutrition demonstrate better growth results than all other tested methods. The program that combined micronutrient supplementation with lipid-based nutrient supplements and dietary counseling and maternal support showed its highest effectiveness during the first 1,000 days of life which scientists recognize as the essential period to avoid permanent physical and mental impairments. The results provide strong evidence that UNICEF-supported initiatives together with previous large-scale trials demonstrate that nutrition-sensitive methods which include food fortification and social protection systems that use cash transfers can effectively decrease stunting and wasting. Multi-sectoral programs which focus on sanitation and infection control together with caregiver education provide more lasting advantages than single-component interventions which show that social factors beyond food access play a role in childhood malnutrition.
Children around the world still experience micronutrient deficiencies which particularly include iron deficiency anemia. The supplementation trials which researchers examined showed that hemoglobin levels and immune function and developmental outcomes all improved through the tested interventions which earlier meta-analyses identified as one of the most cost-effective public health interventions for iron supplementation. The vitamin A and iodine programs showed improved growth results which reduced illness rates in accordance with World Health Organization (WHO) guidelines that have existed for a long time. The common results which researchers found in different locations show that routine micronutrient programs need to continue because they protect vulnerable groups who include refugees and children from rural areas without resources.
Maternal and early childhood nutrition interventions show that malnutrition affects multiple generations of people. Evidence shows that better maternal nutrition during pregnancy and lactation leads to improved birth results and enhanced infant nutrient levels and better initial growth development. The results of this study support the developmental origins of health and disease (DOHaD) framework which states that early life experiences determine the risk of developing health problems in later life. Previous cohort studies have shown that maternal deficiencies lead to increased risk of low birth weight and skeletal development problems and subsequent anemia. The current review expands existing knowledge by demonstrating that maternal-child health programs which combine nutrition education with psychosocial support and water sanitation and hygiene (WASH) programs deliver better child health results both in the short term and long term.
The review contains long-term observational studies and cohort studies which show how nutritional deficiencies continue to affect individuals after their early childhood period. Children who experienced severe malnutrition during their early years faced ongoing difficulties with their growth patterns and development of anemia and micronutrient deficiencies throughout their subsequent growth periods. The findings of this study support earlier longitudinal studies which demonstrated that early nutritional deprivation leads to educational and metabolic and productivity impairments that endure throughout life. The observation results from different datasets show that child nutrition patterns have become more consistently tracked because of better global system monitoring and public health reporting, which leads to greater awareness about child nutrition patterns.
The study results show positive outcomes, but researchers need to examine specific methodological aspects. The evidence of publication bias which exists in multiple intervention-focused groups shows that smaller studies with null findings may be underrepresented according to previous research, which the previous nutrition meta-analyses confirmed. The study results display different research results because of variations in participant nutritional conditions and local feeding customs and medical facilities and study methods. The observed differences demonstrate that local communities need to develop their unique nutrition plans instead of following standardized models which exist throughout the world.
The evidence quality assessment showed evidence quality at three different levels because some observational studies had indirect evidence and their results were not precise enough. The low bias risk found in recent random control trials increases trust in the efficacy of both supplementation treatments and integrated intervention programs. Modern studies show better research methods than previous decades because current trials achieve higher standards which support evidence-based nutrition policies.
Public health experts need to establish multiple prevention programs which combine various approaches to stop childhood malnutrition and rickets and anemia. Organizations should implement nutrition-specific solutions together with their existing programs for poverty reduction and maternal education and food system resilience and equal healthcare distribution. The detection and prevention processes will receive better support through school-based supplementation and antenatal nutrition programs and community health worker programs.
Strengths
4.2
- The research study provides an extensive compilation of 96 studies which examine multiple geographic locations and different income levels from low-income to middle-income and high-income countries.
- The research study combines different study methods which include randomized controlled trials and observational studies and cohort analyses and meta-analyses.
- The research study includes multiple types of interventions which include micronutrient supplementation and maternal and child nutrition programs and integrated health and hygiene and behavior-change strategies.
- The researchers used standardized quality assessment tools together with risk-of-bias evaluation methods and publication bias analysis techniques to establish their methodological framework.
- The research team used subgroup analysis methods to study nutritional deficiencies and the impact of interventions throughout different population groups and stages of human development.
Limitations
4.3
- The research shows that intervention-oriented groups face publication bias which leads to their underreporting of non-significant results.
- Two types of observational studies experienced two problems, which led to their evidence base becoming less reliable.
- The different diagnostic criteria used to identify malnutrition, rickets, and anemia created inconsistencies in measurement results.
- The requirement to use only published literature causes researchers to miss important gray literature and program-level information from low-resource environments.
- Non-English studies were excluded.
Future prospects
4.4
- Researchers should perform extensive longitudinal studies which require proper design to study the extended impacts of early-life nutritional deficiencies.
- Researchers should establish standardized outcome measurements together with diagnostic standards which will assist in better cross-study research comparisons.
- The research should concentrate on developing practical nutrition solutions which provide affordable nutritional programs that can be implemented in different local environments.
- Public health strategies should include nutrition programs which combine maternal education efforts with food system improvements and WASH programs.
- The study will investigate new methods which include precision nutrition and digital health monitoring and community-based delivery systems to achieve early detection and targeted supplementation and worldwide monitoring.
Conclusion
5
The compiled research from 96 studies through this systematic review and meta-analysis reveals the various causes of childhood malnutrition, rickets, and anemia in different global settings. Vitamin D and calcium deficiencies are still the main reasons for nutritional rickets while deficiencies in micronutrients such as iron, vitamin A, and iodine are responsible for eventually impaired growth, cognitive, and immune abilities. Nutritional interventions for mothers and infants, particularly when combined with health, hygiene, and behavior-change strategies during critical periods like the first 1,000 days, always show protective effects. Long-term follow-up studies continuously show nutrition deficiency and thus underlining the necessity of constant monitoring and context-specific interventions. In general, the findings of this research support the very high position of comprehensive and multi-level nutrition programs which are directed not only toward children but also mothers, in the process of eliminating childhood malnutrition, preventing rickets and anemia, and ensuring long-term growth, development, and health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dabas A Dabas V Dabla PK Marwaha RK Yadav S Bharadwaj M . Daily v. weekly oral vitamin D 3 therapy for nutritional rickets in Indian children: a randomised controlled open-label trial. Br J Nutr. (2023) 129:1473–80. doi: 10.1017/S 0007114522001477, 35550679 · doi ↗ · pubmed ↗
- 2Lautatzis M-E Keya FK Al Mahmud A Tariq U Lam C Morris SK . Maternal vitamin D supplementation and infantile rickets: secondary analysis of a randomized trial. Pediatrics. (2024) 153:e 2023063263. doi: 10.1542/peds.2023-063263, 38726565 · doi ↗ · pubmed ↗
- 3Bouillon R Le Boff MS Neale RE. Health effects of vitamin D supplementation: lessons learned from randomized controlled trials and Mendelian randomization studies. J Bone Miner Res. (2023) 38:1391–403. doi: 10.1002/jbmr.4888, 37483080 PMC 10592274 · doi ↗ · pubmed ↗
- 4Kiely M Brennan L Dunlop T Tate G Woodside JV Moretti D . Prevention of chronic disease using vitamins—a case study of the vitamin D and cardiovascular disease hypothesis using evidence from randomised controlled and prospective cohort studies. Eur J Nutr. (2025) 64:199. doi: 10.1007/s 00394-025-03706-w, 40448712 PMC 12126319 · doi ↗ · pubmed ↗
- 5Soofi SB Khan GN Ariff S Ihtesham Y Tanimoune M Rizvi A . Effectiveness of nutritional supplementation during the first 1000-days of life to reduce child undernutrition: a cluster randomized controlled trial in Pakistan. Lancet Regional Health. (2022) 4. doi: 10.1016/j.lansea.2022.100035, 37383995 PMC 10305932 · doi ↗ · pubmed ↗
- 6Kambale RM Ntagazibwa JN Kasengi JB Zigashane AB Francisca IN Mashukano BN . Probiotics for children with uncomplicated severe acute malnutrition (Pru SAM study): a randomized controlled trial in the Democratic Republic of Congo. Am J Clin Nutr. (2023) 117:976–84. doi: 10.1016/j.ajcnut.2023.01.01937137616 · doi ↗ · pubmed ↗
- 7Sangalang SO Lemence ALG Ottong ZJ Valencia JC Olaguera M Canja RJF . School water, sanitation, and hygiene (Wa SH) intervention to improve malnutrition, dehydration, health literacy, and handwashing: a cluster-randomised controlled trial in metro Manila, Philippines. BMC Public Health. (2022) 22:2034. doi: 10.1186/s 12889-022-14398-w, 36344973 PMC 9641834 · doi ↗ · pubmed ↗
- 8Chek LP Gan WY Chin YS Sulaiman N. A nutrition programme using positive deviance approach to reduce undernutrition among urban poor children under-five in Malaysia: a cluster randomised controlled trial protocol. P Lo S One. (2022) 17:e 0275357. doi: 10.1371/journal.pone.0275357, 36227928 PMC 9562161 · doi ↗ · pubmed ↗