Lessons from irritable bowel syndrome: potential for understanding and managing post-COVID
Andreas Stallmach, Peter Layer, Katrin Katzer, Philipp A. Reuken

TL;DR
This paper compares post-COVID symptoms to irritable bowel syndrome to better understand and manage long-term effects of the virus.
Contribution
It proposes using IBS as a model to explore post-COVID mechanisms and treatment challenges.
Findings
Post-COVID and IBS share similar diagnostic and therapeutic challenges.
Both conditions are functional disorders with multifactorial causes.
Lessons from IBS suggest limited near-term treatment options for post-COVID.
Abstract
Post-COVID presents a complex medical challenge characterized by persistent symptoms following SARS-CoV-2 infection. Similarities between post-COVID and post-infectious Irritable Bowel Syndrome (PI-IBS) suggest that the latter can serve as a useful model for understanding pathophysiological mechanisms and developing therapeutic approaches. Both conditions are functional disorders triggered by an acute infection, with multifactorial etiology and limited biomarker-based diagnostics. The variability of symptoms and the high frequency of comorbidities make these disorders particularly difficult to diagnose. Diagnostic efforts may be further hindered by the stigmatization of such disorders among healthcare providers, the health insurance industry, and the general public. This article explores the parallels between PI-IBS and post-COVID, highlighting, on the one hand, what can be learned from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
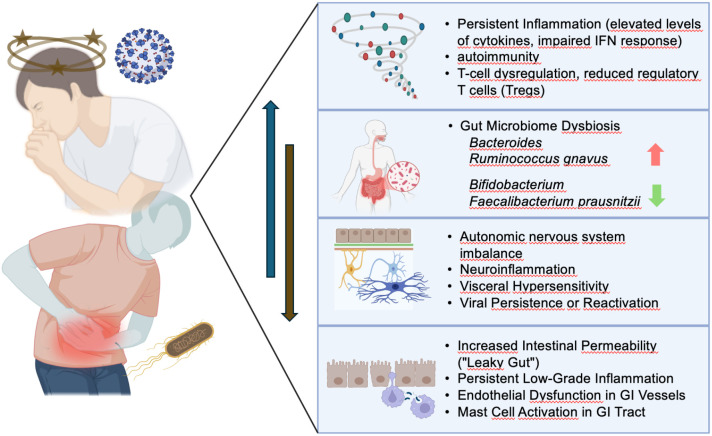 Figure 1
Figure 1| Diagnostic strategy | Background |
|---|---|
| Clinical evaluation | Thorough history and physical examination to assess symptoms, their duration, and any associated factors. Fulfillment of the Rome IV-criteria as well as absence of red flags should be ascertained in all patients presenting with symptoms compatible with IBS. |
| Stool tests | 1. Fecal calprotectin. 2. Occult blood testing (if malignant disease is deemed possible). 3. Microbiological testing (if gastrointestinal infection is deemed possible, especially in the diarrhea-predominent type). |
| Blood tests | Basic laboratory tests including inflammatory parameters (C-reactive protein (CRP) and white blood cell count (WBC)) as well as testing for celiac disease |
| Ileocolonoscopy/gastroscopy including biopsies | To rule out malignancy, inflammatory bowel disease (IBD), microscopic colitis, celiac disease or Whipple’s disease. |
| Breath tests | To rule out lactose or fructose malabsorption or small intestinal bacterial overgrowth (SIBO), if deemed possible. |
| Abdominal ultrasound | Should be performed in all patients to rule out other abdominal pathologies, e.g. tumors. |
| Imaging, e.g. CT or MRI | Should only be performed in specific cases, especially if red flags are present. |
| Psychological assessment | Evaluation of mental health conditions that may influence IBS symptoms, such as anxiety or depression. |
| Parameter | PI-IBS | PCS |
|---|---|---|
| Trigger | SARS-CoV-2 virus | |
| Time interval between infection and symptom onset | 6 months ( | 3 months ( |
| Long-term course | Spontaneous improvement in about 25-50% over several years ( | Reduction of severe cases from 31.3 to 19.4% within six months ( |
| Symptoms | Abdominal pain, bloating, altered bowel habits (diarrhea, constipation, or both) | Fatigue, dyspnea, cognitive dysfunction (“brain fog”), gastrointestinal complaints (e.g., nausea, diarrhea), and others |
| Mechanism | PCS | PI-IBS |
|---|---|---|
| Similarities | ||
| Low-grade mucosal inflammation | present ( | |
| Increased intestinal permeability (“leaky gut”) | Observed ( | |
| Elevated pro-inflammatory cytokines | IL-1β, IL-6, IL-8, TNF- α ( | |
| T-cell activation | present ( | |
| Mast cell involvement | Possibly role in pathophysiology ( | Established role in IBS pathophysiology ( |
| Differences | ||
| Systemic inflammation | More prominent — COVID can trigger widespread immune dysregulation and “cytokine storm” in acute phase ( | Mostly confined to the gut mucosa ( |
| Viral immune signature | Associated with type I interferon response and viral persistence ( | Often driven by bacterial toxins or pathogen-associated molecular patterns (PAMPs) ( |
| Immune exhaustion/dysregulation | Evidence of T-cell exhaustion and long-term immune dysfunction in some PCS cases ( | Less documented; immune activation is more localized and self-limited ( |
| Elevated cytokines | tachykinins, IFN- α 2, IL-10, IL-32 ( | IL-4, IL-5, IL-17, IL-22 ( |
| Parameter | PCS | PI-IBS |
|---|---|---|
| Similarities | ||
| Microbiota Signatures | loss of beneficial commensals and an overrepresentation of pro-inflammatory or pathogenic species | |
| Neuroimmune Pathways | Dysbiosis may contribute to symptomatology via interactions with the gut-brain axis | |
| Differences | ||
| Causality Strength | Emerging evidence for dysbiosis as a | Dysbiosis is |
| Systemic Manifestations | Multisystemic (neurological, cardiovascular, etc.) | Primarily gastrointestinal |
| Therapeutic Trials | Early-stage for microbiota-directed therapies | Ongoing, including probiotics, FMT, antibiotics |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · Gastrointestinal motility and disorders · Obsessive-Compulsive Spectrum Disorders
Introduction
After the first cases of acute SARS-CoV-2 infection, a substantial proportion of patients were found to experience long-lasting sequalae (1, 2). The World Health Organization (WHO) defines symptoms that persist for 12 weeks or longer following an acute SARS-CoV-2 infection, without any other plausible explanation, as post-COVID-19 syndrome (PCS) (3).
While the initial waves of SARS-CoV-2 infection led to PCS in approximately 6–10% of cases (4), subsequent increases in population immunity and the emergence of less pathogenic variants have significantly reduced the likelihood of long-term sequelae (5). Even though the incidence of PCS is decreasing, patients with long-term courses following infections during the first waves, as well as newly affected individuals, continue to present a challenge in medical care.
One major challenge in handling of PCS patients is the broad spectrum of symptoms. Until today, more than 200 different symptoms have been attributed as long-term sequelae of a SARS-CoV-2 infection (6) with fatigue being one of the most frequently reported symptoms (7). Additionally, anxiety, depression, cognitive problems and respiratory symptoms are often reported (8). In addition, an increased incidence of functional gastrointestinal disorders, including irritable bowel syndrome (IBS), functional diarrhea, functional constipation, and functional dyspepsia, was observed in COVID-19 patients compared to healthy controls at a six-month follow-up (9). Furthermore, a large-scale, multicenter, controlled study involving over 2,000 hospitalized patients demonstrated that individuals with SARS-CoV-2 infection exhibited significantly higher rates of IBS—characterized by abdominal pain and altered bowel habits—than non-COVID patients (3.2% vs. 0.5%, respectively) (10).
PCS and post-infectious IBS represent sequelae of infectious diseases in which the acute phase resolves before persistent symptoms emerge. Both conditions are characterized by ongoing immune activation with low-grade inflammation, alterations of the intestinal microbiome, and disturbances of the gut–brain axis and autonomic regulation. They can thus be conceptualized as post-infectious long-term syndromes arising from the interplay of immune dysregulation, microbial imbalance, and neurovegetative dysfunction. While post-COVID manifests as a systemic disorder, post-infectious irritable bowel syndrome is primarily confined to the gastrointestinal tract. Due to its clinical manifestations, IBS is considered also a potentially disabling condition. It is associated with substantial healthcare expenditures, reduced occupational productivity and school attendance, and a significantly impaired health-related quality of life among affected individuals (11, 12). Despite its high prevalence in contemporary gastroenterological practice, the pathophysiological mechanisms underlying IBS remain incompletely understood. Similar to PCS it is recognized as a complex, multifactorial disorder influenced by a variety of factors including age, sex, genetic predisposition, dietary habits, psychosocial stressors, alterations in the gut microbiota, subclinical inflammation, and visceral hypersensitivity (13–15). The risk factors for the development of PCS and IBS are therefore the same — another indication of their numerous similarities. Both conditions are reported more frequently in female patients, younger age and can be associated with severity of the initial infection and psychological preconditions (7, 16–18).
Another major challenge for both, patients and physicians, is the absence of objective markers in laboratory tests or imaging diagnostics. The German PCS-guidelines emphasize that no routinely available parameters can confirm or exclude PCS (19). Furthermore, the lack of a universally accepted, coherent pathophysiological concept complicates the development of causal therapeutic approaches.
It is widely accepted for both conditions that no single, definitive cause exists (16, 20), making a monotherapy-based approach unlikely to cure the condition. Understanding IBS, which has been known for many decades, with the various research and treatment approaches can also provide valuable insights into effective diagnostic and therapeutic strategies for PCS patients. IBS — particularly in its post-infectious form (PI-IBS) — serves as a well-studied model of a functional, chronic disorder that arises following an acute infectious event. This article explores the parallels between PI-IBS and PCS, highlighting how management strategies developed for PI-IBS can inform and enhance the care of patients with PCS.
Diagnostic challenges
Patient symptoms following COVID-19 and in individuals with PI-IBS often remain unexplained by objective findings in routine testing, highlighting the complexity and evolving nature of these conditions. Diagnostic strategies often depend on persistent symptom patterns and ruling out alternative causes, and should follow national and international guidelines or consensus recommendations (19, 21–24). Results are often normal in PCS or IBS patients; only through advanced methods of clinical research can morphological, immunological, or genetically based deviations from healthy individuals be detected. However, due to their low specificity, these findings are not suitable for use in routine clinical practice. Both conditions are marked by variable symptom expression. Recent studies suggest, that one such mechanism involves a reduction in tissue blood supply, which is associated with a proposed quantifiable index (25). This mechanism was evaluated by analyzing the incidence rates of Long COVID symptoms directly linked to this mechanism, and it was found to account for the majority (76%) of the reported symptoms (26). PI-IBS patients may present with abdominal pain, bloating, diarrhea, or constipation, in these patients Rome IV criteria guide diagnosis. PCS patients report fatigue, “brain fog”, chest pain, gastrointestinal symptoms, and more (7). This heterogeneity complicates diagnosis and management but underscores the need for personalized care (see also Table 1). It is important that if the diagnostic results are negative and there are no changes in symptoms or red flags (e.g. fever, anemia, weight loss, visible or occult blood in the stool), the test should not be repeated (“there must be something wrong, I feel so bad”). Attentive, empathetic care is important in this context. Healthcare professionals should communicate this uncertainty to patients, but at the same time also communicate that adequate diagnostics should rule out life-threatening diseases.
Pathophysiological parallels
Post-infectious onset
Both PCS and PI-IBS frequently follow acute infections. In IBS, the onset often occurs after microbial gastroenteritis, whereas PCS follows viral infection. Timeline and features of symptom development in both cases suggest shared mechanisms of post-infectious sequelae. PI-IBS is defined by a constellation of persistent gastrointestinal symptoms that develop subsequent to an episode of infectious enteritis, with other causes of symptoms having been excluded. Common clinical features include abdominal pain, altered bowel habits—such as diarrhea, constipation, or a combination of both—bloating, and increased visceral sensitivity. The severity and duration of symptoms can vary considerably, often leading to substantial impairment in daily functioning and quality of life. Considerable efforts were made to elucidate the pathophysiological mechanisms underlying PI-IBS. Current evidence suggests that the inciting gastrointestinal infection induces deficient intestinal barrier functions, aberrant immune responses and disturbances of the composition of the intestinal microbiota. This, in turn, may result in chronic low-grade inflammation, altered gut motor and secretory functions, and visceral hypersensitivity (see also Figure 1).
Pathogenetic similarities between PCS and PI-IBS. Systemic immunological imbalances are more pronounced in PCS (the blue arrow indicates their increasing relevance in PCS), whereas disturbances in the microbiota and gastrointestinal permeability (brown arrow) are likely of greater significance in PI-IBS.
These interconnected processes are thought to contribute to both the onset and persistence of PI-IBS symptoms. Epidemiological studies have investigated the incidence and prevalence of PI-IBS across diverse populations, underscoring its clinical relevance. Reported incidence rates following infectious enteritis range from 5% to 32%, depending on the characteristics of the study cohort and the duration of follow-up. PI-IBS is diagnosed when at least 6 months have passed since the initial infection and symptoms have been present for at least 3 months. In subsets of affected individuals, symptoms may improve over 6 to 24 months. However, in other patients, PI-IBS may persist for several years or even decades. Poor prognostic factors include: severe course of the initial infection, psychological stress, female sex, and pre-existing gastrointestinal conditions. As there is no causal therapy, treatment is symptom-oriented. A comparison between PI-IBS and PCS is provided in Table 2.
Immune dysregulation
Both PCS and classical post-infectious IBS (PI-IBS) are characterized by persistent immune activation following an acute infectious insult (32, 33). They share several immunopathological features, including low-grade mucosal inflammation, increased intestinal permeability, dysbiosis, and heightened immune cell activity. Elevated levels of pro-inflammatory cytokines such as IL-6, IL-8, TNF-α, and IL-1β have been documented in both conditions, contributing to chronic gastrointestinal symptoms and altered gut-brain axis signaling (34–36). In PI-IBS, the immune response is typically localized to the gastrointestinal tract and follows a clearly defined episode of bacterial or parasitic gastroenteritis. Histological studies have shown increased intraepithelial lymphocytes and mucosal mast cells, particularly in proximity to enteric neurons, suggesting a neuroimmune component underlying the characteristic visceral hypersensitivity. In contrast, PCS-IBS arises in the aftermath of SARS-CoV-2 infection and can occur even in patients who did not experience acute gastrointestinal symptoms. SARS-CoV-2 infects intestinal epithelial cells via ACE2 receptors, and viral RNA and proteins have been detected in the intestinal mucosa for weeks to months after the resolution of respiratory symptoms, indicating potential viral persistence and chronic immune stimulation (37). This has been associated with persistent elevation of systemic inflammatory markers and ongoing immune dysregulation, a hallmark of PCS (38). Moreover, PCS-IBS differs from PI-IBS in its systemic immune involvement. While PI-IBS is generally confined to the gut, PCS-IBS may reflect a broader immune dysregulation affecting multiple organ systems. Several studies have reported T cell exhaustion, altered interferon signaling, and the presence of autoantibodies in individuals with PCS, suggesting overlapping autoimmune features (39). These immune phenomena may influence gastrointestinal function through complex systemic and local mechanisms that are not typically observed in classical PI-IBS. In summary, while both PI-IBS and PCS-IBS share common features of mucosal immune activation, the latter is distinguished by more widespread and prolonged immune dysregulation. PCS-IBS may represent a distinct clinical phenotype within the spectrum of post-infectious functional gastrointestinal disorders, influenced by the unique virological and immunological properties of SARS-CoV-2. An overview of similarities and differences regarding immune dysregulation is provided in Table 3.
Gut microbiota and dysbiosis
Gastrointestinal dysbiosis—an imbalance in the composition, diversity, or metabolic function of the gut microbiota—has been implicated in both PCS and IBS, suggesting a possible shared pathophysiological pathway. However, while overlaps exist, the causal relationships and underlying mechanisms differ in nuance and extent.
Recent longitudinal and cross-sectional studies have demonstrated that individuals with PCS often exhibit persistent alterations in their gut microbiota following acute SARS-CoV-2 infection (63–65). PCS is significantly associated with persistent intestinal dysbiosis, characterized by a marked reduction in microbial diversity and the depletion of beneficial commensal bacteria (63, 66). Specifically, patients experiencing lingering symptoms often exhibit a significant loss of short-chain fatty acid (SCFA)-producing taxa, such as Fecalibacterium prausnitzii, Eubacterium rectale, Akkermansia and Bifidobacterium pseudocatenulatum, which are critical for maintaining the intestinal barrier and regulating systemic inflammation (63, 67–69). Conversely, there is an enrichment of opportunistic pathogens and pro-inflammatory species, including Ruminococcus gnavus and Bacteroides vulgatus, which have been correlated with persistent fatigue and neuropsychiatric symptoms (63, 70). Beyond bacterial dysbiosis, some studies have also provided insights into the associations between fungal dysbiosis including gut candidiasis, and PCS (71). This state of dysbiosis is thought to facilitate microbial translocation—the “leaky gut” phenomenon—whereby microbial products enter the bloodstream, sustaining low-grade systemic inflammation and potentially driving the multi-organ pathology observed in post-COVID syndrome through the gut-lung and gut-brain axes (66, 70). Although definitive proof of causality in humans remains challenging, the temporal sequence of SARS-CoV-2 infection, followed by persistent dysbiosis and long-term symptoms, supports a causal hypothesis.
In IBS, dysbiosis has long been implicated as one of several interrelated pathophysiological mechanisms (72, 73). Studies consistently report altered gut microbial composition in IBS patients, including reduced microbial diversity, decreased levels of short-chain fatty acid (SCFA)-producing bacteria, and an increase in gas-producing or pro-inflammatory microbes (74). Importantly, PI-IBS provides the strongest evidence of dysbiosis as a potential causal factor, much like in PCS gastrointestinal sequelae (Table 4).
In conclusion, both PCS and PI-IBS involve gut dysbiosis, but differ in their clinical scope and strength of causal evidence. While dysbiosis in PI-IBS is one of several contributors to a complex functional disorder, PCS dysbiosis may act as a downstream consequence of SARS-CoV-2 infection that actively contributes to ongoing systemic symptoms. It is important to note that the alterations reported across various PCS and PI-IBS studies differ considerably, potentially reflecting the influence of dietary, lifestyle, environmental, and genetic factors on gut microbiome composition. Furthermore, as the majority of microbiome samples were collected several months after symptom onset, secondary effects cannot be ruled out. Consequently, experimental models and early interventional studies employing microbiota-modulating therapies are essential to establish causality.
Neuro-immune and autonomic dysfunction
Both disorders involve dysfunction in the autonomic nervous system and neuroimmune communication. Patients with IBS and PCS may exhibit symptoms of postural orthostatic tachycardia syndrome (POTS), abnormal heart rate variability, and heightened visceral or systemic hypersensitivity. Systemic inflammation and neuroinflammation have been implicated in the development of depressive disorders and other neurocognitive symptoms including fatigue following COVID-19 (77–79). It is now widely believed that immune system dysregulation and ongoing inflammatory signaling play a central role in the pathophysiology of many PCS symptoms by disrupting multiple homeostatic systems (80, 81). Disrupted catecholamine and acetylcholine signaling may lead to autonomic dysfunction, manifesting as tachycardia, impaired regulation of vascular tone and coagulation, and a reduced capacity to control inflammation (82).
Post-exertional malaise (PEM) is frequently observed in PCS alongside fatigue and marked exercise intolerance (7, 30). Although these symptoms are pathophysiologically related, they represent distinct clinical phenomena within the spectrum of PCS manifestations. Exercise intolerance is characterized by an inability to sustain physical exertion due to diminished energy reserves or the rapid onset of symptoms such as palpitations, tachycardia, or dyspnea. In contrast, PEM refers to a delayed and maladaptive physiological response following exertion, leading to the exacerbation of symptoms including fatigue, pain, cognitive dysfunction, and a reduction in overall physical functioning (20). PEM can be triggered not just by exercise, but also by moderate physical activity or everyday tasks (83, 84). In individuals with severe myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), even minimal exertion—such as sitting upright or performing oral hygiene—may provoke PEM.
Although there are hardly any systemic manifestations in IBS compared to PCS reported, there are still indications of a dysregulation of the autonomic nervous system, with reports showing deterioration of parasympathetic response and increase in sympathetic response when performing autonomous neuropathy tests (e.g. response to standing up, deep breathing, Valsalva) (85–87). Indeed there is evidence suggesting a greater prevalence of impaired parasympathetic function in constipation-predominant IBS compared to other IBS subgroups (88).
Therapeutic insights from IBS management
A key lesson from IBS is the effectiveness of a multimodal treatment approach, including dietary interventions, psychological support, and pharmacological management. Applying similar principles to PCS may offer symptom relief and improve functional outcomes. Low-FODMAP diets, probiotics, and other gut-targeted nutritional therapies have shown benefit in IBS and may hold promise for PCS patients with gastrointestinal involvement or microbiome alterations. A recent phase III study indeed reported an improvement in PCS related fatigue and tissue metabolism using a 3-month course of a symbiotic mixture (89) and further studies are recruiting (90).
Symptomatic treatment of PCS and IBS: commonalities and differences
PCS and PI-IBS are both chronic, multisystem disorders characterized by heterogeneous and often overlapping symptomatology. To date, no definitive causal pharmacological therapies have been established for either condition. As such, the cornerstone of clinical management remains symptomatic treatment, which, while sharing certain similarities across both syndromes, also diverges in important ways due to their differing pathophysiological underpinnings. Both PCS and IBS are marked by non-specific, fluctuating symptoms—including fatigue, pain, and gastrointestinal disturbances—that necessitate individualized, multimodal therapeutic approaches tailored to the patient’s symptom profile and functional status. Dietary management is central in PI-IBS and is increasingly recognized in PCS management. For IBS, the low-FODMAP diet is often effective in reducing bloating and abdominal discomfort (91). For PCS, diet and nutrition may support recovery by targeting inflammation and the gut microbiome to alleviate symptoms and improve functional outcomes (92). In a preliminary study, a combined dietary strategy beginning with a ketogenic diet to reduce inflammation and oxidative stress, followed by the Mediterranean diet rich in whole grains, olive oil, fruits, vegetables, legumes, nuts, and lean proteins, has been proposed to improve metabolic health and alleviate symptoms, especially in individuals with obesity (93). Nutritional supplementation with compounds like acetyl L-carnitine, hydroxytyrosol, and vitamins B, C, and D has shown potential benefits in reducing fatigue and supporting immune recovery in small pilot studies (94). Additionally, dietary polysaccharides were found to provide immunomodulatory, antioxidant, and prebiotic effects in PCS and therefore may help modulate the immune response, although further validation is needed (95). While these interventions are promising, they are still experimental settings and evidence for nutritional intervention is still scare. Therefore, further research is required to establish optimized recommendations and to standardized dietary guidelines for PCS.
Cognitive behavioral therapy (CBT) and other psychological interventions are recommended for both IBS and PCS, particularly due to the strong biopsychosocial interplay. For IBS, CBT has demonstrated effectiveness in reducing symptom severity (96). In PCS, psychological support is emphasized for managing anxiety, depression, and fatigue (2).
Despite these similarities, key differences exist in the treatment strategies due to the systemic nature of PCS. Unlike PI-IBS, PCS often includes respiratory, neurological, and cardiovascular symptoms. Although these respiratory and neuro-psychological symptoms are reported more often than GI-Symptoms (7, 8) and some of these symptoms are linked to the GI-tract, there are also other pathophysiological aspects that are involved in the pathogenesis of PCS, such as a disrupted blood-brain barrier (97, 98), autoimmunity (20). This necessitates a broader therapeutic approach, involving pulmonary rehabilitation, pacing strategies for post-exertional malaise, and sometimes anticoagulants or antihistamines (99). IBS treatment, in contrast, is typically confined to the gastrointestinal tract and its functional regulation. While both conditions can be chronic, IBS is considered a lifelong functional disorder, whereas PCS is expected to resolve in some individuals over time. This distinction impacts the therapeutic goal—long-term symptom management in IBS versus potentially temporary support and monitoring in PCS.
Patient-physician-interaction
Given both, the complex multisymptomatic presentation and the therapeutic options, in PSC and IBS, strong physician-patient communication becomes crucial to ensure accurate diagnosis, effective management, and appropriate psychosocial support. In particular, physician empathy and clear communication are associated with higher patient satisfaction and better psychological outcomes, as they help patients feel validated and understood in their experience of symptoms (100). Moreover, patients with PCS or IBS often benefit from a holistic approach that addresses both the physical and psychological components of their conditions, and evidence suggests that improving communication in the clinical setting may also improve adherence to treatment plans and long-term recovery (101). Central to this interaction are advanced communication competencies, including attentive, non-directive listening, empathic validation of the patient’s experience, and the formulation of realistic therapeutic objectives—emphasizing symptom mitigation and functional improvement over curative intent. The strategic use of nonverbal communication—such as sustained eye contact, affirming gestures, forward-leaning posture, and open body orientation—further serves to foster trust and engagement. Critically, the clinical encounter should extend beyond a narrow somatic focus to encompass the patient’s broader biopsychosocial context and individual health-related goals. By fostering trust and ensuring that patients feel heard, physicians can create a supportive environment that enhances the overall quality of care and potentially accelerates recovery.
Discussion
IBS—especially in its post-infectious form—provides a valuable framework for understanding PCS. Shared features such as immune dysregulation, dysbiosis, autonomic dysfunction, and complex symptomatology suggest that therapeutic strategies used in IBS may be adapted to support PCS patients. The parallels between IBS and PCS highlight the importance of understanding post-infectious syndromes within a biopsychosocial framework. While PCS presents novel challenges, existing models like IBS offer a starting point for developing diagnostic criteria and treatment algorithms. Interdisciplinary collaboration, longitudinal research, and patient engagement are key to advancing care. Establishing a robust therapeutic alliance is a cornerstone in the effective management of patients with IBS, particularly given the complex interplay of biological, psychological, and social factors. The often unsatisfactory outcomes associated with causal therapeutic approaches for IBS support the rationale for symptom-oriented therapeutic approaches. As research advances, integrating insights from chronic functional disorders will be essential to addressing the long-term sequelae of COVID-19 and to rapidly establishing evidence-based treatment pathways for patients affected by PCS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lundberg-Morris L Leach S Xu Y Martikainen J Santosa A Gisslén M . Covid-19 vaccine effectiveness against post-covid-19 condition among 589 722 individuals in Sweden: population based cohort study. BMJ. (2023) 383:e 076990. doi: 10.1136/bmj-2023-076990, PMID: 37993131 PMC 10666099 · doi ↗ · pubmed ↗
- 2Nalbandian A Sehgal K Gupta A Madhavan MV Mc Groder C Stevens JS . Post-acute COVID-19 syndrome. Nat Med. (2021) 27:601–15. doi: 10.1038/s 41591-021-01283-z, PMID: 33753937 PMC 8893149 · doi ↗ · pubmed ↗
- 3Soriano JB Murthy S Marshall JC Relan P Diaz JVWHO Clinical Case Definition Working Group on Post-COVID-19 Conditi;on . A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. (2022) 22:e 102–7. doi: 10.1016/S 1473-3099(21)00703-9, PMID: 34951953 PMC 8691845 · doi ↗ · pubmed ↗
- 4Giszas B Trommer S Schüßler N Rodewald A Besteher B Bleidorn J . Post-COVID-19 condition is not only a question of persistent symptoms: structured screening including health-related quality of life reveals two separate clusters of post-COVID. Infection. (2023) 51:365–77. doi: 10.1007/s 15010-022-01886-9, PMID: 35869353 PMC 9307219 · doi ↗ · pubmed ↗
- 5Xie Y Choi T Al-Aly Z . Postacute sequelae of SARS-co V-2 infection in the pre-delta, delta, and omicron eras. N Engl J Med. (2024) 391:515–25. doi: 10.1056/NEJ Moa 2403211, PMID: 39018527 PMC 11687648 · doi ↗ · pubmed ↗
- 6Lopez-Leon S Wegman-Ostrosky T Perelman C Sepulveda R Rebolledo PA Cuapio A . More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. (2021) 11:16144. doi: 10.1038/s 41598-021-95565-8, PMID: 34373540 PMC 8352980 · doi ↗ · pubmed ↗
- 7Stallmach A Kesselmeier M Bauer M Gramlich J Finke K Fischer A . Comparison of fatigue, cognitive dysfunction and psychological disorders in post-COVID patients and patients after sepsis: is there a specific constellation? Infection. (2022) 50:661–9. doi: 10.1007/s 15010-021-01733-3, PMID: 34997542 PMC 8741139 · doi ↗ · pubmed ↗
- 8Taquet M Dercon Q Luciano S Geddes JR Husain M Harrison PJ . Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. P Lo S Med. (2021) 18:e 1003773. doi: 10.1371/journal.pmed.1003773, PMID: 34582441 PMC 8478214 · doi ↗ · pubmed ↗