Minimally invasive surfactant administration in extremely preterm infants <28 weeks gestation with spontaneous breathing: a retrospective quality improvement study on reducing invasive ventilation burden
Wenxin Dong, Hui Zhang, Xinyue Li, Hua Zhang, Zailing Li, Tongyan Han

TL;DR
Using a less invasive method to give surfactant to extremely preterm infants reduced their need for mechanical ventilation and lowered complications like heart issues and infections.
Contribution
This study shows that minimally invasive surfactant administration reduces invasive ventilation and complications in extremely preterm infants.
Findings
MISA reduced median IMV duration in the first 72 hours from 71 hours to 0 hours.
MISA was linked to lower rates of patent ductus arteriosus and nosocomial pneumonia.
Non-invasive ventilation duration increased with MISA use.
Abstract
Invasive surfactant delivery via endotracheal intubation increases exposure to invasive mechanical ventilation (IMV) in extremely preterm infants (EPIs, <28 weeks). This quality improvement (QI) initiative aimed to evaluate whether minimally invasive surfactant administration (MISA) was associated with a reduced IMV burden in EPIs. A single-center retrospective QI study (2013–2024) included 115 infants (24–27⁺⁶ weeks) with spontaneous breathing diagnosed with respiratory distress syndrome (RDS). Controls (2013–2019, n = 55) received surfactant via intubation; the MISA group (2020–2024, n = 60) received surfactant via thin catheter during nasal continuous positive airway pressure/nasal intermittent positive pressure ventilation (NCPAP/NIPPV). Apart from the structured implementation of MISA, background respiratory and supportive care practices evolved gradually over time without other…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
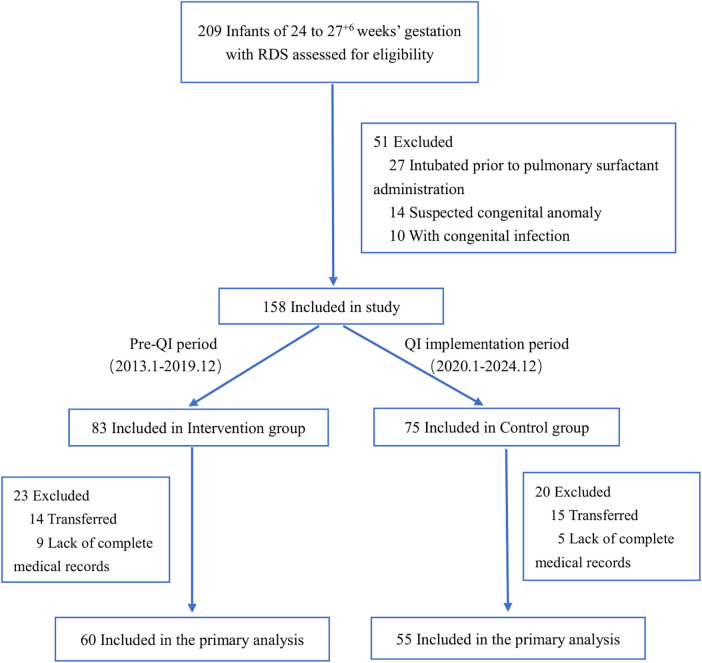 Figure 1
Figure 1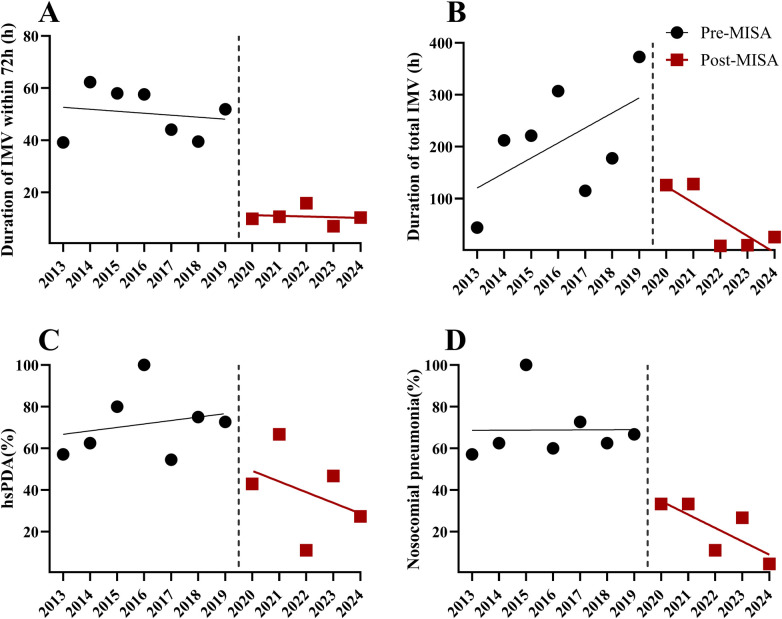 Figure 2
Figure 2| Variables | Intervention group ( | Control group ( |
| |
|---|---|---|---|---|
| Gestational age at birth, mean (SD), wk | 26.8 (0.7) | 26.7 (0.7) | 0.191 | 0.849 |
| Birth weight, mean (SD), g | 953.0 (158.0) | 979.0 (158.0) | 0.869 | 0.387 |
| Male, No. (%) | 27 (45.0) | 30 (54.5) | 1.050 | 0.306 |
| Small-for-gestational-age birth weight, No. (%) | 2 (3.33) | 0 (0) | 0.172 | |
| Multiple birth, No. (%) | 23 (38.3) | 23 (41.8) | 0.145 | 0.703 |
| Exposure to any antenatal corticosteroids, No. (%) | 54 (90.0) | 52 (94.5) | 0.822 | 0.365 |
| Apgar score ≤3 at 1 min, No. (%) | 0 | 0 | 1.000 | |
| Apgar score ≤7 at 1 min, No. (%) | 5 (8.3) | 6 (10.9) | 0.218 | 0.641 |
| Apgar score ≤7 at 5 min, No. (%) | 0 | 0 | 1.000 |
| Outcomes | Intervention group ( | Control group ( | Effect size (95% CI) | ||
|---|---|---|---|---|---|
| Primary outcome | |||||
| Duration of IMV within 72 h after birth, median (IQR), h | 0 (0,0) | 71.0 (19.0,72.0) | −7.351 | MD −40.3 (−49.8 to −30.8) | <0.001 |
| Secondary outcomes | |||||
| Required ≥ 2doses of surfactant, No./total (%) | 4/60 (6.67) | 3/55 (5.45) | OR 1.24 (0.26–5.80) | 0.549 | |
| BPD grade in survivors at 36 wk, No./total (%) | |||||
| None | 30/56 (53.6) | 25/46 (54.3) | 0.006 | OR 0.97 (0.44–2.12) | 0.938 |
| Grade 1 | 18/56 (32.1) | 12/46 (26.1) | 0.188 | OR 1.34 (0.57–3.19) | 0.665 |
| Grade 2 | 8/56 (14.3) | 9/46 (19.6) | 0.472 | OR 0.69 (0.24–1.95) | 0.492 |
| Grade 3 | 0/56 (0) | 0/46 (0) | 1 | ||
| IVH, No./total (%) | |||||
| Grade 3–4 | 5/60 (8.33) | 11/54 (20.4) | 2.383 | OR 0.36 (0.11–1.10) | 0.123 |
| Grade 1–2 | 55/60 (91.5) | 43/54 (79.6) | 0.542 | OR 3.07 (1.00–9.38) | 0.462 |
| PVL, No./total (%) | 4/60 (6.67) | 4/54 (7.41) | OR 0.89 (0.21–3.76) | 0.581 | |
| hsPDA, No./total (%) | 21/60 (35.0) | 38/55 (69.1) | 13.3 | OR 0.24 (0.11–0.53) | <0.001 |
| Pulmonary hemorrhage, No./total (%) | 3/60 (5.00) | 8/55 (14.5) | OR 0.31 (0.08–1.23) | 0.077 | |
| Pneumothorax, No./total (%) | 1/60 (1.78) | 0/55 (0) | OR 2.80 (0.11–70.14) | 0.522 | |
| Nosocomial pneumonia, No./total (%) | 11/58 (18.9) | 36/53 (67.9) | 27.2 | OR 0.11 (0.05–0.26) | <0.001 |
| LOS, No./total (%) | 14/59 (23.7) | 14/53 (26.4) | 0.107 | OR 0.87 (0.37–2.04) | 0.828 |
| ROP (stage >2), No./total (%) | 4/56 (7.1) | 1/46 (2.17) | OR 3.46 (0.37–32.06) | 0.369 | |
| In-hospital mortality, No./total (%) | 4/60 (6.67) | 9/55 (16.4) | 2.69 | OR 0.37 (0.11–1.29) | 0.101 |
| Alive at hospital discharge | |||||
| Hospitalization days, mean (SD), d | 72.6 (15.5) | 68.5 (19.7) | 1.204 | MD 3.8 (−2.3 to 10.0) | 0.232 |
| Total duration of IMV, median (IQR), h | 0 (0, 14.0) | 111.0 (38.7, 264.0) | −6.381 | MD −187.5 (−259.1 to −115.9) | <0.001 |
| Total duration of NIV, median (IQR), d | 51.5 (41.0, 57.0) | 37.0 (30, 50.3) | −3.464 | MD 10.1 (5.1–15.1) | <0.001 |
| Duration of supplemental oxygen, mean (SD), d | 59.7 (15.1) | 60.1 (20.4) | −0.142 | MD 1.1 (−5.4 to 7.6) | 0.887 |
| Outcome | Adjusted | Adjusted OR (95% CI) | |
|---|---|---|---|
| Continuous outcomes | |||
| Duration of IMV within 72 h (h) | −41.9 (−52.8 to −30.9) | — | <0.001 |
| Total duration of IMV (h) | −148.6 (−220.7 to −76.5) | — | <0.001 |
| Total duration of NIV (days) | 12.0 (6.0–18.1) | — | <0.001 |
| Duration of supplemental oxygen (days) | −2.8 (−11.0 to 5.4) | — | 0.50 |
| Binary outcomes | |||
| Nosocomial pneumonia | — | 0.084 (0.029–0.244) | <0.001 |
| hsPDA | — | 0.290 (0.106–0.794) | 0.016 |
| Late-onset sepsis | — | 1.01 (0.356–2.857) | 0.99 |
| In-hospital mortality | — | 0.306 (0.072–1.299) | 0.11 |
| Severe IVH (Grade III–IV) | — | 0.429 (0.116–1.587) | 0.21 |
| Pulmonary hemorrhage | — | 0.275 (0.056–1.351) | 0.112 |
| PVL | — | 1.85 (0.25–13.51) | 0.548 |
| Required ≥ 2 doses of surfactant | — | 0.91 (0.162–5.00) | 0.912 |
| BPD (Any grade) | — | 1.69 (0.699–4.17) | 0.242 |
| Outcome | Baseline trend (β, 95% CI) | Immediate level change (β, 95% CI) | Change in slope (β, 95% CI) | |||
|---|---|---|---|---|---|---|
| Continuous outcomes | ||||||
| Duration of IMV within 72 h | −0.76 (−4.41 to 2.90) | 0.65 | −36.05 (−58.21 to −13.90) | 0.006 | 0.49 (−6.63 to 7.61) | 0.88 |
| Total duration of IMV | 28.96 (−7.29 to 65.21) | 0.10 | −199.59 (−419.48 to 20.30) | 0.070 | −60.80 (−131.46 to 9.86) | 0.083 |
| Binary outcomes (%) | ||||||
| Nosocomial pneumonia | 0.05 (−6.07 to 6.16) | 0.99 | −34.33 (−71.42 to 2.76) | 0.065 | −6.47 (−18.39 to 5.45) | 0.25 |
| hsPDA | 1.65 (−6.63 to 9.93) | 0.66 | −29.17 (−79.40 to 21.07) | 0.22 | −6.77 (−22.91 to 9.37) | 0.36 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Respiratory Support and Mechanisms · Infant Development and Preterm Care
Introduction
Respiratory distress syndrome (RDS) remains the predominant cause of morbidity and mortality in extremely preterm infants (EPIs) born at <28 weeks' gestation (1, 2). The pathophysiology centers on pulmonary surfactant deficiency compounded by structural lung immaturity. Conventional management requires endotracheal intubation for surfactant delivery coupled with invasive mechanical ventilation (IMV) (3). Although this approach improves respiratory failure, it inherently carries significant iatrogenic risks—notably bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (IVH), and ventilator-induced lung injury (4). These complications disproportionately affect EPIs due to heightened vulnerability of their developing organs to invasive interventions (5).
Minimally invasive surfactant administration (MISA) has emerged as a paradigm-shifting alternative (6, 7). By administering surfactant via a thin catheter during non-invasive ventilation (NIV), MISA preserves spontaneous breathing, circumvents laryngeal trauma, and reduces IMV exposure (2, 8). Current evidence, however, predominantly supports its efficacy in preterm infants ≥28 weeks' gestation (3, 9, 10). Multicenter trials demonstrate reduced IMV duration in this cohort, yet subgroup analyses for infants <28 weeks remain underpowered due to limited sample sizes. Consequently, robust evidence regarding MISA's safety and effectiveness in the most vulnerable EPIs (<28 weeks)—a population with distinct physiological challenges including frequent respiratory failure and diminished tolerance to procedural stress—remains limited.
This relative paucity of specific data for the <28 weeks subgroup necessitates careful evaluation of MISA implementation in real-world settings, particularly within individual institutions. While quality improvement (QI) initiatives have refined respiratory support protocols in neonatal intensive care units (NICUs) (11, 12), the practical impact of MISA on reducing invasive ventilation burden specifically in EPIs <28 weeks warrants further examination based on institutional experience.
In our NICU, MISA has been progressively incorporated into the clinical pathway for spontaneously breathing preterm infants with RDS since 2020, building upon emerging evidence suggesting potential benefits in younger infants (3). This retrospective quality improvement study aimed to evaluate our institutional experience with MISA in EPIs. We compared outcomes between a historical cohort receiving surfactant via traditional endotracheal intubation and a subsequent cohort managed with the MISA approach. Our primary objective was to assess whether implementing MISA within our standardized QI framework was associated with changes in the duration of invasive mechanical ventilation within the critical first 72 h of life. Secondary objectives included exploring potential differences on other respiratory support durations and relevant complications. By analyzing this experience, we aimed to provide real-world data from a single-center QI initiative to inform surfactant administration strategies in this high-risk population and to offer contextual insights for similar clinical settings.
Materials and methods
Study design
This was a single-center, retrospective QI study conducted in NICU of Peking University Third Hospital from January 1, 2013, to December 31, 2024. The study compared two surfactant administration strategies:
Control group (pre-QI period: 2013–2019): Surfactant delivery via endotracheal intubation with IMV.
Intervention group (during QI implementation period: 2020–2024): MISA, involving surfactant delivery via a thin catheter during nasal continuous positive airway pressure (NCPAP) or nasal intermittent positive pressure ventilation (NIPPV)-assisted spontaneous breathing.
The QI initiative commenced on January 1, 2020, following the formation of a dedicated team (comprising three neonatologists) responsible for standardizing MISA protocols and facilitating staff training.
Study population
Inclusion criteria:
- Infants of 24 to 27^+6^ weeks' gestation.
- Infants with spontaneous breaths and signs of respiratory distress that received non-invasive respiratory support immediately after birth in a delivery room and during transfer to the NICU.
- Clinical diagnosis of RDS within the first 6 h of life. The diagnosis of RDS was based on clinical manifestations (respiratory rate >60/min, nasal flaring, retractions, grunting, or skin cyanosis) and [FiO_2_] > 0.3 for [SpO_2_] > 85%. Exclusion criteria:
Infants meeting any of the following criteria were excluded:
- Infants intubated prior to pulmonary surfactant administration due to postnatal
- resuscitation or other reasons.
- Infants with obvious malformations affecting respiratory function.
- Infants transferred to other hospitals for surgery with incomplete data.
- Infants withdrawn from the NICU by parents due to financial difficulties or poor prognosis.
- Lack of complete medical records.
Intervention: MISA protocol
This technique is also described in the literature as less invasive surfactant administration (LISA) or minimally invasive surfactant therapy (MIST).Although terminology varies, these terms refer to the same thin-catheter surfactant delivery approach during spontaneous breathing. In this manuscript, we use “MISA” for our institutional practice while retaining the original terminology when citing external studies. Throughout the 12-year study period (2013–2024), the general clinical management of extremely preterm infants in our unit evolved gradually in accordance with contemporaneous international and national guidelines, without abrupt structural changes in core respiratory or supportive care strategies. Delivery-room stabilization, early non-invasive respiratory support (primarily CPAP-based), routine caffeine administration, infection-prevention practices, nutritional support, and PDA management followed standardized institutional protocols that were updated incrementally over time in line with evolving evidence (13, 14). During the transition between periods, no additional structured respiratory quality-improvement programs were introduced apart from MISA. Within this relatively stable clinical framework, the implementation of the MISA protocol represented the principal structured quality-improvement intervention specifically targeting surfactant administration strategy.
Standardized MISA procedure
Under NCPAP or NIPPV, the pulmonary surfactant was administered via MISA method within 6 h after birth if infants were clinically diagnosed with RDS. While the infants received NCPAP or NIPPV, a direct laryngoscope and a specifically designed thin catheter with 1.67 mm in diameter (catheter R, Beijing Double-crane pharmaceutical Co. LTD) were used to finish the surfactant administration. A direct laryngoscope was introduced to provide a glottal view before the operator inserts the catheter R 0.5–1.0 cm below the inverted V-shaped vocal cords. After withdrawing the laryngoscope, the operator fixed the thin catheter at the infant's mouth corner with the forefinger and thumb, and the end of the catheter R was connected to a 5 mL syringe containing surfactant solution. The surfactant at a dose of 100 mg/kg calf pulmonary surfactant (Beijing Double-Crane Pharmaceuticals Co. Ltd.) or a dose of 200 mg/kg Curosurf ® (Poractant alfa, Chiesi Farmaceutici, Italy) was administered through the catheter R by a nurse within 120–300 s by mini-boluses. The catheter R was immediately removed after surfactant administration. Infants remained on NCPAP or NIPPV post-administration unless meeting predefined intubation criteria (FiO_2_ > 0.4, pH: <7.20, or recurrent apnea).
All infants breathing spontaneously and those planned to be extubated soon received caffeine.
Multiteam engagement
Weekly audits of surfactant administration practices.Real-time feedback to clinicians on adherence to MISA protocols.Monthly training sessions for NICU staff on catheter insertion techniques and complication management.
Documentation and feedback
Electronic health records (EHRs) were updated to include MISA-specific fields (e.g., catheter placement attempts, adverse events).Quarterly reports on MISA utilization rates and outcomes were reviewed by the QI team.
Data collection and variables
Data were extracted retrospectively from EHRs using a structured template. The clinical data collected encompassed maternal and neonatal demographic characteristics (including birth weight, gestational age, sex, singleton/multiple gestation, Apgar scores at 1 and 5 min, antenatal corticosteroid administration), and in-hospital outcomes.
Outcome measures
Primary outcome measure
The primary outcome was duration of IMV within 72 h after birth.
Secondary outcome measures
The secondary outcomes were as follows: requirement for≥2 doses of surfactant, BPD, IVH, periventricular leukomalacia (PVL), hemodynamically significant patent ductus arteriosus (hsPDA), pulmonary hemorrhage, pneumothorax, nosocomial pneumonia, late-onset sepsis (LOS) and severe retinopathy of prematurity (ROP, stage >2), in-hospital mortality, length of hospital stay, total duration of NIV, total duration of IMV, and days on supplemental oxygen.
Disease diagnosis
BPD will be diagnosed according to the National Institutes of Health criteria (15). Pneumothorax will be diagnosed by the presence of air in the pleural cavity in a chest x-ray. Pulmonary hemorrhage will be diagnosed based on the gushing of bloody fluid from the upper airway or endotracheal intubation and when the chest x-ray is consistent with the relevant clinical findings. The diagnosis for hsPDA will be based on clinical signs and echocardiogram (16). IVH and PVL will be diagnosed by cranial ultrasound examination, and IVH will be graded by the Papile classification system (17). Nosocomial pneumonia developing ≥48 h after hospital admission with clinical and radiographic evidence. LOS will be defined as clinical sepsis with evidence of pathogens in blood culture. The diagnosis and staging of ROP will be based on retinal examination by a consultant ophthalmologist.
Statistical analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corp.). Continuous data are presented as mean ± standard deviation for normally distributed variables or median with interquartile range (IQR) for non-normally distributed variables. Group comparisons for continuous variables utilized the Student's t-test (parametric) or the Mann–Whitney U test (non-parametric), based on distribution normality. Categorical variables are reported as frequencies (percentages), with group differences assessed using the chi-square test or Fisher's exact test for small cell counts.
To evaluate the independent effect of MISA, multivariable logistic and linear regressions were performed to adjust for confounders (gestational age, birth weight, sex, and antenatal steroids). Furthermore, Interrupted time-series (ITS) analysis was conducted based on annual data points (2013–2024, n = 12) to adjust for secular trends. Effect sizes are reported as odds ratios (ORs) or mean differences with 95% confidence intervals (CIs). Figures were generated using GraphPad Prism version 10.0. Given the retrospective and exploratory nature of this study, no formal adjustment for multiple comparisons (e.g., Bonferroni correction) was applied to the secondary outcomes. Two-tailed p-values <0.05 were considered significant; p-values reported as 0.000 by software were corrected to p < 0.001.
Ethical considerations
The study was approved by the Institutional Review Board of Peking University Third Hospital (Protocol No: M20250673). Patient data were de-identified, and informed consent was waived due to the retrospective nature of the study.
Results
Trial population
A total of 209 infants born at 24–27^+6^ weeks' gestation with RDS were assessed for eligibility between January 2013 and December 2024 (Figure 1). After excluding 51 infants (27 intubated prior to surfactant administration, 14 with suspected congenital anomalies, and 10 with congenital infections), 158 infants were enrolled in the study. Following additional exclusions due to transfers and incomplete records, 115 infants were included in the final analysis: 60 in the intervention group (2020–2024 QI period) and 55 in the control group (2013–2019 pre-QI period).
Patient recruitment flowchart. RDS, respiratory distress syndrome; QI, quality improvement.
Baseline characteristics
Infant demographics and clinical characteristics were comparable between groups (Table 1). There were no significant differences in gestational age (26.8 ± 0.7 vs. 26.7 ± 0.7 weeks, P = 0.849), birth weight (953 ± 158 g vs. 979 ± 158 g, P = 0.387), sex distribution (45.0% vs. 54.5% male, P = 0.306), antenatal corticosteroid exposure (90.0% vs. 94.5%, P = 0.365), or Apgar scores indicative of asphyxia at 1 or 5 min (all P > 0.05).
Primary outcome
The median duration of IMV within the first 72 h after birth was 0 h (IQR: 0–0) in the intervention group compared to 71.0 h (IQR: 19.0–72.0) in the control group (Z = −7.351, P < 0.001) (Table 2). In multivariable linear regression analysis adjusting for gestational age, birth weight, sex, multiple gestation, antenatal steroid exposure, and 5 min Apgar score, the estimated difference in early IMV duration between groups remained statistically significant (adjusted β = 41.9 h, 95% CI: 30.9–52.8, P < 0.001) (Table 3).
Secondary outcomes
Total IMV duration was reduced [0 h (IQR: 0–14) vs. 111 h (IQR: 39–264); P < 0.001], while NIV duration was longer [51.5d (IQR: 41–57) vs. 37d (IQR: 30–50); P < 0.001] in the intervention group compared to the control group. After adjustment for baseline characteristics, these differences remained statistically significant (IMV: adjusted β = −148.6, 95% CI: −220.7 to −76.5, P < 0.001; NIV: adjusted β = 12.0, 95% CI: 6.0–18.1, P < 0.001) (Tables 2, 3).
The incidence of hsPDA was lower in the intervention group compared with the control group (35.0% vs. 69.1%; P < 0.001). In the adjusted logistic regression model, the between-group difference was statistically significant (adjusted OR = 0.290, 95% CI: 0.106–0.794, P = 0.016). Nosocomial pneumonia occurred less frequently in the intervention group (18.9% vs. 67.9%; P < 0.001). The adjusted analysis yielded a statistically significant between-group difference (adjusted OR = 0.084, 95% CI: 0.029–0.244, P < 0.001) (Tables 2, 3).
Additionally, no significant between-group differences were observed for severe IVH, mortality, requirement for ≥2 doses of surfactant, BPD severity, PVL, pulmonary hemorrhage, LOS, severe ROP, duration of supplemental oxygen, or length of hospital stay (all P > 0.05). After multivariable adjustment, these findings remained unchanged, and no statistically significant associations were identified for these outcomes (Tables 2, 3).
The analysis of BPD and hospitalization outcomes was restricted to infants who survived to discharge. Analyses for LOS and nosocomial pneumonia excluded three infants who died within 72 h, with one of these also excluded from IVH and PVL assessments due to lacking cranial ultrasound.
Interrupted time-series analysis
The results of the ITS analysis are presented in Table 4 and Figure 2. While the ITS model included annual time points, the relatively small sample size per year may have contributed to fluctuations in the estimates. Following implementation of MISA, an immediate level change in early IMV duration was estimated (β = −36.05 h, 95% CI: −58.21 to −13.90, P = 0.006). No statistically significant baseline pre-intervention trend was detected. For total IMV duration, a change in slope was estimated (β = −199.59, 95% CI: −419.48 to 20.30, P = 0.070), although the result did not reach statistical significance. For hsPDA and nosocomial pneumonia, regression coefficients showed changes in the same direction as those observed in the cohort analysis; however, these did not reach statistical significance in the ITS model (all P > 0.05).
Interrupted time series analysis of key outcomes (A) IMV duration within 72 h. (B) Total IMV duration. (C) Incidence of hsPDA. (D) Incidence of nosocomial pneumonia. The vertical dashed line marks the MISA implementation. Circles and squares denote observed pre- and post-intervention data, respectively; solid lines represent regression trends. IMV, invasive mechanical ventilation; hsPDA, hemodynamically significant patent ductus arteriosus; MISA, minimally invasive surfactant administration.
Discussion
This retrospective quality improvement study evaluated the integration of MISA into the management pathway for RDS in spontaneously breathing EPIs under 28 weeks of gestation within a standardized framework. The baseline characteristics, including gestational age, birth weight, antenatal corticosteroid exposure, and Apgar scores indicative of perinatal asphyxia at 1 and 5 min, were comparable between the two groups. Compared to the historical control group receiving surfactant via endotracheal intubation, MISA implementation was associated with shorter IMV duration within the first 72 h and lower incidences of hsPDA and nosocomial pneumonia, with findings remaining consistent after multivariable adjustment. In the ITS analysis, only early IMV showed a significant immediate reduction, whereas hsPDA and nosocomial pneumonia demonstrated similar directional trends without statistical significance. Nevertheless, these observations should be considered exploratory and interpreted with caution given the relatively small number of patients per year and the inherent limitations of the historical-control design with potential residual confounding.
The primary finding of this study—that MISA was associated with a reduced burden of mechanical ventilation within 72 h and overall—aligns with the conclusions of several previous studies involving similar gestational age groups, including those by Boskabadi et al. (26–34 weeks) (18), Anand et al. (26–34 weeks) (19), Dargaville et al. (25–28 weeks) (20), Kaleem et al. (<34 weeks) (21), and Wang et al. (<32 weeks) (22). Furthermore, a meta-analysis by Abdel-Latif et al., which pooled evidence from 16 randomized trials, reported that the MISA method reduced the risk of death or BPD, decreased intubation within 72 h, and lowered the incidence of major complications and in-hospital mortality (23). This beneficial effect may stem from MISA's dual protective mechanisms: avoiding the stress of intubation and eliminating the injury associated with early positive pressure ventilation. Animal studies suggest that mechanical ventilation can impair the initial lung tissue association of exogenous surfactant, linked to reduced dynamic compliance and increased surfactant inactivation. In contrast, the surfactant distribution process during MISA is likely more physiological (18, 24?–26).
Regarding secondary outcomes, the MISA group was associated with a lower incidence of hsPDA, aligning with findings from previous studies (3). This observed association may be related to the avoidance of invasive positive pressure ventilation and its associated hemodynamic fluctuations. First, MISA preserves spontaneous breathing and physiological intrathoracic pressure, which avoids the compromised systemic venous return and hemodynamic instability often linked to invasive ventilation—factors known to influence ductal patency. Second, by minimizing procedure-related hypoxia and mechanical lung injury, MISA may help maintain stable arterial oxygen tension and reduce the release of inflammatory mediators (e.g., prostaglandins), both of which are critical for facilitating ductal constriction (18, 27, 28). The incidence of nosocomial pneumonia was also lower in the MISA group. Boskabadi et al. similarly reported reduced infection-related complications in their MIST group (18). This observed association may be partially explained by avoiding endotracheal intubation and significantly shortening IMV duration, thereby directly reducing exposure to the risk of VAP. Interestingly, the incidence of LOS remained comparable between the two groups. While the continuous refinement of neonatal intensive care practices over the study period undoubtedly improved overall clinical safety, the observed reduction in pneumonia—in the context of stable LOS rates—suggests that the implementation of MISA may have provided an additional, targeted advantage in protecting the vulnerable respiratory tract of these extremely preterm infants.
In the present study, no significant differences were observed between groups for other outcomes, including severe IVH, mortality, BPD, PVL, pulmonary hemorrhage, LOS, severe ROP, or length of hospital stay. Specifically, our study may have been underpowered to detect differences in mortality and severe IVH due to the small sample size. Additionally, the absence of severe BPD cases may be attributed to our inclusion criteria and a potential survival bias, as the most critical infants might not have survived to the assessment age. Our findings regarding secondary complications are consistent with the heterogeneity observed in existing literature. For instance, while the OPTIMIST-A trial reported a reduced incidence of BPD with LISA (20), other studies and a systematic review by Kuitunen et al. found mixed results or no significant differences in outcomes such as IVH and pneumothorax (29–31). The heterogeneity in reported outcomes for these complications across the literature may be attributed to the inherently high-risk profile of EPIs. The elevated baseline rate of severe morbidities in infants under 28 weeks can dilute the measurable effect of a single intervention, thereby complicating the interpretation of MISA's independent contribution. Furthermore, differences in study design, sample size, and background care practices likely contribute to these discrepant findings.
This study involved a trade-off associated with the change in respiratory support mode. While MISA shortened IMV duration and avoided its direct risks (barotrauma, VAP), it was associated with a prolonged duration of NIV, which could potentially increase the risks of nasal injury and high oxygen requirements. A key strength of this study is its focus on the EPI subgroup under 28 weeks, for which evidence is scarce, providing high-quality real-world data. The implementation within a standardized QI framework—incorporating defined procedures, training, and auditing—enhances the reproducibility of this practice.
Nevertheless, this study has several limitations. The retrospective, historical control design cannot entirely separate the independent effect of MISA from the secular trends in NICU care over the 12-year period. We acknowledge that clinical protocols and respiratory management evolved progressively, which may have contributed to the improved outcomes. Although we employed multivariable regression and ITS analysis to mitigate these effects, residual confounding may still remain. Furthermore, the single-center nature limits generalizability, and the relatively small sample size may have underpowered our ability to detect differences in less frequent outcomes, such as mortality and severe IVH. To confirm these preliminary findings, prospective parallel-controlled trials or multi-center contemporaneous comparisons are warranted.
Conclusion
This study indicates that the implementation of MISA, supported by a systematic quality improvement framework, is associated with a significant reduction in both early and total invasive mechanical ventilation burden in extremely preterm infants under 28 weeks of gestation. It is also associated with a decreased incidence of hemodynamically significant PDA and nosocomial pneumonia, without evidence of increased major short-term risks in this cohort. These findings support MISA as a feasible and potentially beneficial strategy for reducing exposure to invasive ventilation in this vulnerable population. However, the prolonged duration of non-invasive ventilation (NIV) observed during the MISA period represents a potential trade-off that warrants further evaluation. Given the inherent limitations of the retrospective, single-center, historical-control design, these findings should be interpreted as associations rather than definitive causal links, as residual confounding from secular trends in neonatal intensive care practices cannot be entirely excluded. Furthermore, the impact of MISA on long-term neurodevelopmental and pulmonary outcomes requires validation through large-scale, prospective, multicenter randomized controlled trials. Continual optimization of MISA procedures and integration of robust quality improvement initiatives remain essential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alsina-Casanova M Brito N Balcells-Esponera C Herranz-Barbero A Teresa-Palacio M Soler-García A Predictors of CPAP failure after less-invasive surfactant administration in preterm infants. Front Pediatr. (2024) 12:1444906. 10.3389/fped.2024.144490639258148 PMC 11383777 · doi ↗ · pubmed ↗
- 2Heiring C Hedegaard SS Carlsen EM Kristensen R Breindahl N Schmidt C Less invasive surfactant administration versus intubate-surfactant-extubate: associated with reduced mechanical ventilation in extremely preterm infants. Acta Paediatr. (2025). 10.1111/apa.70041 PMC 1225812940008543 · doi ↗ · pubmed ↗
- 3Han T Liu H Zhang H Guo M Zhang X Duan Y Minimally invasive surfactant administration for the treatment of neonatal respiratory distress syndrome: a multicenter randomized study in China. Front Pediatr. (2020) 8:182. 10.3389/fped.2020.00182 PMC 722105532457854 · doi ↗ · pubmed ↗
- 4Dini G Santini MG Celi F Verrotti A. Less invasive surfactant administration versus intubation-surfactant-extubation in preterm infants: a retrospective study. Med Glas (Zenica). (2024) 21(2):309–14.39526720 10.17392/1726-21-02 · doi ↗ · pubmed ↗
- 5Edwards EM Ehret DEY Cohen H Zayack D Soll RF Horbar JD. Quality improvement interventions to prevent intraventricular hemorrhage: a systematic review. Pediatrics. (2024) 154(2):e 2023064431. 10.1542/peds.2023-06443138982935 · doi ↗ · pubmed ↗
- 6Breindahl N Henriksen TB Heiring C Bay ET Haaber J Salmonsen TG NON-pharmacological approach less invasive surfactant administration (NONA-LISA) trial: protocol for a randomised controlled trial. Pediatr Res. (2024) 96(4):1084–9. 10.1038/s 41390-023-02998-038200325 PMC 11502479 · doi ↗ · pubmed ↗
- 7Buyuktiryaki M Alarcon-Martinez T Simsek GK Canpolat FE Tayman C Oguz SS Five-year single center experience on surfactant treatment in preterm infants with respiratory distress syndrome: LISA vs INSURE. Early Hum Dev. (2019) 135:32–6. 10.1016/j.earlhumdev.2019.06.00431229792 · doi ↗ · pubmed ↗
- 8Federici C Fornaro G Roehr CC. Cost-saving effect of early less invasive surfactant administration versus continuous positive airway pressure therapy alone for preterm infants with respiratory distress syndrome. Eur J Hosp Pharm. (2022) 29(6):346–52. 10.1136/ejhpharm-2020-00246533658228 PMC 9614139 · doi ↗ · pubmed ↗