Racial and Gender Disparities in the Occurrence and Outcomes of Alcohol-Associated Hepatitis in Hospitalized Patients With Prior Bariatric Surgery
Sarpong Boateng, Solomon Gyabaah, Yussif Issaka, Guy Loic Nguefang Tchoukeu, Prince Ameyaw, Chimezirim Ezeano, Yazan Al-Ajlouni, Basile Njei

TL;DR
Bariatric surgery may protect against severe outcomes in alcohol-related liver disease, with higher hospitalization rates among women and Black patients.
Contribution
This study identifies a potential protective effect of bariatric surgery on alcohol-associated hepatitis outcomes and highlights racial and gender disparities in hospitalization rates.
Findings
Bariatric surgery was linked to lower in-hospital mortality and complications in patients with alcohol-associated hepatitis.
Female and Black patients had higher odds of AAH hospitalization following bariatric surgery compared to males and White patients.
No differences in outcomes were observed across sex or race after bariatric surgery.
Abstract
Background There is an increased risk of alcohol use disorder post-bariatric surgery. The impact of bariatric surgery on the outcomes of alcohol-associated hepatitis (AAH) remains unclear. Hence, we aimed to evaluate whether a history of bariatric surgery influences in-hospital outcomes of AAH and whether these associations vary by sex or race. Methodology We conducted a retrospective, cross-sectional study using the 2016-2020 National Inpatient Sample to identify adult hospitalizations with AAH and bariatric surgery diagnoses. We performed a 1:1 propensity score matching. Matching variables included baseline characteristics (age, sex, primary payer source, race, etc.), clinical comorbidities (diabetes, hypertension, etc.), and outcomes (in-hospital mortality, acute kidney injury, heart failure, major adverse cardiovascular event, length of stay, death, etc). Multivariable regression…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
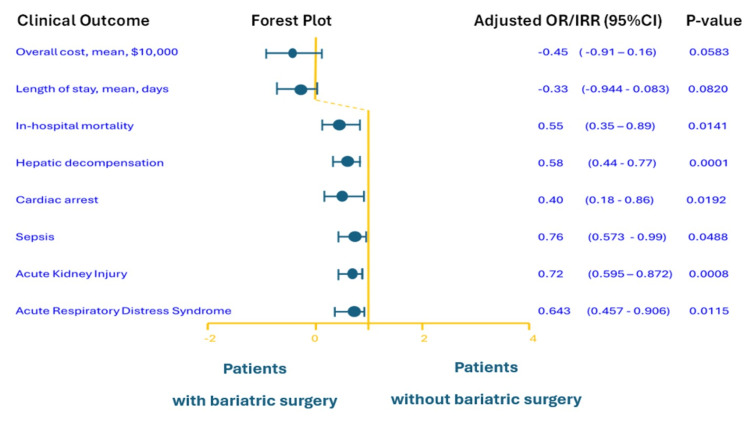 Figure 1
Figure 1| History of bariatric surgery | No | Yes | Total | Test statistic | P-value |
| (N = 98,548) | (N = 2,362) | (N = 100,910) | |||
| Age in years at admission | 0.80 | 0.371 | |||
| N | 98,548 | 2,362 | 100,910 | ||
| Mean (SD) | 47.60 (12.44) | 47.40 (9.43) | 47.6 (12.38) | ||
| Sex | 2,218.25 | <0.012 | |||
| Male | 68,421 (69.44%) | 563 (23.84%) | 68,984 (68.37%) | ||
| Female | 30,114 (30.56%) | 1,799 (76.16%) | 31,913 (31.63%) | ||
| Primary payer source | 225.58 | <0.012 | |||
| Private insurance | 16,028 (16.30%) | 424 (18.00%) | 16,452 (16.30%) | ||
| Medicaid | 39,411 (40.10%) | 774 (32.80%) | 40,185 (39.90%) | ||
| Medicare | 25,111 (25.50%) | 889 (37.70%) | 26,000 (25.80%) | ||
| Other payment source | 12,803 (13.00%) | 185 (7.80%) | 12,988 (12.90%) | ||
| Self-pay | 1,310 (1.30%) | 16 (0.70%) | 1,326 (1.30%) | ||
| No charge | 3,688 (3.70%) | 70 (3.00%) | 3,758 (3.70%) | ||
| Race/Ethnicity | 82.96 | <0.012 | |||
| White | 66,706 (70.00%) | 1,680 (73.30%) | 68,386 (70.10%) | ||
| Black | 10,625 (11.10%) | 324 (14.10%) | 10,949 (11.20%) | ||
| Hispanic | 11,752 (12.30%) | 192 (8.40%) | 11,944 (12.20%) | ||
| Asian or Pacific Islander | 1,189 (1.20%) | 12 (0.50%) | 1,201 (1.20%) | ||
| Native American | 2,309 (2.40%) | 20 (0.90%) | 2,329 (2.40%) | ||
| Other | 2,749 (2.90%) | 64 (2.80%) | 2,813 (2.90%) | ||
| Median household income ($) | 27.60 | 0.012 | |||
| <38,999 | 26,040 (27.30%) | 558 (24.10%) | 26,598 (27.20%) | ||
| 39,000–47,999 | 24,479 (25.70%) | 617 (26.60%) | 25,096 (25.70%) | ||
| 48,000–62,999 | 24,572 (25.80%) | 609 (26.30%) | 25,181 (25.80%) | ||
| >63,000 | 20,253 (21.20%) | 534 (23.00%) | 20,787 (21.30%) | ||
| Weekend admission | 0.59 | 0.442 | |||
| No | 73,490 (74.60%) | 1,745 (73.90%) | 75,235 (74.60%) | ||
| Yes | 25,058 (25.40%) | 617 (26.10%) | 25,675 (25.40%) | ||
| Elective admission | 1.56 | 0.922 | |||
| No | 95,093 (96.60%) | 2,278 (96.60%) | 97,371 (96.60%) | ||
| Yes | 3,336 (3.40%) | 79 (3.40%) | 3,415 (3.40%) | ||
| Region of the hospital | 34.81 | <0.012 | |||
| Northeast | 19,659 (19.90%) | 557 (23.60%) | 20,216 (20.00%) | ||
| Midwest | 23,599 (23.90%) | 620 (26.20%) | 24,219 (24.00%) | ||
| South | 28,957 (29.40%) | 621 (26.30%) | 29,578 (29.30%) | ||
| West | 26,333 (26.70%) | 564 (23.90%) | 26,897 (26.70%) | ||
| Hospital size | 0.53 | 0.762 | |||
| Small | 22,654 (23.00%) | 553 (23.40%) | 23,207 (23.00%) | ||
| Medium | 30,149 (30.60%) | 707 (29.90%) | 30,856 (30.60%) | ||
| Large | 45,745 (46.40%) | 1,102 (46.70%) | 46,847 (46.40%) | ||
| Location/Teaching status | 8.04 | 0.022 | |||
| Rural | 7,377 (7.50%) | 142 (6.00%) | 7,519 (7.50%) | ||
| Urban non-teaching | 22,588 (22.90%) | 532 (22.50%) | 23,120 (22.90%) | ||
| Urban teaching | 68,583 (69.60%) | 1,688 (71.50%) | 70,271 (69.60%) | ||
| Elixhauser Comorbidity Index | 54.18 | <0.011 | |||
| N | 76,145 | 1,804 | 77,949 | ||
| Mean (SD) | 5.20 (1.75) | 5.50 (1.77) | 5.20 (1.75) | ||
| Diabetes | 13.62 | <0.012 | |||
| No | 91,946 (93.30%) | 2,249 (95.20%) | 94,195 (93.30%) | ||
| Yes | 6,602 (6.70%) | 113 (4.80%) | 6,715 (6.70%) | ||
| Hypertension | 2.09 | 0.152 | |||
| No | 54,056 (54.90%) | 1,331 (56.40%) | 55,387 (54.90%) | ||
| Yes | 44,492 (45.10%) | 1,031 (43.60%) | 45,523 (45.10%) | ||
| Obesity | 1,165.63 | <0.012 | |||
| No | 88,911 (90.20%) | 1,621 (68.60%) | 90,532 (89.70%) | ||
| Yes | 9,637 (9.80%) | 741 (31.40%) | 10,378 (10.30%) | ||
| Variable | P-value | Test statistic | Standardized difference | ||
| History of bariatric surgery | No | Yes | |||
| (N = 2,242) | (N = 2,242) | ||||
| Age in years at admission | 0.451 | 0.57 | 0.01 | ||
| N | 2,242 | 2,242 | |||
| Mean (SD) | 47.20 (12.24) | 47.30 (9.43) | |||
| Sex | 0.172 | 1.88 | 0.04 | ||
| Male | 500 (22.30%) | 539 (24.04%) | |||
| Female | 1,742 (77.70%) | 1,703 (75.56%) | |||
| Primary payer source | 0.992 | 0.30 | 0.04 | ||
| Private Insurance | 398 (17.80%) | 403 (18.00%) | |||
| Medicaid | 728 (32.50%) | 735 (32.80%) | |||
| Medicare | 851 (38.00%) | 841 (37.50%) | |||
| Other payment source | 183 (8.20%) | 179 (8.00%) | |||
| Self-pay | 14 (0.60%) | 16 (0.70%) | |||
| No charge | 68 (3.00%) | 68 (3.00%) | |||
| Race/Ethnicity | 0.662 | 3.25 | 0.12 | ||
| White | 1,665 (74.30%) | 1,644 (73.30%) | |||
| Black | 305 (13.60%) | 319 (14.20%) | |||
| Hispanic | 192 (8.60%) | 186 (8.30%) | |||
| Asian or Pacific Islander | 14 (0.60%) | 12 (0.50%) | |||
| Native American | 11 (0.50%) | 19 (0.80%) | |||
| Other | 55 (2.50%) | 62 (2.80%) | |||
| Median household income ($) | 0.572 | 2.01 | 0.07 | ||
| <38,999 | 571 (25.50%) | 538 (24.00%) | |||
| 39,000–47,999 | 599 (26.70%) | 602 (26.90%) | |||
| 48,000–62,999 | 586 (26.10%) | 585 (26.10%) | |||
| >63,000 | 486 (21.70%) | 517 (23.10%) | |||
| Weekend admission | 0.542 | 0.38 | 0.04 | ||
| No | 1,669 (74.40%) | 1,651 (73.60%) | |||
| Yes | 573 (25.60%) | 591 (26.40%) | |||
| Elective admission | 0.332 | 0.98 | 0.02 | ||
| No | 2,181 (97.30%) | 2,170 (96.80%) | |||
| Yes | 61 (2.70%) | 72 (3.20%) | |||
| Region of the hospital | 0.932 | 0.18 | 0.11 | ||
| Northeast | 544 (24.30%) | 546 (24.40%) | |||
| Midwest | 573 (25.60%) | 568 (25.30%) | |||
| South | 583 (26.00%) | 600 (26.80%) | |||
| West | 542 (24.20%) | 528 (23.60%) | |||
| Hospital size | 0.622 | 0.95 | 0.00 | ||
| Small | 500 (22.30%) | 525 (23.40%) | |||
| Medium | 707 (31.50%) | 685 (30.60%) | |||
| Large | 1,035 (46.20%) | 1,032 (46.00%) | |||
| Location/Teaching status | 0.512 | 1.35 | 0.06 | ||
| Rural | 131 (5.80%) | 130 (5.80%) | |||
| Urban non-teaching | 471 (21.00%) | 503 (22.40%) | |||
| Urban teaching | 1,640 (73.10%) | 1,609 (71.80%) | |||
| Elixhauser Comorbidity Index | 0.032 | 4.62 | 0.00 | ||
| N | 1,705 | 1,706 | |||
| Mean (SD) | 5.4 (1.83) | 5.5 (1.77) | |||
| Diabetes | 0.352 | 0.87 | 0.015 | ||
| No | 2,117 (94.40%) | 2,131 (95.00%) | |||
| Yes | 125 (5.60%) | 111 (5.00%) | |||
| Hypertension | 0.762 | 0.00 | 0.01 | ||
| No | 1,246 (55.60%) | 1,256 (56.00%) | |||
| Yes | 996 (44.40%) | 986 (44.00%) | |||
| Obesity | 1.002 | 0.00 | 0.00 | ||
| No | 1,530 (68.20%) | 1,530 (68.20%) | |||
| Yes | 712 (31.80%) | 712 (31.80%) | |||
| Alcohol-associated hepatitis outcomes (bariatric surgery vs. no bariatric surgery) | OR | 95% CI | Test statistics | P-value | aOR | 95% CI | Test statistics | P-value |
| Cardiac arrest | 0.38 | 0.19–0.76 | 7.57 | <0.01 | 0.40 | 0.18–0.86 | 5.53 | 0.02 |
| ACS | 0.21 | 0.08–0.57 | 9.63 | <0.01 | 0.24 | 0.07–0.80 | 8.12 | 0.02 |
| AKI | 0.71 | 0.60–0.83 | 18.3 | <0.01 | 0.72 | 0.60–0.87 | 11.45 | <0.01 |
| Sepsis | 0.84 | 0.66–1.07 | 1.97 | 0.16 | 0.76 | 0.57–0.99 | 4.46 | 0.05 |
| Ileus | 0.37 | 0.19–0.72 | 8.48 | <0.01 | 0.45 | 0.21–0.95 | 4.52 | 0.03 |
| Acute MI | 0.25 | 0.09–0.66 | 7.73 | 0.01 | 0.7 | 0.08–0.92 | 5.96 | 0.04 |
| Shock | 0.81 | 0.53–1.24 | 0.93 | 0.33 | 0.87 | 0.53–1.42 | 0.23 | 0.57 |
| Venous thrombosis | 0.48 | 0.25–0.91 | 5.06 | 0.02 | 0.58 | 0.28–1.22 | 1.94 | 0.15 |
| PE | 1.00 | 0.53–1.89 | 0.00 | 1.00 | 1.15 | 0.55–2.44 | 0.11 | 0.71 |
| DVT | 1.00 | 0.42–2.41 | 0.00 | 1.00 | 1.10 | 0.40–3.08 | 1.94 | 0.85 |
| Portal vein thrombosis | 0.59 | 0.27–1.28 | 1.76 | 0.18 | 0.74 | 0.30–1.84 | 0.34 | 0.52 |
| GI bleeding | 1.12 | 0.88–1.44 | 0.88 | 0.35 | 1.18 | 0.89–1.57 | 2.08 | 0.26 |
| Decompensated liver disease | 0.67 | 0.57–0.86 | 11.35 | <0.01 | 0.58 | 0.44–0.77 | 6.33 | <0.01 |
| Abdominal CT | 1.06 | 0.54–2.11 | 0.03 | 0.86 | 1.36 | 0.62–3.01 | 0.70 | 0.44 |
| ARDS | 0.62 | 0.46–0.83 | 9.94 | <0.02 | 0.64 | 0.46–0.91 | 6.65 | 0.01 |
| Paracentesis | 1.51 | 0.80–2.84 | 1.59 | 0.21 | 1.27 | 0.61–2.63 | 0.81 | 0.52 |
| Cholecystectomy | 2.35 | 1.07–5.13 | 4.55 | 0.03 | 1.85 | 0.77–4.42 | 1.90 | 0.17 |
| Cholangiogram | 2.01 | 0.75–5.35 | 1.93 | 0.16 | 1.73 | 0.57–5.25 | 0.99 | 0.33 |
| Parenteral nutrition (TPN) | 1.51 | 0.53–4.23 | 0.59 | 0.44 | 1.10 | 0.33–3.70 | 0.02 | 0.87 |
| MACE | 0.75 | 0.62–0.90 | 9.87 | <0.01 | 1.13 | 0.89–1.42 | 0.03 | 0.32 |
| Heart failure | 0.87 | 0.69–1.10 | 1.30 | 0.25 | 1.29 | 0.93–1.79 | 0.20 | 0.12 |
| Death | 0.64 | 0.43–0.99 | 4.78 | 0.03 | 0.55 | 0.35–0.89 | 6.33 | 0.01 |
| Alcohol-associated hepatitis outcomes (bariatric surgery vs. no bariatric surgery) | IRR | 95% CI | Test statistics | P-value |
| Inflation-adjusted charges, ($) | -4,569.23 | -8,839.38 to -299.09 | 4.40 | 0.04 |
| Inflation-adjusted charges, ($) | -4,477.17 | -9,112.13 to 157.78 | 4.80 | 0.06 |
| Length of stay (days) | -0.12 | -0.42 to 0.18 | 0.60 | 0.44 |
| Length of stay (days) | -0.33 | -0.65 to 0.01 | 3.81 | 0.05 |
| Overall | History of bariatric surgery | No history of bariatric surgery | ||||
| Characteristics | Weighted number of U.S. hospitalizations, 2016–2020 | % (95% CI) | Weighted number of U.S. hospitalizations, 2016–2020 | Prevalence, % (95% CI) | Weighted number of U.S. hospitalizations, 2016–2020 | Prevalence, % (95% CI) |
| Sex | ||||||
| Male | 344,920 | 68.37 (68.06–68.68) | 2,815 | 0.82 (0.75–0.89) | 342,105 | 99.18 (99.11–99.25) |
| Female | 159,565 | 31.63 (31.32–31.94) | 8,995 | 5.64 (5.37–5.91) | 159,565 | 94.36 (94.09–94.63) |
| Total | 504,550 | 100 | 11,810 | 2.34 (2.24–2.44) | 492,740 | 97.66 (97.56–97.76) |
| Variable | Unadjusted | Adjusted | |||||
| OR (95% CI) | Test statistic | P-value | aOR (95% CI) | Test statistic | P-value | ||
| Gender | Females vs. males | 7.26 (6.60–7.99) | 22,406.96 | <0.01 | 6.90 (6.15–7.74) | 1,073.74 | <0.01 |
| Race | Whites (Ref) | ||||||
| Blacks | 1.21 (1.07-1.37) | 8.98 | <0.01 | 1.18 (1.04–1.35) | 7.08 | <0.01 | |
| Hispanics | 0.65 (0.56-0.75) | 33.0 | 0.58 | 0.80 (0.68–0.93) | 7.82 | 0.32 | |
| Asians | 0.40 (0.23-0.71) | 10.3 | 0.03 | 0.56 (0.32–1.00) | 3.96 | 0.30 | |
| Native American/Pacific Indians | 0.92 (0.72-1.19) | 0.42 | 0.10 | 1.08 (0.83–1.40) | 0.34 | 0.20 | |
| Outcome | OR (95% CI) | P-value | Test statistic | aOR (95% CI) | P-value | Test statistic | |
| Alcoholic hepatitis | |||||||
| All patients | Females versus males | 0.72 (0.62–0.94) | <0.01 | 9.57 | 0.94 (0.88–1.07) | 0.10 | 1.54 |
| Patients with bariatric surgery | Females versus males | 7.26 (6.60–7.99) | <0.01 | 1,653.21 | 6.90 (6.15–7.74) | <0.01 | 1,084.19 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlcohol Consumption and Health Effects · Alcoholism and Thiamine Deficiency · Substance Abuse Treatment and Outcomes
Introduction
Alcohol-associated liver disease (ALD) has become a leading cause of liver-related morbidity and mortality in the United States. Within ALD, alcohol-associated hepatitis (AAH) is an acute, life-threatening liver injury triggered by heavy alcohol use, with mortality of up to 30% in severe cases [1]. With a changing epidemiology of AAH, recent analyses report rising hospitalization and mortality rates for ALD, particularly among young adults and women [1]. This trend is driven in part by increased drinking patterns in these demographics [2]. Many patients with AAH have coexisting obesity or metabolic dysfunction, which may exacerbate liver injury through steatosis and inflammation [3]. Importantly, severe AAH can also occur in patients who are malnourished or lean, suggesting that obesity is not a uniform driver of disease severity [4,5]. Bariatric surgery leads to significant and sustained weight loss, thereby reducing comorbidities and mortality in patients with obesity [6], as well as lowering cardiovascular events and improving survival [7]. Additionally, among patients with obesity and compensated cirrhosis, bariatric surgery is associated with improved long-term survival at an acceptable cost, suggesting that improving metabolic health can favorably modify outcomes of chronic liver disease [8].
While bariatric surgery improves metabolic risk factors, it has been associated with an increased risk of alcohol use disorder (AUD) due to a combination of altered alcohol metabolism, changes in neurohormonal and reward pathways, and psychosocial factors such as addiction transfer [6,9]. Post-bariatric surgery, around 20-30% of patients report increased alcohol intake or new AUD, with about 5% developing ALD [10]. Overall, approximately 80% of bariatric procedures in the United States are performed in White individuals, while Hispanic women have the lowest rates [11]. Data on the clinical outcomes of patients who develop severe AAH after surgery are lacking.
Given this background, we designed this study to address two questions: (1) Does a history of bariatric surgery impact the clinical outcomes of patients hospitalized with AAH? (2) Are there gender or racial disparities in the occurrence of AAH and outcomes among patients post-bariatric surgery? By addressing these questions, we aim to inform clinical strategies for risk stratification and long-term follow-up in bariatric patients, while also guiding health policy to improve care for individuals at the intersection of obesity and ALD.
Materials and methods
Data source and study population
We conducted a retrospective study using the National Inpatient Sample (NIS) database for the years 2016-2020 [12]. The NIS is the largest all-payer inpatient database in the United States, containing a 20% stratified sample of hospital discharges nationwide, and it provides weighted estimates for national hospitalization trends [12].
We identified adult hospitalizations with AAH as the primary diagnosis. The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic codes were used to capture AAH, specifically, code K70.1 (alcoholic hepatitis) and its sub-classifications (e.g., K70.11 for alcoholic hepatitis with ascites, K70.10 without ascites). We included discharges aged ≥18 years. We excluded a small number of encounters with missing key outcome data (e.g., missing discharge disposition, which is needed to determine in-hospital mortality) or implausible patient demographics (e.g., invalid age). If a patient had multiple AAH admissions in the dataset, each admission was treated as a separate observation. The entire adult NIS population was used to estimate the odds of AAH hospitalizations. The other analysis was conducted with the AAH-only cohort for assessing outcomes.
Exposure
The exposure of interest was the history of bariatric surgery before or during the index admission. We identified bariatric surgery using a combination of International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) procedure codes and ICD-10-CM diagnosis codes indicative of a past bariatric procedure. The specific codes captured common metabolic/bariatric operations, namely, Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, biliopancreatic diversion/duodenal switch, and gastric banding. We included codes for both open and laparoscopic approaches. Different bariatric procedures were analyzed as a composite variable.
Outcomes and definitions
The primary outcome was in-hospital mortality, defined by discharge disposition of death in the hospital. Secondary outcomes included hepatic decompensation events, a composite of acute complications of liver failure during hospitalization, including ascites, hepatic encephalopathy, variceal hemorrhage, or hepatorenal syndrome; length of stay (LOS), measured in days from admission to discharge; and hospitalization cost, total hospital charges converted to cost using cost-to-charge ratios, adjusted for inflation to 2020 USD. We also captured patient demographics, hospital characteristics, and comorbid conditions.
Statistical analysis
We first described patient characteristics in the bariatric surgery versus no bariatric surgery groups before matching, including demographics, hospital characteristics, and comorbidities. We compared these characteristics using chi-square tests for categorical variables and t-tests or Wilcoxon rank-sum tests for continuous variables as appropriate.
A propensity score for having undergone bariatric surgery before admission was calculated for each patient using a logistic regression model. A 1:1 matching was performed for the bariatric surgery group versus the non-bariatric surgery group using nearest-neighbor matching without replacement, with a caliper width of 0.2 standard deviations of the logit of the propensity score. Matching variables included baseline characteristics (age, sex, primary payer source, race, median household income, weekend admission, elective admission, region of hospital, hospital size, location), clinical comorbidities (diabetes, hypertension), and outcomes (in-hospital mortality, overall cost, hepatic decompensation, cardiac arrest, sepsis, acute respiratory distress syndrome, gastrointestinal bleeding, acute kidney injury, heart failure, portal vein thrombosis, major adverse cardiovascular event, LOS, death). Balance of covariates post-matching was assessed using standardized mean differences (SMDs), with an SMD <0.1 indicating good balance.
After matching, we compared outcomes between the two groups. Chi-square tests were used for categorical outcomes and t-test or Wilcoxon rank-sum (as appropriate) for continuous outcomes in the unadjusted analysis. We then fit multivariable logistic regression models on the matched to estimate the adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for each binary outcome associated with prior bariatric surgery and AAH. For LOS and cost, we used generalized linear models to estimate adjusted differences. These models adjusted for any residual imbalanced covariates post-propensity score matching.
We subsequently performed subgroup analyses by sex and race. First, we estimated the weighted prevalence of AAH, stratified by sex. We then performed a logistic regression analysis to assess the odds of AAH hospitalization in patients with prior bariatric surgery across race and sex. Finally, we conducted an exploratory analysis to compare outcomes of AAH in patients with prior bariatric surgery by sex and race/ethnicity.
All analyses incorporated NIS survey weights to derive national estimates. A two-sided p-value <0.05 was considered statistically significant. Statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The study used de-identified public data and was exempt from institutional review board approval.
Results
Patient characteristics and bariatric surgery utilization
Over the five-year study period (2016-2020), we identified 100,910 adult hospitalizations for AAH among patients in the NIS sample, corresponding to 504,550 weighted hospitalizations nationwide. Among these, only 2.30% had a documented history of bariatric surgery (unweighted n = 2,362). Approximately three-quarters of the AAH patients with prior bariatric surgery were female compared to only about one-third in the no-surgery group (p < 0.01) (Table 1). The cohort’s mean age was around 47.60 ± 12 years, with the majority falling in the 40-60-year age range.
Significant differences in race and ethnicity were observed between groups (p < 0.01) (Table 1). Patients with prior bariatric surgery were more likely to be non-Hispanic White (around 73% of the surgery group vs. 70% of the no-surgery group) and less likely to be Hispanic (8% vs. 12% in the no-surgery group). The proportion of Black patients was similar between groups (about 14% in the surgery group vs. 11% in the no-surgery group). Other racial groups (Asian/Pacific Islander, Native American, and other/unknown) each constituted 1-3% of the cohort in either group. Socioeconomic differences were also evident in the primary payer mix (p < 0.01). Patients with prior bariatric surgery were more likely to have private insurance (18% vs. 16) and less likely to be insured through Medicaid (33% vs. 40%) compared to those without bariatric surgery.
Table 2 presents the baseline characteristics after 1:1 propensity score matching. We matched 2,242 patients with a history of bariatric surgery to 2,242 patients without bariatric surgery. Post-matching balance diagnostics demonstrated excellent covariate balance, with SMDs ranging from 0.000 to 0.042 across key variables, including age, calendar year, comorbidity burden, socioeconomic status, and hospital characteristics. The range of SMDs was well below the conventional threshold of 0.10, indicating excellent balance between groups (Table 2).
In-hospital outcomes: mortality and complications
After matching, patients with prior bariatric surgery had a 45% lower odds of in-hospital mortality from AAH compared to patients without prior bariatric surgery (aOR = 0.55, 95% CI = 0.35-0.89; p = 0.01) (Figure 1).
Adjusted ratios (ORs or IRRs) and 95% confidence intervals (CIs) for key clinical outcomes comparing hospitalized alcohol-associated hepatitis patients with versus without a history of bariatric surgery. Bariatric surgery was associated with reduced odds of in-hospital mortality and major complications.
We also observed significant reductions in several major complications of AAH among patients with prior bariatric surgery (Figure 1). In the matched cohort, the incidence of acute hepatic decompensation events was lower in the bariatric surgery group. Specifically, the adjusted odds of any hepatic decompensation were 42% lower in the bariatric group compared to the no-surgery group (aOR = 0.58, 95% CI = 0.44-0.77; p = 0.01) Similarly, there was a 28% reduction in the odds of acute kidney injury among patients with prior bariatric surgery (aOR = 0.72, 95% CI = 0.60-0.87; p < 0.01). Other complications followed a similar trend in the adjusted model with significantly lower odds observed among patients with a history of bariatric surgery: cardiac arrest (aOR = 0.40, 95% CI = 0.18-0.86; p = 0.02), acute respiratory distress syndrome (aOR = 0.64, 95% CI = 0.46-0.91; p = 0.01), and sepsis (aOR = 0.76, 95% CI = 0.58-0.99; p = 0.04). The odds of gastrointestinal bleeding, portal vein thrombosis, and shock were comparable between the bariatric and non-bariatric groups, with no significant differences: gastrointestinal bleeding (aOR = 1.18, 95% CI = 0.89-1.57; p = 0.26), portal vein thrombosis (aOR = 0.74, 95% CI = 0.30-1.84; p = 0.52), and shock (aOR = 0.87, 95% CI = 0.53-1.42; p = 0.57) (Table 3).
Length of stay and resource utilization
The median LOS in the bariatric surgery group was 7 days (interquartile range (IQR) = 4-12 days) compared to 8 days (IQR = 5-14) for the no-surgery group. In the adjusted analysis, this difference was not statistically significant (adjusted mean difference of about -0.33 days, 95% CI = -0.65 to +0.01, p = 0.05).
Hospitalization costs were high for AAH in general. The mean total cost per admission was about 90,000 (2020 USD) in both groups. After adjusting for factors, the average cost for the bariatric group was about 4,477, 95% CI = -158), with a p-value of 0.06 (Table 4).
Subgroup analyses by sex and race
The weighted prevalence of AAH hospitalizations was significantly lower among patients with a history of bariatric surgery compared to those without. Of the 504,550 weighted hospitalizations for AAH, only 2.34% (n = 11,810) occurred in patients with prior bariatric surgery, while 97.66% (n = 492,740) occurred in patients without a history of bariatric surgery (Table 5).
Stratified by sex, the prevalence of AAH hospitalizations in males was generally higher (68.37%, 344,920 weighted hospitalizations) compared to females (31.63%, 159,565 weighted hospitalizations). However, among patients with prior bariatric surgery, the prevalence of AAH was markedly lower in males (0.82%) than in females (5.64%). Logistic regression analysis revealed that sex and race significantly modified the odds of AAH hospitalization in patients with prior bariatric surgery. Females had a substantially higher odds of hospitalization for AAH compared to males (aOR = 6.90, 95% CI = 6.15-7.74, p < 0.01) (Tables 6, 7).
Regarding race, the odds of AAH hospitalization were higher for Black patients (aOR = 1.18, 95% CI = 1.04-1.35, p < 0.01), while Hispanic (aOR = 0.80, 95% CI = 0.68-0.93, p = 0.32) and Asian (aOR = 0.56, 95% CI = 0.32-1.00, p = 0.30) patients had lower odds compared to Whites (reference group) (Table 5).
We further examined clinical outcomes among AAH patients with a history of bariatric surgery, stratified by sex and race/ethnicity. Outcomes evaluated included major adverse cardiovascular events, acute kidney injury, sepsis, decompensated liver disease, and in-hospital mortality. No significant differences in outcomes were observed across sex or racial/ethnic groups.
Discussion
In this large national analysis of hospitalized AAH patients, we found striking disparities in the occurrence of AAH after bariatric surgery: women and Black patients were disproportionately represented among post-surgical AAH hospitalizations. Importantly, despite these disparities in occurrence, we also observed that hospitalized patients with AAH and prior bariatric surgery had significantly better inpatient outcomes compared to those without such a history, including lower mortality and reduced odds of hepatic decompensation, acute kidney injury, respiratory failure, sepsis, and cardiac arrest.
While prior studies have explored the risk of ALD following bariatric surgery [9,13], this study is among the first to highlight racial and gender disparities in AAH hospitalizations among this population. This study is also the first national study to challenge prevailing assumptions that prior bariatric surgery worsens alcohol-related liver outcomes and suggests a potentially protective association during acute AAH episodes.
Previous studies have emphasized the potential harms of bariatric surgery in patients with heavy alcohol use. For example, a recent single-center study of 2,634 patients hospitalized for AAH reported that those with prior RYGB had no difference in inpatient mortality but did have higher 30-day readmission rates and significantly worse longer-term outcomes, including increased cirrhosis progression and post-discharge mortality [14]. An earlier NIS-based analysis also reported that prior RYGB was associated with increased risk of hepatic encephalopathy and serious infections among patients hospitalized with ALD, although in-hospital mortality did not differ [15]. These earlier reports align with the established concern that bariatric surgery, especially RYGB, can exacerbate alcohol’s hepatotoxic effects [16,17]. However, our study provides a new perspective: in the acute hospital phase of AAH, prior bariatric surgery was not associated with worse outcomes, and, in fact, was linked to significantly better short-term outcomes. Several factors may explain this divergence. Unlike the single-center RYGB study, our analysis included all types of bariatric procedures (RYGB, sleeve gastrectomy, etc.) and employed propensity score matching to reduce confounding. Our cohort is more contemporary (2016-2020) and reflects a shift in surgical trends, with sleeve gastrectomy now more common and potentially less impactful on alcohol metabolism than RYGB [17]. Finally, by restricting our cohort to patients with obesity-related history, we ensured both groups shared a similar metabolic background, which may have minimized “healthy survivor” bias and allowed us to isolate differences attributable to bariatric surgery itself.
Several hypotheses could explain the observed protective association of prior bariatric surgery with acute AAH outcomes. First, patients who underwent bariatric surgery likely achieved substantial weight loss and metabolic improvement before their AAH episode. Weight loss leads to reduced visceral adiposity, lower systemic inflammation, and improved insulin sensitivity, all of which could positively influence the course of critical illnesses such as severe AAH [18-20]. In contrast, patients with no prior surgery who present with AAH and obesity may suffer a “double hit,” i.e., the synergistic liver insult of obesity-related metabolic dysfunction plus alcohol toxicity [21]. Prior bariatric surgery might attenuate one component of this synergy by ameliorating the obesity and metabolic syndrome factors [18]. It is plausible that in patients with a history of obesity and heavy alcohol use, weight loss, whether surgical or not, reduces baseline hepatic steatosis/fibrosis and systemic inflammation, such that when AAH occurs, the liver and other organs are able to tolerate acute injury. This may explain the significantly lower odds of complications such as acute kidney injury and acute respiratory distress syndrome observed in the bariatric group.
Another contributing factor may be selection and healthcare engagement. Patients who undergo bariatric surgery typically have extensive pre-surgical evaluation and post-surgical follow-up [22,23]. Those who developed AAH despite prior bariatric surgery may represent a subgroup with better healthcare access, potentially leading to earlier recognition and management of complications. Further, it may be that patients with prior bariatric surgery experience a less severe form of AAH (perhaps requiring lower alcohol exposure to trigger hepatitis due to altered alcohol kinetics) and thus present with lower baseline liver injury severity. Unfortunately, granular data on AAH severity (e.g., bilirubin or creatinine levels) were not available in our dataset. Nevertheless, the significantly reduced occurrence of acute-on-chronic liver failure features, captured in our composite “hepatic decompensation” outcome, among patients with prior bariatric surgery suggests they may have presented with less advanced chronic liver disease. In essence, these patients might develop AAH earlier in their disease trajectory, potentially leading to better survival prospects. This interpretation is supported by reports showing that RYGB patients have an elevated risk of developing ALD, including AAH, which may indicate a “fast-tracked” progression to severe injury without prolonged subclinical disease [6,24]. Post-bariatric surgery patients experience better management of any ensuing metabolic syndrome, including lower rates of obesity and diabetes at the time of acute liver injury, which reduces the severity of the initial presentation and reduces the adverse outcome of AAH [9]. Furthermore, higher household income and lower-level education have been identified as risk factors for AUD following bariatric surgery. However, in our study, we did not observe any significant association in the household income of the patients between those who have had prior bariatric surgery and those who have not had bariatric surgery. In addition, patients with previous bariatric surgery are well represented in addiction treatment programs, suggesting that they may be more likely to seek, or be referred to, treatment for their alcohol use disorder [13,25].
Our findings have several important clinical implications. First, they underscore the necessity for proactive alcohol use screening and counseling in high-risk patients undergoing bariatric surgery. Bariatric programs should ensure long-term vigilance for hazardous drinking, especially among female and Black patients. Early intervention may prevent progression to AAH. Second, our results deliver a cautiously optimistic clinical message: an episode of AAH post-bariatric surgery does not confer worse immediate prognosis; indeed, it may be associated with a better short-term outcome compared to non-surgical peers. Clinicians can be somewhat reassured that a history of bariatric surgery does not increase in-hospital mortality risk. Nevertheless, management of AAH remains complex; these patients still require robust initiation of secondary prevention strategies, such as alcohol cessation support and referral to addiction services, because prior studies have demonstrated that post-bariatric surgery patients are at an elevated risk for progressive liver disease over time, particularly among women [26,27].
We acknowledge several limitations of our study. Foremost, the retrospective observational design using NIS is subject to unmeasured confounding and coding inaccuracies. We relied on ICD-10 codes to identify AAH, comorbidities, and prior bariatric surgery status, making misclassification a possibility. We attempted to capture bariatric surgery history comprehensively using both procedure codes and status codes, but we could not determine the timing of surgery relative to the AAH hospitalization or the amount of weight lost. Another limitation is the absence of clinical details, such as laboratory values, in the NIS. Hence, we could not directly compare the severity of AAH between groups. We partly mitigated this by matching on comorbidity burden. Furthermore, there is a chance of selection bias as patients who undergo surgery are screened for psychosocial stability and health. Post-bariatric surgery patients are more likely to be enrolled in an AUD treatment program. Despite these limitations, our study boasts notable strengths. To our knowledge, it is the first nationally representative analysis examining racial and gender disparity outcomes of AAH in the context of prior bariatric surgery, leveraging a large sample size with contemporary ICD-10 coding. The use of propensity score matching improved the comparability of groups, and the consistency of findings across multiple outcomes supports the robustness of the association.
Conclusions
This study demonstrated that among patients with an obesity-related history hospitalized for AAH, those with prior bariatric surgery experience significantly improved in-hospital outcomes, including lower mortality and complication rates. However, this clinical benefit is offset by disparities in the demographic profile of those affected. Women and Black patients were overrepresented among post-bariatric AAH hospitalizations, suggesting disproportionate vulnerability in these groups. These findings highlight the importance of integrating metabolic and addiction care while optimizing postoperative care and long-term monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alcohol-associated liver disease mortality JAMA Netw Open Pan CW Abboud Y Chitnis A Zhang W Singal AK Wong RJ 08202510.1001/jamanetworkopen.2025.14857 PMC 1215977240498484 · doi ↗ · pubmed ↗
- 2Historical trends in young adult solitary alcohol use by age and sex from 1977 to 2022 Alcohol Clin Exp Res (Hoboken) Creswell KG Arterberry BJ Patrick ME 175917674920254057725010.1111/acer.70103 PMC 12365587 · doi ↗ · pubmed ↗
- 3Metabolic and alcohol-associated liver disease (Met ALD): a representation of duality Gut Liver Leal-Lassalle H Estévez-Vázquez O Cubero FJ Nevzorova YA 122025
- 4Alcoholic liver disease and malnutrition Alcohol Clin Exp Res Mc Clain CJ Barve SS Barve A Marsano L 8158203520112128467310.1111/j.1530-0277.2010.01405.x PMC 3771636 · doi ↗ · pubmed ↗
- 5Malnutrition and alcohol-associated hepatitis Clin Liver Dis Mc Clain CJ Rios CD Condon S Marsano LS 5575702520213422983910.1016/j.cld.2021.03.002PMC 8672300 · doi ↗ · pubmed ↗
- 6Alcohol associated liver disease and bariatric surgery: current perspectives and future directions World J Gastrointest Surg Cooper KM Colletta A Hebda N Devuni D 6506571620243857709610.4240/wjgs.v 16.i 3.650PMC 10989338 · doi ↗ · pubmed ↗
- 7Cardiovascular outcomes and mortality after bariatric surgery in patients with nonalcoholic fatty liver disease and obesity JAMA Netw Open Krishnan A Hadi Y Alqahtani SA 06202310.1001/jamanetworkopen.2023.7188 PMC 1008240237027156 · doi ↗ · pubmed ↗
- 8Survival and cost-effectiveness of bariatric surgery among patients with obesity and cirrhosis JAMA Surg Bansal S Bader A Mahmud N Kaplan DE 64565516020254017287110.1001/jamasurg.2025.0490 PMC 11966474 · doi ↗ · pubmed ↗